
Clot Imaging Using Photostable Nanodiamond

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of FND
2.2. Blood Collection and Clot Formation
2.3. Microscopy
3. Results
3.1. Macroscopic Appearance of Clot and Composition
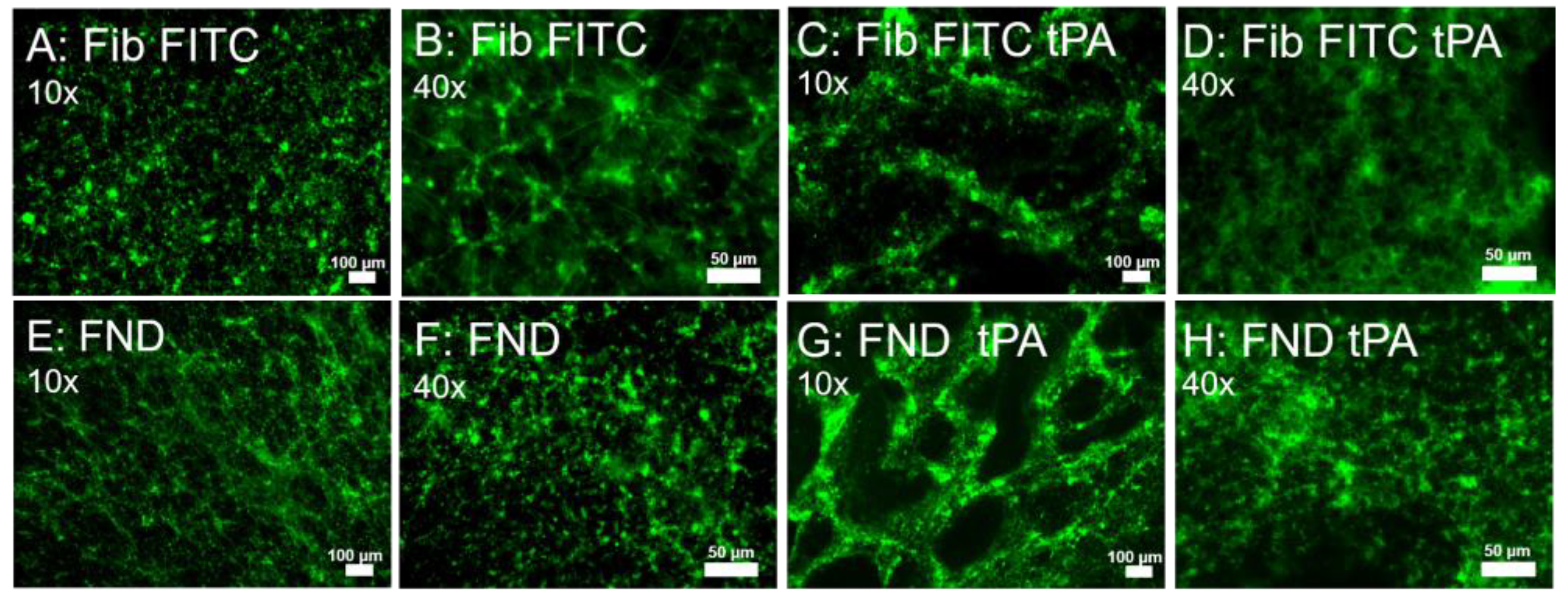
3.2. FND Labeling Is Comparable to Standard Fluorescent Labeling for Imaging Clots
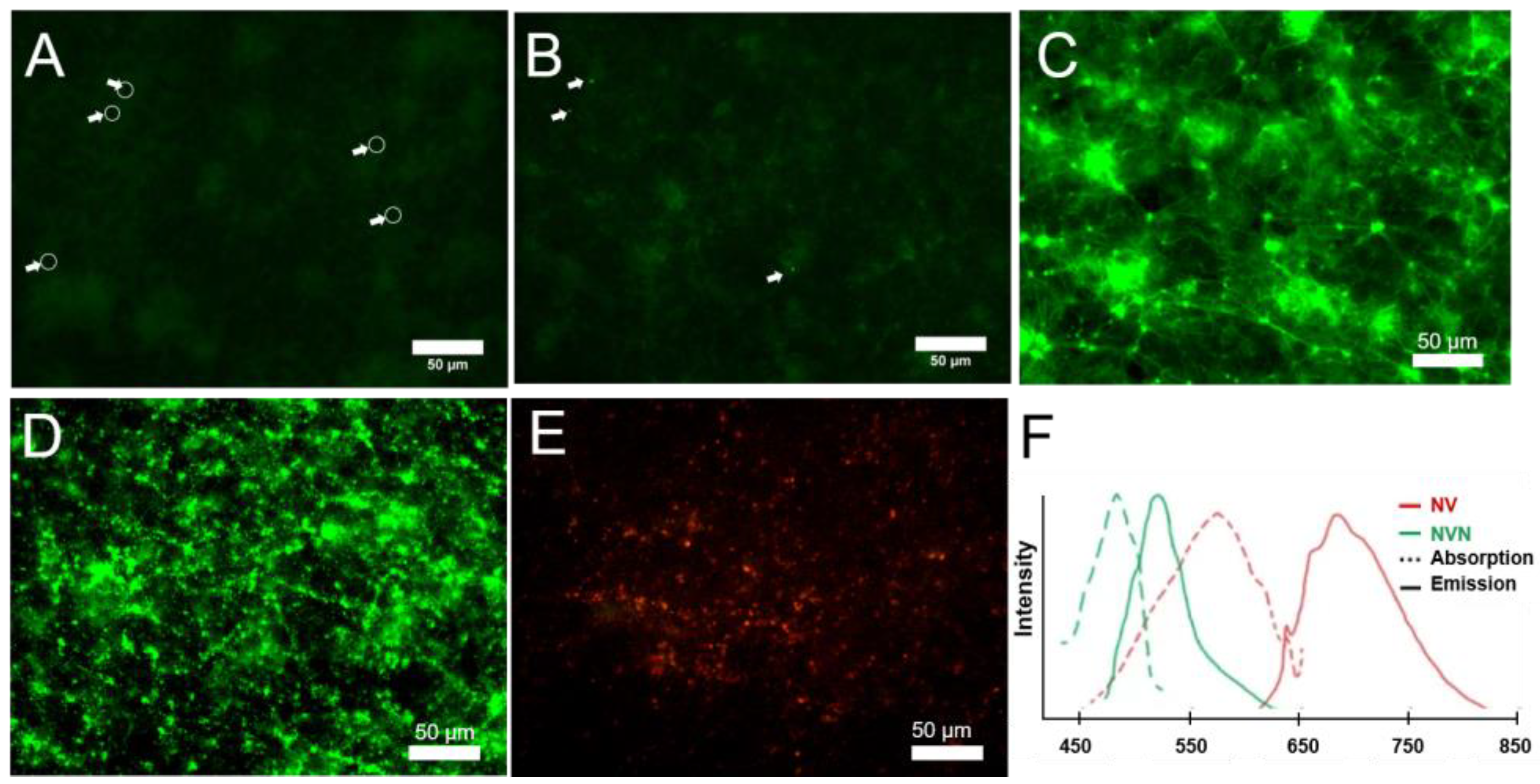
3.3. Comparison of Particle Size for Labeling: 60 nm vs. 120 nm
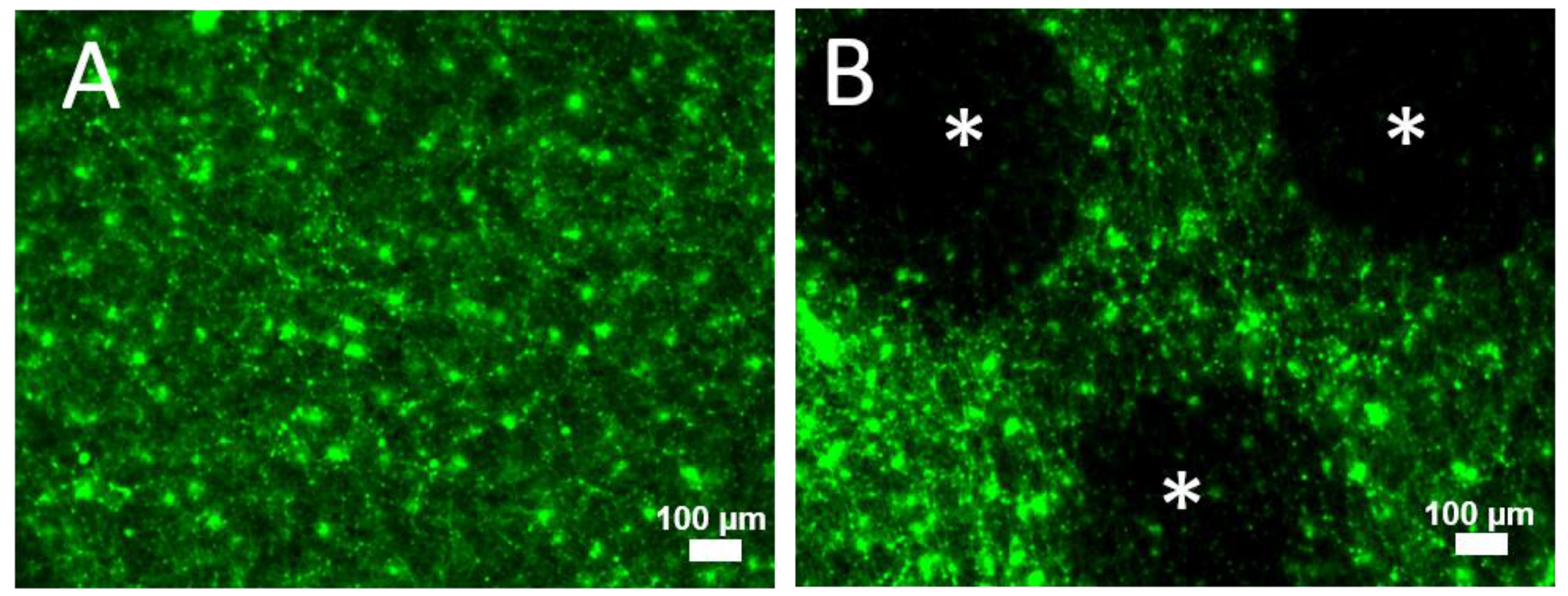
3.4. FND Bound to Fibrinogen Demonstrate Changes in Clot Exposed to tPA
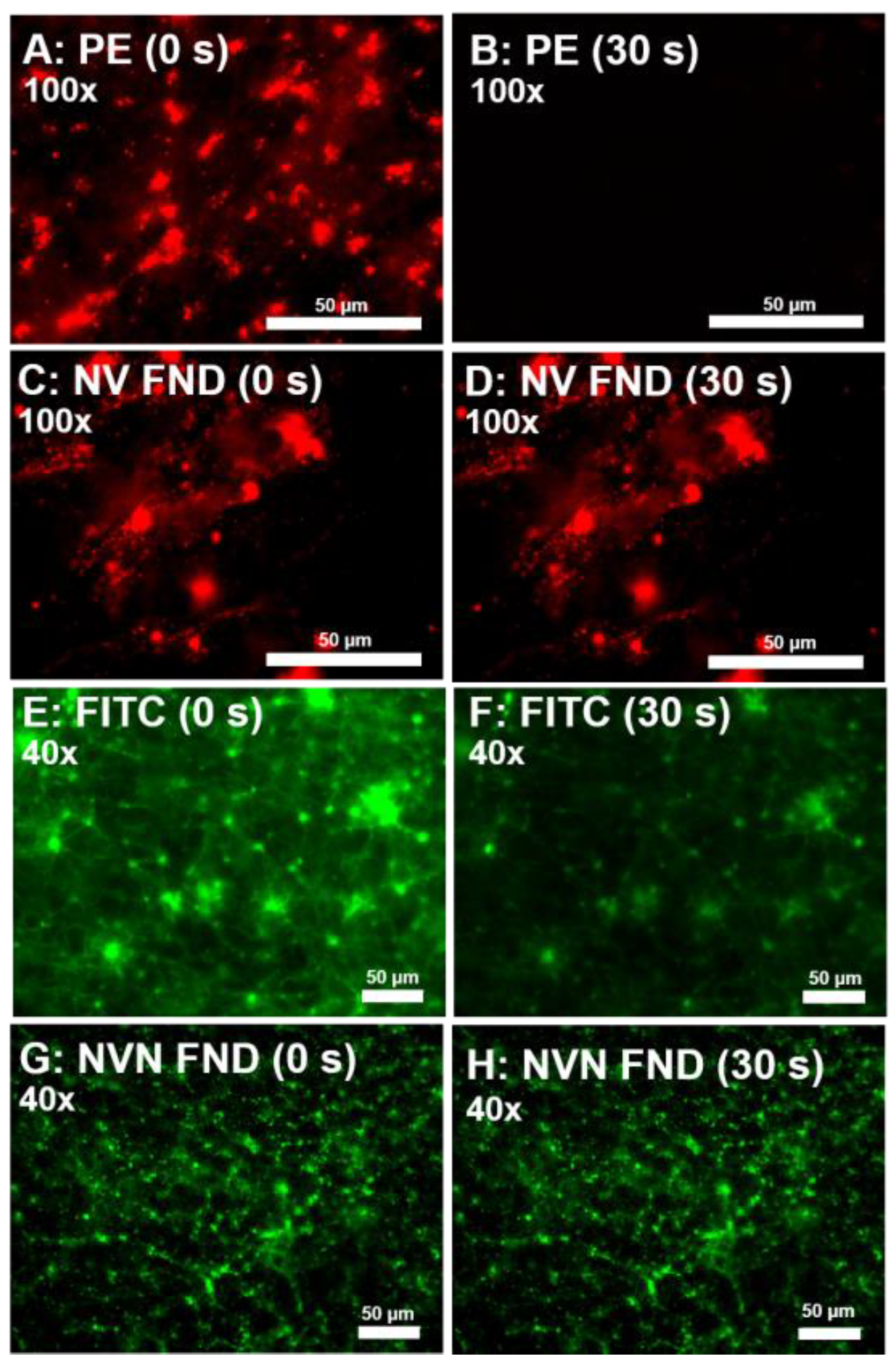
3.5. FND Eliminates Photobleaching Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beckman, M.G.; Hooper, W.C.; Critchley, S.E.; Ortel, T.L. Venous thromboembolism: A public health concern. Am. J. Prev. Med. 2010, 38 (Suppl. 4), S495–S501. [Google Scholar] [CrossRef] [PubMed]
- Pitts, S.R.N.R.; Xu, J.; Burt, C.W. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl. Health Stat. Rep. 2008, 7, 1–40. [Google Scholar]
- Prandoni, P.; Lensing, A.W.; Prins, M.H.; Pesavento, R.; Piccioli, A.; Sartori, M.T.; Tormene, D.; Milan, M.; Vedovetto, V.; Noventa, F.; et al. The impact of residual thrombosis on the long-term outcome of patients with deep venous thrombosis treated with conventional anticoagulation. Semin. Thromb. Hemost. 2015, 41, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C. Natural history of venous thromboembolism. Circulation 2003, 107, I22–I30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Gu, J.P.; Shi, H.F.; Shi, W.Y.; Lu, J.Y.; Chen, L.; Su, H.B. Assessment of the Probability of Post-thrombotic Syndrome in Patients with Lower Extremity Deep Venous Thrombosis. Sci. Rep. 2018, 8, 12663. [Google Scholar] [CrossRef] [Green Version]
- Rabinovich, A.; Kahn, S.R. The postthrombotic syndrome: Current evidence and future challenges. J. Thromb. Haemost. 2017, 15, 230–241. [Google Scholar] [CrossRef] [Green Version]
- Pengo, V.; Lensing, A.W.; Prins, M.H.; Marchiori, A.; Davidson, B.L.; Tiozzo, F.; Albanese, P.; Biasiolo, A.; Pegoraro, C.; Iliceto, S.; et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N. Engl. J. Med. 2004, 350, 2257–2264. [Google Scholar] [CrossRef] [Green Version]
- Kantake, M.; Tanabe, N.; Sugiura, T.; Shigeta, A.; Yanagawa, N.; Jujo, T.; Kawata, N.; Amano, H.; Matsuura, Y.; Nishimura, R.; et al. Association of deep vein thrombosis type with clinical phenotype of chronic thromboembolic pulmonary hypertension. Int. J. Cardiol. 2013, 165, 474–477. [Google Scholar] [CrossRef]
- Korkmaz, A.; Ozlu, T.; Ozsu, S.; Kazaz, Z.; Bulbul, Y. Long-term outcomes in acute pulmonary thromboembolism: The incidence of chronic thromboembolic pulmonary hypertension and associated risk factors. Clin. Appl. Thromb. Hemost. 2012, 18, 281–288. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Jaffer, F.A. High-Resolution Molecular Imaging Via Intravital Microscopy: Illuminating Vascular Biology In Vivo. Integr. Biol. Quant. Biosci. Nano Macro 2013, 5, 278–290. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Peter, K. Molecular Imaging of Atherothrombotic DiseasesHighlights: Seeing Is Believing. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1029–1040. [Google Scholar] [CrossRef] [Green Version]
- Falati, S.; Gross, P.; Merrill-Skoloff, G.; Furie, B.C.; Furie, B. Real-time in vivo imaging of platelets, tissue factor and fibrin during arterial thrombus formation in the mouse. Nat. Med. 2002, 8, 1175. [Google Scholar] [CrossRef]
- Furie, B.; Furie, B. In vivo thrombus formation. J. Thromb. Haemost. 2007, 5, 12–17. [Google Scholar] [CrossRef]
- Reineck, P.; Francis, A.; Orth, A.; Lau, D.W.M.; Nixon-Luke, R.D.V.; Rastogi, I.D.; Razali, W.A.W.; Cordina, N.M.; Parker, L.M.; Sreenivasan, V.K.A.; et al. Brightness and Photostability of Emerging Red and Near-IR Fluorescent Nanomaterials for Bioimaging. Adv. Opt. Mater. 2016, 4, 1549–1557. [Google Scholar] [CrossRef]
- Boisset, J.-C.; Andrieu-Soler, C.; Van Cappellen, W.A.; Clapes, T.; Robin, C. Ex vivo time-lapse confocal imaging of the mouse embryo aorta. Nat. Protoc. 2011, 6, 1792. [Google Scholar] [CrossRef]
- Tajiri, K.; Kishi, H.; Ozawa, T.; Sugiyama, T.; Muraguchi, A. SFMAC: A novel method for analyzing multiple parameters on lymphocytes with a single fluorophore in cell-microarray system. Cytom. Part A J. Int. Soc. Adv. Cytom. 2009, 75, 282–288. [Google Scholar] [CrossRef]
- Zaitsev, A.M. Optical Properties of Diamond: A Data Handbook; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 2001; 502p. [Google Scholar]
- Marcinkiewicz, C.; Gerstenhaber, J.A.; Sternberg, M.; Lelkes, P.I.; Feuerstein, G. Bitistatin-functionalized fluorescent nanodiamond particles specifically bind to purified human platelet integrin receptor αIIbβ3 and activated platelets. Int. J. Nanomed. 2017, 12, 3711. [Google Scholar] [CrossRef] [Green Version]
- Gerstenhaber, J.A.; Barone, F.C.; Marcinkiewicz, C.; Li, J.; Shiloh, A.O.; Sternberg, M.; Lelkes, P.I.; Feuerstein, G. Vascular thrombus imaging in vivo via near-infrared fluorescent nanodiamond particles bioengineered with the disintegrin bitistatin (Part II). Int. J. Nanomed. 2017, 12, 8471. [Google Scholar] [CrossRef] [Green Version]
- Dei Cas, L.; Zeldin, S.; Nunn, N.; Torelli, M.; Shames, A.I.; Zaitsev, A.M.; Shenderova, O. From Fancy Blue to Red: Controlled Production of a Vibrant Color Spectrum of Fluorescent Diamond Particles. Adv. Funct. Mater. 2019, 29, 1808362. [Google Scholar] [CrossRef]
- Nunn, N.; Prabhakar, N.; Reineck, P.; Magidson, V.; Kamiya, E.; Heinz, W.F.; Torelli, M.D.; Rosenholm, J.; Zaitsev, A.; Shenderova, O. Brilliant blue, green, yellow, and red fluorescent diamond particles: Synthesis, characterization, and multiplex imaging demonstrations. Nanoscale 2019, 11, 11584–11595. [Google Scholar] [CrossRef]
- Shenderova, O.A.; Shames, A.I.; Nunn, N.A.; Torelli, M.D.; Vlasov, I.; Zaitsev, A. Synthesis, properties, and applications of fluorescent diamond particles. J. Vac. Sci. Technol. B 2019, 37, 030802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermanson, G.T. Bioconjugate Techniques; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pretorius, E.; Swanepoel, A.C.; DeVilliers, S.; Bester, J. Blood clot parameters: Thromboelastography and scanning electron microscopy in research and clinical practice. Thromb. Res. 2017, 154, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, S.; Saxena, R.K. Age-dependent increase in green autofluorescence of blood erythrocytes. J. Biosci. 2007, 32, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Croce, A.C.; Ferrigno, A.; Bottiroli, G.; Vairetti, M. Autofluorescence-based optical biopsy: An effective diagnostic tool in hepatology. Liver Int. 2018, 38, 1160–1174. [Google Scholar] [CrossRef] [Green Version]
- Zamolodchikov, D.; Strickland, S. Aβ delays fibrin clot lysis by altering fibrin structure and attenuating plasminogen binding to fibrin. Blood 2012, 119, 3342–3351. [Google Scholar] [CrossRef] [Green Version]
- Van Sark, W.G.; Frederix, P.L.; Van den Heuvel, D.J.; Gerritsen, H.C.; Bol, A.A.; Van Lingen, J.N.; de Mello Donega, C.; Meijerink, A. Photooxidation and photobleaching of single CdSe/ZnS quantum dots probed by room-temperature time-resolved spectroscopy. J. Phys. Chem. B 2001, 105, 8281–8284. [Google Scholar] [CrossRef] [Green Version]
- Chashchikhin, O.; Budyka, M. Photoactivation, photobleaching and photoetching of CdS quantum dots− Role of oxygen and solvent. J. Photochem. Photobiol. A Chem. 2017, 343, 72–76. [Google Scholar] [CrossRef]
- Vaijayanthimala, V.; Cheng, P.-Y.; Yeh, S.-H.; Liu, K.-K.; Hsiao, C.-H.; Chao, J.-I.; Chang, H.-C. The long-term stability and biocompatibility of fluorescent nanodiamond as an in vivo contrast agent. Biomaterials 2012, 33, 7794–7802. [Google Scholar] [CrossRef]
- Faklaris, O.; Joshi, V.; Irinopoulou, T.; Tauc, P.; Sennour, M.; Girard, H.; Gesset, C.; Arnault, J.-C.; Thorel, A.; Boudou, J.-P. Photoluminescent diamond nanoparticles for cell labeling: Study of the uptake mechanism in mammalian cells. ACS Nano 2009, 3, 3955–3962. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.-J.; Kang, M.-W.; Chang, H.-C.; Chen, K.-M.; Yu, Y.-C. Bright fluorescent nanodiamonds: No photobleaching and low cytotoxicity. J. Am. Chem. Soc. 2005, 127, 17604–17605. [Google Scholar] [CrossRef]
- Tsoi, K.M.; Dai, Q.; Alman, B.A.; Chan, W.C. Are quantum dots toxic? Exploring the discrepancy between cell culture and animal studies. Acc. Chem. Res. 2013, 46, 662–671. [Google Scholar] [CrossRef]
- Pelley, J.L.; Daar, A.S.; Saner, M.A. State of academic knowledge on toxicity and biological fate of quantum dots. Toxicol. Sci. 2009, 112, 276–296. [Google Scholar] [CrossRef] [Green Version]
- Hardman, R. A toxicologic review of quantum dots: Toxicity depends on physicochemical and environmental factors. Environ. Health Perspect. 2006, 114, 165–172. [Google Scholar] [CrossRef]
- Schrand, A.M.; Hens, S.A.; Shenderova, O.A. Nanodiamond Particles: Properties and Perspectives for Bioapplications. Crit. Rev. Solid State Mater. Sci. 2009, 34, 18–74. [Google Scholar] [CrossRef]
- Yeromonahos, C.; Polack, B.; Caton, F. Nanostructure of the fibrin clot. Biophys. J. 2010, 99, 2018–2027. [Google Scholar] [CrossRef] [Green Version]
- Deatrick, K.B.; Luke, C.E.; Elfline, M.A.; Sood, V.; Baldwin, J.; Upchurch, G.R., Jr.; Jaffer, F.A.; Wakefield, T.W.; Henke, P.K. The effect of matrix metalloproteinase 2 and matrix metalloproteinase 2/9 deletion in experimental post-thrombotic vein wall remodeling. J. Vasc. Surg. 2013, 58, 1375–1384.e1372. [Google Scholar] [CrossRef] [Green Version]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francis, S.J.; Torelli, M.D.; Nunn, N.A.; Arepally, G.M.; Shenderova, O.A. Clot Imaging Using Photostable Nanodiamond. Nanomaterials 2023, 13, 961. https://doi.org/10.3390/nano13060961
Francis SJ, Torelli MD, Nunn NA, Arepally GM, Shenderova OA. Clot Imaging Using Photostable Nanodiamond. Nanomaterials. 2023; 13(6):961. https://doi.org/10.3390/nano13060961
Chicago/Turabian StyleFrancis, Samuel J., Marco D. Torelli, Nicholas A. Nunn, Gowthami M. Arepally, and Olga A. Shenderova. 2023. "Clot Imaging Using Photostable Nanodiamond" Nanomaterials 13, no. 6: 961. https://doi.org/10.3390/nano13060961
APA StyleFrancis, S. J., Torelli, M. D., Nunn, N. A., Arepally, G. M., & Shenderova, O. A. (2023). Clot Imaging Using Photostable Nanodiamond. Nanomaterials, 13(6), 961. https://doi.org/10.3390/nano13060961