A Comparison of Various Chips Used for the Manufacture of Biosensors Applied in Non-Fluidic Array SPRi, Based on the Example of Determination of Cathepsin D

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. SPRi Apparatus
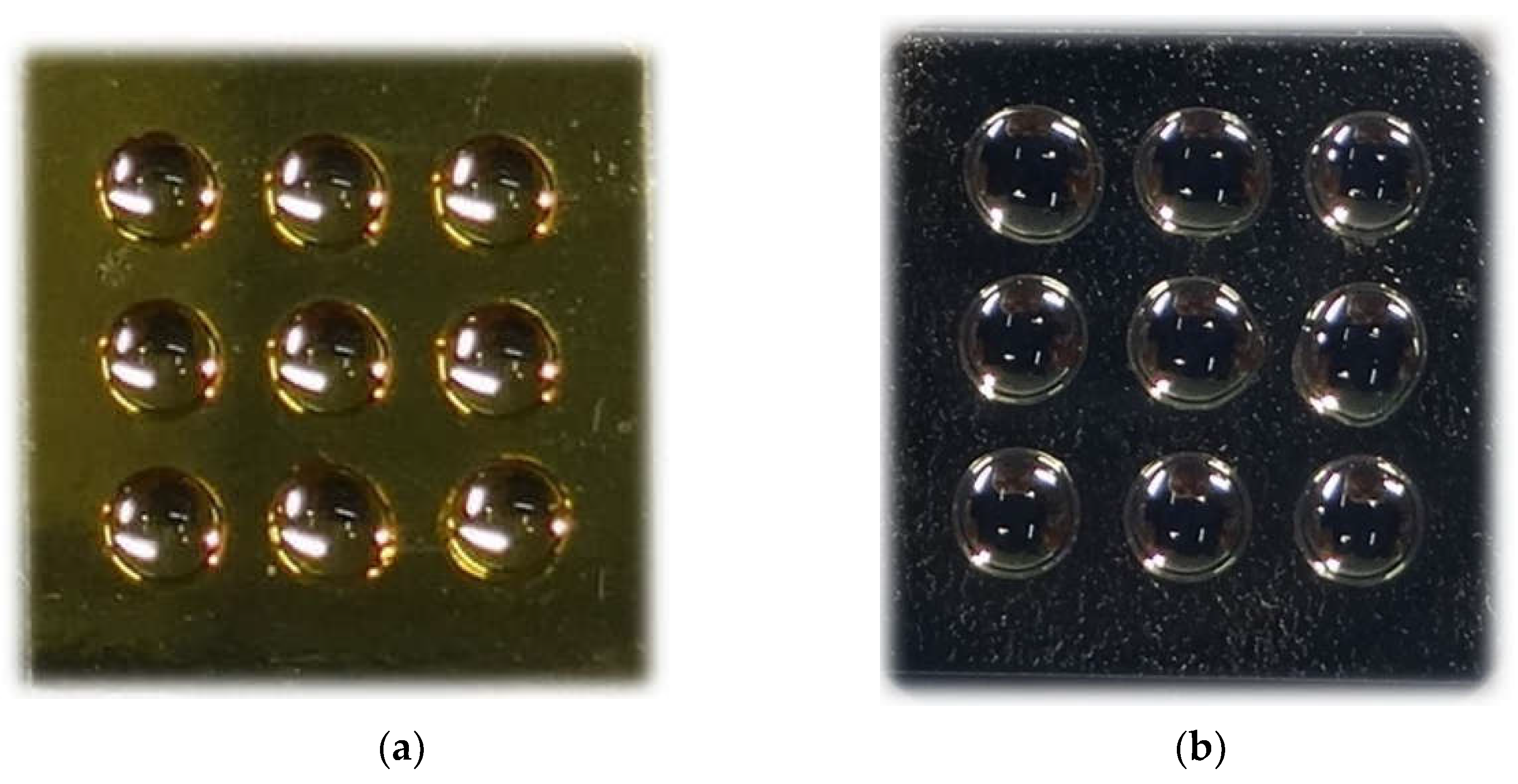
2.2. Chip Manufacture
2.3. Preparation of Separating Paint Layer
2.4. Preparation of Adhesive Polymeric Foil Layer
2.5. Reagents
2.6. Biological Material
2.7. Procedure for Biosensor Preparation
2.8. SPRi Measurement
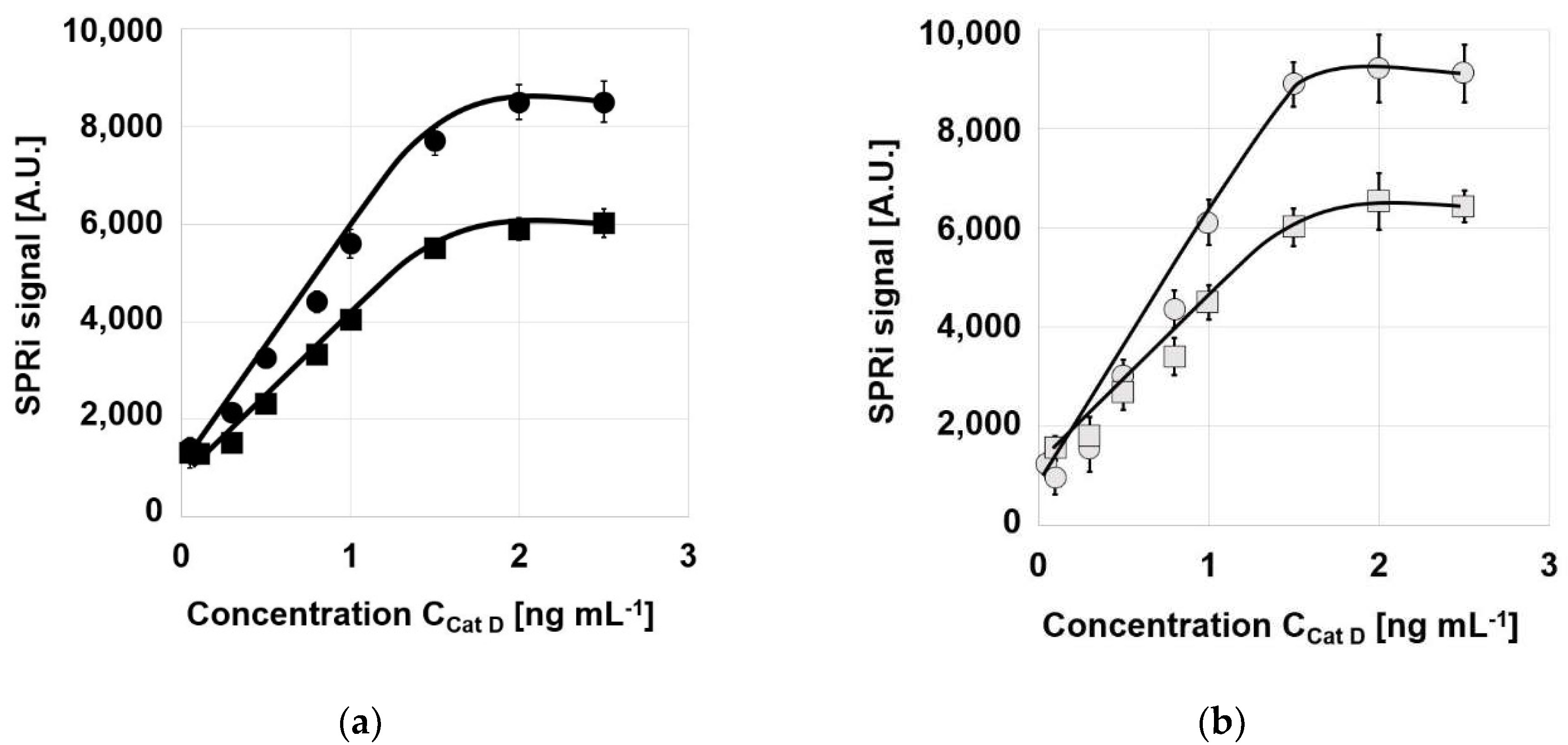
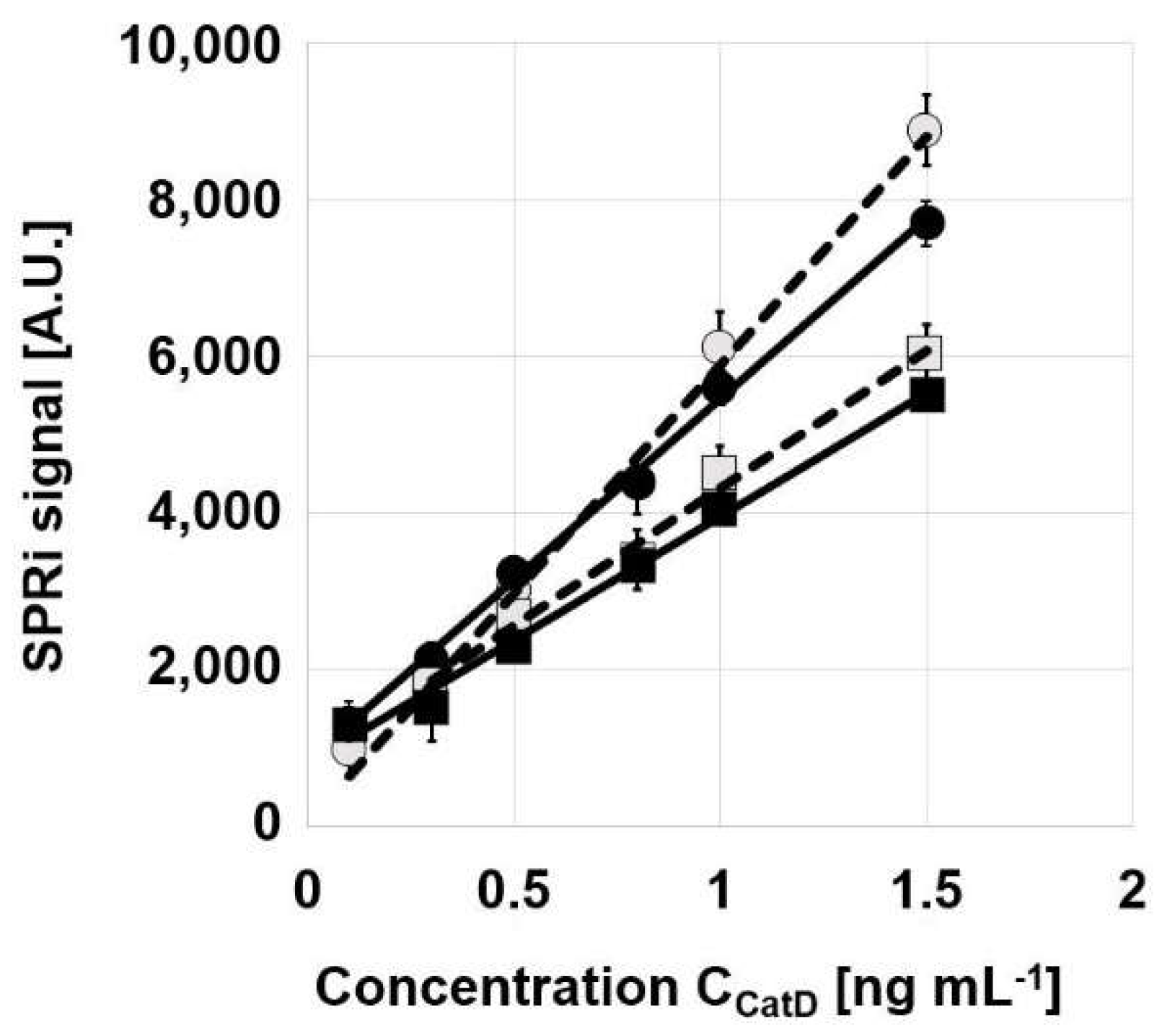
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Szymanska, B.; Lukaszewski, Z.; Zelazowska-Rutkowska, B.; Hermanowicz-Szamatowicz, K.; Gorodkiewicz, E. An SPRi biosensor for determination of the ovarian cancer marker HE 4 in human plasma. Sensors 2021, 21, 3567. [Google Scholar] [CrossRef]
- Szymanska, B.; Lukaszewski, Z.; Hermanowicz-Szamatowicz, K.; Gorodkiewicz, E. A biosensor for determination of the circulating biomarker CA125/MUC16 by Surface Plasmon Resonance Imaging. Talanta 2020, 206, 120. [Google Scholar] [CrossRef] [PubMed]
- Szymanska, B.; Lukaszewski, Z.; Gorodkiewicz, E. An immunosensor for the determination of carcinoembryonic antigen by Surface Plasmon Resonance imaging. Anal. Biochem. 2020, 609, 113964. [Google Scholar] [CrossRef] [PubMed]
- Sankiewicz, A.; Hermanowicz, A.; Grycz, A.; Łukaszewski, Z.; Gorodkiewicz, E. An SPR Imaging immunosensor for leptin determination in blood plasma. Anal. Meth. 2021, 13, 642. [Google Scholar] [CrossRef] [PubMed]
- Gorodkiewicz, E.; Lukaszewski, Z. Recent Progress in Surface Plasmon Resonance Biosensors (2016 to Mid-2018). Biosensors 2018, 4, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falkowski, P.; Lukaszewski, Z.; Gorodkiewicz, E. Potential of Surface Plasmon Resonance Biosensors in cancer detection. J. Pharm. Biomed. Anal. 2021, 194, 113802. [Google Scholar] [CrossRef]
- Gorodkiewicz, E.; Guszcz, T.; Roszkowska-Jakimiec, W.; Kozłowski, R. Cathepsin D serum and urine concentration in superficial and invasive transitional bladder cancer as determined by surface plasmon resonance imaging. Oncol. Lett. 2014, 8, 1323–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sankiewicz, A.; Guszcz, T.; Mena-Hortelano, R.; Zukowski, K.; Gorodkiewicz, E. Podoplanin serum and urine concentration in transitional bladder cancer. Cancer Biomark. 2016, 16, 343–350. [Google Scholar] [CrossRef]
- Guszcz, T.; Szymańska, B.; Kozlowski, R.; Lukaszewski, Z.; Laskowski, P.; Gorodkiewicz, E. Plasma aromatase as a sensitive and selective potential biomarker of bladder cancer and its role in tumorigenesis. Oncol. Lett. 2020, 19, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Laudański, P.; Gorodkiewicz, E.; Ramotowska, B.; Charkiewicz, R.; Kuzmicki, M.; Szamatowicz, J. Determination of cathepsins B, D and G concentration in eutopicproliferative endometrium of women with endometriosis by surface plasmon resonance imaging (SPRI) technique. Eur. J. Obstetr. Gynecol. Reproduc. Biol. 2013, 169, 80–83. [Google Scholar] [CrossRef]
- Weremijewicz, A.; Matuszczak, E.; Sankiewicz, A.; Tylicka, M.; Komarowska, M.; Tokarzewicz, A.; Debek, W.; Gorodkiewicz, E.; Hermanowicz, A. Matrix metalloproteinase-2 and its correlation with basal membrane components laminin-5 and collagen type IV in burn patients measured with Surface Plasmon Resonance Imaging (SPRI) biosensors. Burns 2018, 44, 931–940. [Google Scholar] [CrossRef]
- Matuszczak, E.; Sankiewicz, A.; Debek, W.; Gorodkiewicz, E.; Milewski, R.; Hermanowicz, A. Immunoproteasome in the blood plasma of children with acute appendicitis, and its correlation with proteasome and UCHL1 measured by SPR imaging biosensors. Clin. Exper. Immunol. 2017, 191, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Matuszczak, E.; Komarowska, M.D.; Sankiewicz, A.; Oldak, L.; Gorodkiewicz, E.; Debek, W.; Milewski, R.; Tylicka, M.; Hermanowicz, A. Plasma concentrations of matrix metalloproteinase type 1 and matrix metalloproteinase type 2 in boys with cryptorchidism and its lack of correlation with INSL3 and inhibin B. Scand. J. Clin. Lab. Investig. 2019, 79, 412–418. [Google Scholar] [CrossRef]
- Ermini, M.L.; Chadtová Song, X.; Špringer, T.; Homola, J. Peptide Functionalization of Gold Nanoparticles for the Detection of Carcinoembryonic Antigen in Blood Plasma via SPR-Based Biosensor. Front. Chem. 2019, 7, 40. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Feng, F.; Chen, Z.-Z.; Bai, Y.-F.; Guo, F.-F.; Wu, F.Y.; Zhou, G. Sensitive detection of carcinoembryonic antigen using surface plasmon resonance biosensor with gold nanoparticles signal amplification. Talanta 2015, 140, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Mrozek, P.; Gorodkiewicz, E.; Falkowski, P.; Hosciło, B. Sensitivity Analysis of Single- and Bimetallic Surface Plasmon Resonance Biosensors. Sensors 2021, 21, 4348. [Google Scholar] [CrossRef]
- Falkowski, P.; Mrozek, P.; Lukaszewski, Z.; Oldak, L.; Gorodkiewicz, E. An Immunosensor for the Determination of Cathepsin S in Blood Plasma by Array SPRi—A Comparison of Analytical Properties of Silver–Gold and Pure Gold Chips. Biosensors 2021, 11, 298. [Google Scholar] [CrossRef] [PubMed]
- Sankiewicz, A.; Tokarzewicz, A.; Gorodkiewicz, E. Regeneration of surface plasmon resonance chips for multiple use. Bulgar. Chem. Commun. 2015, 47, 477–482. [Google Scholar]
- Kim, J.-W.; Jung, S.-Y.; Kim, Y.; Heo, H.; Hong, C.-H.; Seo, S.-W.; Choi, S.-H.; Son, S.-J.; Lee, S.; Chang, J. Identification of Cathepsin D as a Plasma Biomarker for Alzheimer’s Disease. Cells 2021, 10, 138. [Google Scholar] [CrossRef] [PubMed]
- Tam, J.M.; Josephson, L.; Pilozzi, A.R.; Huang, X. A Novel Dual Fluorochrome Near-Infrared Imaging Probe for Potential Alzheimer’s Enzyme Biomarkers-BACE1 and Cathepsin D. Molecules 2020, 25, 274. [Google Scholar] [CrossRef] [Green Version]
- Bunk, J.; Prieto Huarcaya, S.; Drobny, A.; Dobert, J.P.; Walther, L.; Rose-John, S.; Arnold, P.; Zunke, F. Cathepsin D Variants Associated with Neurodegenerative Diseases Show Dysregulated Functionality and Modified αSynuclein Degradation Properties. Front. Cell Dev. Biol. 2021, 9, 581805. [Google Scholar] [CrossRef]
- Kang, J.; Yu, Y.; Jeong, S.; Lee, H.; Heo, H.J.; Park, J.J.; Na, H.S.; Ko, D.S.; Kim, Y.H. Prognostic role of high cathepsin D expression in breast cancer: A systematic review and meta-analysis. Ther. Adv. Med. Oncol. 2020, 12, 1–13. [Google Scholar] [CrossRef]
- Dai, J.; Zhang, Q.; Wan, C.; Liu, J.; Zhang, Q.; Yu, Y.; Wang, J. Significances of viable synergistic autophagy-associated cathepsin B and cathepsin D (CTSB/CTSD) as potential biomarkers for sudden cardiac death. BMC Cardiovasc. Disord. 2021, 21, 233. [Google Scholar] [CrossRef]
- Ding, L.; Houben, T.; Oligschlaeger, Y.; Bitorina, A.V.; Verwer, B.J.; Tushuizen, M.E.; Shiri-Sverdlov, R. Plasma Cathepsin D Activity Rather than Levels Correlates with Metabolic Parameters of Type 2 Diabetes in Male Individuals. Front. Endocrinol. 2020, 11, 575070. [Google Scholar] [CrossRef]
- Di Domenico, F.; Tramutola, A.; Perluigi, M. Cathepsin D as a therapeutic target in Alzheimer’s disease. Expert Opin. Ther. Targets 2016, 20, 1393–1395. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Khoo, S.; Chan, W.-K.; Sthaneshwar, P.; Mustapha, N.R.N.; Mahadeva, S. Limited applicability of cathepsin D for the diagnosis and monitoring of non-alcoholic steatohepatitis. J. Gastreoeneter. Hepatol. Open 2019, 3, 417–424. [Google Scholar] [CrossRef]
- Tan, G.; Liu, Q.; Tang, X.; Kang, T.; Li, Y.; Lu, J.; Zhao, X.; Tang, F. Diagnostic values of serum cathepsin B and D in patients with nasopharyngeal carcinoma. BMC Cancer 2016, 16, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- İlhan, G.A.; Yıldızhan, B. Evaluation of serum cathepsin B, D, and L concentrations in women with late-onset preeclampsia. Turk. J. Obstet. Gynecol. 2019, 16, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Mohammadpoura, A.H.; Salehinejada, Z.; Elyasia, S.; Mouhebatic, M.; Mirhafezd, S.R.; Samadie, S.; Ghayour-Mobarhane, M.; Fernsf, G.; Sahebkarg, A. Evaluation of serum cathepsin D concentrations in coronary artery disease. Ind. Heart J. 2018, 70, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Macagno, A.; Athanasiou, A.; Wittig, A.; Huber, R.; Weber, S.; Keller, T.; Rhiel, M.; Golding, G.; Schiess, R. Analytical performance of thrombospondin-1 and cathepsin D immunoassays part of a novel CE-IVD marked test as an aid in the diagnosis of prostate cancer. PLoS ONE 2020, 15, e0233442. [Google Scholar] [CrossRef] [PubMed]
- Afinogenova, Y.; Ruan, J.; Yang, R.; Kleytman, N.; Pastores, G.; Lischuk, A.; Mistry, P.K. Aberrant progranulin, YKL-40, cathepsin D and cathepsin S in Gaucher disease. Mol. Gen. Metabol. 2019, 128, 62–67. [Google Scholar] [CrossRef]
- Kher, M.; Beri, S.; Rehan, H.S.; Prakash, A.; Gupta, L.K. Effect of metformin and insulin combination on monocyte chemoattractant protein-1 and cathepsin-D in type 2 diabetes mellitus. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1703–1710. [Google Scholar] [CrossRef] [PubMed]
- Gorodkiewicz, E.; Regulska, E. SPR Imaging Biosensor for Aspartyl Cathepsins: Sensor Development and Application for Biological Material. Protein Pept. Lett. 2010, 17, 1148. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Disease | Concentration [ng mL−1] | Analytical Method | Manufacturer | Reference |
|---|---|---|---|---|
| Control | 0.144–0.46 | No data | No data | [26] |
| Control | 2.7 ± 0.8 | ELISA | Wuhan Eiaab Science Co. Ltd., Wuhan, China | [27] |
| Control | 4.20 ± 1.65 | ELISA | Elabscience, Houston, TX, USA | [28] |
| Control | 4.22 ± 3.01 | ELISA | Wuhan USCN, SEB280Hu, China | [19] |
| Control | 12.69 ± 9.29 | No data | No data | [29] |
| Healthy donors | 6–15 | ELISA | Proteomedix, Switzerland | [30] |
| Healthy controls | 123.6 ± 10.9 | ELISA | Abcam, USA | [31] |
| Control | 2.88 ± 0.57 | SPRi (a) | This paper | |
| Control | 2.73 ± 0.63 | SPRi (b) | This paper | |
| Control | 2.84 ± 0.63 | SPRi (c) | This paper | |
| Control | 3.08 ± 0.59 | SPRi (d) | This paper | |
| Alzheimer’s | 1.836 ± 1.744 | ELISA | Wuhan USCN, SEB280Hu, China | [19] |
| Gaucher | 363.1 ± 30.7 | ELISA | Abcam, USA | [31] |
| Nasopharyngeal carcinoma | 15.7 ± 8.7 | ELISA | Wuhan Eiaab Science Co. Ltd., China | [27] |
| Type 2 diabetes | 234–1690 | ELISA | Sincere, Japan | [32] |
| Preeclampsia | 4.97 ± 1.24 | ELISA | Elabscience, Houston, USA | [28] |
| Non-alcoholic fatty liver patients | 0.213–0.508 | No data | No data | [26] |
| Glioblastoma | 4.71 ± 1.64 | SPRi (a) | This paper | |
| Glioblastoma | 5.12 ± 1.70 | SPRi (b) | This paper | |
| Glioblastoma | 4.57 ± 1.62 | SPRi (c) | This paper | |
| Glioblastoma | 5.02 ± 1.68 | SPRi (d) | This paper |
| Chip | Separating Polymer | Intercept [ng mL−1] | Slope [ng mL−1] | R2 |
|---|---|---|---|---|
| Au | Two paints | 793 | 3152 | 0.9925 |
| Foil | 827 | 4618 | 0.9907 | |
| Ag/Au | Two paints | 804 | 3507 | 0.9978 |
| Foil | 53 | 5840 | 0.9915 |
| Cath D Spike [ng mL−1] | Found [ng mL−1] | SD [ng mL−1] | RSD [%] | Recovery [%] |
|---|---|---|---|---|
| 0.5 | 0.47 | 0.05 | 10 | 95 |
| 0.8 | 0.79 | 0.06 | 7.5 | 99 |
| 1.0 | 0.97 | 0.12 | 12 | 97 |
| LOD 0.12 | ||||
| LOQ 0.40 |
| Cath D Spike [ng mL−1] | Found [ng mL−1] | SD [ng mL−1] | RSD [%] | Recovery [%] |
|---|---|---|---|---|
| 0.5 | 0.52 | 0.09 | 18 | 104 |
| 0.8 | 0.77 | 0.11 | 14 | 96 |
| 1.0 | 0.95 | 0.12 | 12 | 95 |
| LOD 0.06 | ||||
| LOQ 0.20 |
| Cath D Spike [ng mL−1] | Found [ng mL−1] | SD [ng mL−1] | RSD [%] | Recovery [%] |
|---|---|---|---|---|
| 0.5 | 0.52 | 0.04 | 8 | 104 |
| 0.8 | 0.76 | 0.03 | 3.8 | 95 |
| 1.0 | 1.05 | 0.05 | 5 | 105 |
| LOD 0.09 | ||||
| LOQ 0.30 |
| Cath D Spike [ng mL−1] | Found [ng mL−1] | SD [ng mL−1] | RSD [%] | Recovery [%] |
|---|---|---|---|---|
| 0.3 | 0.34 | 0.15 | 50 | 113 |
| 0.5 | 0.54 | 0.08 | 16 | 108 |
| 0.8 | 0.80 | 0.09 | 11 | 100 |
| LOD 0.05 | ||||
| LOQ 0.17 |
| Sample | CathD (a) [ng mL−1] | CathD (b) [ng mL−1] | CathD (c) [ng mL−1] | CathD (d) [ng mL−1] |
|---|---|---|---|---|
| 1 2 3 4 5 6 7 8 9 | 2.93 ± 0.09 3.86 ± 0.12 | 2.67 ± 0.19 3.25 ± 0.29 | 2.79 ± 0.12 3.59 ± 0.23 | 3.03 ± 0.21 4.01 ± 0.24 |
| 2.05 ± 0.24 2.24 ± 0.15 2.40 ± 0.31 3.13 ± 0.18 2.94 ± 0.22 2.90 ± 0.19 3.37 ± 0.17 | 1.80 ± 0.09 2.02 ± 0.19 2.21 ± 0.09 3.01 ± 0.33 3.21 ± 0.32 2.67 ± 0.23 3.69 ± 0.29 | 2.01 ± 0.29 2.05 ± 0.17 2.11 ± 0.12 3.31 ± 0.19 3.03 ± 0.21 3.18 ± 0.12 3.49 ± 0.25 | 2.24 ± 0.36 2.44 ± 0.25 2.60 ± 0.17 3.46 ± 0.25 3.16 ± 0.28 3.10 ± 0.17 3.74 ± 0.31 | |
| Average | 2.88 ± 0.57 | 2.73 ± 0.63 | 2.84 ± 0.63 | 3.08 ± 0.59 |
| Sample | CathD (a) [ng mL−1] | CathD (b) [ng mL−1] | CathD (c) [ng mL−1] | CathD (d) [ng mL−1] |
|---|---|---|---|---|
| 1 2 3 4 5 6 7 8 9 | 3.95 ± 0.32 4.49 ± 0.28 | 4.19 ± 0.29 4.95 ± 0.32 | 4.02 ± 0.11 4.22 ± 0.17 | 4.23 ± 0.13 4.81 ± 0.29 |
| 3.07 ± 0.10 6.33 ± 0.41 7.49 ± 0.14 3.45 ± 0.12 3.56 ± 0.27 6.56 ± 0.33 3.45 ± 0.11 | 3.34 ± 0.21 6.87 ± 0.45 7.96 ± 0.31 3.97 ± 0.29 3.98 ± 0.17 6.99 ± 0.31 3.82 ± 0.22 | 3.11 ± 0.19 6.22 ± 0.60 7.36 ± 0.43 3.23 ± 0.19 3.30 ± 0.23 6.30 ± 0.34 3.33 ± 0.17 | 3.44 ± 0.23 6.79 ± 0.43 7.89 ± 0.61 3.78 ± 0.21 3.51 ± 0.31 6.79 ± 0.41 3.98 ± 0.21 | |
| Average | 4.71 ± 1.64 | 5.12 ± 1.70 | 4.57 ± 1.62 | 5.02 ± 1.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falkowski, P.; Mrozek, P.; Miluski, P.; Lukaszewski, Z.; Gorodkiewicz, E. A Comparison of Various Chips Used for the Manufacture of Biosensors Applied in Non-Fluidic Array SPRi, Based on the Example of Determination of Cathepsin D. Biosensors 2022, 12, 21. https://doi.org/10.3390/bios12010021
Falkowski P, Mrozek P, Miluski P, Lukaszewski Z, Gorodkiewicz E. A Comparison of Various Chips Used for the Manufacture of Biosensors Applied in Non-Fluidic Array SPRi, Based on the Example of Determination of Cathepsin D. Biosensors. 2022; 12(1):21. https://doi.org/10.3390/bios12010021
Chicago/Turabian StyleFalkowski, Pawel, Piotr Mrozek, Piotr Miluski, Zenon Lukaszewski, and Ewa Gorodkiewicz. 2022. "A Comparison of Various Chips Used for the Manufacture of Biosensors Applied in Non-Fluidic Array SPRi, Based on the Example of Determination of Cathepsin D" Biosensors 12, no. 1: 21. https://doi.org/10.3390/bios12010021
APA StyleFalkowski, P., Mrozek, P., Miluski, P., Lukaszewski, Z., & Gorodkiewicz, E. (2022). A Comparison of Various Chips Used for the Manufacture of Biosensors Applied in Non-Fluidic Array SPRi, Based on the Example of Determination of Cathepsin D. Biosensors, 12(1), 21. https://doi.org/10.3390/bios12010021