Influence of Chromium-Cobalt-Molybdenum Alloy (ASTM F75) on Bone Ingrowth in an Experimental Animal Model

Abstract
:1. Introduction
2. Results
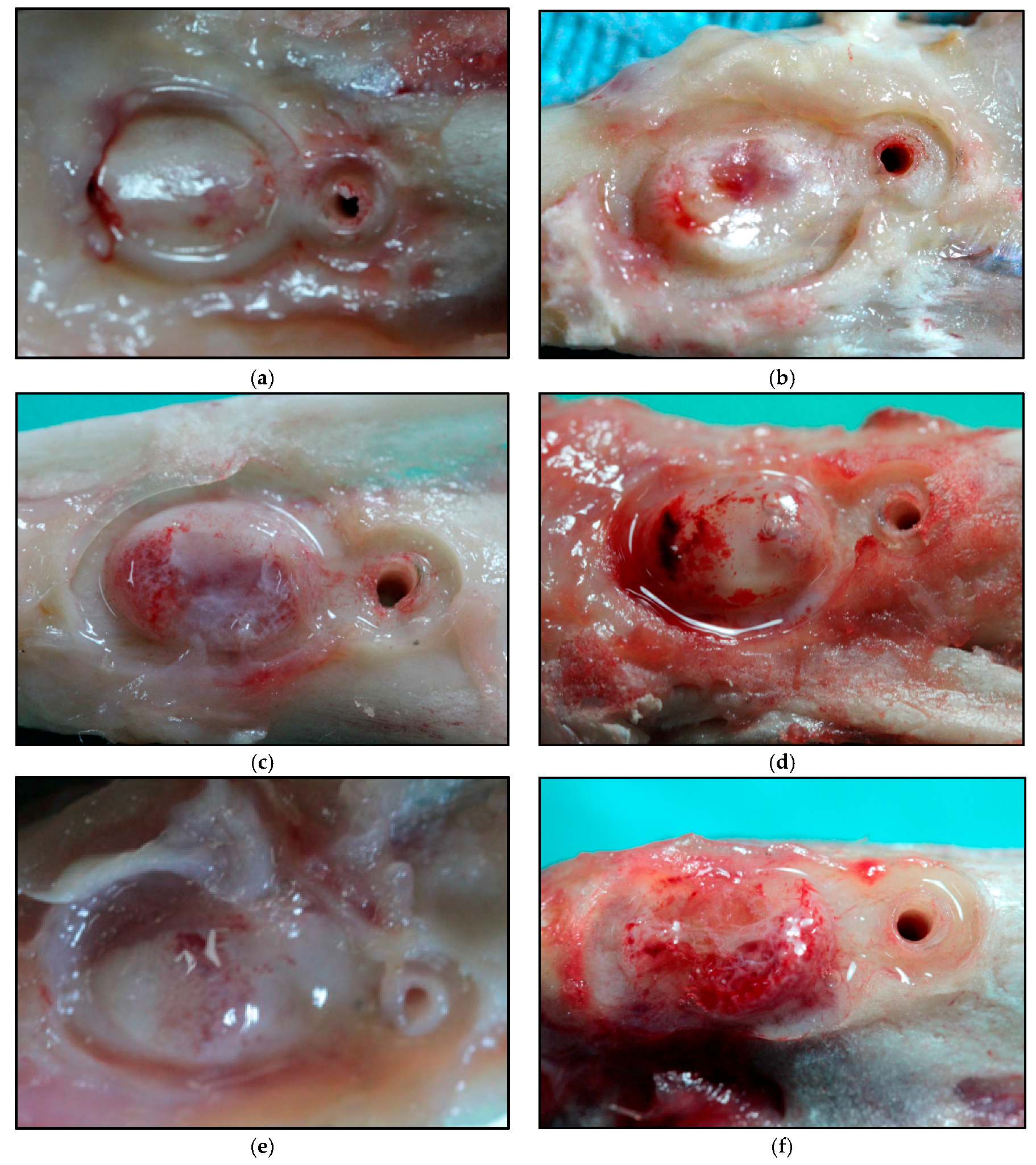
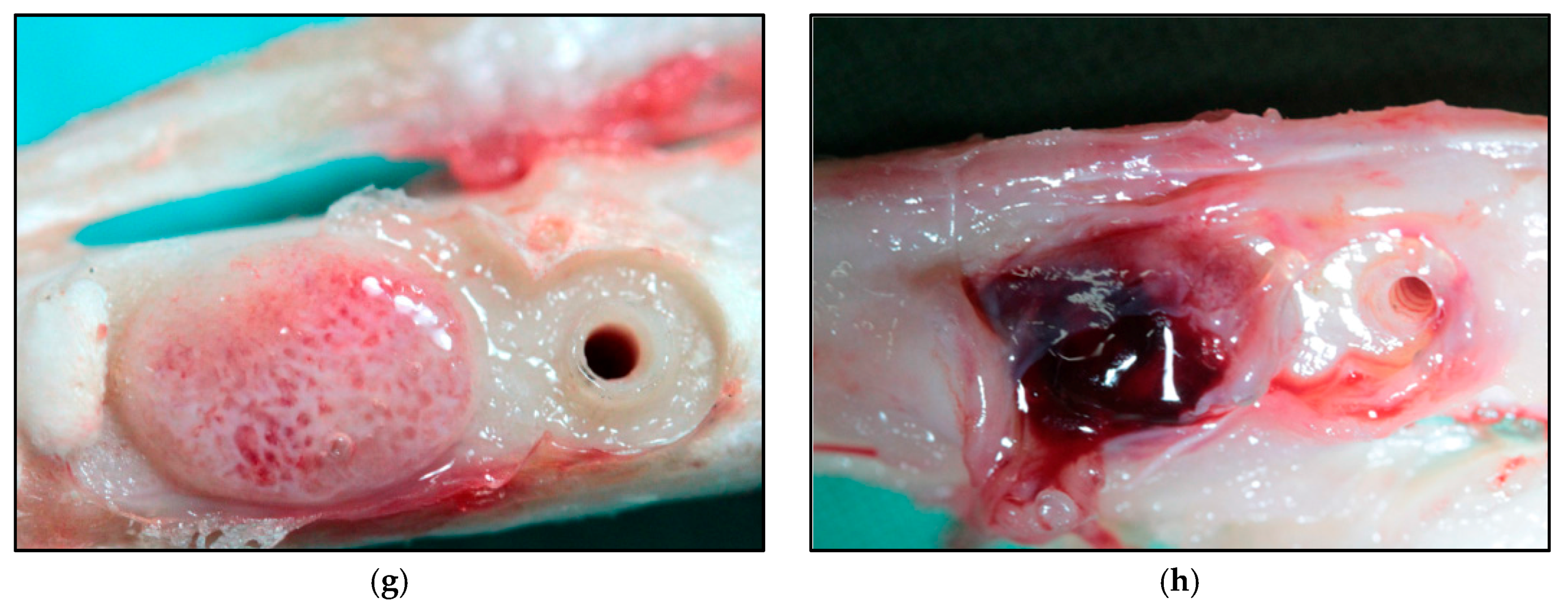
2.1. Macroscopic Analysis
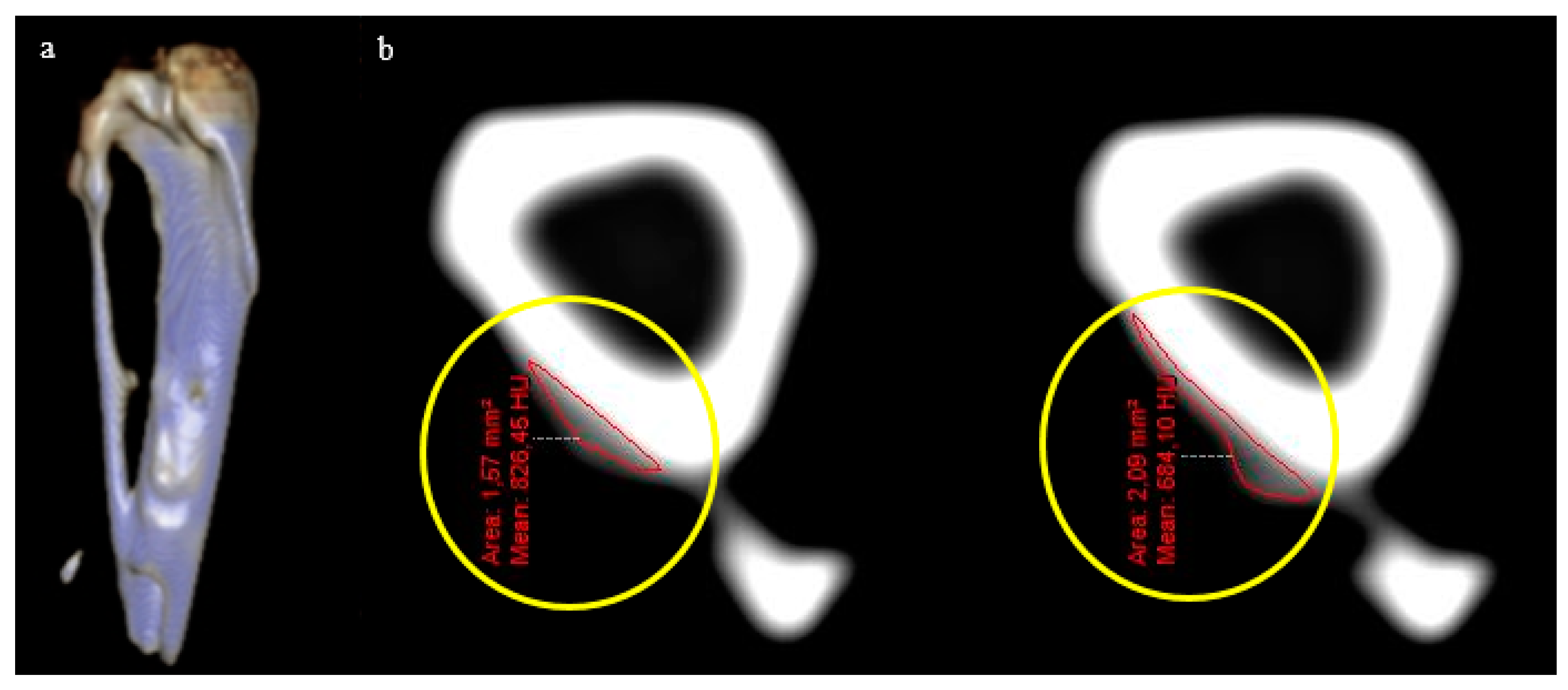
2.2. Tomographic Analysis
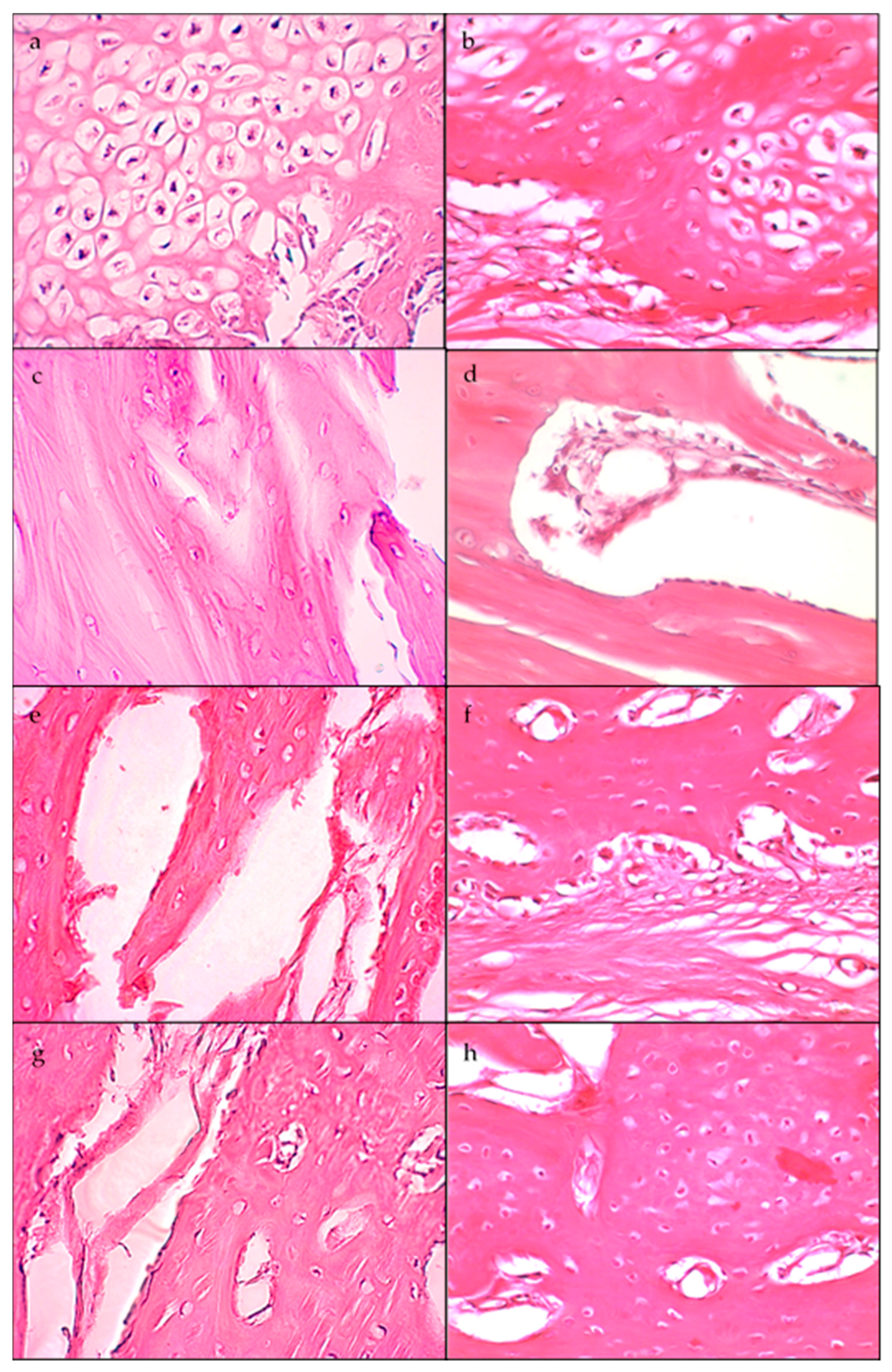
2.3. Histological Analysis
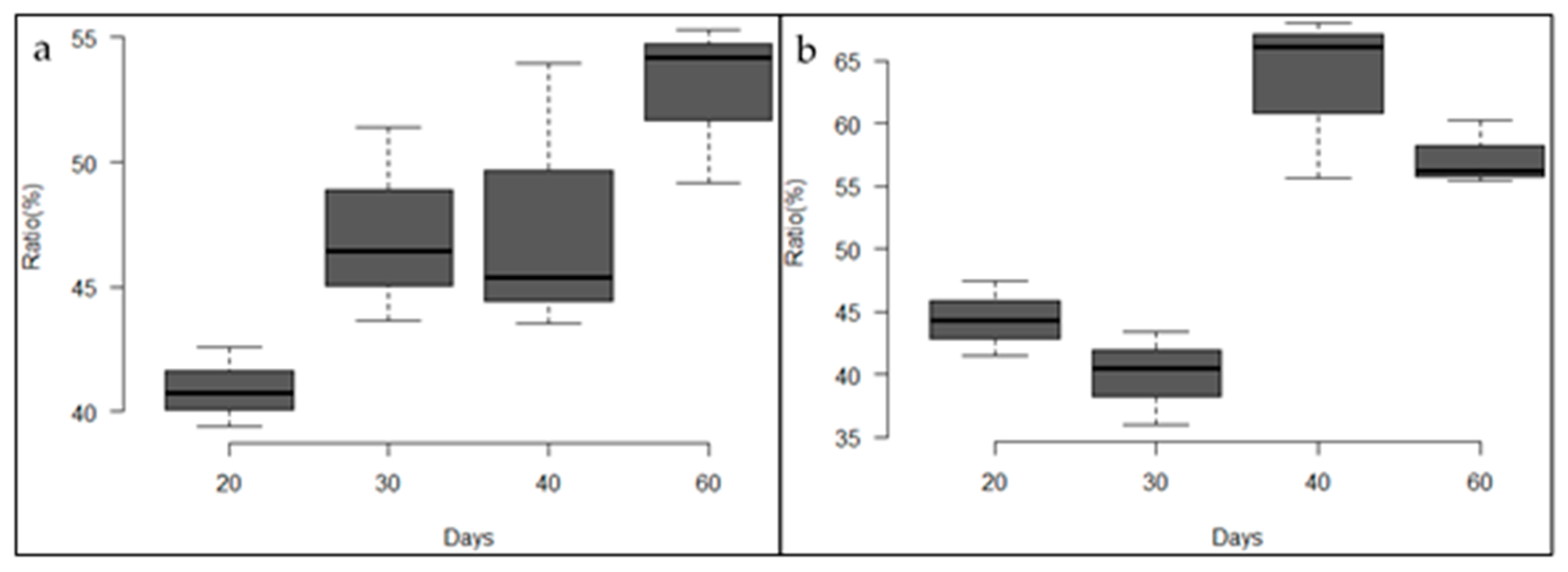
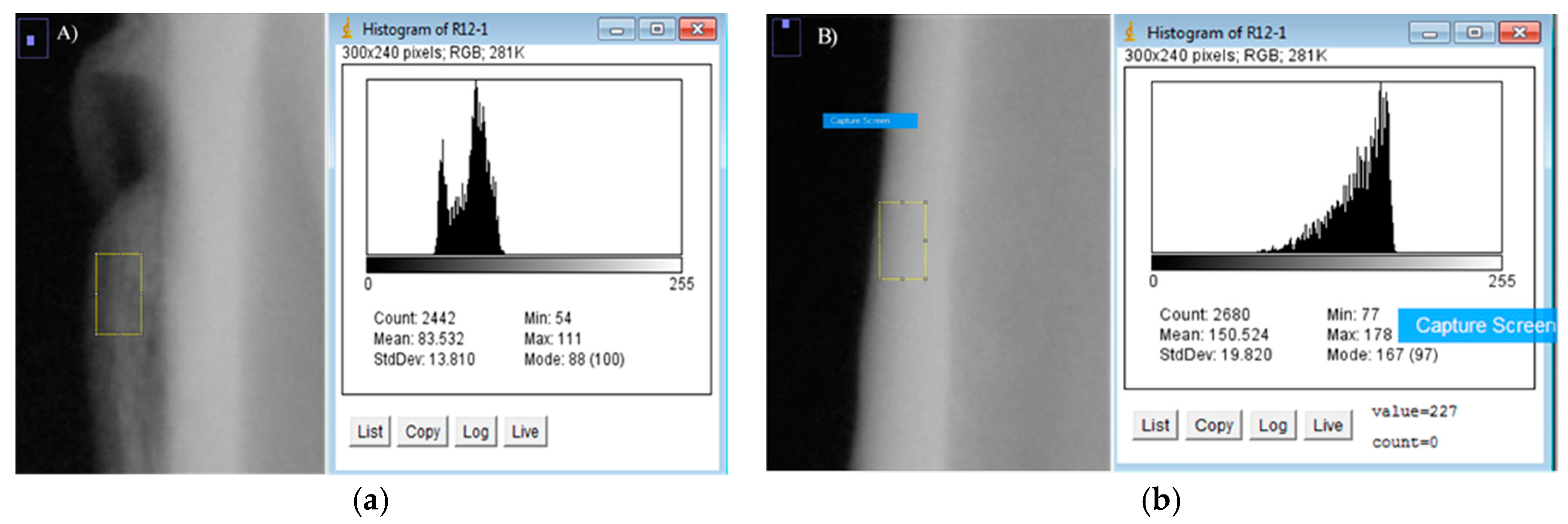
2.4. Densitometric Analysis
3. Discussion
4. Materials and Methods
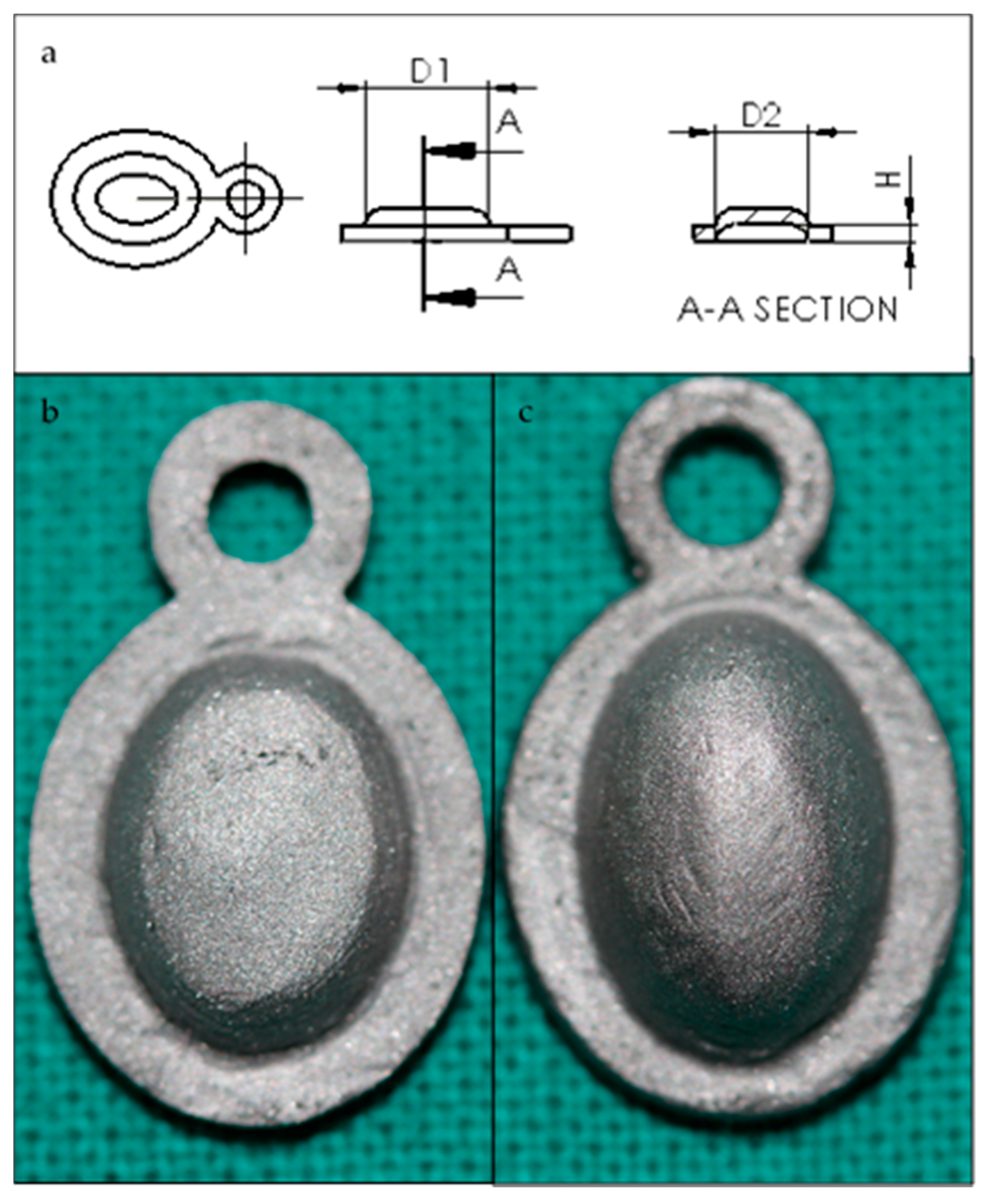
4.1. Cr-Co-Mo Membranes Manufacture
4.2. Surgical Procedure
4.3. Analysis
Author Contributions
Conflicts of Interest
References
- Henkel, J.; Woodruff, M.A.; Epari, D.R.; Steck, R.; Glatt, V.; Dickinson, I.C.; Hutmacher, D.W. Bone regeneration based on tissue engineering conceptions—A 21st century perspective. Bone Res. 2013, 1, 216. [Google Scholar] [CrossRef] [PubMed]
- Jardini, M.A.; De Marco, A.C.; Lima, L.A. Early healing pattern of autogenous bone grafts with and without e-PTFE membranes: A histomorphometric study in rats. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 666–673. [Google Scholar] [CrossRef] [PubMed]
- De Long, W.G.; Einhorn, T.A.; Koval, K.; McKee, M.; Smith, W.; Sanders, R.; Watson, T. Bone grafts and bone graft substitutes in orthopaedic trauma surgery: A critical analysis. J. Bone Jt. Surg. Am. 2007, 89, 649–658. [Google Scholar] [CrossRef]
- Landro, M.E.; Francalaccia, V.; Douglas Price, A.L. Medicina regenerative: Su aplicación en traumatología. Rev. Asoc. Argent. Ortop. Traumatol. 2010, 75, 398–403. [Google Scholar]
- Myeroff, C.; Archdeacon, M. Autogenous bone graft: Donor sites and techniques. J. Bone Jt. Surg. Am. 2011, 93, 2227–2236. [Google Scholar] [CrossRef] [PubMed]
- Masquelet, A.C.; Fitoussi, F.; Begue, T.; Muller, G.P. Reconstruction of the long bones by the induced membrane and spongy autograft. Ann. Chir. Plast. Esthet. 2000, 45, 346–353. [Google Scholar] [PubMed]
- Klaue, K.; Knothe, U.; Masquelet, A. Effet biologique des membranes à corps etranger induites in situ sur la consolidation des greffes d’os spongieux. Rev. Chir. Orthop. Suppl. 1995, 70, 109–110. [Google Scholar]
- Pelissier, P.; Masquelet, A.; Bareille, R.; Mathoulin, S.; Amedee, J. Induced membranes secrete growth factors including vascular and osteoinductive factors and could stimulate bone regeneration. J. Orthop. Res. 2004, 22, 73–79. [Google Scholar] [CrossRef]
- Aho, O.M.; Lehenkari, P.; Ristiniemi, J.; Lehtonen, S.; Risteli, J.; Leskelä, H.V. The mechanism of action of induced membranes in bone repair. J. Bone Jt. Surg. Am. 2013, 95, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Qin, C.H.; Ma, Y.F.; Wang, L.; Yu, B. Possibility of one-stage surgery to reconstruct bone defects using the modified Masquelet technique with degradable calcium sulfate as a cement spacer: A case report and hypothesis. Biomed. Rep. 2016, 4, 374–378. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, N.T.; Kates, S.L. Advances on the Masquelet technique using a cage and nail construct. Arch. Orthop. Trauma Surg. 2012, 132, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Masquelet, A.C. The Evolution of the Induced Membrane Technique: Current Status and Future Directions. Tech. Orthop. 2016, 31, 3–8. [Google Scholar] [CrossRef]
- Van Steenberghe, D.; Johansson, C.; Quirynen, M.; Molly, L.; Albrektsson, T.; Naert, I. Bone augmentation by means of a stiff occlusive titanium barrier. Clin. Oral Implants Res. 2003, 14, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Decco, O.; Cura, A.; Beltrán, V.; Lezcano, F.; Engelke, W. Bone augmentation in rabbit tibia using microfixed cobalt-chromium membranes with whole blood, tricalcium phosphate and bone marrow cells. Int. J. Clin. Exp. Med. 2015, 8, 135–144. [Google Scholar] [PubMed]
- Decco, O.A.; Beltrán, V.; Zuchuat, J.I.; Cura, A.C.; Lezcano, M.F.; Engelke, W. Bone Augmentation in Rabbit Tibia Using Microfixed Cobalt-Chromium Membranes with Whole Blood and Platelet-Rich Plasma. Materials 2015, 8, 4843–4856. [Google Scholar] [CrossRef] [PubMed]
- Zechner, W.; Tangl, S.; Tepper, G. Influence of platelet-rich plasma on osseous healing of dental implants: A histologic and histomorphometric study in mini pigs. Int. J. Oral Maxillofac. Implants 2003, 18, 15–22. [Google Scholar] [PubMed]
- Zellin, G.; Linde, A. Importance of delivery systems for growth-stimulatory factors in combination with osteopromotive membranes. An experimental study using rhBMP-2 in rat mandibular defects. J. Biomed. Mater. Res. 1997, 35, 181–190. [Google Scholar] [CrossRef]
- Antoun, H.; Sitbon, J.M.; Martinez, H.; Missika, P. A prospective randomized study comparing two techniques of bone augmentation: Onlay graft alone or associated with a membrane. Clin. Oral Implants Res. 2001, 12, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E.; Schupbach, P.; Cooper, L. The implant surface and biological response. In Osseointegration and Dental Implants; Jokstad, A., Ed.; Wiley-Blackwell: Oxford, UK, 2009; pp. 213–223. [Google Scholar]
- Carr, B.C.; Goswami, T. Knee implants-Review of models and biomechanics. Mater. Des. 2009, 30, 398–413. [Google Scholar] [CrossRef]
- Sánchez-De Jesús, F.; Bolarín-Miró, A.M.; Torres-Villaseñor, C.A.; Cortés-Escobedo, C.A.; Betancourt-Cantera, J.A. Mechanical alloying of biocompatible Co-28Cr-6Mo alloy. J. Mater. Sci. Mater. Med. 2010, 21, 2021–2026. [Google Scholar] [CrossRef] [PubMed]
- Grgązka-Dahlke, M.; Dąbrowski, J.R.; Dąbrowski, B. Modification of mechanical properties of sintered implant materials on the base of Co-Cr-Mo alloy. J. Mater. Process. Technol. 2008, 204, 199–205. [Google Scholar] [CrossRef]
- Hoshi, S.; Akizuki, T.; Matsuura, T.; Ikawa, T.; Kinoshita, A.; Oda, S.; Izumi, Y. Ridge augmentation using recombinant human fibroblast growth factor-2 with biodegradable gelatin sponges incorporating β-tricalcium phosphate: A preclinical study in dogs. J. Periodontal Res. 2016, 51, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.H.; Lim, G.; Chan, H.L.; Giannobile, W.V.; Wang, H.L. Recombinant human bone morphogenetic protein 2 outcomes for maxillary sinus floor augmentation: A systematic review and meta-analysis. Clin. Oral Implants Res. 2016, 27, 1349–1359. [Google Scholar] [CrossRef] [PubMed]
- Seibert, J.; Nyman, S. Localized ridge augmentation in dogs: A pilot study using membranes and hydroxyapatite. J. Periodontol. 1990, 61, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Bartolucci, E.; Clauser, C.; Pini Prato, G.P. Localized ridge augmentation using guided tissue regeneration in humans. Clin. Oral Implants Res. 1993, 4, 203–209. [Google Scholar] [CrossRef]
- Yamada, Y.; Sato, S.; Yagi, H.; Ujiie, H.; Ezawa, S.; Ito, K. Correlation in the densities of augmented and existing bone in guided bone augmentation. Clin. Oral Implants Res. 2012, 23, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Park, Y.J.; Park, S.N.; Lee, Y.M.; Seol, Y.J.; Ku, Y.; Chung, C.P. Molded porous poly (l-lactide) membranes for guided bone regeneration with enhanced effects by controlled growth factor release. J. Biomed. Mater. Res. 2001, 55, 295–303. [Google Scholar] [CrossRef]
- Ito, K.; Nanba, K.; Murai, S. Effects of bioabsorbable and non-resorbable barrier membranes on bone augmentation in rabbit calvaria. J. Periodontol. 1998, 69, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Rakhmatia, Y.D.; Ayukawa, Y.; Furuhashi, A.; Koyano, K. Current barrier membranes: Titanium mesh and other membranes for guided bone regeneration in dental applications. J. Prosthodont. Res. 2013, 57, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Takiguchi, T.; Kobayashi, M.; Susuki, R.; Yamaguchi, A.; Isatsu, K.; Nishihara, T.; Nagumo, M.; Hasegawa, K. Recombinant human bone morphogenetic protein −2 stimulates osteoblast differentiation and suppresses matrix metalloproteinase −1 production in human bone cells isolated from mandibulae. J. Periodont. Res. 1998, 33, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Davidovitch, Z. Biological Mechanism of Tooth Movement, 2nd ed.; Wiley Blackwell: West Sussex, UK, 2015; ISBN 978-1-118-68887-8. [Google Scholar]
- Cassell, O.; Morrison, W.A.; Messina, A.; Penington, A.J.; Thompson, E.W.; Stevens, G.W.; Perera, J.M.; Kleinman, H.K.; Hurley, J.V.; Romeo, R.; et al. The influence of extracellular matrix on the generation of vascularized, engineered, transplantable tissue. Ann. N. Y. Acad. Sci. 2001, 944, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.L.S. Reinforced Multi-Layered Membrane. U.S. Patent Application No. 14,635,940, 2 March 2015. [Google Scholar]
- Friedenberg, Z.B.; Harlow, M.C.; Heppenstall, B.; Brighton, C.T. Bioelectric potentials in bone. Calcif. Tissue Res. 1973, 13, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Chiarenza, A.R.; Weiss, C.M. Method and Apparatus for Stimulating Osteogenic Activity in Bone Structure Adjacent a Dental Implant. U.S. Patent No. 4,175,565, 27 November 1979. [Google Scholar]
- Park, J.; Lakes, R.S. Biomaterials: An Introduction, 3rd ed.; Springer Science & Business Media: New York, NY, USA, 2007; ISBN 978-0-387-37879-4. [Google Scholar]
- Degidi, M.; Scarano, A.; Piattelli, A. Regeneration of the alveolar crest using titanium micromesh with autologous bone and a resorbable membrane. J. Oral Implantol. 2003, 29, 86–90. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Days | Standard Membrane | High Membrane |
|---|---|---|
| Augmentation Volume [mm3] | Augmentation Volume [mm3] | |
| 20 | 15.63 | 18.23 |
| 30 | 20.61 | 20.66 |
| 40 | 22.79 | 17.58 |
| 60 | 27.16 | 11.41 |
| Days | Average Osteoblasts | Average Osteocytes | ||
|---|---|---|---|---|
| Standard Membrane | High Membrane | Standard Membrane | High Membrane | |
| 20 | 960 (10 fgm) | 310 (10 fgm) | 580 (10 fgm) | 940 (10 fgm) |
| 30 | 50 (4 fgm) | 1400 (10 fgm) | 270 (4 fgm) | 1100 (10 fgm) |
| 40 | 1000 (10 fgm) | 300 (10 fgm) | 680 (10 fgm) | 400 (10 fgm) |
| 60 | 33 (10 fgm) | 310 (10 fgm) | 360 (10 fgm) | 800 (10 fgm) |
| Days | Standard Membrane | High Membrane | ||||
|---|---|---|---|---|---|---|
| ROIint (SD) | ROIref (SD) | Ratio (%) | ROIint (SD) | ROIref (SD) | Ratio | |
| 20 | 77.90 (0.85) | 190.61 (8.64) | 40.91 (1.61) | 65.86 (2.29) | 148.48 (4.91) | 44.42 (3.01) |
| 30 | 59.66 (5.69) | 127.51 (20.99) | 47.16 (3.92) | 64.92 (5.13) | 162.51 (3.33) | 39.99 (3.76) |
| 40 | 78.68 (8.18) | 165.38 (3.09) | 47.62 (5.57) | 117.65 (13.74) | 185.86 (3.82) | 63.24 (6.64) |
| 60 | 86.04 (1.80) | 163.12 (13.55) | 52.93 (3.28) | 106.39 (4.29) | 185.77 (1.17) | 57.28 (2.58) |
| Control | 153.46 (0.97) | 162.94 (1.59) | 94.19 (1.51) | 153.97 (0.57) | 163.88 (2.05) | 93.96 (1.45) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zuchuat, J.; Berli, M.; Maldonado, Y.; Decco, O. Influence of Chromium-Cobalt-Molybdenum Alloy (ASTM F75) on Bone Ingrowth in an Experimental Animal Model. J. Funct. Biomater. 2018, 9, 2. https://doi.org/10.3390/jfb9010002
Zuchuat J, Berli M, Maldonado Y, Decco O. Influence of Chromium-Cobalt-Molybdenum Alloy (ASTM F75) on Bone Ingrowth in an Experimental Animal Model. Journal of Functional Biomaterials. 2018; 9(1):2. https://doi.org/10.3390/jfb9010002
Chicago/Turabian StyleZuchuat, Jésica, Marcelo Berli, Ysaí Maldonado, and Oscar Decco. 2018. "Influence of Chromium-Cobalt-Molybdenum Alloy (ASTM F75) on Bone Ingrowth in an Experimental Animal Model" Journal of Functional Biomaterials 9, no. 1: 2. https://doi.org/10.3390/jfb9010002
APA StyleZuchuat, J., Berli, M., Maldonado, Y., & Decco, O. (2018). Influence of Chromium-Cobalt-Molybdenum Alloy (ASTM F75) on Bone Ingrowth in an Experimental Animal Model. Journal of Functional Biomaterials, 9(1), 2. https://doi.org/10.3390/jfb9010002