Development and Evaluation of an Injectable Chitosan/β-Glycerophosphate Paste as a Local Antibiotic Delivery System for Trauma Care



Abstract
:1. Introduction
2. Results
2.1. Cytocompatibility
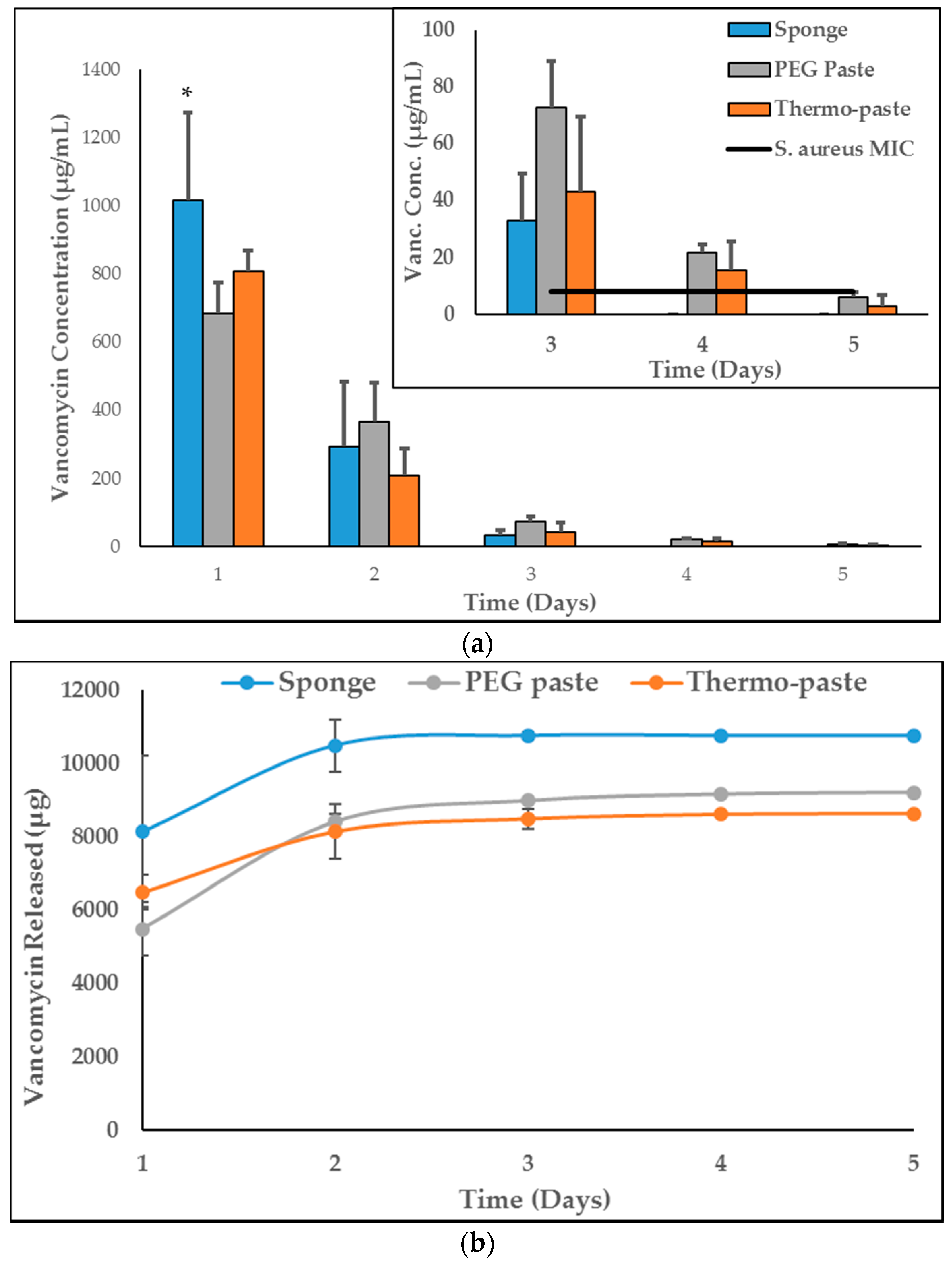
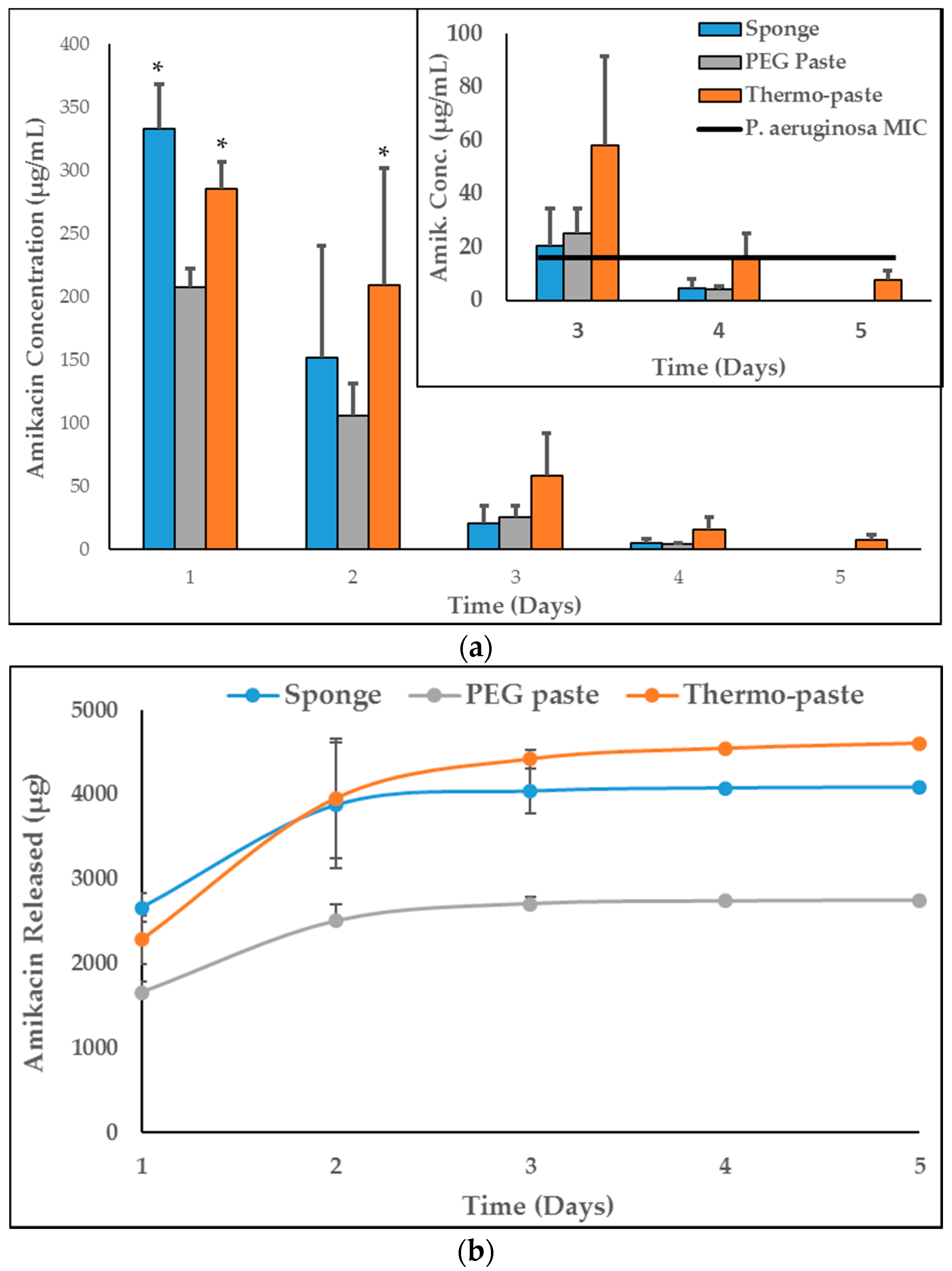
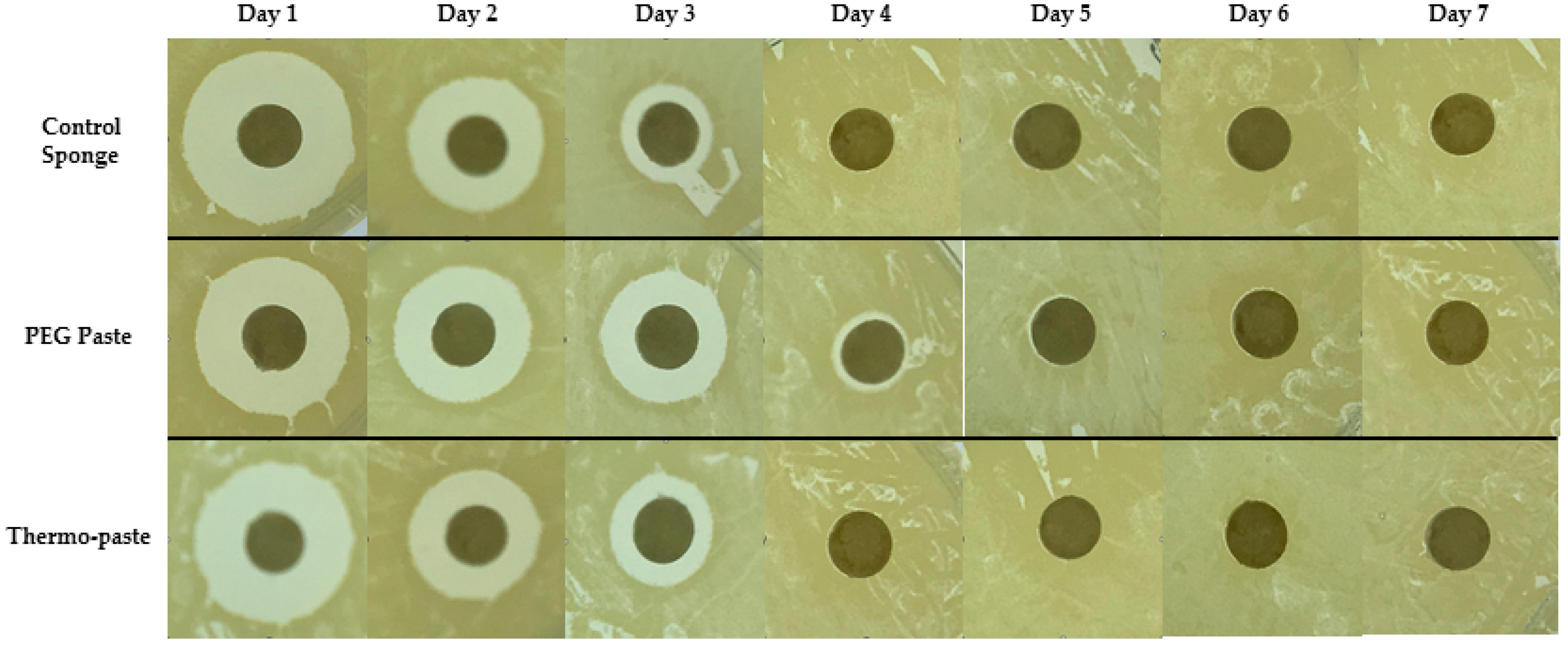
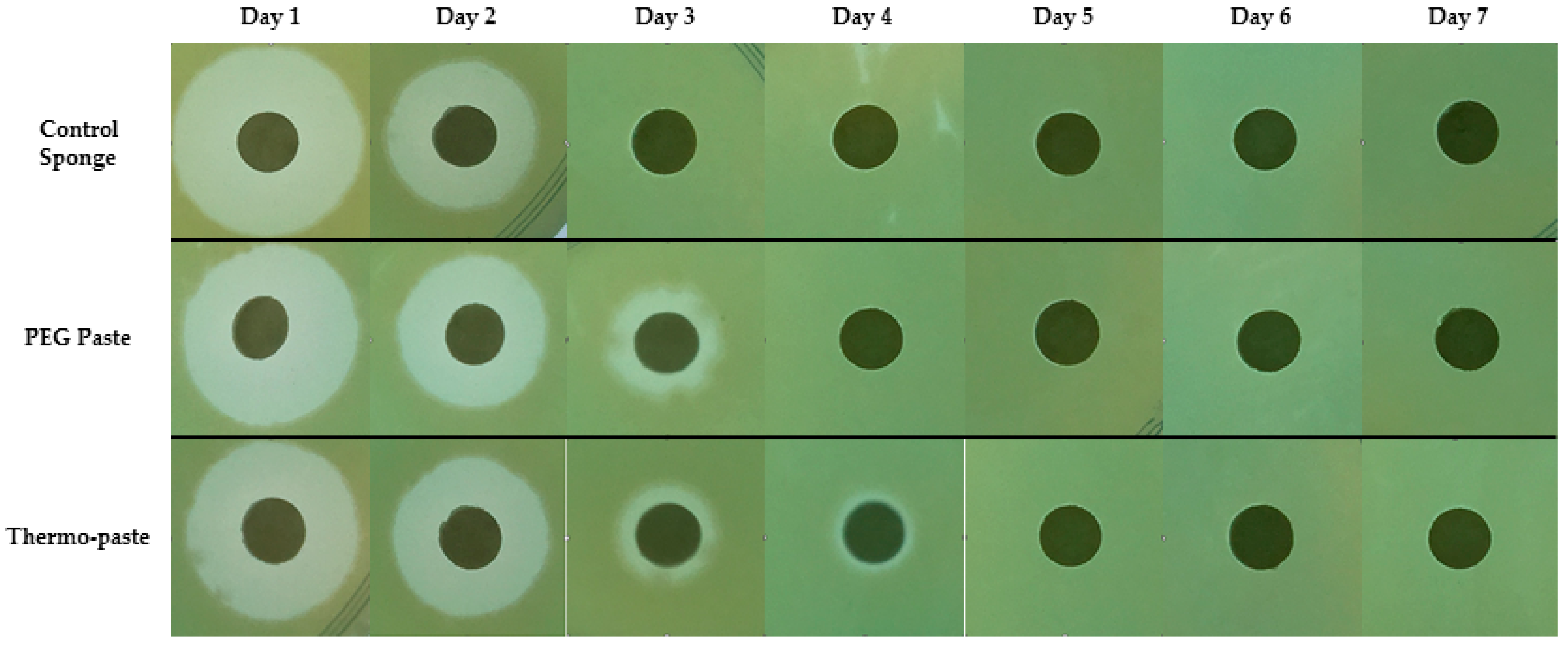
2.2. Antibiotic Elution and Activity
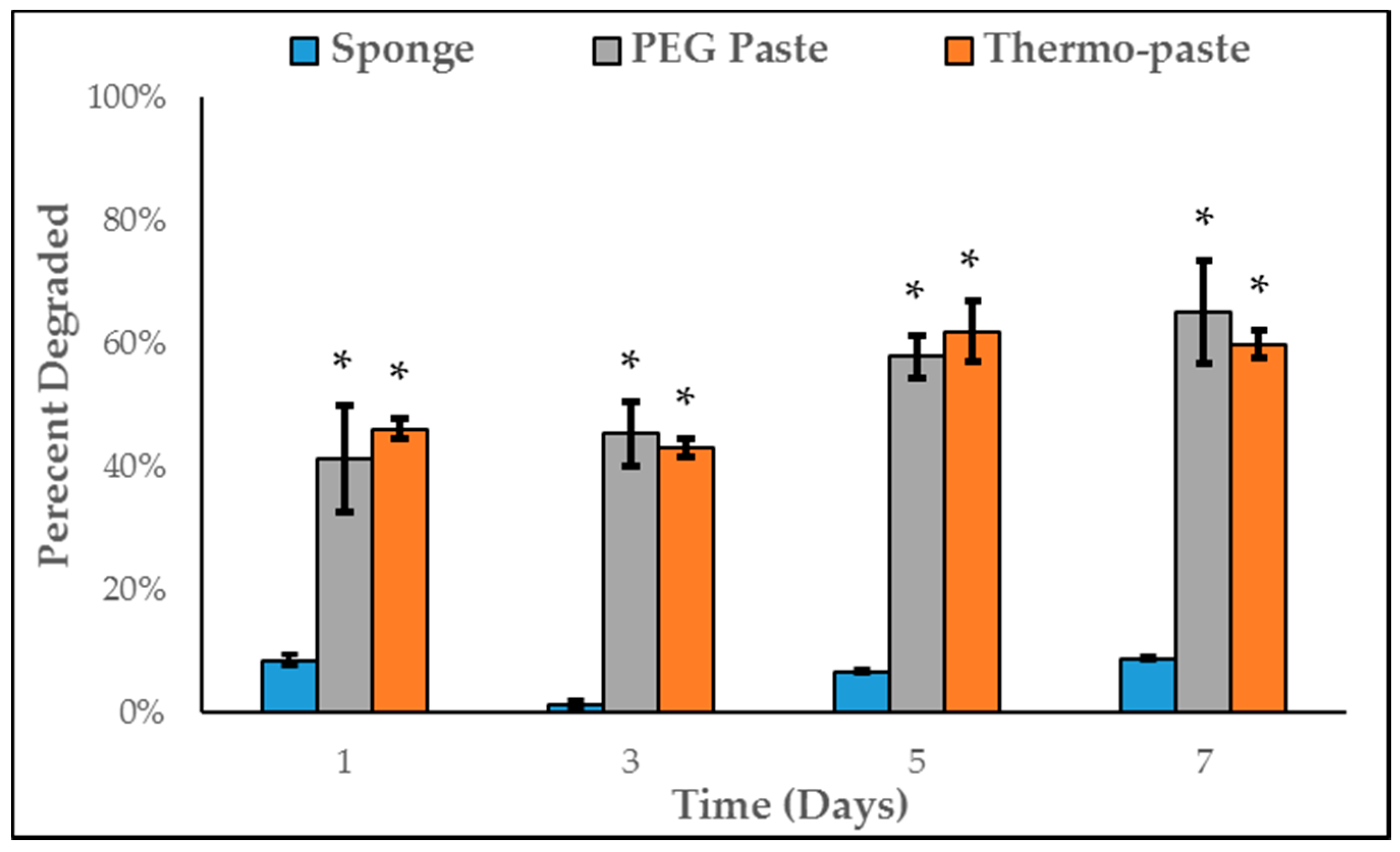
2.3. Degradation
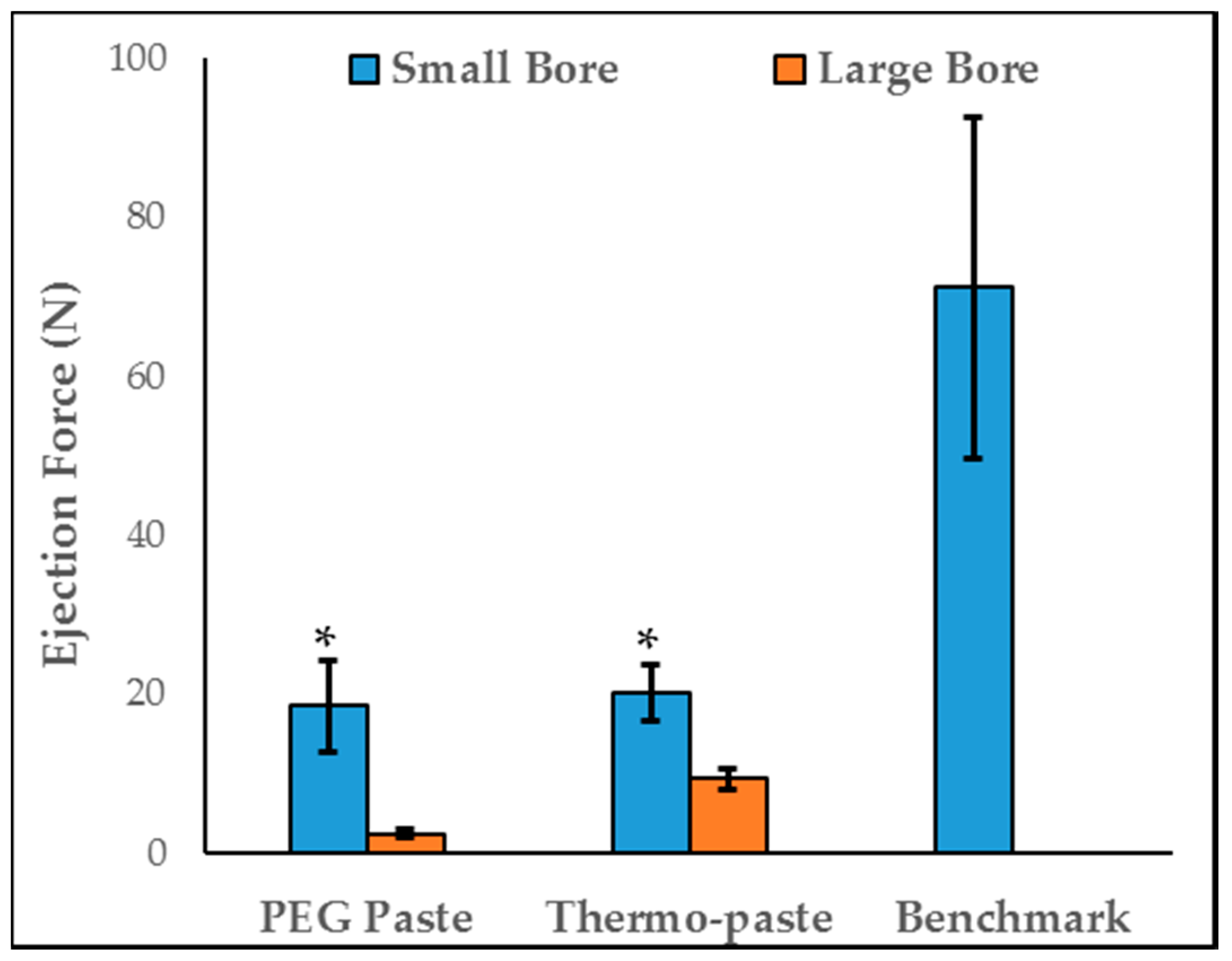
2.4. Injectability
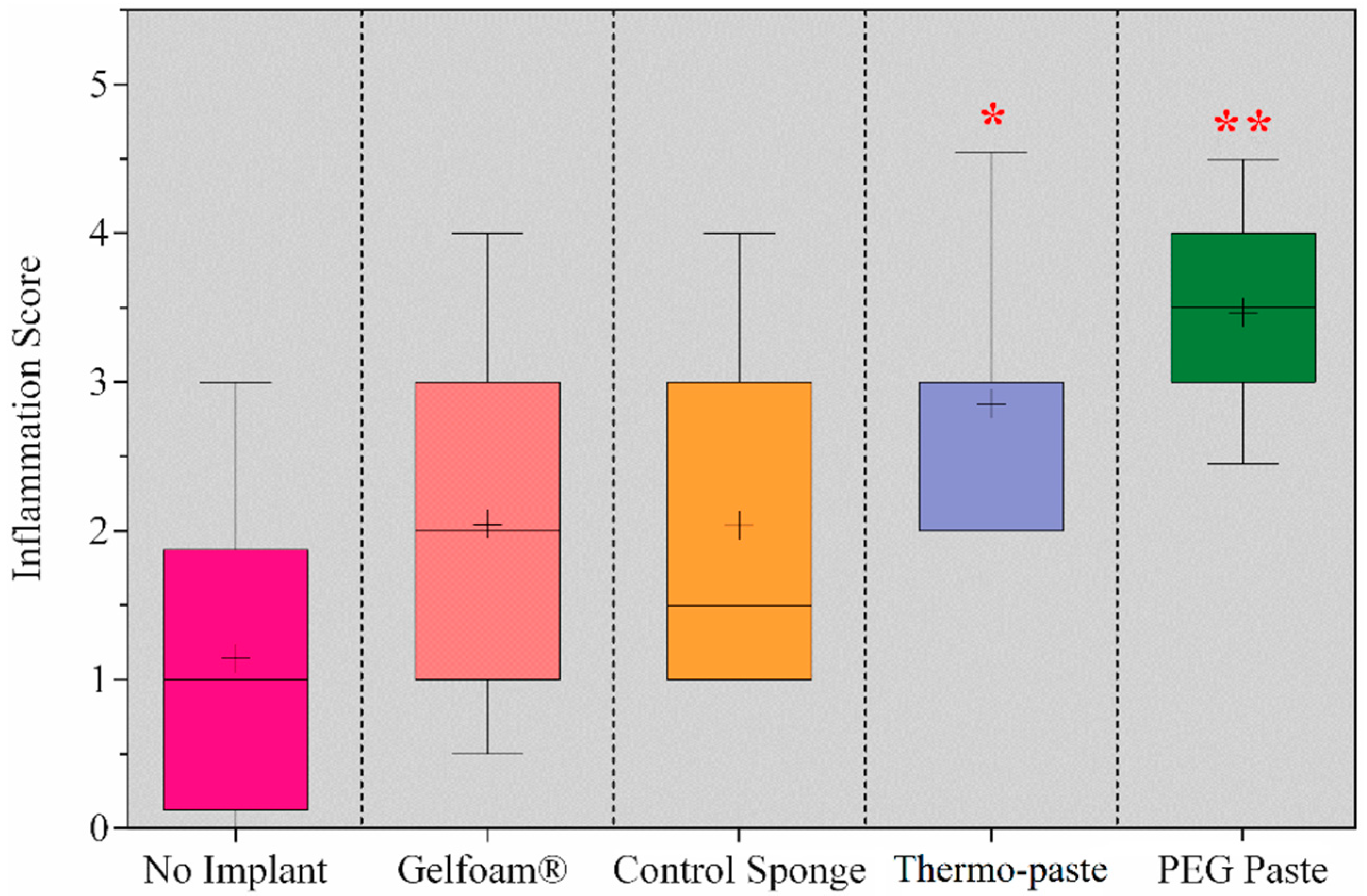
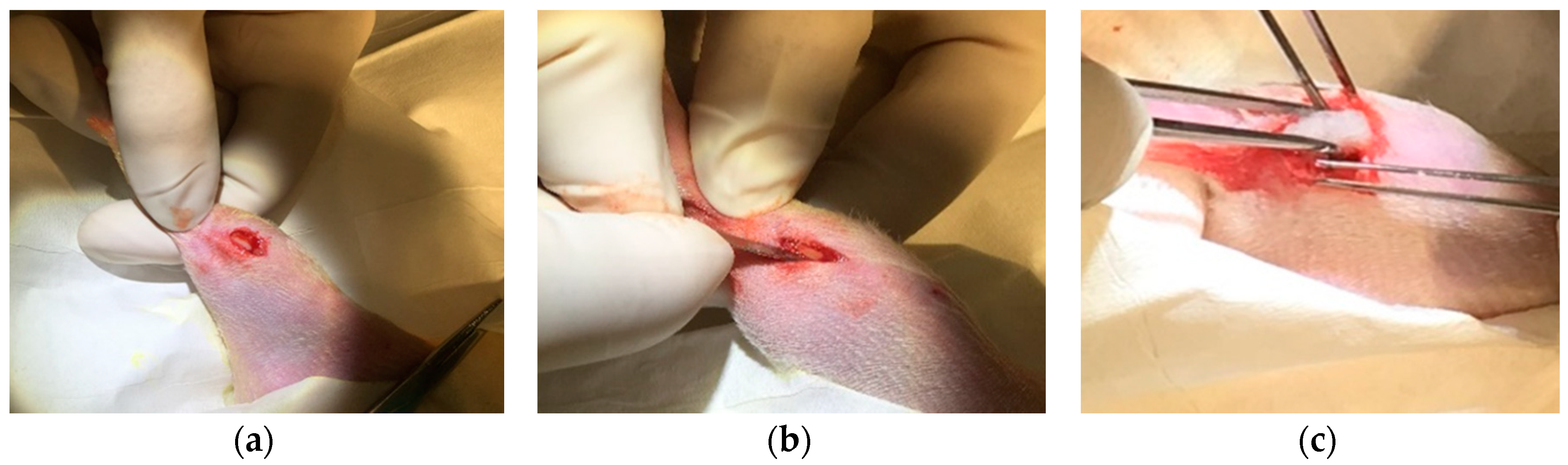
2.5. Preclinical, Functional Model of Biocompatibility
3. Discussion
4. Materials and Methods
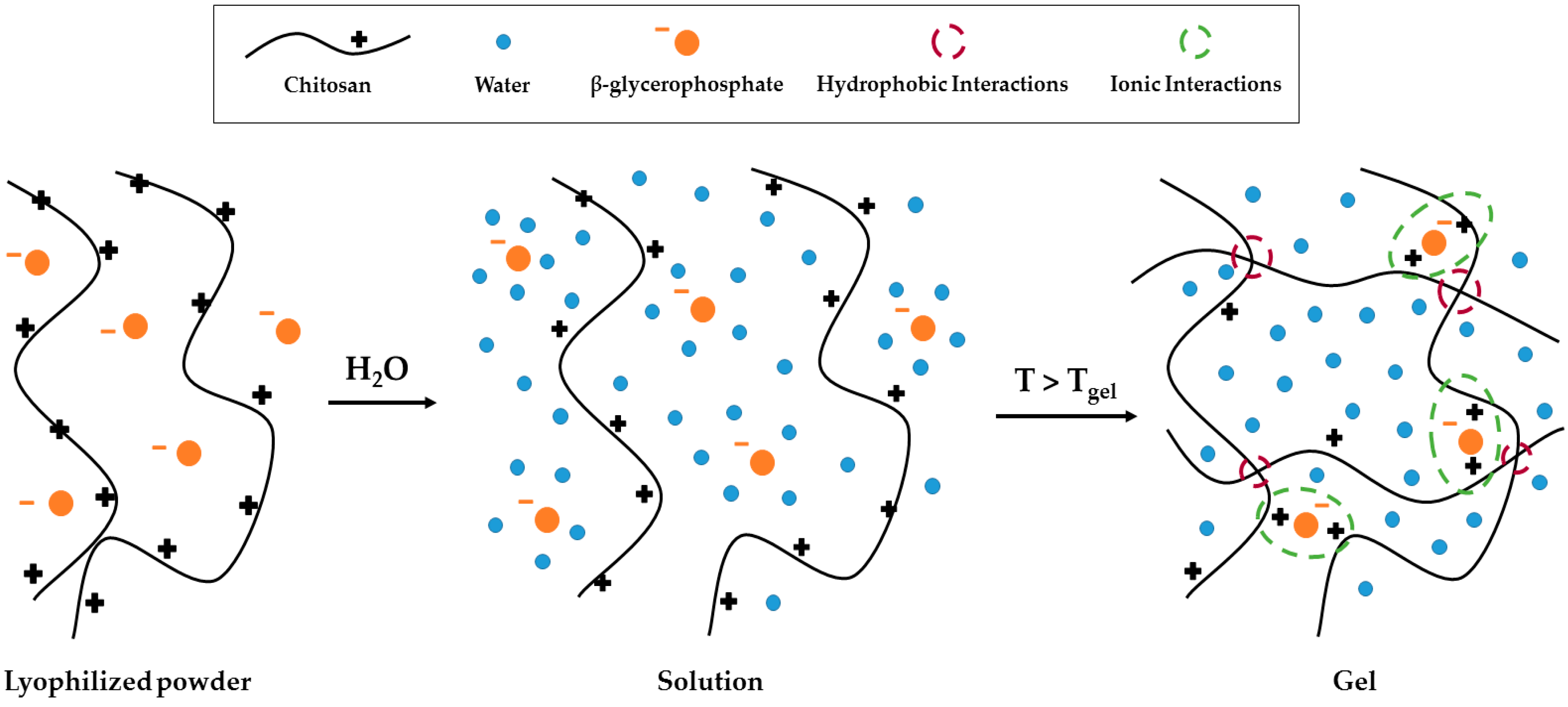
4.1. Fabrication
4.2. Cytocompatibility
4.3. Antibiotic Elution and Activity
4.4. Degradation
4.5. Injectability
4.6. Preclinical, Functional Model of Biocompatibility
4.7. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Park, H.; Copeland, C.; Henry, S.; Barbul, A. Complex wounds and their management. Surg. Clin. 2010, 90, 1181–1194. [Google Scholar] [CrossRef] [PubMed]
- Krug, E.G.; Sharma, G.K.; Lozano, R. The global burden of injuries. Am. J. Public Health 2000, 90, 523–526. [Google Scholar] [PubMed]
- Carver, D.C.; Kuehn, S.B.; Weinlein, J.C. Role of systemic and local antibiotics in the treatment of open fractures. Orthop. Clin. 2017, 48, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Halawi, M.J.; Morwood, M.P. Acute management of open fractures: An evidence-based review. Orthopedics 2015, 38, e1025–e1033. [Google Scholar] [CrossRef] [PubMed]
- Høiby, N.; Ciofu, O.; Johansen, H.K.; Song, Z.J.; Moser, C.; Jensen, P.Ø.; Molin, S.; Givskov, M.; Tolker-Nielsen, T.; Bjarnsholt, T. The clinical impact of bacterial biofilms. Int. J. Oral Sci. 2011, 3, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, W.V.; Shirtliff, M.E.; Stoodley, P. Bacterial biofilms and periprosthetic infections. J. Bone Jt. Surg. Am. 2013, 95, 2223–2229. [Google Scholar]
- Nana, A.; Nelson, S.B.; McLaren, A.; Chen, A.F. What’s new in musculoskeletal infection: Update on biofilms. J. Bone Jt. Surg. Am. 2016, 98, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Ter Boo, G.-J.A.; Grijpma, D.W.; Moriarty, T.F.; Richards, R.G.; Eglin, D. Antimicrobial delivery systems for local infection prophylaxis in orthopedic-and trauma surgery. Biomaterials 2015, 52, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Rinaudo, M. Chitin and chitosan: Properties and applications. Prog. Polym. Sci. 2006, 31, 603–632. [Google Scholar] [CrossRef]
- Inzana, J.A.; Schwarz, E.M.; Kates, S.L.; Awad, H.A. Biomaterials approaches to treating implant-associated osteomyelitis. Biomaterials 2016, 81, 58–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancienne, J.M.; Burrus, M.T.; Weiss, D.B.; Yarboro, S.R. Applications of local antibiotics in orthopedic trauma. Orthop. Clin. 2015, 46, 495–510. [Google Scholar] [CrossRef] [PubMed]
- Beuerlein, M.J.; McKee, M.D. Calcium sulfates: What is the evidence? J. Orthop. Trauma 2010, 24, S46–S51. [Google Scholar] [CrossRef] [PubMed]
- Younes, I.; Rinaudo, M. Chitin and chitosan preparation from marine sources. Structure, properties and applications. Mar. Drugs 2015, 13, 1133–1174. [Google Scholar] [CrossRef] [PubMed]
- VandeVord, P.J.; Matthew, H.W.; DeSilva, S.P.; Mayton, L.; Wu, B.; Wooley, P.H. Evaluation of the biocompatibility of a chitosan scaffold in mice. J. Biomed. Mater. Res. 2002, 59, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Dash, M.; Chiellini, F.; Ottenbrite, R.; Chiellini, E. Chitosan—A versatile semi-synthetic polymer in biomedical applications. Prog. Polym. Sci. 2011, 36, 981–1014. [Google Scholar] [CrossRef]
- McAvoy, K.; Jones, D.; Thakur, R.R.S. Synthesis and characterisation of photocrosslinked poly(ethylene glycol) diacrylate implants for sustained ocular drug delivery. Pharm. Res. 2018, 35, 36. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.C.; Beenken, K.E.; Jennings, J.A.; Hittle, L.; Shirtliff, M.E.; Bumgardner, J.D.; Smeltzer, M.S.; Haggard, W.O. Characterization of local delivery with amphotericin b and vancomycin from modified chitosan sponges and functional biofilm prevention evaluation. J. Orthop. Res. 2015, 33, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Noel, S.P.; Courtney, H.S.; Bumgardner, J.D.; Haggard, W.O. Chitosan sponges to locally deliver amikacin and vancomycin: A pilot in vitro evaluation. Clin. Orthop. Relat. Res. 2010, 468, 2074–2080. [Google Scholar] [CrossRef] [PubMed]
- Stinner, D.J.; Noel, S.P.; Haggard, W.O.; Watson, J.T.; Wenke, J.C. Local antibiotic delivery using tailorable chitosan sponges: The future of infection control? J. Orthop. Trauma 2010, 24, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, C.S.; Alexander, C.M.; Berretta, J.M.; Courtney, H.S.; Beenken, K.E.; Smeltzer, M.S.; Bumgardner, J.D.; Haggard, W.O.; Jennings, J.A. Evaluation of a chitosan-polyethylene glycol paste as a local antibiotic delivery device. World J. Orthop. 2017, 8, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Berretta, J.M.; Jennings, J.A.; Courtney, H.S.; Beenken, K.E.; Smeltzer, M.S.; Haggard, W.O. Blended chitosan paste for infection prevention: Preliminary and preclinical evaluations. Clin. Orthop. Relat. Res. 2017, 475, 1857–1870. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, R.; de Bruijn, J.D. Biocompatibility and gelation of chitosan–glycerol phosphate hydrogels. J. Biomed. Mater. Res. Part A 2008, 86, 824–832. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.Y.; Jiang, L.J.; Cao, P.P.; Li, J.B.; Chen, X.G. Glycerophosphate-based chitosan thermosensitive hydrogels and their biomedical applications. Carbohydr. Polym. 2015, 117, 524–536. [Google Scholar] [CrossRef] [PubMed]
- ISO E. 10993-5. Biological Evaluation of Medical Devices. Part 5: Tests for In Vitro Cytotoxicity; International Organization for Standardization: Geneva, Switzerland, 2009. [Google Scholar]
- Parker, A.C.; Rhodes, C.; Jennings, J.A.; Hittle, L.; Shirtliff, M.; Bumgardner, J.D.; Haggard, W.O. Preliminary evaluation of local drug delivery of amphotericin b and in vivo degradation of chitosan and polyethylene glycol blended sponges. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Hatch, D.; Wells, C.; Ahn, D.; Harris, M.; Jennings, J.; Haggard, W.; Armstrong, D. Characteristics and clinical assessment of antibiotic delivery by chitosan sponge in the high-risk diabetic foot: A case series. J. Wound Care 2017, 26, S32–S48. [Google Scholar] [CrossRef] [PubMed]
- Assaad, E.; Maire, M.; Lerouge, S. Injectable thermosensitive chitosan hydrogels with controlled gelation kinetics and enhanced mechanical resistance. Carbohydr. Polym. 2015, 130, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Jiang, G.; Sun, J.; Ding, F. PEG-g-chitosan thermosensitive hydrogel for implant drug delivery: Cytotoxicity, in vivo degradation and drug release. J. Biomater. Sci. Polym. Ed. 2014, 25, 241–256. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.T.; Hsiao, M.H.; Zhang, M.Y.; Levengood, S.L.; Zhang, M. Chitosan-peg hydrogel with sol–gel transition triggerable by multiple external stimuli. Macromol. Rapid Commun. 2015, 36, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Pakzad, Y.; Ganji, F. Thermosensitive hydrogel for periodontal application: In vitro drug release, antibacterial activity and toxicity evaluation. J. Biomater. Appl. 2016, 30, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Cheung, H.-Y.; Lau, K.-T.; Lu, T.-P.; Hui, D. A critical review on polymer-based bio-engineered materials for scaffold development. Compos. Part B Eng. 2007, 38, 291–300. [Google Scholar] [CrossRef]
- Zugravu, M.V.; Smith, R.A.; Reves, B.T.; Jennings, J.A.; Cooper, J.O.; Haggard, W.O.; Bumgardner, J.D. Physical properties and in vitro evaluation of collagen–chitosan–calcium phosphate microparticle-based scaffolds for bone tissue regeneration. J. Biomater. Appl. 2013, 28, 566–579. [Google Scholar] [CrossRef] [PubMed]
- Gorczyca, G.; Tylingo, R.; Szweda, P.; Augustin, E.; Sadowska, M.; Milewski, S. Preparation and characterization of genipin cross-linked porous chitosan–collagen–gelatin scaffolds using chitosan—CO2 solution. Carbohydr. Polym. 2014, 102, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Haka, A.S.; Grosheva, I.; Chiang, E.; Buxbaum, A.R.; Baird, B.A.; Pierini, L.M.; Maxfield, F.R. Macrophages create an acidic extracellular hydrolytic compartment to digest aggregated lipoproteins. Mol. Biol. Cell 2009, 20, 4932–4940. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, V.; Wilson, K.; Sonne, M.W.; Keir, P.J. Grip type alters maximal pinch forces in syringe use. Hum. Factors 2017, 59, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Heuzey, M.-C.; Bégin, A.; Carreau, P.J. Physical gelation of chitosan in the presence of β-glycerophosphate: The effect of temperature. Biomacromolecules 2005, 6, 3267–3275. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Liang, J.; Wen, Y.; Sun, X.; Li, T.; Zhang, G.; Sun, K.; Xu, X. In vitro and in vivo evaluation of chitosan/β-glycerol phosphate composite membrane for guided bone regeneration. J. Biomed. Mater. Res. Part A 2014, 102, 2911–2917. [Google Scholar] [CrossRef] [PubMed]
- Omar, M.A.; Ahmed, H.M.; Hammad, M.A.; Derayea, S.M. Validated spectrofluorimetric method for determination of selected aminoglycosides. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2015, 135, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Beenken, K.E.; Dunman, P.M.; McAleese, F.; Macapagal, D.; Murphy, E.; Projan, S.J.; Blevins, J.S.; Smeltzer, M.S. Global gene expression in Staphylococcus aureus biofilms. J. Bacteriol. 2004, 186, 4665–4684. [Google Scholar] [CrossRef] [PubMed]
- Masters, E.; Harris, M.; Jennings, J. Cis-2-decenoic acid interacts with bacterial cell membranes to potentiate additive and synergistic responses against biofilm. J. Bacteriol. Mycol. 2016, 3, 1031–1038. [Google Scholar]
- Knodell, R.G.; Ishak, K.G.; Black, W.C.; Chen, T.S.; Craig, R.; Kaplowitz, N.; Kiernan, T.W.; Wollman, J. Formulation and application of a numerical scoring system for assessing histological activity in asymptomatic chronic active hepatitis. Hepatology 1981, 1, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.C.; Jennings, J.A.; Bumgardner, J.D.; Courtney, H.S.; Lindner, E.; Haggard, W.O. Preliminary investigation of crosslinked chitosan sponges for tailorable drug delivery and infection control. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 110–123. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A. Staphylococcus aureus Zone of Inhibition Diameter (mm) | |||||||
|---|---|---|---|---|---|---|---|
| Group | Antibiotic Eluate Time Point (day) | ||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| 1. Control sponge | 11.6 | 7.1 | 2.9 | 0 | 0 | 0 | 0 |
| 2. PEG paste | 8.9 | 7.9 | 5.6 | 1.9 | 0 | 0 | 0 |
| 3. Thermo-paste | 10.9 | 6.8 | 4.2 | 0 | 0 | 0 | 0 |
| B. Pseudomonas aeruginosa Zone of Inhibition Diameter (mm) | |||||||
| 1. Control sponge | 12.7 | 8.2 | 0 | 0 | 0 | 0 | 0 |
| 2. PEG paste | 10.8 | 8.6 | 3.7 | 0 | 0 | 0 | 0 |
| 3. Thermo-paste | 12.1 | 9.6 | 2.8 | 1.5 | 0 | 0 | 0 |
| Experimental Group | Chitosan (w/v) | Acetic Acid (v/v) | Additive (w/v) | pH | |
|---|---|---|---|---|---|
| 1. Control Chitosan | 1% | 1% | - | neutral | |
| 2. PEG Paste | 1% | 0.85% | 0.5% PEG | acidic | |
| 3. Thermo-paste | 50% | 1% | 1% | - | neutral |
| 50% | 2% | 0.5% | 10% β-GP | acidic | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boles, L.; Alexander, C.; Pace, L.; Haggard, W.; Bumgardner, J.; Jennings, J. Development and Evaluation of an Injectable Chitosan/β-Glycerophosphate Paste as a Local Antibiotic Delivery System for Trauma Care. J. Funct. Biomater. 2018, 9, 56. https://doi.org/10.3390/jfb9040056
Boles L, Alexander C, Pace L, Haggard W, Bumgardner J, Jennings J. Development and Evaluation of an Injectable Chitosan/β-Glycerophosphate Paste as a Local Antibiotic Delivery System for Trauma Care. Journal of Functional Biomaterials. 2018; 9(4):56. https://doi.org/10.3390/jfb9040056
Chicago/Turabian StyleBoles, Logan, Christopher Alexander, Leslie Pace, Warren Haggard, Joel Bumgardner, and Jessica Jennings. 2018. "Development and Evaluation of an Injectable Chitosan/β-Glycerophosphate Paste as a Local Antibiotic Delivery System for Trauma Care" Journal of Functional Biomaterials 9, no. 4: 56. https://doi.org/10.3390/jfb9040056
APA StyleBoles, L., Alexander, C., Pace, L., Haggard, W., Bumgardner, J., & Jennings, J. (2018). Development and Evaluation of an Injectable Chitosan/β-Glycerophosphate Paste as a Local Antibiotic Delivery System for Trauma Care. Journal of Functional Biomaterials, 9(4), 56. https://doi.org/10.3390/jfb9040056