Diagnoses Based on C-Reactive Protein Point-of-Care Tests


Abstract
:1. Introduction
2. The Use of CRP in Diagnoses
3. Routine CRP Point-of-Care Tests and Immunochemical Tests
4. New Biosensors and Point-of-Care Bioassays for CRP
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qian, W.H.; Song, T.; Ye, M.; Huang, X.Y.; Li, Y.J.; Hao, B.J. Functionalized nanographene oxide/PEG/rhodamine B/gold nanocomposite for electrochemical determination of glucose. J. Mater. Sci. Technol. 2022, 122, 141–147. [Google Scholar] [CrossRef]
- Wu, B.F.; Xu, H.T.; Shi, Y.F.; Yao, Z.J.; Yu, J.Y.; Zhou, H.; Li, Y.P.; Chen, Q.L.; Long, Y.B. Microelectrode glucose biosensor based on nanoporous platinum/graphene oxide nanostructure for rapid glucose detection of tomato and cucumber fruits. Food Qual. Saf. 2022, 6, 11. [Google Scholar] [CrossRef]
- Yang, B.; Wang, K.Y.; Zhou, J.H.; Shao, X.Y.; Gu, X.F.; Xue, Y.S.; Tian, S. Ratiometric SERS detection of H2O2 and glucose using a pyrroloquinoline skeleton containing molecule as H2O2-responsive probe. Appl. Surf. Sci. 2022, 590, 10. [Google Scholar] [CrossRef]
- Kuznetsova, L.S.; Arlyapov, V.A.; Kamanina, O.A.; Lantsova, E.A.; Tarasov, S.E.; Reshetilov, A.N. Development of Nanocomposite Materials Based on Conductive Polymers for Using in Glucose Biosensor. Polymers 2022, 14, 1543. [Google Scholar] [CrossRef] [PubMed]
- Lew, T.T.S.; Aung, K.M.M.; Ow, S.Y.; Amrun, S.N.; Sutarlie, L.; Ng, L.F.P.; Su, X.D. Epitope-Functionalized Gold Nanoparticles for Rapid and Selective Detection of SARS-CoV-2 IgG Antibodies. ACS Nano 2021, 15, 12286–12297. [Google Scholar] [CrossRef] [PubMed]
- Polvere, I.; Voccola, S.; D’Andrea, S.; Zerillo, L.; Varricchio, R.; Madera, J.R.; Stilo, R.; Vito, P.; Zotti, T. Evaluation of FAST COVID-19 SARS-CoV-2 Antigen Rapid Test Kit for Detection of SARS-CoV-2 in Respiratory Samples from Mildly Symptomatic or Asymptomatic Patients. Diagnostics 2022, 12, 650. [Google Scholar] [CrossRef]
- Lustig, Y.; Keler, S.; Kolodny, R.; Ben-Tal, N.; Atias-Varon, D.; Shlush, E.; Gerlic, M.; Munitz, A.; Doolman, R.; Asraf, K.; et al. Potential Antigenic Cross-reactivity Between Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Dengue Viruses. Clin. Infect. Dis. 2021, 73, E2444–E2449. [Google Scholar] [CrossRef]
- Anderson, C.E.; Huynh, T.; Gasperino, D.J.; Alonzo, L.F.; Cantera, J.L.; Harston, S.P.; Hsieh, H.V.; Marzan, R.; McGuire, S.K.; Williford, J.R.; et al. Automated liquid handling robot for rapid lateral flow assay development. Anal. Bioanal. Chem. 2022, 414, 2607–2618. [Google Scholar] [CrossRef]
- Rahbar, M.; Zou, S.Y.; Baharfar, M.; Liu, G.Z. A Customized Microfluidic Paper-Based Platform for Colorimetric Immunosensing: Demonstrated via hCG Assay for Pregnancy Test. Biosensors 2021, 11, 474. [Google Scholar] [CrossRef]
- Wang, X.; Xue, C.H.; Yang, D.; Jia, S.T.; Ding, Y.R.; Lei, L.; Gao, K.Y.; Jia, T.T. Modification of a nitrocellulose membrane with nanofibers for sensitivity enhancement in lateral flow test strips. RSC Adv. 2021, 11, 26493–26501. [Google Scholar] [CrossRef]
- Chang, R.C.H.; Wang, C.Y.; Li, H.H.; Chiu, C.D. Drunk Driving Detection Using Two-Stage Deep Neural Network. IEEE Access 2021, 9, 116564–116571. [Google Scholar] [CrossRef]
- Hackett, M.A.; Gorczynski, L.Y.; Martin, T.L. The effect of non-alcoholic food and beverage consumption on preliminary breath alcohol testing by the Drager Alcotest 6810 and Alco-Sensor FST. Can. Soc. Forensic Sci. J. 2017, 50, 131–145. [Google Scholar] [CrossRef]
- Zhang, K.; Xie, K.; Zhang, C.X.; Liang, Y.J.; Chen, Z.K.; Wang, H.F. C-reactive protein testing to reduce antibiotic prescribing for acute respiratory infections in adults: A systematic review and meta-analysis. J. Thorac. Dis. 2022, 14, 123. [Google Scholar] [CrossRef]
- Kharel, S.; Ojha, R.; Preethish-Kumar, V.; Bhagat, R. C-reactive protein levels in patients with amyotrophic lateral sclerosis: A systematic review. Brain Behav. 2022, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Sampedro, M.; Sanles-Gonzalez, I.; Garcia-Ibarbia, C.; Fananas-Rodriquez, N.; Fakkas-Fernandez, M.; Farinas, M.C. The poor accuracy of D-dimer for the diagnosis of prosthetic joint infection but its potential usefulness in early postoperative infections following revision arthroplasty for aseptic loosening. BMC Infect. Dis. 2022, 22, 10. [Google Scholar] [CrossRef]
- Moutachakkir, M.; Lamrani Hanchi, A.; Baraou, A.; Boukhira, A.; Chellak, S. Immunoanalytical characteristics of C-reactive protein and high sensitivity C-reactive protein. Ann. Biol. Clin. 2017, 75, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Pathak, A.; Agrawal, A. Evolution of C-Reactive Protein. Front. Immunol. 2019, 10, 943. [Google Scholar] [CrossRef] [Green Version]
- Shrive, A.K.; Cheetham, G.M.; Holden, D.; Myles, D.A.; Turnell, W.G.; Volanakis, J.E.; Pepys, M.B.; Bloomer, A.C.; Greenhough, T.J. Three dimensional structure of human C-reactive protein. Nat. Struct. Biol. 1996, 3, 346–354. [Google Scholar] [CrossRef]
- Wang, H.W.; Sui, S.F. Dissociation and subunit rearrangement of membrane-bound human C-reactive proteins. Biochem. Biophys. Res. Commun. 2001, 288, 75–79. [Google Scholar] [CrossRef]
- Nazarov, P.G.; Polevshchikov, A.V.; Berestovaya, L.K.; Petrov, I.V.; Ponomarenko, V.V. Characterization of antigenic and cytotropic properties of C-reactive protein subunits. Bull. Exp. Biol. Med. 1993, 116, 1512–1514. [Google Scholar] [CrossRef]
- Eisenhardt, S.U.; Thiele, J.R.; Bannasch, H.; Stark, G.B.; Peter, K. C-reactive protein How conformational changes influence inflammatory properties. Cell Cycle 2009, 8, 3885–3892. [Google Scholar] [CrossRef] [PubMed]
- Zen, Q.; Zhong, W.J.; Mortensen, R.F. Binding site on human C-reactive protein (CRP) recognized by the leukocyte CRP-receptor. J. Cell. Biochem. 1997, 64, 140–151. [Google Scholar] [CrossRef]
- Guillon, C.; Bigouagou, U.M.; Folio, C.; Jeannin, P.; Delneste, Y.; Gouet, P. A staggered decameric assembly of human C-reactive protein stabilized by zinc ions revealed by X-ray crystallography. Protein Pept. Lett. 2014, 22, 248–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waterhouse, A.; Bertoni, M.; Bienert, S.; Studer, G.; Tauriello, G.; Gumienny, R.; Heer, F.T.; de Beer, T.A.P.; Rempfer, C.; Bordoli, L.; et al. SWISS-MODEL: Homology modelling of protein structures and complexes. Nucleic Acids Res. 2018, 46, W296–W303. [Google Scholar] [CrossRef] [Green Version]
- Bienert, S.; Waterhouse, A.; de Beer, T.A.; Tauriello, G.; Studer, G.; Bordoli, L.; Schwede, T. The SWISS-MODEL Repository-new features and functionality. Nucleic Acids Res. 2017, 45, D313–D319. [Google Scholar] [CrossRef] [Green Version]
- Guex, N.; Peitsch, M.C.; Schwede, T. Automated comparative protein structure modeling with SWISS-MODEL and Swiss-PdbViewer: A historical perspective. Electrophoresis 2009, 30, S162–S173. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Sucajtys-Szulc, E.; Debska-Slizien, A.; Rutkowski, B.; Milczarek, R.; Pelikant-Malecka, I.; Sledzinski, T.; Swierczynski, J.; Szolkiewicz, M. Hepatocyte nuclear factors as possible C-reactive protein transcriptional inducer in the liver and white adipose tissue of rats with experimental chronic renal failure. Mol. Cell. Biochem. 2018, 446, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Alikiaii, B.; Heidari, Z.; Bagherniya, M.; Askari, G.; Sathyapalan, T.; Sahebkar, A. The Effect of Statins on C-Reactive Protein in Stroke Patients: A Systematic Review of Clinical Trials. Mediat. Inflamm. 2021, 2021, 10. [Google Scholar] [CrossRef]
- Kayser, S.; Brunner, P.; Althaus, K.; Dorst, J.; Sheriff, A. Selective Apheresis of C-Reactive Protein for Treatment of Indications with Elevated CRP Concentrations. J. Clin. Med. 2020, 9, 2947. [Google Scholar] [CrossRef]
- Enocsson, H.; Karlsson, J.; Li, H.Y.; Wu, Y.; Kushner, I.; Wetterö, J.; Sjöwall, C. The Complex Role of C-Reactive Protein in Systemic Lupus Erythematosus. J. Clin. Med. 2021, 10, 5837. [Google Scholar] [CrossRef] [PubMed]
- Melnikov, I.S.; Kozlov, S.G.; Saburova, O.S.; Avtaeva, Y.N.; Prokofieva, L.V.; Gabbasov, Z.A. Current Position on the Role of Monomeric C-reactive Protein in Vascular Pathology and Atherothrombosis. Curr. Pharm. Des. 2020, 26, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Ji, S.R.; Wang, H.W.; Sui, S.F. Study of the spontaneous dissociation of rabbit C-reactive protein. Biochemistry 2002, 67, 1377–1382. [Google Scholar] [CrossRef] [PubMed]
- Heuertz, R.M.; Schneider, G.P.; Poternpa, L.A.; Webster, R.O. Native and modified C-reactive protein bind different receptors on human neutrophils. Int. J. Biochem. Cell Biol. 2005, 37, 320–335. [Google Scholar] [CrossRef] [PubMed]
- Michowitz, Y.; Arbel, Y.; Wexler, D.; Sheps, D.; Rogowski, O.; Shapira, I.; Berliner, S.; Keren, G.; George, J.; Roth, A. Predictive value of high sensitivity CRP in patients with diastolic heart failure. Int. J. Cardiol. 2008, 125, 347–351. [Google Scholar] [CrossRef]
- Monneret, D.; Mestari, F.; Djiavoudine, S.; Bachelot, G.; Cloison, M.; Imbert-Bismut, F.; Bernard, M.; Hausfater, P.; Lacorte, J.M.; Bonnefont-Rousselot, D. Wide-range CRP versus high-sensitivity CRP on Roche analyzers: Focus on low-grade inflammation ranges and high-sensitivity cardiac troponin T levels. Scand. J. Clin. Lab. Investig. 2018, 78, 346–351. [Google Scholar] [CrossRef]
- Kondo, F.; Takegami, Y.; Ishizuka, S.; Hasegawa, Y.; Imagama, S. The association of the progression of knee osteoarthritis with high-sensitivity CRP in community-dwelling people-the Yakumo study. Clin. Rheumatol. 2021, 40, 2643–2649. [Google Scholar] [CrossRef]
- Tsuriya, D.; Morita, H.; Morioka, T.; Takahashi, N.; Ito, T.; Oki, Y.; Nakamura, H. Significant Correlation Between Visceral Adiposity and High-sensitivity C-reactive Protein (hs-CRP) in Japanese Subjects. Intern. Med. 2011, 50, 2767–2773. [Google Scholar] [CrossRef] [Green Version]
- Komulainen, P.; Lakka, T.A.; Kivipelto, M.; Hassinen, M.; Penttila, I.M.; Helkala, E.L.; Gylling, H.; Nissinen, A.; Rauramaa, R. Serum high sensitivity C-reactive protein and cognitive function in elderly women. Age Ageing 2007, 36, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Bisaria, S.; Terrigno, V.; Hunter, K.; Roy, S. Association of Elevated Levels of Inflammatory Marker High-Sensitivity C-Reactive Protein and Hypertension. J. Prim. Care Community Health 2020, 11, 8. [Google Scholar] [CrossRef]
- Kumar, R.; Porwal, Y.C.; Dev, N.; Kumar, P.; Chakravarthy, S.; Kumawat, A. Association of high-sensitivity C-reactive protein (hs-CRP) with non-alcoholic fatty liver disease (NAFLD) in Asian Indians: A cross-sectional study. J. Fam. Med. Prim. Care 2020, 9, 390–394. [Google Scholar] [CrossRef]
- Orlandi, M.; Muñoz Aguilera, E.; Marletta, D.; Petrie, A.; Suvan, J.; D’Aiuto, F. Impact of the treatment of periodontitis on systemic health and quality of life: A systematic review. J. Clin. Periodontol. 2021. [Google Scholar] [CrossRef]
- Choubaya, C.; Chahine, N.; Aoun, G.; Anil, S.; Zalloua, P.; Salameh, Z. Expression of Inflammatory Mediators in Periodontitis Over Established Diabetes: An Experimental Study in Rats. Med. Arch. 2021, 75, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Sondenaa, K.; Buan, B.; Soreide, J.A.; Nysted, A.; Andersen, E.; Nesvik, I.; Osland, A. Rapid C-reactive protein (CRP) measurements in the diagnosis of acute appendicitis. Scand. J. Clin. Lab. Investig. 1992, 52, 585–589. [Google Scholar] [CrossRef]
- Gibson, A.E.; Buchholz, A.C.; Martin Ginis, K.A. C-Reactive protein in adults with chronic spinal cord injury: Increased chronic inflammation in tetraplegia vs paraplegia. Spinal Cord 2008, 46, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Gorabi, A.M.; Abbasifard, M.; Imani, D.; Aslani, S.; Razi, B.; Alizadeh, S.; Bagheri-Hosseinabadi, Z.; Sathyapalan, T.; Sahebkar, A. Effect of curcumin on C-reactive protein as a biomarker of systemic inflammation: An updated meta-analysis of randomized controlled trials. Phytother. Res. 2022, 36, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Arbutina, D.D.; Milic, L.; Cuk, V.V.; Juloski, J.T.; Radulovic, R.; Starcevic, A.; Karamarkovic, A.R. Significance of Biomarkers in Early Diagnosis of Abdominal Sepsis. Chirurgia 2022, 117, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hu, Y.; Kuang, Z.; Chen, Y.; Xing, L.; Wei, W.; Xue, M.; Mu, S.; Tong, C.; Yang, Y.; et al. GPR174 mRNA Acts as a Novel Prognostic Biomarker for Patients With Sepsis via Regulating the Inflammatory Response. Front. Immunol. 2021, 12, 789141. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Askar, G.A.; Farghaly, H.S.; Ahmed, A.O.; Kamal, D.T.; Ahmed, S.S.; Mohamad, I.L. Accuracy of Cerebrospinal Fluid C-Reactive Protein and Multiplex Polymerase Chain Reaction and Serum Procalcitonin in Diagnosis of Bacterial and Viral Meningitis in Children. Acta Neurol. Taiwan 2022, 31, 61–71. [Google Scholar]
- Tao, M.; Zheng, D.; Liang, X.; He, Q.; Zhang, W. Diagnostic value of procalcitonin for bacterial infections in patients undergoing hemodialysis: A systematic review and meta-analysis. Ren. Fail. 2022, 44, 81–93. [Google Scholar] [CrossRef]
- Kusumaningrum, R.; Anam, M.S.; Dadiyanto, D.W.; Sidhartani, M.; Mexitalia, M. High sensitivity C-reactive protein level in various manifestations of tuberculosis in children. Paediatr. Indones. 2021, 61, 253–260. [Google Scholar] [CrossRef]
- Tong-Minh, K.; van der Does, Y.; Engelen, S.; de Jong, E.; Ramakers, C.; Gommers, D.; van Gorp, E.; Endeman, H. High procalcitonin levels associated with increased intensive care unit admission and mortality in patients with a COVID-19 infection in the emergency department. BMC Infect. Dis. 2022, 22, 165. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Shobeiri, P.; Kulasinghe, A.; Rezaei, N. Novel Systemic Inflammation Markers to Predict COVID-19 Prognosis. Front. Immunol. 2021, 12, 741061. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wu, Y.; Gao, Y.; Niu, X.; Li, J.; Tang, M.; Fu, C.; Qi, R.; Song, B.; Chen, H.; et al. Machine-learning based prediction of prognostic risk factors in patients with invasive candidiasis infection and bacterial bloodstream infection: A singled centered retrospective study. BMC Infect. Dis. 2022, 22, 150. [Google Scholar] [CrossRef]
- Guo, J.; Wu, Y.; Lai, W.; Lu, W.; Mu, X. The diagnostic value of (1,3)-β-D-glucan alone or combined with traditional inflammatory markers in neonatal invasive candidiasis. BMC Infect. Dis. 2019, 19, 716. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Marchinena, P.; Billordo-Peres, N.; Tobia-Gonzalez, I.; Jurado, A.; Damia, O.; Gueglio, G. High-sensitivity C-reactive protein as a predictor of locally advanced renal cell carcinoma. Arch. Esp. Urol. 2012, 65, 601–607. [Google Scholar]
- Lanki, M.; Seppanen, H.; Mustonen, H.; Salmiheimo, A.; Stenman, U.H.; Salmi, M.; Jalkanen, S.; Haglund, C. Pancreatic cancer survival prediction via inflammatory serum markers. Cancer Immunol. Immunother. 2022, 6, 1–6. [Google Scholar] [CrossRef]
- Suzuki, S.; Katagiri, R.; Yamaji, T.; Sawada, N.; Imatoh, T.; Ihira, H.; Inoue, M.; Tsugane, S.; Iwasaki, M.; Japan Public Hlth Ctr-based, P. Association between C-reactive protein and risk of overall and 18 site-specific cancers in a Japanese case-cohort. Br. J. Cancer 2022, 9, 1481–1489. [Google Scholar] [CrossRef]
- Sydenham, R.V.; Hansen, M.P.; Justesen, U.S.; Pedersen, L.B.; Aabenhus, R.M.; Wehberg, S.; Jarbøl, D.E. Factors associated with C-reactive protein testing when prescribing antibiotics in general practice: A register-based study. BMC Prim Care 2022, 23, 17. [Google Scholar] [CrossRef]
- Prins, H.J.; Duijkers, R.; van der Valk, P.; Schoorl, M.; Daniels, J.M.A.; van der Werf, T.S.; Boersma, W.G. CRP-guided antibiotic treatment in acute exacerbations of COPD in hospital admissions. Eur. Resp. J. 2019, 53, 10. [Google Scholar] [CrossRef]
- Hoffmann, K.; Leifheit, A.K.; Reichardt, B.; Maier, M. The antibiotic prescription and redemption gap and opportunistic CRP point-of-care testing. A cross-sectional study in primary health care from Eastern Austria. Wien. Klin. Wochen. 2013, 125, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, K.A.; Melbye, H.; Kelly, M.J.; Ceynowa, C.; Molstad, S.; Hood, K.; Butler, C.C. Influence of CRP testing and clinical findings on antibiotic prescribing in adults presenting with acute cough in primary care. Scand. J. Prim. Health Care 2010, 28, 229–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindstrom, J.; Nordeman, L.; Hagstrom, B. What a difference a CRP makes. A prospective observational study on how point-of-care C-reactive protein testing influences antibiotic prescription for respiratory tract infections in Swedish primary health care. Scand. J. Prim. Health Care 2015, 33, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Hart, P.C.; Rajab, I.M.; Alebraheem, M.; Potempa, L.A. C-Reactive Protein and Cancer-Diagnostic and Therapeutic Insights. Front. Immunol. 2020, 11, 595835. [Google Scholar] [CrossRef] [PubMed]
- Potempa, L.A.; Rajab, I.M.; Olson, M.E.; Hart, P.C. C-Reactive Protein and Cancer: Interpreting the Differential Bioactivities of Its Pentameric and Monomeric, Modified Isoforms. Front. Immunol. 2021, 12, 744129. [Google Scholar] [CrossRef] [PubMed]
- Siennicka, A. Association between microvesicles bearing monomeric C-reactive protein and platelet reactivity. Relationship with low response to antiplatelet drugs? J. Physiol. Pharmacol. 2021, 72. [Google Scholar] [CrossRef]
- Slevin, M.; Heidari, N.; Azamfirei, L. Monomeric C-Reactive Protein: Current Perspectives for Utilization and Inclusion as a Prognostic Indicator and Therapeutic Target. Front. Immunol. 2022, 13, 866379. [Google Scholar] [CrossRef]
- Moriarity, D.P.; Horn, S.R.; Kautz, M.M.; Haslbeck, J.M.B.; Alloy, L.B. How handling extreme C-reactive protein (CRP) values and regularization influences CRP and depression criteria associations in network analyses. Brain Behav. Immun. 2021, 91, 393–403. [Google Scholar] [CrossRef]
- Socha, M.W.; Malinowski, B.; Puk, O.; Wartęga, M.; Bernard, P.; Nowaczyk, M.; Wolski, B.; Wiciński, M. C-reactive protein as a diagnostic and prognostic factor of endometrial cancer. Crit. Rev. Oncol. Hematol. 2021, 164, 103419. [Google Scholar] [CrossRef]
- Ridker, P.M. C-reactive protein, inflammation, and cardiovascular disease: Clinical update. Tex. Heart. Inst. J. 2005, 32, 384–386. [Google Scholar]
- Wu, T.L.; Tsao, K.C.; Chang, C.P.Y.; Li, C.N.; Sun, C.F.; Wu, J.T. Development of ELISA on microplate for serum C-reactive protein and establishment of age-dependent normal reference range. Clin. Chim. Acta 2002, 322, 163–168. [Google Scholar] [CrossRef]
- Shields, M.J.; Siegel, J.N.; Clark, C.R.; Hines, K.K.; Potempa, L.A.; Gewurz, H.; Anderson, B. An appraisal of polystyrene-based (ELISA) and nitrocellulose-based (ELIFA) enzyme-immunoassay systems using monoclonal antibodies reactive toward antigenically distinct forms of human C-reactive protein. J. Immunol. Methods 1991, 141, 253–261. [Google Scholar] [CrossRef]
- Wei, W.R.; Tang, Y.Y.; He, H.M.; Gopinath, S.C.B.; Wang, L.L. Determination of cardiac disease biomarker by plasmonic sandwich ELISA. Biotechnol. Appl. Biochem. 2022, 6. [Google Scholar] [CrossRef]
- Vashist, S.K.; Czilwik, G.; van Oordt, T.; von Stetten, F.; Zengerle, R.; Schneider, E.M.; Luong, J.H.T. One-step kinetics-based immunoassay for the highly sensitive detection of C-reactive protein in less than 30 min. Anal. Biochem. 2014, 456, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhan, F.; Zhang, X.; Lin, S. Toll-like receptor-9 is involved in the development of B cell stimulating factor-induced systemic lupus erythematosus. Exp. Ther. Med. 2018, 15, 585–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elamir, A.M.; Senara, S.; Abdelghaffar, N.K.; Gaber, S.N.; El Sayed, H.S. Diagnostic role of lncRNA GAS5 and its genetic polymorphisms rs2067079, rs6790 and rs17359906 in rheumatoid arthritis. Biomed. Rep. 2021, 15, 93. [Google Scholar] [CrossRef] [PubMed]
- Ren, T.; Xiong, J.; Liu, G.; Wang, S.; Tan, Z.; Fu, B.; Zhang, R.; Liao, X.; Wang, Q.; Guo, Z. Imbalance of Th22/Treg cells causes microinflammation in uremic patients undergoing hemodialysis. Biosci. Rep. 2019, 39, BSR20191585. [Google Scholar] [CrossRef] [Green Version]
- Xing, Y.; Gao, Q.; Zhang, Y.M.; Ma, L.; Loh, K.Y.; Peng, M.L.; Chen, C.; Cui, Y.L. The improved sensitive detection of C-reactive protein based on the chemiluminescence immunoassay by employing monodispersed PAA-Au/Fe3O4 nanoparticles and zwitterionic glycerophosphoryl choline. J. Mat. Chem. B 2017, 5, 3919–3926. [Google Scholar] [CrossRef]
- Trifanescu, R.; Fica, S.; Dimuleselt, D.; Barbit, C.; Sirbu, A.; Rotaru, M.; Florea, S.; Purice, M.; Coculescu, M. Thyroid hormones and proinflammatory cytokines’ profile in amiodarone-induced thyrotoxicosis. Acta Endocrinol. 2007, 3, 417–435. [Google Scholar] [CrossRef]
- Fan, A.P.; Cao, Z.J.; Li, H.A.; Kai, M.; Lu, J.Z. Chemiluminescence Platforms in Immunoassay and DNA Analyses. Anal. Sci. 2009, 25, 587–597. [Google Scholar] [CrossRef] [Green Version]
- Denham, E.; Mohn, B.; Tucker, L.; Lun, A.; Cleave, P.; Boswell, D.R. Evaluation of immunoturbidimetric specific protein methods using the Architect ci8200: Comparison with immunonephelometry. Ann. Clin. Biochem. 2007, 44, 529–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mali, B.; Armbruster, D.; Serediak, E.; Ottenbreit, T. Comparison of immunoturbidimetric and immunonephelometric assays for specific proteins. Clin. Biochem. 2009, 42, 1568–1571. [Google Scholar] [CrossRef] [PubMed]
- Eckersall, P.D.; Conner, J.G.; Harvie, J. An immunoturbidimetric assay for canine reactive protein. Vet. Res. Commun. 1991, 15, 17–24. [Google Scholar] [CrossRef]
- Jinbo, T.; Hayashi, S.; Iguchi, K.; Shimizu, M.; Matsumoto, T.; Naiki, M.; Yamamoto, S. Development of monkey C-reactive protein (CRP) assay methods. Vet. Immunol. Immunopathol. 1998, 61, 195–202. [Google Scholar] [CrossRef]
- Pedersen, L.M.; Nordin, H.; Svensson, B.; Bliddal, H. Microalbuminuria in patients with rheumatoid-arthritis. Ann. Rheum. Dis. 1995, 54, 189–192. [Google Scholar] [CrossRef] [Green Version]
- Covin, M.A.; Gomez, R.R.; Suchodolski, J.S.; Steiner, J.M.; Lidbury, J.A. Analytical validation of a point-of-care test and an automated immunoturbidimetric assay for the measurement of canine C-reactive protein in serum. Can. J. Vet. Res. 2021, 85, 285–292. [Google Scholar]
- Dupuy, A.M.; Badiou, S.; Descomps, B.; Cristol, J.P. Immunoturbidimetric determination of C-reactive protein (CRP) and high-sensitivity CRP on heparin plasma. Comparison with serum determination. Clin. Chem. Lab. Med. 2003, 41, 948–949. [Google Scholar] [CrossRef]
- Berlanda, M.; Valente, C.; Bonsembiante, F.; Badon, T.; Bedin, S.; Contiero, B.; Guglielmini, C.; Poser, H. Evaluation of an automated immunoturbidimetric assay for detecting canine C-reactive protein. J. Vet. Diagn. Investig. 2020, 32, 948–952. [Google Scholar] [CrossRef]
- Hillström, A.; Hagman, R.; Tvedten, H.; Kjelgaard-Hansen, M. Validation of a commercially available automated canine-specific immunoturbidimetric method for measuring canine C-reactive protein. Vet. Clin. Pathol. 2014, 43, 235–243. [Google Scholar] [CrossRef]
- Klenner, S.; Bauer, N.; Moritz, A. Evaluation of three automated human immunoturbidimetric assays for the detection of C-reactive protein in dogs. J. Vet. Diagn. Investig. 2010, 22, 544–552. [Google Scholar] [CrossRef] [Green Version]
- Kiemle, J.; Hindenberg, S.; Bauer, N.; Roecken, M. Comparison of a point-of-care serum amyloid A analyzer frequently used in equine practice with 2 turbidimetric immunoassays used in human and veterinary medicine. J. Vet. Diagn. Investig. 2022, 34, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Veltman, E.M.; Lamers, F.; Comijs, H.C.; Stek, M.L.; van der Mast, R.C.; Rhebergen, D. Inflammatory markers and cortisol parameters across depressive subtypes in an older cohort. J. Affect. Disord. 2018, 234, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Thuillier, F.; Demarquilly, C.; Szymanowicz, A.; Gaillard, C.; Boniface, M.; Braidy, C.; Daunizeau, A.; Gascht, D.; Gruson, A.; Lagabrielle, J.F.; et al. Nephelometry or turbidimetry for the determination of albumin, ApoA, CRP, haptoglobin, IgM and transthyretin: Which choice? Ann. Biol. Clin. 2008, 66, 63–78. [Google Scholar] [CrossRef]
- Blirup-Jensen, S. Protein standardization III: Method optimization basic principles for quantitative determination of human serum proteins on automated instruments based on turbidimetry or nephelometry. Clin. Chem. Lab. Med. 2001, 39, 1098–1109. [Google Scholar] [CrossRef] [PubMed]
- Messiaen, A.S.; De Sloovere, M.M.W.; Claus, P.E.; Vercammen, M.; Van Hoovels, L.; Heylen, O.; Debrabandere, J.; Vanpoucke, H.; De Smet, D. Performance Evaluation of Serum Free Light Chain Analysis Nephelometry vs. Turbidimetry, Monoclonal vs Polyclonal Reagents. Am. J. Clin. Pathol. 2017, 147, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Zhmendak, D.; Mioulet, V.; King, D.P.; Burman, A.; Nfon, C.K. Combining a Universal Capture Ligand and Pan-Serotype Monoclonal Antibody to Develop a Pan-Serotype Lateral Flow Strip Test for Foot-and-Mouth Disease Virus Detection. Viruses 2022, 14, 785. [Google Scholar] [CrossRef]
- Tuells, J.; Parra-Grande, M.; Santos-Calle, F.J.; Montagud, A.C.; Egoavil, C.M.; Garcia-Rivera, C.; Caballero, P.; Gabaldon-Bravo, E.M.; Rodriguez-Diaz, J.C.; Hurtado-Sanchez, J.A. Detection of Neutralizing Antibodies against SARS-CoV-2 Post-Vaccination in Health Care Workers of a Large Tertiary Hospital in Spain by Using a Rapid Test LFIC and sVNT-ELISA. Vaccines 2022, 10, 510. [Google Scholar] [CrossRef]
- Tulloch, J.S.P.; Micocci, M.; Buckle, P.; Lawrenson, K.; Kierkegaard, P.; McLister, A.; Gordon, A.L.; Garcia-Finana, M.; Peddie, S.; Ashton, M.; et al. Enhanced lateral flow testing strategies in care homes are associated with poor adherence and were insufficient to prevent COVID-19 outbreaks: Results from a mixed methods implementation study. Age Ageing 2021, 50, 1868–1875. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Ding, M.Y.; Mao, Y.X.; Huang, X.Q.; Xie, X.H.; Song, L.J.; Qiao, M.W.; Zhang, J.W.; Wang, T.L.; Zhu, H.H.; et al. A comparative study of "turn-off’ mode and "turn-on" mode lateral flow immunoassay for T-2 toxin detection. Sens. Actuator B-Chem. 2022, 359, 10. [Google Scholar] [CrossRef]
- Lai, S.C.; Huang, Y.Y.; Wey, J.J.; Tsai, M.H.; Chen, Y.L.; Shu, P.Y.; Chang, S.F.; Hung, Y.J.; Hou, J.N.; Lin, C.C. Development of Novel Dengue NS1 Multiplex Lateral Flow Immunoassay to Differentiate Serotypes in Serum of Acute Phase Patients and Infected Mosquitoes. Front. Immunol. 2022, 13, 15. [Google Scholar] [CrossRef]
- Gebrecherkos, T.; Kiros, Y.K.; Challa, F.; Abdella, S.; Gebreegzabher, A.; Leta, D.; Desta, A.; Hailu, A.; Tasew, G.; Abdulkader, M.; et al. Longitudinal profile of antibody response to SARS-CoV-2 in patients with COVID-19 in a setting from Sub-Saharan Africa: A prospective longitudinal study. PLoS ONE 2022, 17, 18. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Kang, M.; Wu, S.Y.; Wu, L.J.; He, L.; Xiao, Y.L.; Zhang, W.L.; Liao, Q.F.; Deng, J.; Chen, Z.X.; et al. Evaluation of a Cryptococcus capsular polysaccharide detection FungiXpert LFA (lateral flow assay) for the rapid diagnosis of Cryptococcosis. Med. Mycol. 2022, 60, 8. [Google Scholar] [CrossRef] [PubMed]
- Mathers, J.; Poyner, C.; Thompson, D.; Rudge, G.; Pritchett, R.V. Exploration of the uptake of asymptomatic COVID-19 lateral flow testing in Birmingham, UK: Survey and qualitative research. BMJ Open 2022, 12, 10. [Google Scholar] [CrossRef]
- Davies, B.; Araghi, M.; Moshe, M.; Gao, H.; Bennet, K.; Jenkins, J.; Atchison, C.; Darzi, A.; Ashby, D.; Riley, S.; et al. Acceptability, Usability, and Performance of Lateral Flow Immunoassay Tests for Severe Acute Respiratory Syndrome Coronavirus 2 Antibodies: REACT-2 Study of Self-Testing in Nonhealthcare Key Workers. Open Forum Infect. Dis. 2021, 8, 7. [Google Scholar] [CrossRef]
- Panferov, V.G.; Byzova, N.A.; Zherdev, A.V.; Dzantiev, B.B. Peroxidase-mimicking nanozyme with surface-dispersed Pt atoms for the colorimetric lateral flow immunoassay of C-reactive protein. Microchim. Acta 2021, 188, 11. [Google Scholar] [CrossRef]
- Kong, D.Y.; Heo, N.S.; Kang, J.W.; Lee, J.B.; Kim, H.J.; Kim, M.I. Nanoceria-based lateral flow immunoassay for hydrogen peroxide-free colorimetric biosensing for C-reactive protein. Anal. Bioanal. Chem. 2022, 414, 3257–3265. [Google Scholar] [CrossRef]
- Galanis, P.P.; Katis, I.N.; He, P.J.W.; Iles, A.H.; Kumar, A.J.U.; Eason, R.W.; Sones, C.L. Laser-patterned paper-based flow-through filters and lateral flow immunoassays to enable the detection of C-reactive protein. Talanta 2022, 238, 10. [Google Scholar] [CrossRef]
- Pang, R.Z.; Zhu, Q.Y.; Wei, J.; Wang, Y.Q.; Xu, F.Q.; Meng, X.Y.; Wang, Z.X. Development of a gold-nanorod-based lateral flow immunoassay for a fast and dual-modal detection of C-reactive protein in clinical plasma samples. RSC Adv. 2021, 11, 28388–28394. [Google Scholar] [CrossRef]
- Sişman, A.R.; Küme, T.; Taş, G.; Akan, P.; Tuncel, P. Comparison and evaluation of two C-reactive protein assays based on particle-enhanced immunoturbidimetry. J. Clin. Lab. Anal. 2007, 21, 71–76. [Google Scholar] [CrossRef]
- Zhang, L.; Li, H.Y.; Li, W.; Shen, Z.Y.; Wang, Y.D.; Ji, S.R.; Wu, Y. An ELISA Assay for Quantifying Monomeric C-Reactive Protein in Plasma. Front. Immunol. 2018, 9, 511. [Google Scholar] [CrossRef]
- Salvo, P.; Dini, V.; Kirchhain, A.; Janowska, A.; Oranges, T.; Chiricozzi, A.; Lomonaco, T.; Di Francesco, F.; Romanelli, M. Sensors and Biosensors for C-Reactive Protein, Temperature and pH, and Their Applications for Monitoring Wound Healing: A Review. Sensors 2017, 17, 2952. [Google Scholar] [CrossRef] [Green Version]
- Noh, S.; Kim, J.; Kim, G.; Park, C.; Jang, H.; Lee, M.; Lee, T. Recent Advances in CRP Biosensor Based on Electrical, Electrochemical and Optical Methods. Sensors 2021, 21, 3024. [Google Scholar] [CrossRef]
- Imas, J.J.; Zamarreno, C.R.; Zubiate, P.; Sanchez-Martin, L.; Campion, J.; Matias, I.R. Optical Biosensors for the Detection of Rheumatoid Arthritis (RA) Biomarkers: A Comprehensive Review. Sensors 2020, 20, 6289. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, H.; Kordasht, H.K.; Pashazadeh-Panahi, P.; Nezhad-Mokhtari, P.; Hashemzaei, M.; Majidi, M.R.; Mosafer, J.; Oroojalian, F.; Mokhtarzadeh, A.; de la Guardia, M. Recent advances of electrochemical and optical biosensors for detection of C-reactive protein as a major inflammatory biomarker. Microchem J. 2020, 158, 14. [Google Scholar] [CrossRef]
- Balayan, S.; Chauhan, N.; Chandra, R.; Jain, U. Electrochemical Based C-Reactive Protein (CRP) Sensing Through Molecularly Imprinted Polymer (MIP) Pore Structure Coupled with Bi-Metallic Tuned Screen-Printed Electrode. Biointerface Res. Appl. Chem. 2022, 12, 7697–7714. [Google Scholar] [CrossRef]
- Tabrizi, M.A.; Acedo, P. Highly Sensitive RNA-Based Electrochemical Aptasensor for the Determination of C-Reactive Protein Using Carbon Nanofiber-Chitosan Modified Screen-Printed Electrode. Nanomaterials 2022, 12, 415. [Google Scholar] [CrossRef]
- Lakshmanakumar, M.; Nesakumar, N.; Sethuraman, S.; Rajan, K.S.; Krishnan, U.M.; Rayappan, J.B.B. Fabrication of GQD-Electrodeposited Screen-Printed Carbon Electrodes for the Detection of the CRP Biomarker. ACS Omega 2021, 6, 32528–32536. [Google Scholar] [CrossRef]
- Pohanka, M. Piezoelectric Immunosensor for the Determination of C-Reactive Protein. Int. J. Electrochem. Sci. 2019, 14, 8470–8478. [Google Scholar] [CrossRef]
- Kang, M.; Jeong, H.; Park, S.W.; Hong, J.; Lee, H.; Chae, Y.; Yang, S.; Ahn, J.H. Wireless graphene-based thermal patch for obtaining temperature distribution and performing thermography. Sci. Adv. 2022, 8, 8. [Google Scholar] [CrossRef]
- Anbalagan, B.; Anantha, S.K.; Kalpana, R. Novel Approach to Prognosis Parkinson’s Disease with Wireless Technology Using Resting Tremors. Wirel. Pers. Commun. 2022, 15, 1–15. [Google Scholar] [CrossRef]
- Yeh, C.T.; Barshilia, D.; Hsieh, C.J.; Li, H.Y.; Hsieh, W.H.; Chang, G.E. Rapid and Highly Sensitive Detection of C-Reaction Protein Using Robust Self-Compensated Guided-Mode Resonance BioSensing System for Point-of-Care Applications. Biosensors 2021, 11, 523. [Google Scholar] [CrossRef]
- Esposito, F.; Sansone, L.; Srivastava, A.; Baldini, F.; Campopiano, S.; Chiavaioli, F.; Giordano, M.; Giannetti, A.; Iadicicco, A. Real time and label-free detection of C-reactive protein in serum by long period grating in double cladding fiber. In Optical Sensors 2021; International Society for Optics and Photonics: Bellingham, WA, USA, 2021; Volume 11772, p. 117720Q. [Google Scholar] [CrossRef]
- Al-Enezi, E.; Vakurov, A.; Eades, A.; Ding, M.Y.; Jose, G.; Saha, S.; Millner, P. Affimer-Based Europium Chelates Allow Sensitive Optical Biosensing in a Range of Human Disease Biomarkers. Sensors 2021, 21, 831. [Google Scholar] [CrossRef] [PubMed]
- Petrou, P.; Koukouvinos, G.; Drygiannakis, D.; Goustouridis, D.; Raptis, I.; Misiakos, K.; Kakabakos, S.E. Real-time multi-analyte label-free detection of proteins by white light-reflectance spectroscopy. In Conference on Microfluidics, BioMEMS, and Medical Microsystems XII; International Society for Optics and Photonics: Bellingham, WA, USA, 2014; Volume 8976, p. 8976. [Google Scholar] [CrossRef]
- Koukouvinos, G.; Goustouridis, D.; Misiakos, K.; Kakabakos, S.; Raptis, I.; Petrou, P. Rapid C-reactive protein determination in whole blood with a White Light Reflectance Spectroscopy label-free immunosensor for Point-of-Care applications. Sens. Actuator B-Chem. 2018, 260, 282–288. [Google Scholar] [CrossRef]
- Tsounidi, D.; Koukouvinos, G.; Christianidis, V.; Legaki, E.; Giogli, V.; Panagiotopoulou, K.; Taka, S.; Ekaterinidi, Z.; Kakabakos, S.; Raptis, I.; et al. Development of a Point-of-Care System Based on White Light Reflectance Spectroscopy: Application in CRP Determination. Biosensors 2021, 11, 268. [Google Scholar] [CrossRef] [PubMed]
- Li, S.F.; Floriano, P.N.; Christodoulides, N.; Fozdar, D.Y.; Shao, D.B.; Ali, M.F.; Dharshan, P.; Mohanty, S.; Neikirk, D.; McDevitt, J.T.; et al. Disposable polydimethylsiloxane/silicon hybrid chips for protein detection. Biosens. Bioelectron. 2005, 21, 574–580. [Google Scholar] [CrossRef]
- Kim, C.H.; Ahn, J.H.; Kim, J.Y.; Choi, J.M.; Lim, K.C.; Park, T.J.; Heo, N.S.; Lee, H.G.; Kim, J.W.; Choi, Y.K. CRP detection from serum for chip-based point-of-care testing system. Biosens. Bioelectron. 2013, 41, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Yoon, D.; Kim, T.S. The Mach-Zehnder Interferometer Based on Silicon Oxides for Label Free Detection of C-reactive Protein (CRP). BioChip J. 2009, 3, 1–11. [Google Scholar]
- Choi, H.W.; Sakata, Y.; Kurihara, Y.; Ooya, T.; Takeuchi, T. Label-free detection of C-reactive protein using reflectometric interference spectroscopy-based sensing system. Anal. Chim. Acta. 2012, 728, 64–68. [Google Scholar] [CrossRef]
- Psarouli, A.; Botsialas, A.; Salapatas, A.; Stefanitsis, G.; Nikita, D.; Jobst, G.; Chaniotakis, N.; Goustouridis, D.; Makarona, E.; Petrou, P.S.; et al. Fast label-free detection of C-reactive protein using broad-band Mach-Zehnder interferometers integrated on silicon chips. Talanta 2017, 165, 458–465. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Feature | Specifications of CRP | References |
|---|---|---|
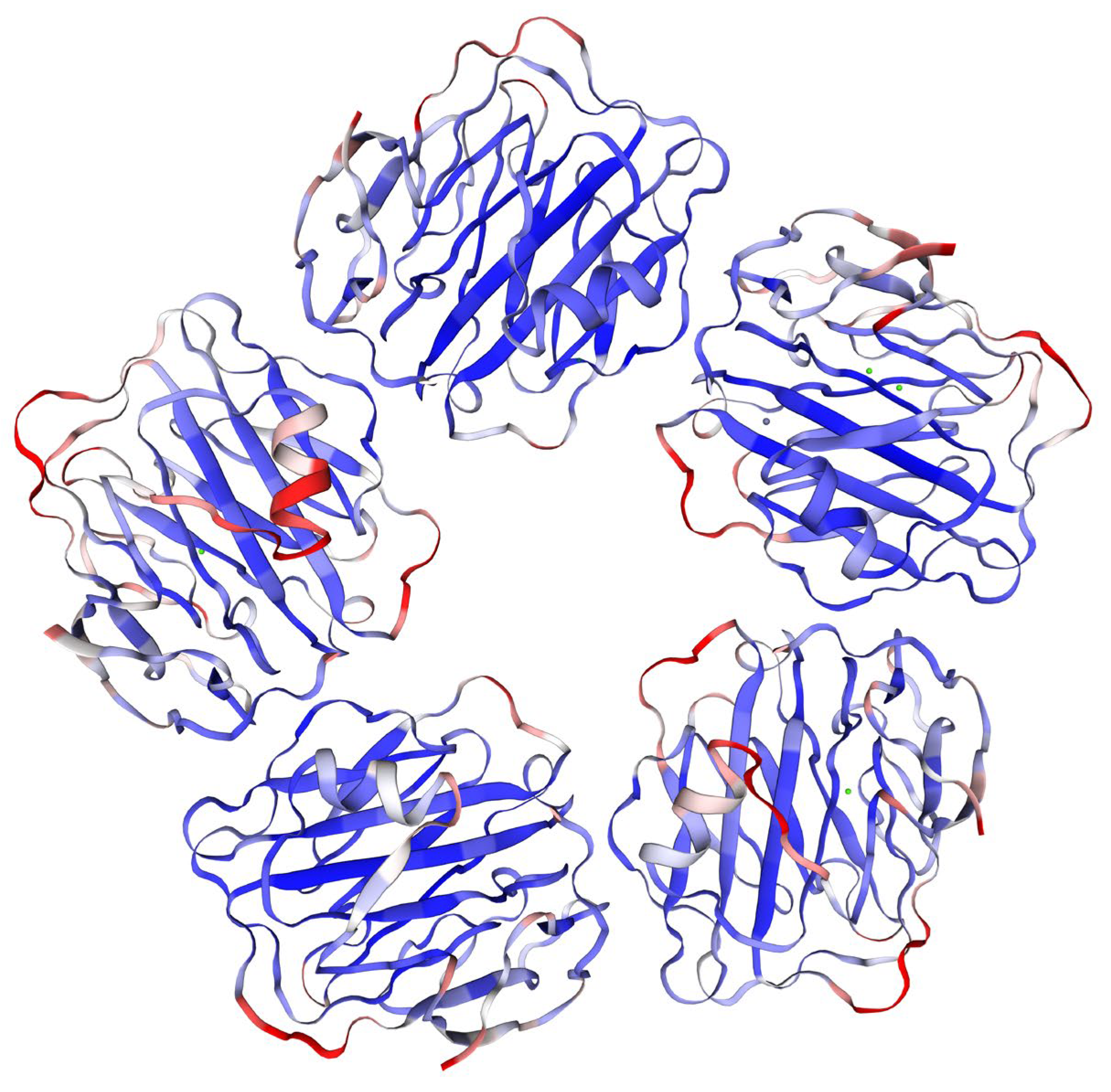
| Structure | protein with five identical subunits each sized 206 amino acids | [16,17,18] |
| Size | 120 kDa (human origin, pentameric structure) | [16] |
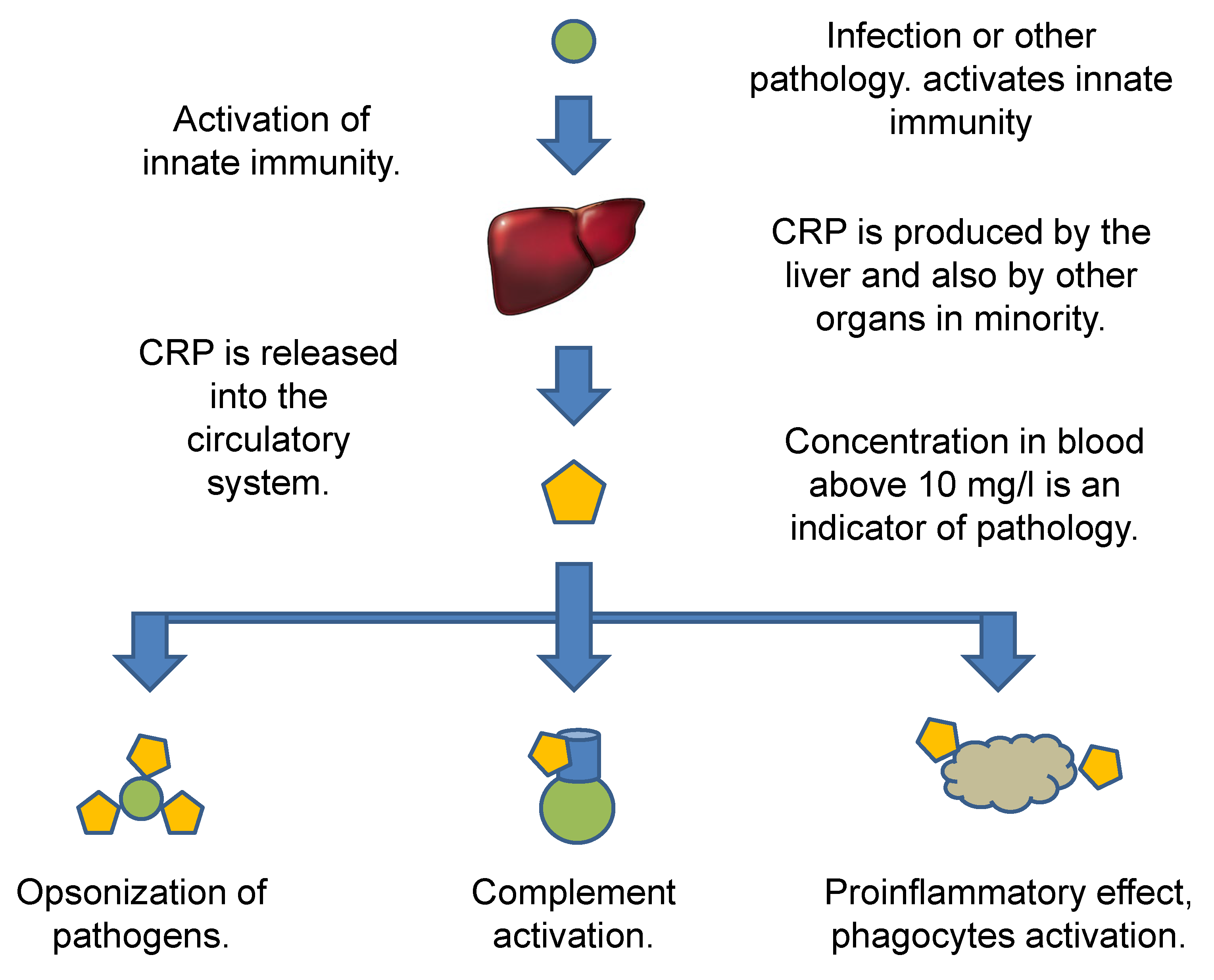
| Occurrence and major source | dominantly produced by hepatocytes and released into the blood | [28,29] |
| Minor producers | macrophages, lymphocytes, adipocytes, smooth muscle cells, and epithelial cells | [27] |
| Role in the organism | opsonization of pathogens and other target cells, a part of inflammatory reaction, involved in both classic and alternative complements, and activation of leukocytes | [30,31,32] |
| Increased level—typical marker | chronic and systemic inflammation, bacterial infection | [40,45,46,49,50,51] |
| Examples of other relevant reasons for an increased level | heart failures and cardiovascular diseases, osteoarthritis, visceral adiposity, alcohol intake, and some dementias, non-alcoholic fatty liver disease, periodontitis, appendicitis, sepsis, some viral infections such as severe coronavirus disease 2019, candidiasis, and some types of cancer | [35,36,37,38,40,41,42,43,44,47,48,52,53,54,55,56,57,58] |
| Blood concentrations—typical threshold levels | concentrations under 10 mg/L are taken for normal and levels above 10 mg/L are indicators of pathology | [68] |
| Other threshold levels and thresholds for hsCRP tests | under 1 mg/L of blood, CRP is a low risk of pathologies such as cardiovascular disorders, 1–3 mg/L is a moderate risk, and a high risk starts at CRP blood levels above 3 mg/L | [70] |
| Assay Principle | User | Quantification | Limit of Detection and Applicability Range | Time Per One Assay | Declared Accuracy |
|---|---|---|---|---|---|
| ELISA, CLIA | standard and small laboratories | yes | 5 ng/L; 5 ng/L to 50 µg/L | 90 min up to one day | relative standard error of 1.5%, inter-assay precision up to 15% |
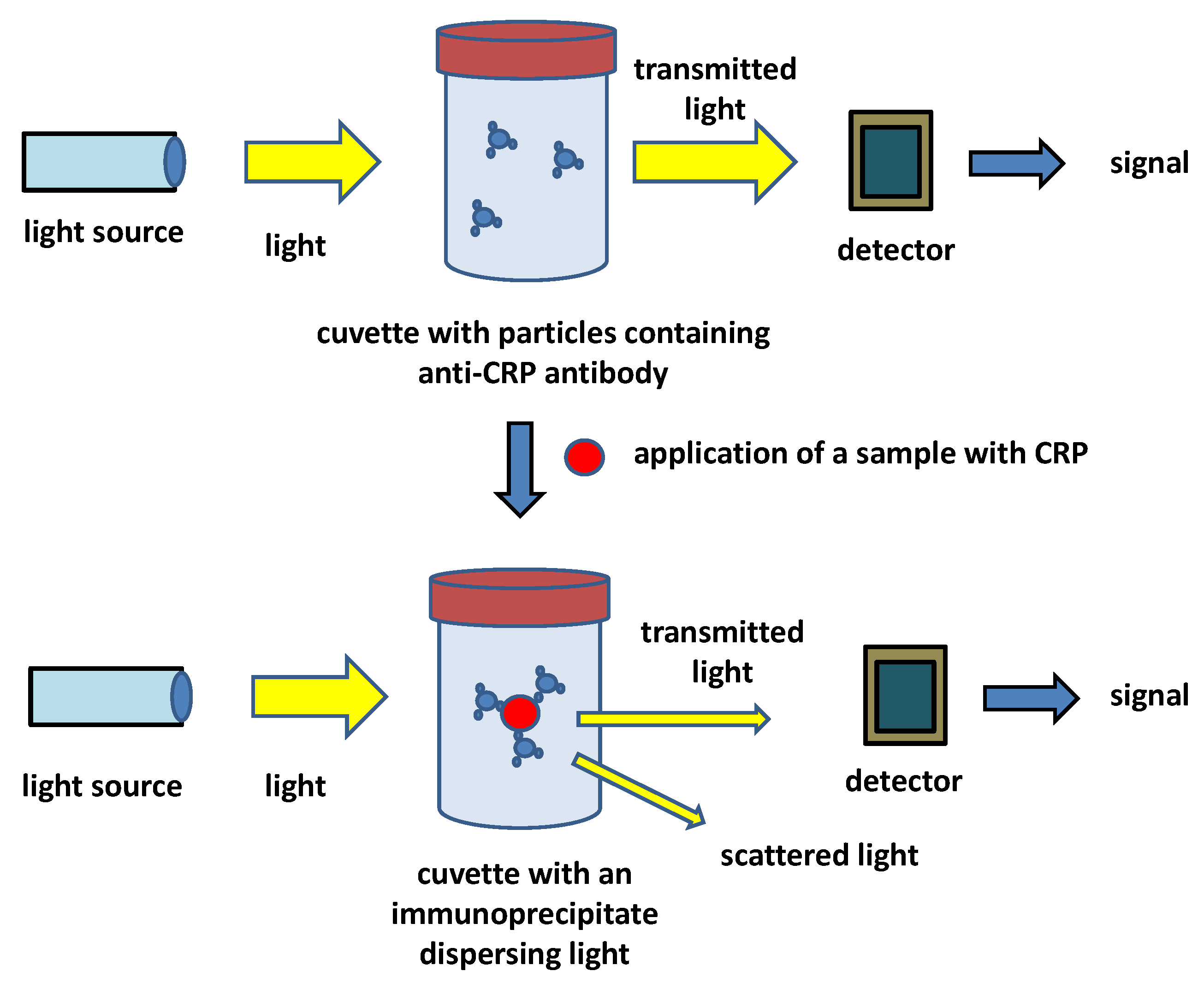
| Immunoturbidimetry | Small laboratories, physician offices, point-of-care conditions | yes | 2 mg/L; 2 to 150 mg/L | 5 to 15 min | relative standard error 4%, inter-assay precision 10% |
| Lateral flow tests | physician offices, point-of-care conditions, marginal in laboratories | no or semiquantitative | 2.5 mg/L; 2.5 to 200 mg/L | 15 min | relative standard error of 15%, inter-assay precision around 20% |
| Assay Principle | Recognition Part | Sensor Platform | Limits of detection and Other Reported Specifications | References |
|---|---|---|---|---|
| Impedimetry, cyclic voltammetry | Molecularly imprinted polymer: CRP imprinted into methacrylate membrane | screen-printed electrodes with metallic nanoparticles | limit of detection 120 µg/L | [115] |
| Square wave voltammetry | RNA aptamer | screen-printed electrodes with chitosan containing carbon nanofibers and methylene blue | linear range 120 ng/L–1.8 µg/L, limit of detection 44 ng/L | [116] |
| Differential pulse voltammetry | anti-CRP antibody | screen-printed carbon electrodes sprayed and electrodeposited with graphene quantum dots | linearity 0.05–10 µg/L, limit of quantification 0.072 µg/L, limit of detection 0.024 µg/L | [117] |
| Piezoelectric | anti-CRP antibody | quartz crystal microbalance | limit of detection 0.08 mg/L | [118] |
| Optical guided-mode resonance | anti-CRP antibody | guided-mode resonance optofluidic biosensing system | limit of detection 19.5 µg/L, assay time 20 min | [121] |
| Optical long-period fiber grating | anti-CRP antibody | optical fiber | limit of detection 0.15 µg/L and working range 1 µg/–100 mg/L | [122] |
| Fluorimetric bioassay | affimer: Eu3+ ions chelated by a modified synthetic protein | fluorimetry | limit of detection 1.2 pg/L, applicable range 1.2 pg/L–1.2 µg/L, time of an assay 2–3 min | [123] |
| White light reflectance spectroscopy | anti-CRP antibody | light reflectance spectroscopy | dynamic range for 0.05–200 mg/L, limit of detection 1 µg/L | [126] |
| Mach–Zehnder interferometry | anti-CRP antibody | silicon chip as a part of Mach–Zehnder interferometer | limit of detection 2.1 µg/L, one assay cycle 12 min | [131] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pohanka, M. Diagnoses Based on C-Reactive Protein Point-of-Care Tests. Biosensors 2022, 12, 344. https://doi.org/10.3390/bios12050344
Pohanka M. Diagnoses Based on C-Reactive Protein Point-of-Care Tests. Biosensors. 2022; 12(5):344. https://doi.org/10.3390/bios12050344
Chicago/Turabian StylePohanka, Miroslav. 2022. "Diagnoses Based on C-Reactive Protein Point-of-Care Tests" Biosensors 12, no. 5: 344. https://doi.org/10.3390/bios12050344
APA StylePohanka, M. (2022). Diagnoses Based on C-Reactive Protein Point-of-Care Tests. Biosensors, 12(5), 344. https://doi.org/10.3390/bios12050344