Direct Use of a Saliva-Collected Cotton Swab in Lateral Flow Immunoassay for the Detection of Cotinine


Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Instruments
2.2. Construction of Gold Conjugates with Antibody
2.3. Preparation of Gap-LFIA Strip Sensor
2.4. Gap-LFIA Testing of Cotinine in a Buffer and Spiked Saliva
2.5. Test of Real Samples Collected from Smokers and Non-Smokers and Comparison with ELISA
3. Results and Discussion
3.1. Optimization of the Gap-LFIA Sensor for Cotinine Using Cotton Swabs
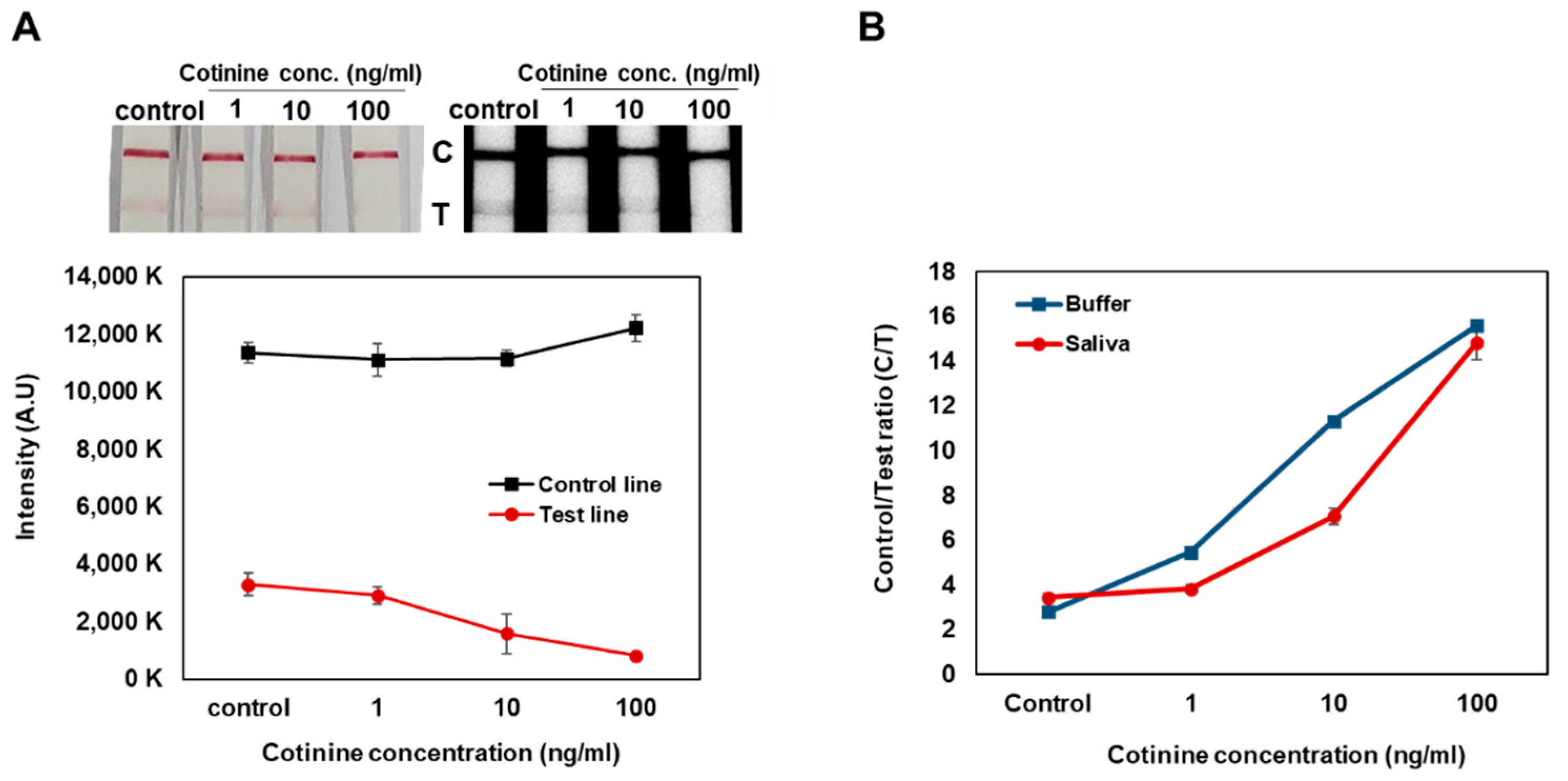
3.2. Sensitivity and Specificity of the LFIA Test for Standard Cotinine and Spiked Saliva
3.3. Salivary Cotinine Sensitivity Test with Smokers and Non-Smokers
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Almulla, A.; Hassan-Yassoub, N.; Fu, D.; El-Awa, F.; Alebshehy, R.; Ismail, M.; Fraser, C.P. Smoking cessation services in the eastern mediterranean region: Highlights and findings from the WHO report on the global tobacco epidemic 2019. East. Mediterr. Health J. 2020, 26, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Messner, B.; Bernhard, D. Smoking and Cardiovascular Disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Eyre, H.; Kahn, R.; Robertson, R.M. Preventing cancer, cardiovascular disease, and diabetes: A common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Diabetes Care 2004, 27, 1812–1824. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.E.; Hong, Y.C.; Park, H.; Ha, M.; Hyeong Kim, J.; Chang, N.; Roh, Y.M.; Kim, B.N.; Kim, Y.; Oh, S.Y.; et al. Secondhand smoke exposure during pregnancy and infantile neurodevelopment. Environ. Res. 2011, 111, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Yoon, T.; Yang, H.; Cha, S.; Cheon, Y.; Kashefi-Kheyrabadi, L.; Jung, H. All-in-one platform for salivary cotinine detection integrated with a microfluidic channel and an electrochemical biosensor. Lab Chip 2020, 20, 320–331. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.; Zhao, W.; Liu, S.; Sui, G. Microfluidic immunoassay for rapid detection of cotinine in saliva. Biomed. Microdevices 2013, 15, 949–957. [Google Scholar] [CrossRef] [PubMed]
- Langone, J.J.; Cook, G.; Bjercke, R.J.; Lifschitz, M.H. Monoclonal antibody ELISA for cotinine in saliva and urine of active and passive smokers. J. Immunol. Methods 1988, 114, 73–78. [Google Scholar] [CrossRef]
- Etter, J.F. Assessment of the accuracy of salivary cotinine readings from NicAlert strips against a liquid chromatography tandem mass spectrometry assay in self-reported non-smokers who passed carbon monoxide but failed NicAlert validation. Addiction 2019, 114, 2252–2256. [Google Scholar] [CrossRef] [PubMed]
- Petersen, G.O.; Leite, C.E.; Chatkin, J.M.; Thiesen, F.V. Cotinine as a biomarker of tobacco exposure: Development of a HPLC method and comparison of matrices. J. Sep. Sci. 2010, 33, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.K.; Kim, J.W.; Kim, J.M.; Kim, M.G. High sensitive and broad-range detection of cortisol in human saliva using a trap lateral flow immunoassay (trapLFI) sensor. Analyst 2018, 143, 3883–3889. [Google Scholar] [CrossRef] [PubMed]
- Raja, M.; Garg, A.; Yadav, P.; Jha, K.; Handa, S. Diagnostic methods for detection of cotinine level in tobacco users: A review. J. Clin. Diagn. Res. JCDR 2016, 10, ZE04. [Google Scholar] [CrossRef] [PubMed]
- Ramdzan, A.N.; Almeida, M.I.G.S.; McCullough, M.J.; Segundo, M.A.; Kolev, S.D. Determination of salivary cotinine as tobacco smoking biomarker. TrAC—Trends Anal. Chem. 2018, 105, 89–97. [Google Scholar] [CrossRef]
- Topkas, E.; Keith, P.; Dimeski, G.; Cooper-White, J.; Punyadeera, C. Evaluation of saliva collection devices for the analysis of proteins. Clin. Chim. Acta 2012, 413, 1066–1070. [Google Scholar] [CrossRef] [PubMed]
- Miočević, O.; Cole, C.R.; Laughlin, M.J.; Buck, R.L.; Slowey, P.D.; Shirtcliff, E.A. Quantitative Lateral Flow Assays for Salivary Biomarker Assessment: A Review. Front. Public Health 2017, 5, 133. [Google Scholar] [CrossRef]
- Freire, M.G.; Neves, C.M.S.S.; Marrucho, I.M.; Canongia Lopes, J.N.; Rebelo, L.P.N.; Coutinho, J.A.P. High-performance extraction of alkaloids using aqueous two-phase systems with ionic liquids. Green Chem. 2010, 12, 1715–1718. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Detection Method | Collection | Pretreatment | Sensitivity | Reference |
|---|---|---|---|---|
| Microfluidic/ electrochemical | Cotton collector | Filter | 1 pg/mL | [5] |
| LC-MS/MS | Spit | Centrifuge, dilution | 1 pg/mL | [5] |
| Microfluidic immunofluorescence | Spit | Dilution | 1 ng/mL | [6] |
| ELISA | n/a | n/a | 1 ng/mL | [7] |
| Colorimetric immunoassay | Spit | Dilution | 10 ng/mL | [8] |
| Colorimetric immunoassay | Cotton swab | n/a | 10 ng/mL | This work |
| Company | Products | Collection Tool | Sensitivity |
|---|---|---|---|
| ConfirmBioscience | NicAlert™ | Spit | 10 ng/mL |
| NicoTests | NicoTests | Spit | 30 ng/mL |
| ALCOPRO | iScreen Oral Fluid Nicotine Test | Sponge | 30 ng/mL |
| STAT Technologies | NicDetect Oral Cotinine Test | Sponge | 30 ng/mL |
| ALLTEST | Nico Quick Saliva Test | Stick | 20 ng/mL |
| ONP | N-Checker | Spit | 50 ng/mL |
| HUBIOTECH | NicoCheck Saliva Test | Stick | 20 ng/mL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, C.; Kim, M.-G. Direct Use of a Saliva-Collected Cotton Swab in Lateral Flow Immunoassay for the Detection of Cotinine. Biosensors 2022, 12, 214. https://doi.org/10.3390/bios12040214
Jung C, Kim M-G. Direct Use of a Saliva-Collected Cotton Swab in Lateral Flow Immunoassay for the Detection of Cotinine. Biosensors. 2022; 12(4):214. https://doi.org/10.3390/bios12040214
Chicago/Turabian StyleJung, Chaewon, and Min-Gon Kim. 2022. "Direct Use of a Saliva-Collected Cotton Swab in Lateral Flow Immunoassay for the Detection of Cotinine" Biosensors 12, no. 4: 214. https://doi.org/10.3390/bios12040214
APA StyleJung, C., & Kim, M. -G. (2022). Direct Use of a Saliva-Collected Cotton Swab in Lateral Flow Immunoassay for the Detection of Cotinine. Biosensors, 12(4), 214. https://doi.org/10.3390/bios12040214