Deep Airway Inflammation and Respiratory Disorders in Nanocomposite Workers

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Workplace Processes
2.2. Workplace Aerosol Measurements
2.3. Subjects
2.4. Collection and Analysis of Inflammation Markers in EBC
2.5. Statistical Analysis
3. Results
3.1. Workplace Aerosol Measurements
3.2. Subjects Characteristics
3.3. Respiratory Disease/Symptoms
3.4. Spirometry
3.5. FeNO
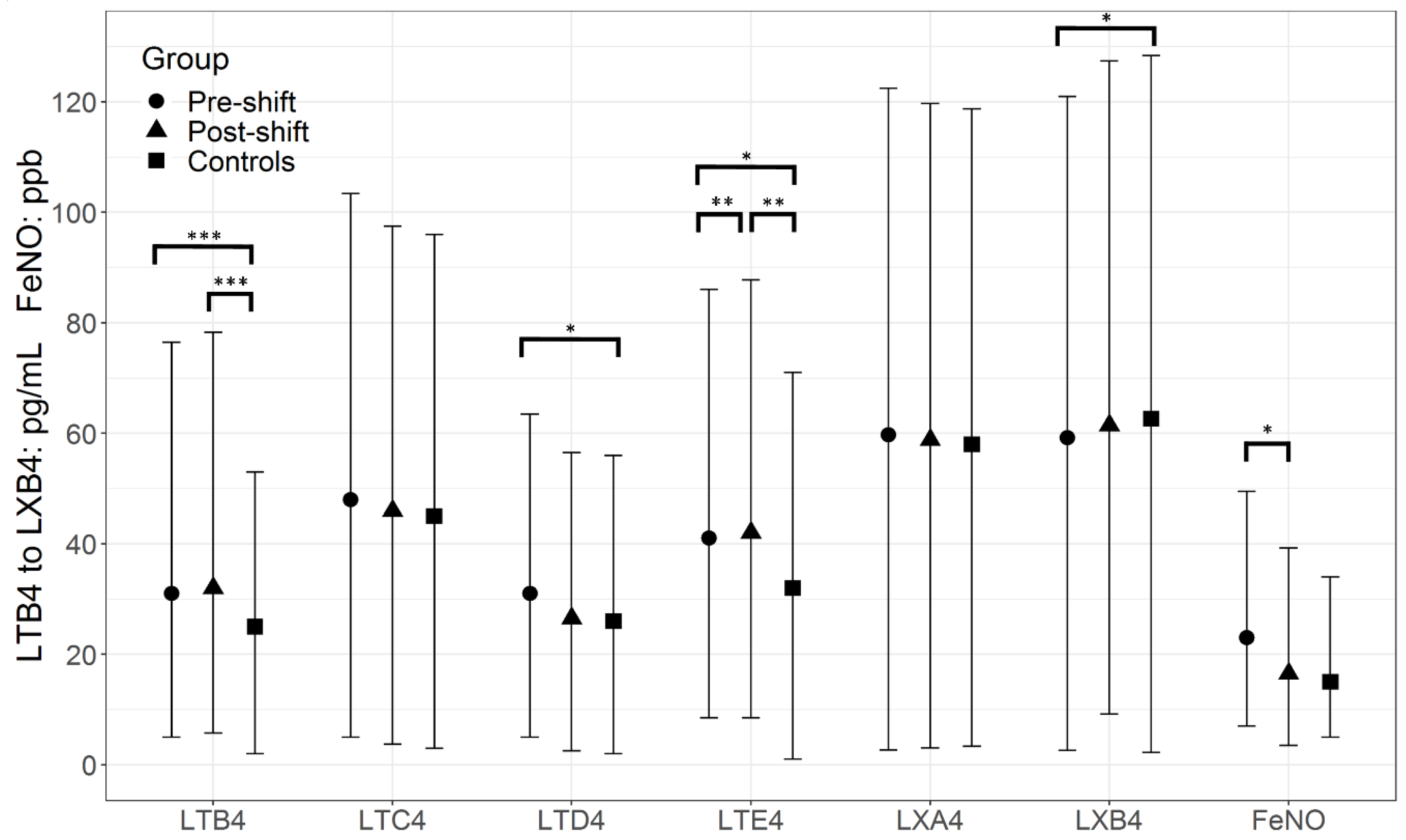
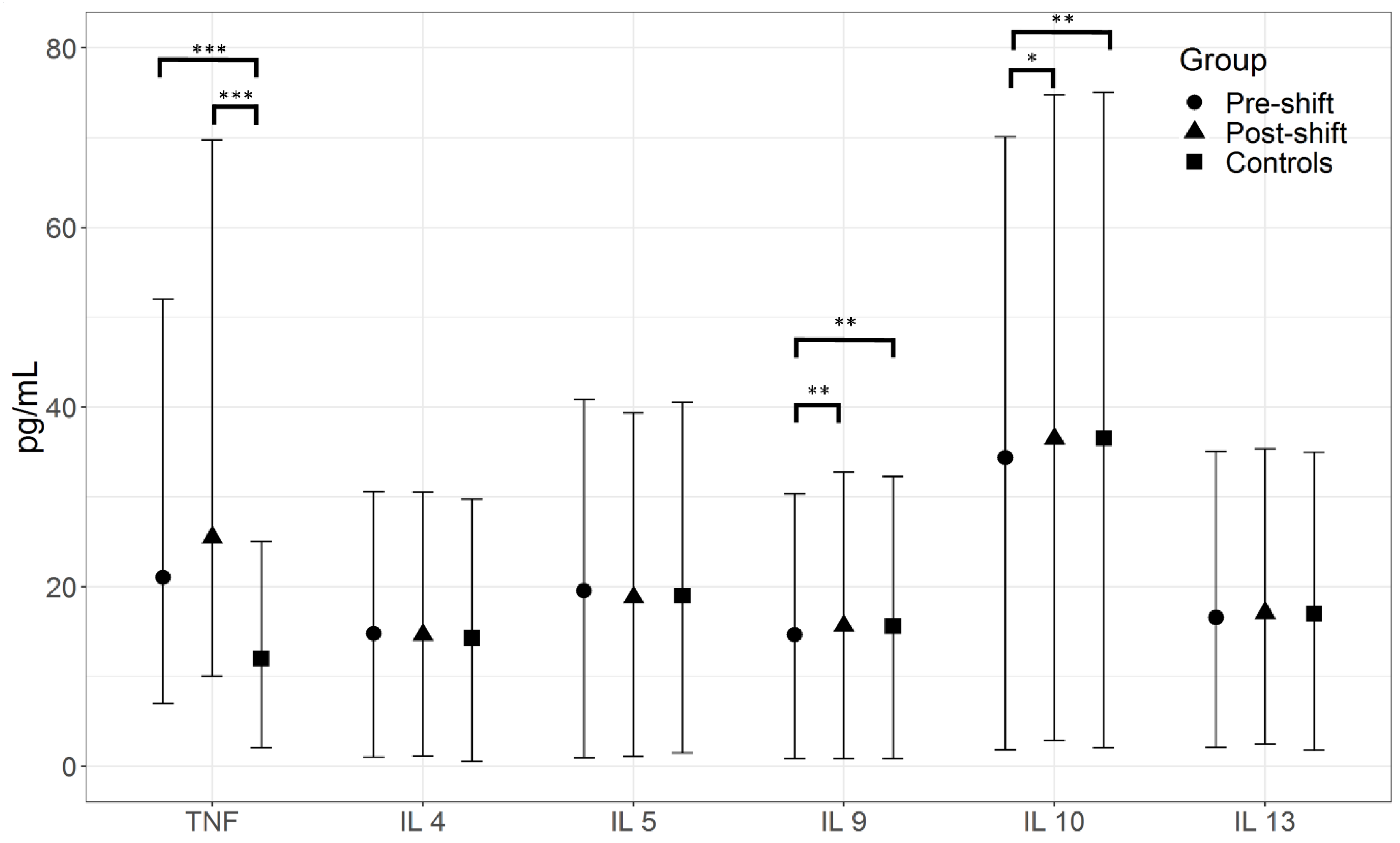
3.6. Markers in EBC
3.7. Multiple Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gomez, V.; Levin, M.; Saber, A.T.; Irusta, S.; Dal Maso, M.; Hanoi, R.; Santamaria, J.; Jensen, K.A.; Wallin, H.; Koponen, I.K. Comparison of dust release from epoxy and paint nanocomposites and conventional products during sanding and sawing. Ann. Occup. Hyg. 2014, 58, 983–994. [Google Scholar] [CrossRef] [PubMed]
- Liou, S.H.; Tsai, C.S.; Pelclova, D.; Schubauer-Berigan, M.K.; Schulte, P.A. Assessing the first wave of epidemiological studies of nanomaterial workers. J. Nanopart. Res. 2015, 17, 413. [Google Scholar] [CrossRef] [PubMed]
- Iavicoli, I.; Leso, V.; Schulte, P.A. Biomarkers of susceptibility. State of the art and implications for occupational exposure to engineered nanomaterials. Toxicol. Appl. Pharmacol. 2016, 299, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Liou, S.H.; Wu, W.T.; Liao, H.Y.; Chen, C.Y.; Tsai, C.Y.; Jung, W.T.; Lee, H.L. Global DNA methylation and oxidative stress biomarkers in workers exposed to metal oxide nanoparticles. J. Hazard. Mater. 2017, 331, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Guseva Canu, I.; Schulte, P.A.; Riediker, M.; Fatkhutdinova, L.; Bergamaschi, E. Methodological, political and legal issues in the assessment of the effects of nanotechnology on human health. J. Epidemiol. Community Health 2018, 72, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Bradna, P.; Ondrackova, L.; Zdimal, V.; Navratil, T.; Pelclova, D. Detection of nanoparticles released at finishing of dental composite materials. Monatsh. Chem. 2017, 148, 531–537. [Google Scholar] [CrossRef]
- Schulte, P.A.; Iavicoli, I.; Rantanen, J.H.; Dahmann, D.; Iavicoli, S.; Pipke, R.; Guseva Canu, I.; Boccuni, F.; Ricci, M.; Polci, M.L.; et al. Assessing the protection of the nanomaterial workforce. Nanotoxicology 2016, 10, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Kurjane, N.; Zvagule, T.; Reste, J.; Martinsone, Z.; Pavlovska, I.; Martinsone, I.; Vanadzins, I. The effect of different workplace nanoparticles on the immune systems of employees. J. Nanopart. Res. 2017, 19, 320. [Google Scholar] [CrossRef] [PubMed]
- Liou, S.H.; Tsou, T.C.; Wang, S.L.; Li, L.A.; Chiang, H.C.; Li, W.F.; Lai, H.Y.; Lee, H.L.; Lin, M.H.; Hsu, J.H.; et al. Epidemiological study of health hazards among workers handling engineered nanomaterials. J. Nanopart. Res. 2012, 14, 878. [Google Scholar] [CrossRef]
- Liao, H.Y.; Chung, Y.T.; Lai, C.H.; Wang, S.L.; Chiang, H.C.; Li, L.A.; Tsou, T.C.; Li, W.F.; Lee, H.L.; Wu, W.T.; Lin, M.H.; et al. Six-month follow-up study of health markers of nanomaterials among workers handling engineered nanomaterials. Nanotoxicology 2014, 8 (Suppl. 1), 100–110. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Zdimal, V.; Kacer, P.; Fenclova, Z.; Vlckova, S.; Komarc, M.; Navratil, T.; Schwarz, J.; Zikova, N.; Makes, O.; et al. Leukotrienes in exhaled breath condensate and fractional exhaled nitric oxide in workers exposed to TiO2 nanoparticles. J. Breath Res. 2016, 10, 036004. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Choi, Y.C.; Shin, J.H.; Lee, J.H.; Lee, Y.; Park, S.Y.; Baek, J.E.; Park, J.D.; Ahn, K.; Yu, I.J. Health surveillance study of workers who manufacture multi-walled carbon nanotubes. Nanotoxicology 2015, 9, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Zdimal, V.; Fenclova, Z.; Vlckova, S.; Turci, F.; Corazzari, I.; Kacer, P.; Schwarz, J.; Zikova, N.; Makes, O.; et al. Markers of oxidative damage of nucleic acids and proteins among workers exposed to TiO2 (nano) particles. Occup. Environ. Med. 2016, 73, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Zdimal, V.; Kacer, P.; Zikova, N.; Komarc, M.; Fenclova, Z.; Vlckova, S.; Schwarz, J.; Makes, O.; Syslova, K.; et al. Markers of lipid oxidative damage in the exhaled breath condensate of nanoTiO2 production workers. Nanotoxicology 2017, 11, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhu, Y.; Chen, Z.; Xu, H.; Zhou, J.; Tang, S.; Xu, Z.; Kong, F.; Li, X.; Zhang, Y.; et al. Cardiopulmonary effects induced by occupational exposure to titanium dioxide nanoparticles. Nanotoxicology 2018, 12, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Bové, H.; Nawrot, T.S.; Nemery, B. Carbon load in airway macrophages as a biomarker of exposure to particulate air pollution; a longitudinal study of an international Panel. Part. Fibre Toxicol. 2018, 15, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forest, V.; Vergnon, J.M.; Guibert, C.; Bitounis, D.; Leclerc, L.; Sarry, G.; Pourchez, J. Metal load assessment in patient pulmonary lavages: Towards a comprehensive mineralogical analysis including the nano-sized fraction. Nanotoxicology 2017, 11, 1211–1224. [Google Scholar] [CrossRef] [PubMed]
- Horváth, I.; Barnes, P.J.; Loukides, S.; Sterk, P.J.; Högman, M.; Olin, A.C.; Amann, A.; Antus, B.; Baraldi, E.; Bikov, A.; et al. A European Respiratory Society technical standard: Exhaled biomarkers in lung disease. Eur. Respir. J. 2017, 49, 1600965. [Google Scholar] [CrossRef] [PubMed]
- Peters-Golden, M. Expanding roles for leukotrienes in airway inflammation. Curr. Allergy Asthma Rep. 2008, 8, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Fenclova, Z.; Kacer, P.; Kuzma, M.; Navratil, T.; Lebedova, J. 8-isoprostane and leukotrienes in exhaled breath condensate in Czech subjects with silicosis. Ind. Health 2007, 45, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Fenclova, Z.; Kacer, P.; Kuzma, M.; Navratil, T.; Lebedova, J. 2008 Increased 8-isoprostane, a marker of oxidative stress in exhaled breath condensate in subjects with asbestos exposure. Ind. Health 2008, 46, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Beck-Speier, I.; Karg, E.; Behrendt, H.; Stoeger, T.; Alessandrini, F. Ultrafine particles affect the balance of endogenous pro- and anti-inflammatory lipid mediators in the lung: In-vitro and in-vivo studies. Part. Fibre Toxicol. 2012, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Zdimal, V.; Kacer, P.; Fenclova, Z.; Vlckova, S.; Syslova, K.; Navratil, T.; Schwarz, J.; Zikova, N.; Barosova, H.; et al. Oxidative stress markers are elevated in exhaled breath condensate of workers exposed to nanoparticles during iron oxide pigment production. J. Breath Res. 2016, 10, 016004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelclova, D.; Zdimal, V.; Schwarz, J.; Dvorackova, S.; Komarc, M.; Ondracek, J.; Kostejn, M.; Kacer, P.; Vlckova, S.; Fenclova, Z.; et al. Markers of oxidative stress in the exhaled breath condensate of workers handling nanocomposites. Nanomaterials 2018, 8, 611. [Google Scholar] [CrossRef] [PubMed]
- Duvall, M.G.; Bruggemann, T.R.; Levy, B.D. Bronchoprotective mechanisms for specialized pro-resolving mediators in the resolution of lung inflammation. Mol. Aspects Med. 2017, 58, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Stefancova, L.; Schwarz, J.; Mäkelä, T.; Hillamo, R.; Smolik, J. Comprehensive characterization of original 10-stage and 7-stage modified Berner type impactors. Aerosol Sci. Technol. 2011, 45, 88–100. [Google Scholar] [CrossRef]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Archer, S.; Fagan, K.; Hassoun, P.M.; Hill, N.S.; Humbert, M.; Kawut, S.M.; Krowka, M.; et al. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Neprasova, M.; Maixnerova, D.; Novak, J.; Reily, C.; Julian, B.A.; Boron, J.; Novotny, P.; Suchanek, M.; Tesar, V.; Kacer, P. Toward noninvasive diagnosis of IgA nephropathy: A pilot urinary metabolomic and proteomic study. Dis. Mark. 2016, 2016, 3650909. [Google Scholar] [CrossRef]
- Schlosser, G.; Kacer, P.; Kuzma, M.; Szilágyi, Z.; Sorrentino, A.; Manzo, C.; Pizzano, R.; Malorni, L.; Pocsfalvi, G. Coupling immunomagnetic separation on magnetic beads with matrix-assisted laser desorption ionization-time of flight mass spectrometry for detection of staphylococcal enterotoxin B. Appl. Environ. Microbiol. 2007, 73, 6945–6952. [Google Scholar] [CrossRef] [PubMed]
- Klusackova, P.; Lebedova, J.; Kacer, P.; Kuzma, M.; Brabec, M.; Pelclova, D.; Fenclova, Z.; Navratil, T. Leukotrienes and 8-isoprostane in exhaled breath condensate in bronchoprovocation tests with occupational allergens. Prostaglandins Leuk. Essent. Fat. Acids 2008, 78, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Khan, M.I.; Patil, G.; Chauhan, L.K. Evaluation of cytotoxic, genotoxic and inflammatory responses of micro- and nano-particles of granite on human lung fibroblast cell IMR-90. Toxicol. Lett. 2012, 208, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Bello, D.; Wardle, B.L.; Zhang, J.; Yamamoto, N.; Santeufemio, C.; Hallock, M.; Virji, M.A. Characterization of exposures to nanoscale particles and fibers during solid core drilling of hybrid carbon nanotube advanced composites. Int. J. Occup. Environ. Health 2010, 16, 434–450. [Google Scholar] [CrossRef] [PubMed]
- Boonruksa, P.; Bello, D.; Zhang, J.; Isaacs, J.A.; Mead, J.L.; Woskie, S.R. Exposures to nanoparticles and fibers during injection molding and recycling of carbon nanotube reinforced polycarbonate composites. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Barosova, H.; Kukutschova, J.; Zdimal, V.; Navratil, T.; Fenclova, Z.; Vlckova, S.; Schwarz, J.; Zikova, N.; Kacer, P.; et al. Raman microspectroscopy of exhaled breath condensate and urine in workers exposed to fine and nanoTiO2 particles: A cross-sectional study. J. Breath Res. 2015, 9, 036008. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekharan, J.A.; Sharma-Walia, N. Lipoxins: Nature’s way to resolve inflammation. J. Inflamm. Res. 2015, 8, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. Targeting cytokines to treat asthma and chronic obstructive pulmonary disease. Nat. Rev. Immunol. 2018, 18, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Elajami, T.K.; Colas, R.A.; Dalli, J.; Chiang, N.; Serhan, C.N.; Welty, F.K. Specialized proresolving lipid mediators in patients with coronary artery disease and their potential for clot remodeling. FASEB J. 2016, 30, 2792–27801. [Google Scholar] [CrossRef] [PubMed]
- Khatri, M.; Bello, D.; Gaines, P.; Martin, J.; Pal, A.K.; Gore, R.; Woskie, S. Nanoparticles from photocopiers induce oxidative stress and upper respiratory tract inflammation in healthy volunteers. Nanotoxicology 2013, 7, 1014–1027. [Google Scholar] [CrossRef] [PubMed]
- Khatri, M.; Bello, D.; Martin, J.; Bello, A.; Gore, R.; Demokritou, P.; Gaines, P. Chronic upper airway inflammation and oxidative stress in photocopier operators: Mechanistic insights. NanoImpact 2017, 5, 133–145. [Google Scholar] [CrossRef]
- Glass, D.C.; Mazhar, M.; Xiang, S.; Dean, P.; Simpson, P.; Priestly, B.; Plebanski, M.; Abramson, M.; Sim, M.R.; Dennekamp, M. Immunological effects among workers who handle engineered nanoparticles. Occup. Environ. Med. 2017, 74, 868–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, E.M.; Pylkkänen, L.; Koivisto, A.J.; Dean, P.; Simpson, P.; Priestly, B.; Plebanski, M.; Abramson, M.; Sim, M.R.; Dennekamp, M. Inhalation exposure to nanosized and fine TiO2 particles inhibits features of allergic asthma in a murine model. Part. Fibre Toxicol. 2010, 7, 35. [Google Scholar] [CrossRef] [PubMed]
- Jacinto, T.; Malinovschi, A.; Janson, C.; Fonseca, J.; Alving, K. Differential effect of cigarette smoke exposure on exhaled nitric oxide and blood eosinophils in healthy and asthmatic individuals. J. Breath Res. 2017, 11, 036006. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Dai, Y.; Zhang, X.; Niu, Y.; Meng, T.; Li, Y.; Duan, H.; Bin, P.; Ye, M.; Jia, X.; et al. Reduced pulmonary function and increased pro-inflammatory cytokines in nanoscale carbon black-exposed workers. Part. Fibre Toxicol. 2014, 11, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelclova, D.; Fenclova, Z.; Syslova, K.; Vlckova, S.; Lebedova, J.; Pecha, O.; Belacek, J.; Navratil, T.; Kuzma, M.; Kacer, P. Oxidative stress markers in exhaled breath condensate in lung fibroses are not significantly affected by systemic diseases. Ind. Health 2011, 49, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Pirela, S.V.; Martin, J.; Bello, D.; Demokritou, P. Nanoparticle exposures from nano-enabled toner-based printing equipment and human health: State of science and future research needs. Crit. Rev. Toxicol. 2017, 47, 683–709. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Zdimal, V.; Kacer, P.; Komarc, M.; Fenclova, Z.; Vlckova, S.; Zikova, N.; Schwarz, J.; Makes, O.; Navratil, T.; et al. Markers of lipid oxidative damage among office workers exposed intermittently to air pollutants including nanoTiO2 particles. Rev. Environ. Health 2017, 32, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Pelclova, D.; Zdimal, V.; Kacer, P.; Vlckova, S.; Fenclova, Z.; Navratil, T.; Komarc, M.; Schwarz, J.; Zikova, N.; Makes, O.; et al. Markers of nucleic acids and proteins oxidation among office workers exposed to air pollutants including (nano)TiO2 particles. Neuro Endocrinol. Lett. 2016, 37 (Suppl. 1), 13–16. [Google Scholar]
- Rossnerova, A.; Pokorna, M.; Svecova, V.; Sram, R.J.; Topinka, J.; Zölzer, F.; Rossner, P., Jr. Adaptation of the human population to the environment: Current knowledge, clues from Czech cytogenetic and “omics” biomonitoring studies and possible mechanisms. Mutat. Res. 2017, 773, 188–203. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Symptom/Disorder | Exposed | Controls | |
|---|---|---|---|
| N | 20 | 21 | p Value |
| Acute bronchitis/bronchopneumonia in past five years (n, %) | 10 (50.0%) | 9 (42.9%) | 0.758 |
| Allergic rhinitis (n, %) | 7 (35.0%) | 10 (60.0%) | 0.530 |
| Asthma (n, %) | 1 (5.0%) | 1 (4.8%) | 1.000 |
| Cough (n, %) | 5 (25.0%) | 1 (4.8%) | 0.093 |
| Chronic bronchitis (n, %) | 4 (20.0%) | 0/0% | * |
| Dyspnea (NYHA class II) (n, %) | 3 (15.0%) | 0 (0%) | * |
| Examination | FVC (L) | %FVC | VCIN (L) | %VCIN | FEV1 (L) | %FEV1 | FEV1/FVC | PEF (L/min) | %PEF |
|---|---|---|---|---|---|---|---|---|---|
| Pre-shift | 4.33 ± 1.02 | 94.70 ± 13.30 | 4.36 ± 1.01 | 92.15 ± 13.04 | 3.86 ± 0.95 | 102.20 ± 13.54 | 0.89 ± 0.06 | 9.77 ± 1.95 | 110.15 ± 14.28 |
| Post-shift | 4.33 ± 0.91 | 94.95 ± 11.64 | 4.39 ± 0.90 | 93.05 ± 11.01 | 3.73 ± 0.81 ⁰ | 99.00 ± 12.03 * | 0.86 ± 0.06 + | 9.44 ± 2.06 | 106.80 ± 15.19 |
| Controls | 4.43 ± 1.05 | 100.76 ± 13.63 | 4.47 ± 1.08 | 98.71 ± 13.04 | 3.88 ± 0.96 | 106.10 ± 13.96 | 0.89 ± 0.06 | 9.72 ± 1.80 | 111.81 ± 20.17 |
| Pre-Shift | Post-Shift | |||||||
|---|---|---|---|---|---|---|---|---|
| Markers | LTB4 | LTD4 | LTE4 | LXB4 | TNF | LTB4 | LTE4 | TNF |
| Nanocomposites production (Yes/No) | 10.70 *** (4.89, 16.51) | 3.09 * (0.24, 5.95) | 4.35 * (0.19, 8.51) | −3.23 * (−6.01, −0.45) | 10.58 *** (6.21, 14.95) | 10.51 *** (4.85, 16.17) | 5.22 * (0.94, 9.50) | 20.34 *** (11.07, 29.61) |
| Age (years) | 0.31 * (0.03, 0.58) | −0.08 (−0.21, 0.06) | −0.05 (−0.25, 0.15) | 0.05 (−0.08, −0.18) | 0.20 (−0.01, 0.41) | 0.29 * (0.02, 0.56) | −0.06 (−0.26, 0.14) | −0.06 (−0.50, 0.39) |
| Gender (Male/Female) | 4.14 (−3.21, 11.48) | −0.57 (−4.17, 3.04) | −4.72 (−9.97, 0.54) | −0.25 (−3.72, 3.21) | 2.56 (−2.97, 8.08) | 3.92 (−3.23, 11.08) | −5.01 (−10.42, 0.40) | 7.61 (−4.12, 19.33) |
| Alcohol (Yes/No) | 9.41 (−0.29, 19.10) | 1.17 (−3.59, 5.93) | 0.68 (−6.26, 7.62) | −2.35 (−6.93, 2.22) | 5.73 (−1.57, 13.03) | 8.57 (−0.87, 18.01) | 0.01 (−7.14, 7.16) | 1.09 (−14.39, 16.57) |
| BMI (kg/m2) | −0.07 (−0.65, 0.51) | 0.15 (−0.14, 0.44) | 0.18 (−0.23, 0.60) | 0.02 (−0.26, 0.29) | −0.16 (−0.60, 0.28) | −0.08 (−0.65, 0.48) | 0.19 (−0.24, 0.61) | −0.36 (−1.29, 0.56) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelclova, D.; Zdimal, V.; Komarc, M.; Vlckova, S.; Fenclova, Z.; Ondracek, J.; Schwarz, J.; Kostejn, M.; Kacer, P.; Dvorackova, S.; et al. Deep Airway Inflammation and Respiratory Disorders in Nanocomposite Workers. Nanomaterials 2018, 8, 731. https://doi.org/10.3390/nano8090731
Pelclova D, Zdimal V, Komarc M, Vlckova S, Fenclova Z, Ondracek J, Schwarz J, Kostejn M, Kacer P, Dvorackova S, et al. Deep Airway Inflammation and Respiratory Disorders in Nanocomposite Workers. Nanomaterials. 2018; 8(9):731. https://doi.org/10.3390/nano8090731
Chicago/Turabian StylePelclova, Daniela, Vladimir Zdimal, Martin Komarc, Stepanka Vlckova, Zdenka Fenclova, Jakub Ondracek, Jaroslav Schwarz, Martin Kostejn, Petr Kacer, Stepanka Dvorackova, and et al. 2018. "Deep Airway Inflammation and Respiratory Disorders in Nanocomposite Workers" Nanomaterials 8, no. 9: 731. https://doi.org/10.3390/nano8090731
APA StylePelclova, D., Zdimal, V., Komarc, M., Vlckova, S., Fenclova, Z., Ondracek, J., Schwarz, J., Kostejn, M., Kacer, P., Dvorackova, S., Popov, A., Klusackova, P., Zakharov, S., & Bello, D. (2018). Deep Airway Inflammation and Respiratory Disorders in Nanocomposite Workers. Nanomaterials, 8(9), 731. https://doi.org/10.3390/nano8090731