Nail Properties and Bone Health: A Review



Abstract
:1. Introduction
2. Association between Nail Mineral Composition and BMD
3. Association between Nail Protein and BMD
4. Association between Nail and Bone Proteins
Nail Viscoelastic Properties and Bone Health
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Price, C.T.; Langford, J.R.; Liporace, F.A. Essential nutrients for bone health and a review of their availability in the average north american diet. Open Orthop. J. 2012, 6, 143–149. [Google Scholar] [CrossRef] [PubMed]
- O’Flaherty, E.J. Modeling normal aging bone loss, with consideration of bone loss in osteoporosis. Toxicol. Sci. 2000, 55, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Sui, L.; Gai, P.; Li, G.; Qi, X.; Jiang, X. The efficacy and safety of vertebral fracture prevention therapies in post-menopausal osteoporosis treatment: Which therapies work best? A network meta-analysis. Bone Jt. J. 2017, 6, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, M.C.; Cummings, S.R. Type of fall and risk of hip and wrist fractures: The study of osteoporotic fractures. The study of osteoporotic fractures research group. J. Am. Geriatr. Soc. 1993, 41, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Heilmeier, U.; Youm, J.; Torabi, S.; Link, T.M. Osteoporosis imaging in the geriatric patient. Curr. Radiol. Rep. 2016, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Aaron, J.E.; Shore, P.A.; Shore, R.C.; Beneton, M.; Kanis, J.A. Trabecular architecture in women and men of similar bone mass with and without vertebral fracture: II. Three-dimensional histology. Bone 2000, 27, 277–282. [Google Scholar] [CrossRef]
- Banse, X.; Devogelaer, J.P.; Delloye, C.; Lafosse, A.; Holmyard, D.; Grynpas, M. Irreversible perforations in vertebral trabeculae? J. Bone Miner. Res. 2003, 18, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, E.A.; Busse, B.; Ritchie, R.O. The fracture mechanics of human bone: Influence of disease and treatment. BoneKEy Rep. 2015, 4, 743. [Google Scholar] [CrossRef] [PubMed]
- Brzozka, P.; Kolodziejski, W. Sex-related chemical differences in keratin from fingernail plates: A solid-state carbon-13 nmr study. RSC Adv. 2017, 7, 28213–28223. [Google Scholar] [CrossRef]
- Ohgitani, S.; Fujita, T.; Fujii, Y.; Hayashi, C.; Nishio, H. Nail calcium and magnesium content in relation to age and bone mineral density. J. Bone Miner. Metab. 2005, 23, 318–322. [Google Scholar] [PubMed]
- Yesil, Y.; Kuyumcu, M.E.; Ozturk, Z.A.; Ulger, Z.; Sahin, U.; Cankurtaran, M.; Halil, M.; Yavuz, B.B.; Vural, H.; Kara, Y.; et al. The relationship between metabolic bone diseases and fingernail calcium levels in the elderly. Eur. Geriatr. Med. 2012, 3, 341–344. [Google Scholar] [CrossRef]
- Mehra, R.; Juneja, M. Variation of concentration of heavy metals, calcium and magnesium with sex as determined by atomic absorption spectrophotometry. Indian J. Environ. Health 2003, 45, 317–324. [Google Scholar] [PubMed]
- Djaldetti, M.; Fishman, P.; Hart, J. The iron content of finger-nails in iron deficient patients. Clin. Sci. (Lond.) 1987, 72, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.R.; Zhang, S.Q.; Xiong, Y.; Zhao, Y.; Fu, H.; Zhang, H.P.; Xiong, K.M. Studies of five microelement contents in human serum, hair, and fingernails correlated with aged hypertension and coronary heart disease. Biol. Trace Elem. Res. 2003, 92, 97–104. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Gorgojo, L.; Riemersma, R.A.; Gomez-Aracena, J.; Kark, J.D.; Guillen, J.; Jimenez, J.; Ringstad, J.J.; Fernandez-Crehuet, J.; Bode, P.; et al. Myocardial infarction risk in relation to zinc concentration in toenails. Br. J. Nutr. 2003, 89, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Kardinaal, A.F.; Kok, F.J.; Kohlmeier, L.; Martin-Moreno, J.M.; Ringstad, J.; Gomez-Aracena, J.; Mazaev, V.P.; Thamm, M.; Martin, B.C.; Aro, A.; et al. Association between toenail selenium and risk of acute myocardial infarction in European men. The euramic study. European antioxidant myocardial infarction and breast cancer. Am. J. Epidemiol. 1997, 145, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Aracena, J.; Riemersma, R.A.; Gutierrez-Bedmar, M.; Bode, P.; Kark, J.D.; Garcia-Rodriguez, A.; Gorgojo, L.; Van’t Veer, P.; Fernandez-Crehuet, J.; Kok, F.J.; et al. Toenail cerium levels and risk of a first acute myocardial infarction: The euramic and heavy metals study. Chemosphere 2006, 64, 112–120. [Google Scholar] [CrossRef] [PubMed]
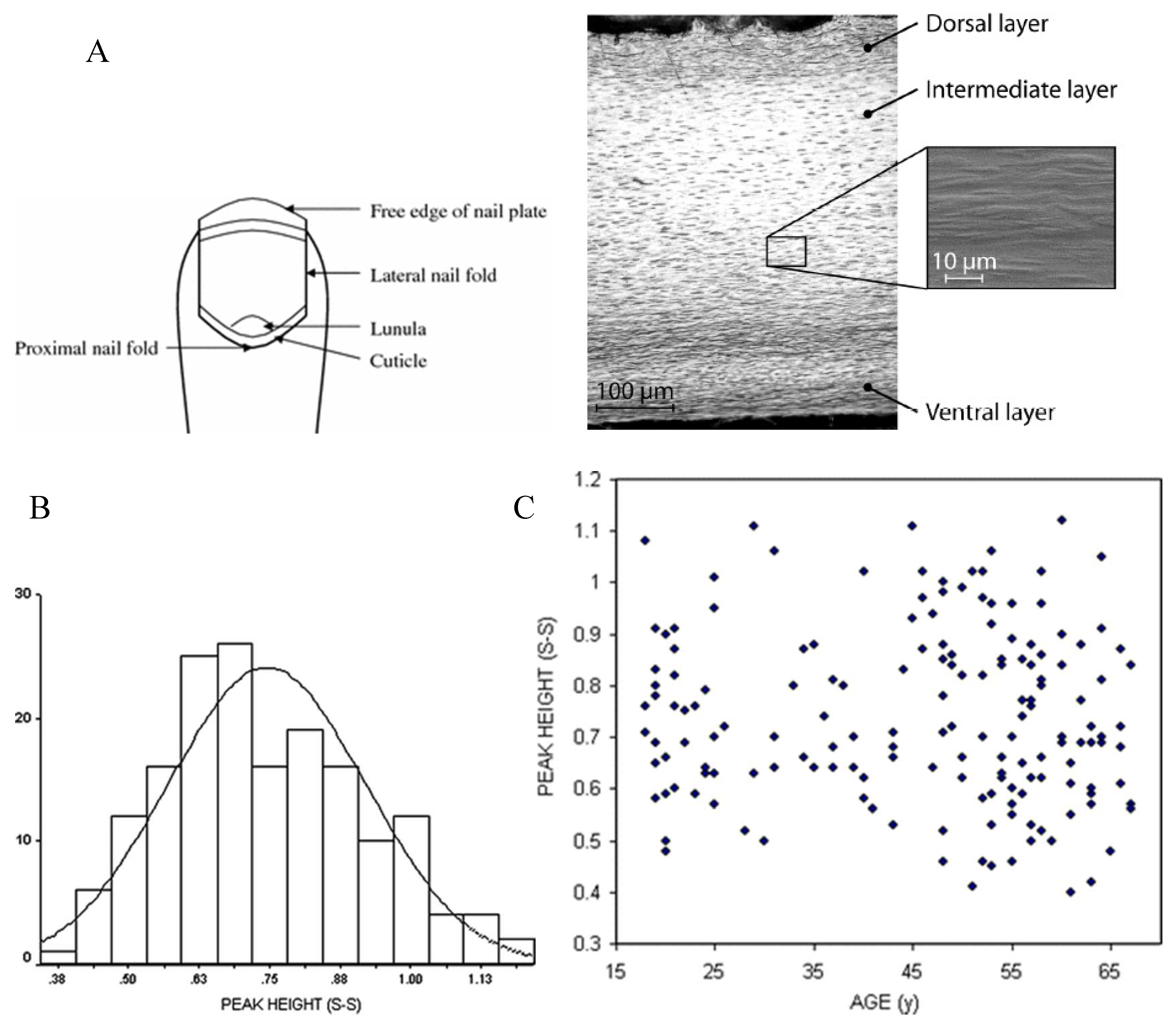
- De Berker, D. Nail anatomy. Clin. Dermatol. 2013, 31, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Beattie, J.R.; Pawlak, A.M.; Boulton, M.E.; Zhang, J.; Monnier, V.M.; McGarvey, J.J.; Stitt, A.W. Multiplex analysis of age-related protein and lipid modifications in human bruch’s membrane. FASEB J. 2010, 24, 4816–4824. [Google Scholar] [CrossRef] [PubMed]
- Buckley, K.; Matousek, P.; Parker, A.W.; Goodship, A.E. Raman spectroscopy reveals differences in collagen secondary structure which relate to the levels of mineralisation in bones that have evolved for different functions. J. Raman Spectrosc. 2012, 43, 1237–1243. [Google Scholar] [CrossRef]
- Rey, C.; Combes, C.; Drouet, C.; Glimcher, M.J. Bone mineral: Update on chemical composition and structure. Osteoporos. Int. 2009, 20, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Vecht-Hart, C.M.; Bode, P.; Trouerbach, W.T.; Collette, H.J. Calcium and magnesium in human toenails do not reflect bone mineral density. Clin. Chim. Acta 1995, 236, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Bahreini, M.; Hosseinimakarem, Z.; Hassan Tavassoli, S. A study of association between fingernail elements and osteoporosis by laser-induced breakdown spectroscopy. J. Appl. Phys. 2012, 112, 054701. [Google Scholar] [CrossRef]
- Razmandeh, R.; Nasli-Esfahani, E.; Heydarpour, R.; Faridbod, F.; Ganjali, M.R.; Norouzi, P.; Larijani, B.; Khoda-Amorzideh, D. Association of zinc, copper and magnesium with bone mineral density in iranian postmenopausal women—A case control study. J. Diabetes Metab. Disord. 2014, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Karita, K.; Takano, T. [Relation of fingernail mineral concentrations to bone mineral density in elderly japanese women]. Nihon Koshu Eisei Zasshi 1994, 41, 759–763. [Google Scholar] [PubMed]
- Karita, K.; Takano, T.; Nakamura, S.; Haga, N.; Iwaya, T. A search for calcium, magnesium and zinc levels in fingernails of 135 patients with osteogenesis imperfecta. J. Trace Elem. Med. Biol. 2001, 15, 36–39. [Google Scholar] [CrossRef]
- Van Dijk, F.S.; Cobben, J.M.; Kariminejad, A.; Maugeri, A.; Nikkels, P.G.J.; van Rijn, R.R.; Pals, G. Osteogenesis imperfecta: A review with clinical examples. Mol. Syndromol. 2011, 2, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Reichenbächer, M.; Popp, J. Vibrational spectroscopy. In Challenges in Molecular Structure Determination; Reichenbächer, M., Popp, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 63–143. [Google Scholar]
- Pandey, G.; Nakamura, T.; Singh, R.P. Investigation into the correlation between viscoelastic properties of fingernails and osteoporosis. In Proceedings of the XIth International Congress and Exposition, Orlando, FL, USA, 2–5 June 2008; Society for Experimental Mechanics Inc.: Orlando, FL, USA, 2008. [Google Scholar]
- Kuzuhara, A. Analysis of internal structure changes in black human hair keratin fibers resulting from bleaching treatments using raman spectroscopy. J. Mol. Struct. 2013, 1047, 186–193. [Google Scholar] [CrossRef]
- Towler, M.R.; Wren, A.; Rushe, N.; Saunders, J.; Cummins, N.M.; Jakeman, P.M. Raman spectroscopy of the human nail: A potential tool for evaluating bone health? J. Mater. Sci. Mater. Med. 2007, 18, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Carron, K.; Towler, M. Method for Determination of Bone Fracture Risk Using Raman Spectroscopy. Google Patents US20090012403A1, 8 January 2009. [Google Scholar]
- Moran, P.; Towler, M.R.; Chowdhury, S.; Saunders, J.; German, M.J.; Lawson, N.S.; Pollock, H.M.; Pillay, I.; Lyons, D. Preliminary work on the development of a novel detection method for osteoporosis. J. Mater. Sci. Mater. Med. 2007, 18, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Pillay, I.; Lyons, D.; German, M.J.; Lawson, N.S.; Pollock, H.M.; Saunders, J.; Chowdhury, S.; Moran, P.; Towler, M.R. The use of fingernails as a means of assessing bone health: A pilot study. J. Womens Health 2005, 14, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Mussatto, J.C.; Perez, M.C.; de Souza, R.A.; Pacheco, M.T.T.; Zângaro, R.A.; Silveira, L. Could the bone mineral density (t-score) be correlated with the raman spectral features of keratin from women’s nails and be used to predict osteoporosis? Lasers Med. Sci. 2015, 30, 287–294. [Google Scholar] [CrossRef] [PubMed]
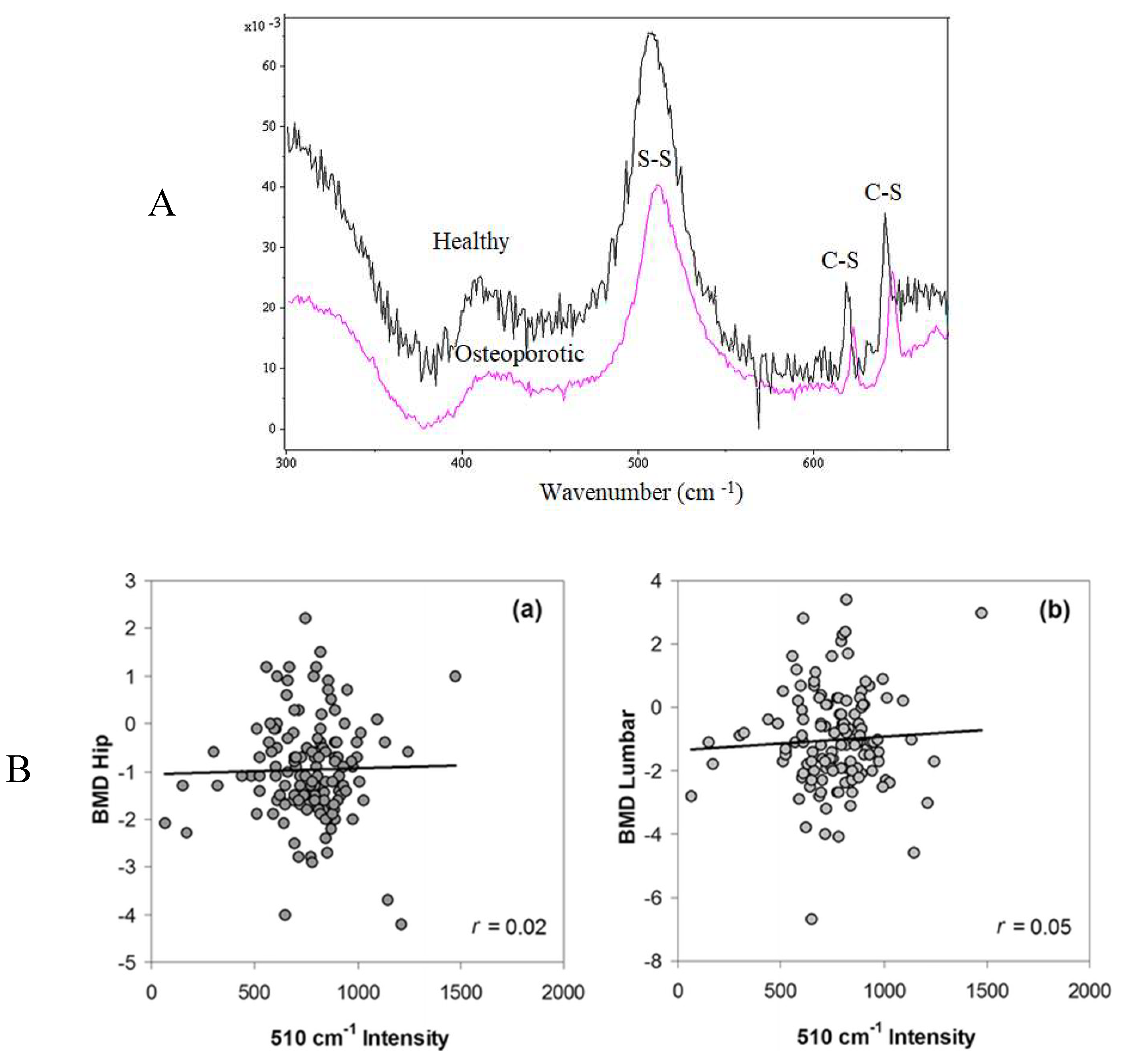
- Beattie, J.R.; Caraher, M.C.; Cummins, N.M.; O’Driscoll, O.M.; Eastell, R.; Ralston, S.H.; Towler, M.R. Raman spectral variation for human fingernails of postmenopausal women is dependent on fracture risk and osteoporosis status. J. Raman Spectrosc. 2017, 48, 813–821. [Google Scholar] [CrossRef]
- Cummins, N.M.; Day, J.C.C.; Wren, A.; Carroll, P.; Murphy, N.; Jakeman, P.M.; Towler, M.R. Raman spectroscopy of fingernails: A novel tool for evaluation of bone quality? Spectroscopy 2010, 24, 517–524. [Google Scholar] [CrossRef]
- Weinstein, S.L.; Buckwalter, J.A. Turek’s Orthopaedics: Principles and Their Application; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Beattie, J.R.; Cummins, N.M.; Caraher, C.; O’Driscoll, O.M.; Bansal, A.T.; Eastell, R.; Ralston, S.H.; Stone, M.D.; Pearson, G.; Towler, M.R. Raman spectroscopic analysis of fingernail clippings can help differentiate between postmenopausal women who have and have not suffered a fracture. Clin. Med. Insights Arthritis 2016, 9, 109–116. [Google Scholar]
- Delany, A.M.; Amling, M.; Priemel, M.; Howe, C.; Baron, R.; Canalis, E. Osteopenia and decreased bone formation in osteonectin-deficient mice. J. Clin. Investig. 2000, 105, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.L.; Keck, P.C.; Sampath, T.K.; Rueger, D.C.; Carlson, W.D. Three-dimensional structure of recombinant human osteogenic protein 1: Structural paradigm for the transforming growth factor beta superfamily. Proc. Natl. Acad. Sci. USA 1996, 93, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Hossein-nezhad, A.; Sadeghi Afjeh, M.; Saghafi, H.; Rahmani, M.; Parviz, M.; Maghbooli, Z.; Larijani, B. The fingernail protein content may predict bone turnover in postmenopausal women. Iran J. Public Health 2008, 37, 55–62. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Sample Population | Country | Measurements | Result | Ref |
|---|---|---|---|---|
| n = 135, 61 osteogenesis imperfecta (OI) males and 74 females 1–61 years old. 61 males and 74 females healthy controls | Japan | AAS | Significantly higher Levels of Zn in OI nails. The ratios of Ca/Zn and Mg/Zn in OI nails differed significantly from those in controls. Zn Levels in fingernails may reflect abnormal Zn metabolism in OI. | [26] |
| n = 123, Postmenopausal women 53–56 years old | Iran | DXA, X-ray Radiography Serum Osteocalcin and Cross laps concentrations | Fingernail protein content significantly correlated with serum. Cross laps concentration, lumbar spine BMD, and total hip BMD fingernail protein content predicted vertebral fracture. | [42] |
| n = 159, ≥65 years old | Turkey | DXA, AAS | No statistically significant difference in nail Ca levels between osteoporotic and non-osteoporotic patients and similarly between vitamin D deficient and normal patients. No change in nail Ca concentrations in osteoporosis and vitamin D deficiency. | [11] |
| n = 2, One healthy 38 years old male; One osteoporotic 65 years old female | USA | Nano indentation Raman spectroscopy | Osteoporotic nail samples showed greater creep than non-osteoporotic nail samples. | [29] |
| n = 169, Females aged 18–67 years old | Ireland | Raman spectroscopy DXA | Lower disulphide content in women postmenopause. The disulphide content of nails from women with a history of fracture was significantly lower than those with no history of fracture. | [31] |
| n = 22, 9 osteoporotic 13 non osteoporotic | Ireland | Nano indentation Raman spectroscopy | Significantly lower S–S bond content fingernail in the osteoporotic group. The differences in nano indentation were not statistically significant. | [33] |
| n = 22, 9 osteoporotic 13 non osteoporotic | Ireland | Nano indentation Raman spectroscopy | The differences in nano indentation were not statistically significant. Sharper disulfide bond peak for nail from control group than for the nail from the osteoporosis group | [34] |
| n = 184, 69 women 115 men and 20–80 years old | Japan | AAS for Ca and Mg DXA | Mineral content may be utilized as one of the indicators of bone mineral metabolism. Fingernail and toenail Ca concentrations decreased with age in both men and women. Postmenopausal women had lower nail Ca concentrations than premenopausal women. LBMD showed a significant positive correlation with nail Ca content. | [10] |
| n = 8, Postmenopausal women 36–60 years old | Iran | ICP-AES for Zn, Copper and Mg and DXA | No correlation between case and control groups in trace minerals in the nail samples. | [24] |
| n = 99, 27 healthy, 47 osteopenic, and 25 osteoporotic | Iran | LIBS Sodium, potassium, Ca and iron, Mg and silicon | The classification between nail samples of healthy, osteopenic, and osteoporotic subjects is attainable. Some evidence for association between osteoporosis and elemental composition of fingernails measured by LIBS. | [23] |
| n = 633, Postmenopausal women | UK/Ireland | Raman spectroscopy and DXA | Raman spectroscopy can provide insight into a subject’s fracture risk. Increasing disorder in S–S bonding orientation transition from alpha helical secondary structure to random differences in the amino acid composition of the two groups. | [36,39] |
| n = 220, Women 54.6 ± 9.1 years old | Netherland | INAA for Ca and Mg DXA | Ca and Mg measurements in nail clippings by INAA cannot be used for screening purposes in the prevention of osteoporosis. | [22] |
| n = 159, Women 18–67 years old | Ireland | Raman spectroscopy DXA | Raman spectroscopy of keratin may have potential as a diagnostic tool for screening bone quality in large populations. | [37] |
| n = 213 women | Brazil | Raman spectroscopy DXA | No differences in the mean Raman spectra of nails of groups with and without osteoporosis. BMD and fracture risk could not be assessed by the nail keratin features. | [35] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeedi, P.; Shavandi, A.; Meredith-Jones, K. Nail Properties and Bone Health: A Review. J. Funct. Biomater. 2018, 9, 31. https://doi.org/10.3390/jfb9020031
Saeedi P, Shavandi A, Meredith-Jones K. Nail Properties and Bone Health: A Review. Journal of Functional Biomaterials. 2018; 9(2):31. https://doi.org/10.3390/jfb9020031
Chicago/Turabian StyleSaeedi, Pouya, Amin Shavandi, and Kim Meredith-Jones. 2018. "Nail Properties and Bone Health: A Review" Journal of Functional Biomaterials 9, no. 2: 31. https://doi.org/10.3390/jfb9020031
APA StyleSaeedi, P., Shavandi, A., & Meredith-Jones, K. (2018). Nail Properties and Bone Health: A Review. Journal of Functional Biomaterials, 9(2), 31. https://doi.org/10.3390/jfb9020031