In Situ Investigation of Upper Airway Occlusion in Sleep Disordered Breathing Using Ultrasonic Transducer Arrays


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
- Known or been diagnosed to have a sensitivity to ultrasonic gel or mineral oil (baby oil);
- Known or been diagnosed to have abnormal growth or tumor in or near the upper airway;
- Difficulty with swallowing;
- Known or been diagnosed to have insomnia;
- Known or suspected of having neurological disorders that may mediate SDB;
- Known or suspected of having cardiovascular conditions that may increase patient risk during the study.
2.2. Patient Demography
2.3. Full Night NPSG Sleep Study
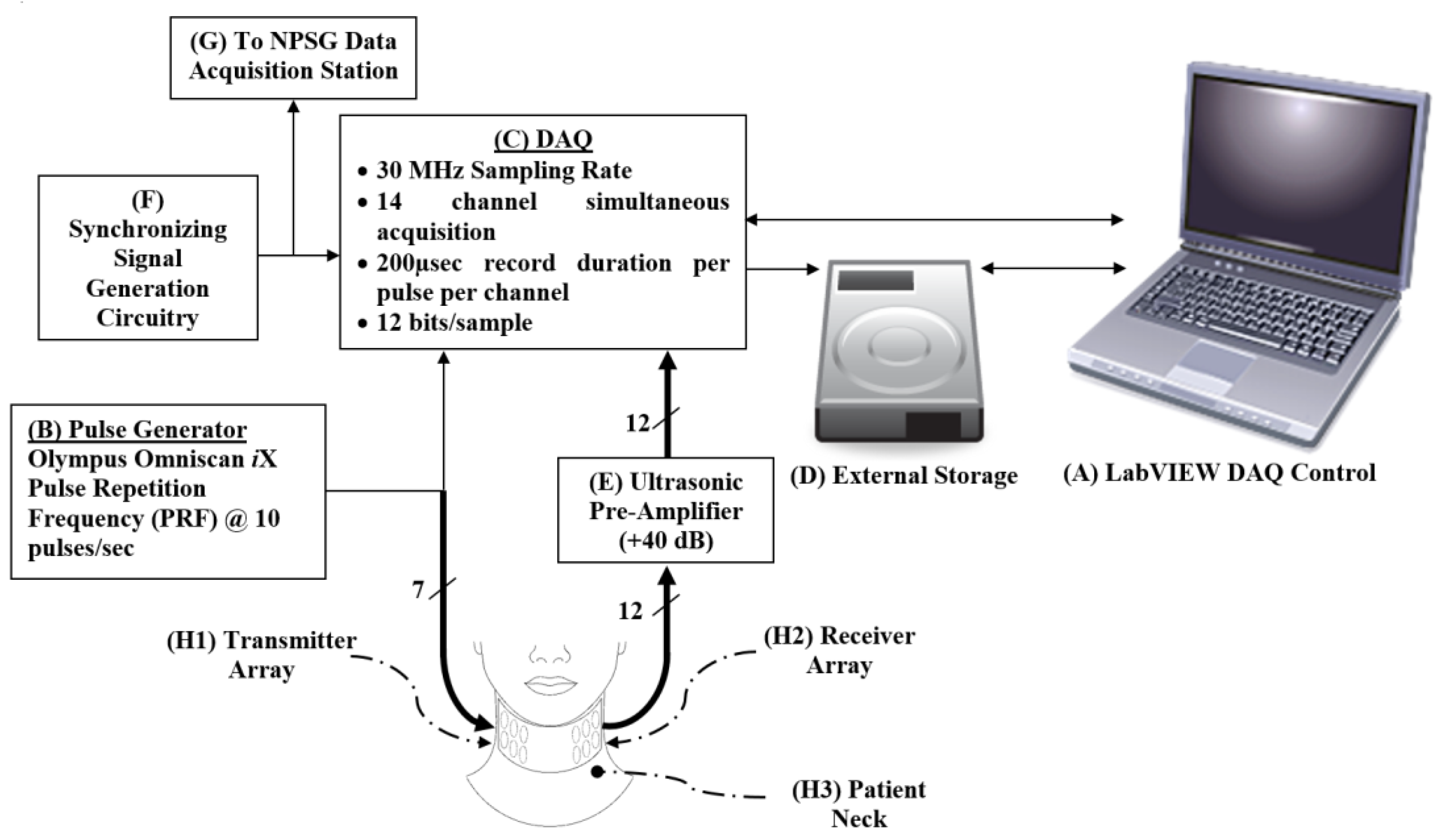
2.4. Experimental Setup
2.4.1. Transmitter and Receiver Arrays
- Considering the neck curvature, the sensors must have a small surface while being large enough for handling and assembly;
- The curvature of the neck also requires the receivers’ ability to detect the ultrasonic pulses at either normal or oblique incidence;
- The heterogeneity of the tissue media (i.e., skin, fat, muscle, bone, cartilage, air, etc.);
- The main site of occlusion differs between patients, which requires a longitudinal array of sensors, pulsed simultaneously, to capture the occlusion when it occurs and to allow reception spatial resolution to estimate the location of the occlusion.
- The housing of the sensor arrays must be flexible to adhere to the neck curvature, allowing complete contact between the sensors and the skin;
- The sensor array housing must allow for a full night study, which includes the patient’s movement and avoids repeated application of the acoustic gel.
2.4.2. Pulse Generator
2.4.3. Acoustic Pre-Amplifier
2.4.4. Data Acquisition (DAQ) Station
2.4.5. Practical Considerations
2.5. Study Protocol
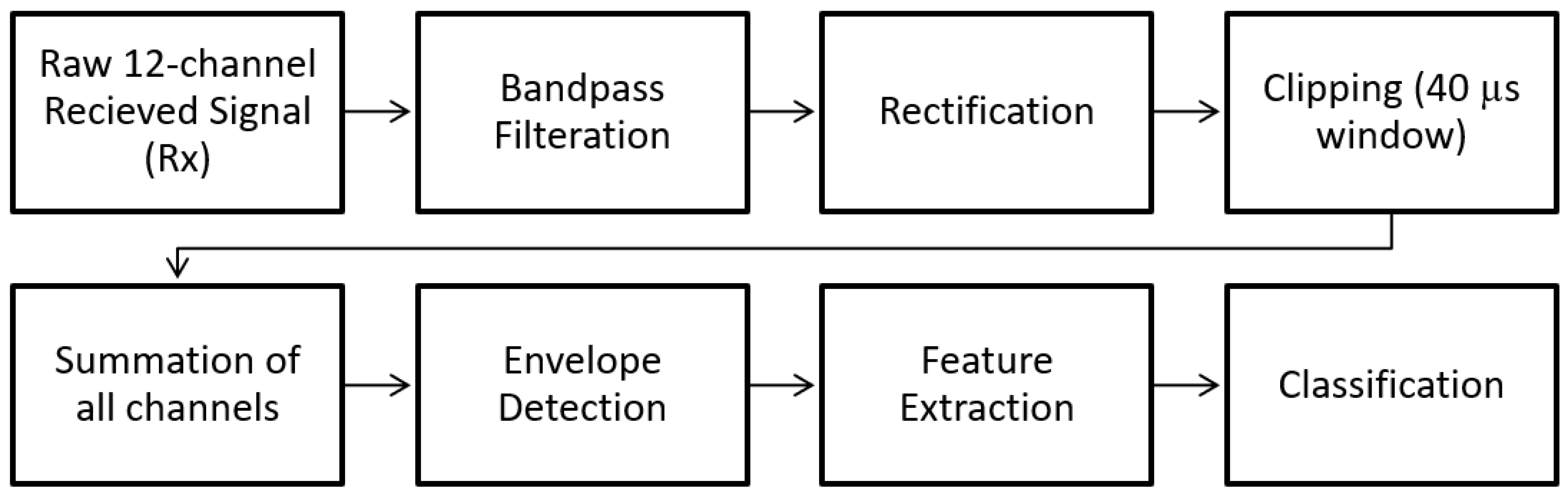
2.6. Post-Processing
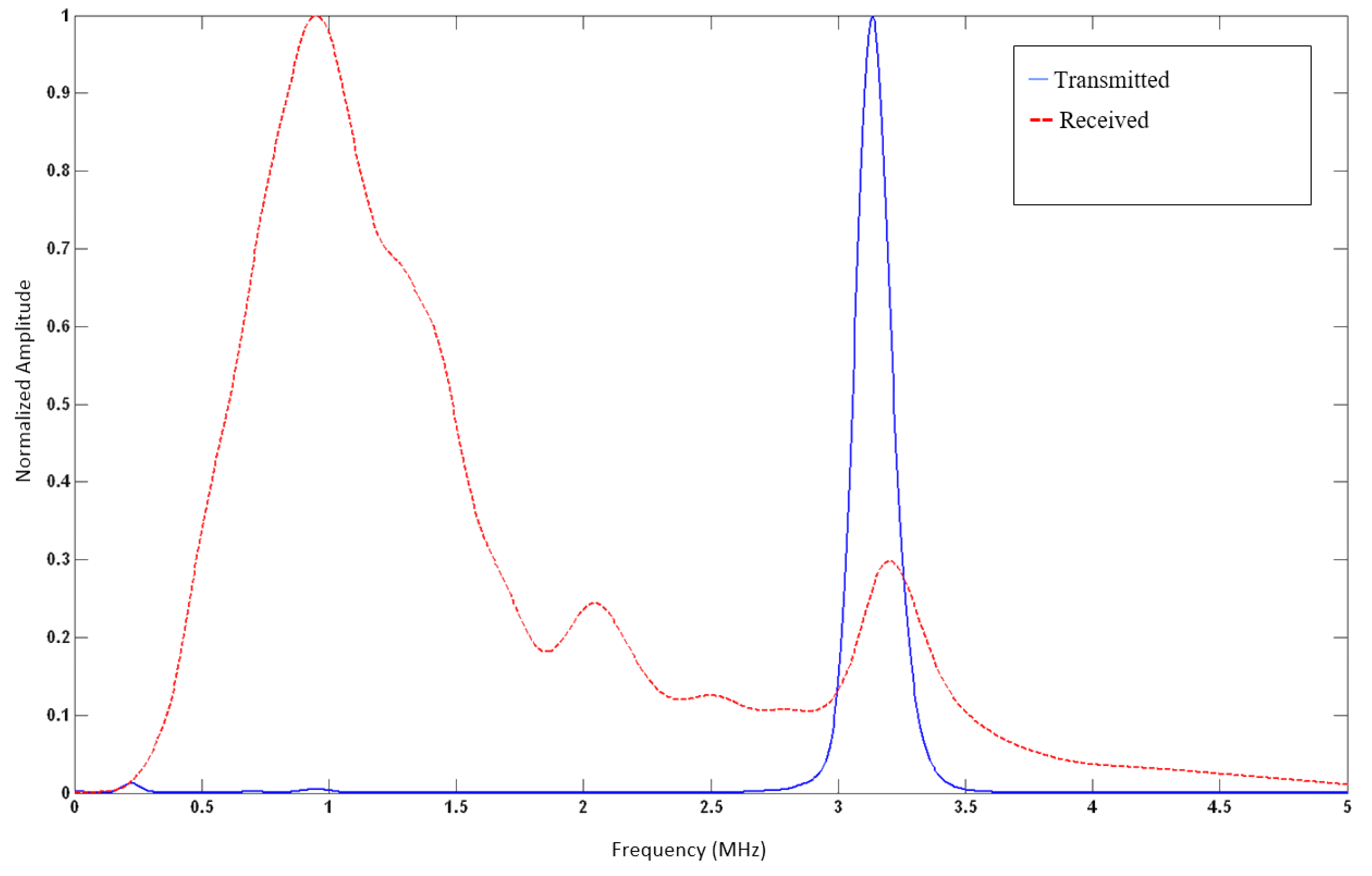
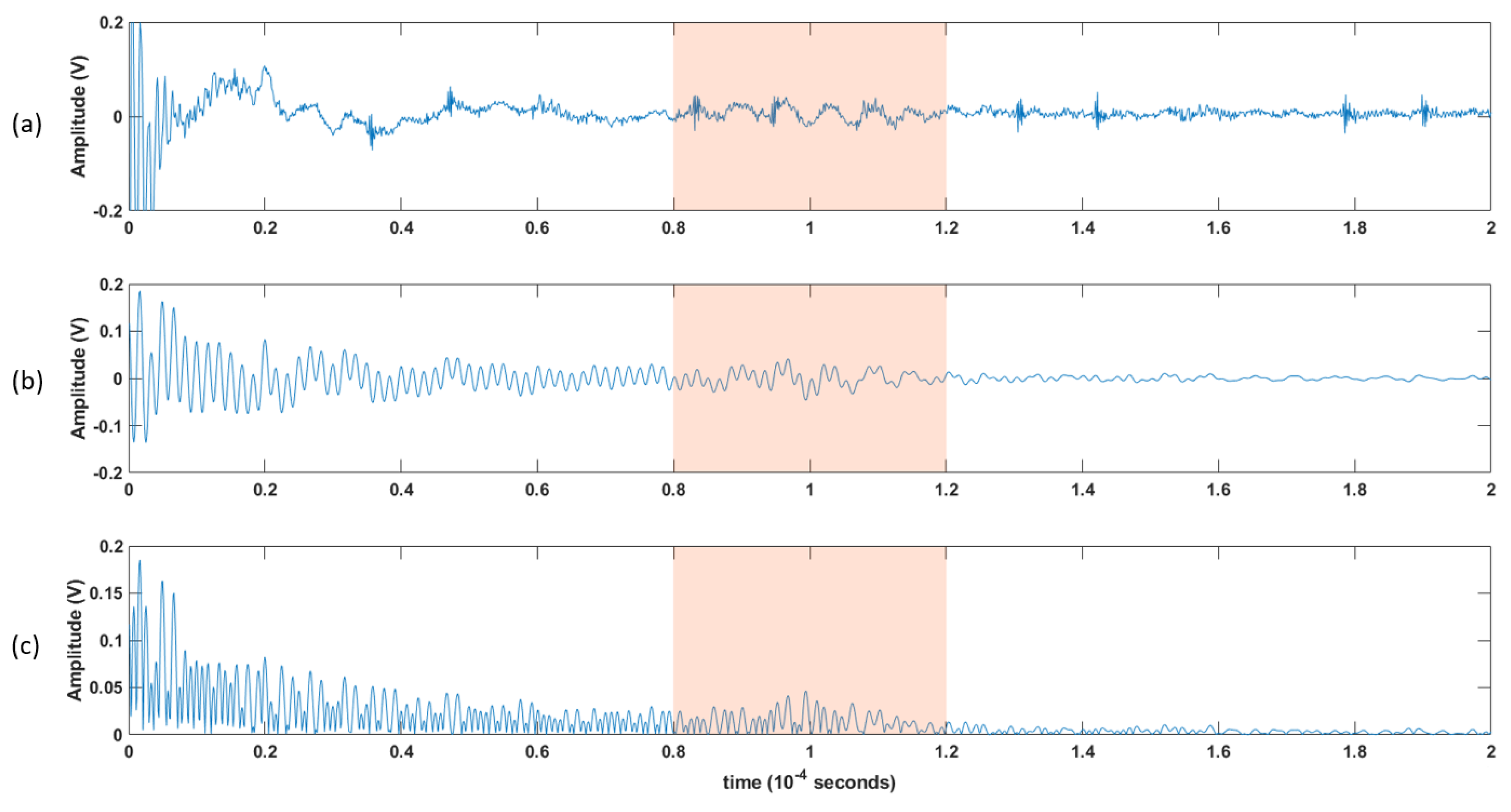
- Each channel was filtered using a Kaiser finite impulse response (FIR) zero-shift bandpass filter, with a lower cutoff frequency of 0.15 MHz and an upper cutoff frequency of 2 MHz. This removed the high-frequency noise, and the baseline was wandering.
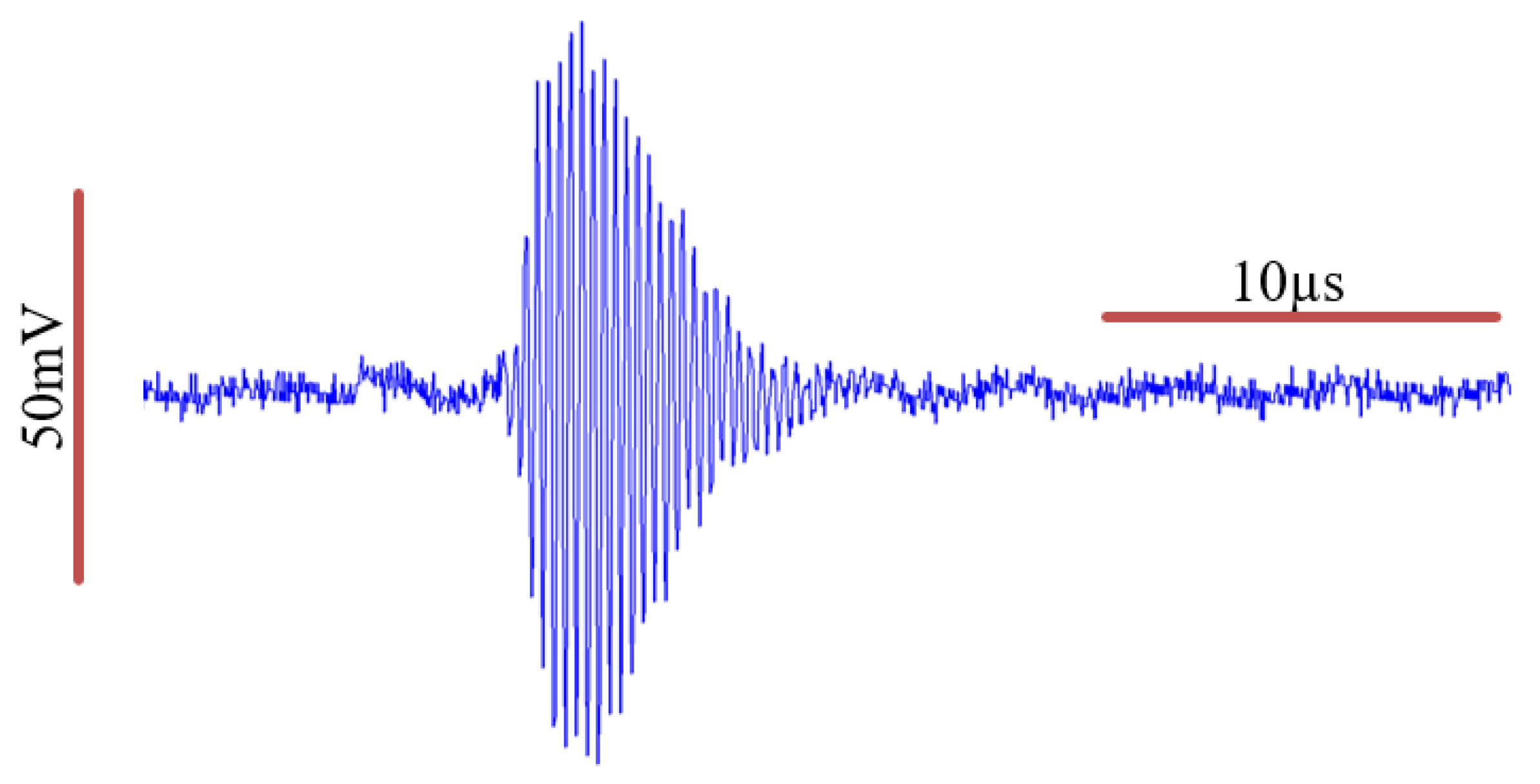
- As the receiver array does not capture any signals until the ultrasonic pulse has traveled the distance representing the diameter of the neck, the first 80 µs (12cm) of the recorded signal does not carry any information. Hence, a 40 µs “window of interest” spanning 80–120 µs was clipped from the 200 µs record. This generalized period represents a signal travel distance of 12–18 cm in the neck. This window corresponds to the expected period of the arrival of the received ultrasonic signal.
- It is assumed here that changes in the upper airway shape occur at a slower rate than the rate of pulses passing through the airway at 10 pulses per second. Hence, the received signal from every 10 pulses was summed, creating a single waveform per second.
- Furthermore, the waveforms collected from the channels were added together, resulting in one waveform per second.
- A cubic spline, sampled at a rate of 30 MHz, was used to estimate the envelope of the resultant waveform connecting the peaks of the resulting signal from the previous step.
- The envelope was the basis from which temporal and spectral features were extracted, as discussed in the following section.
2.7. Feature Extraction
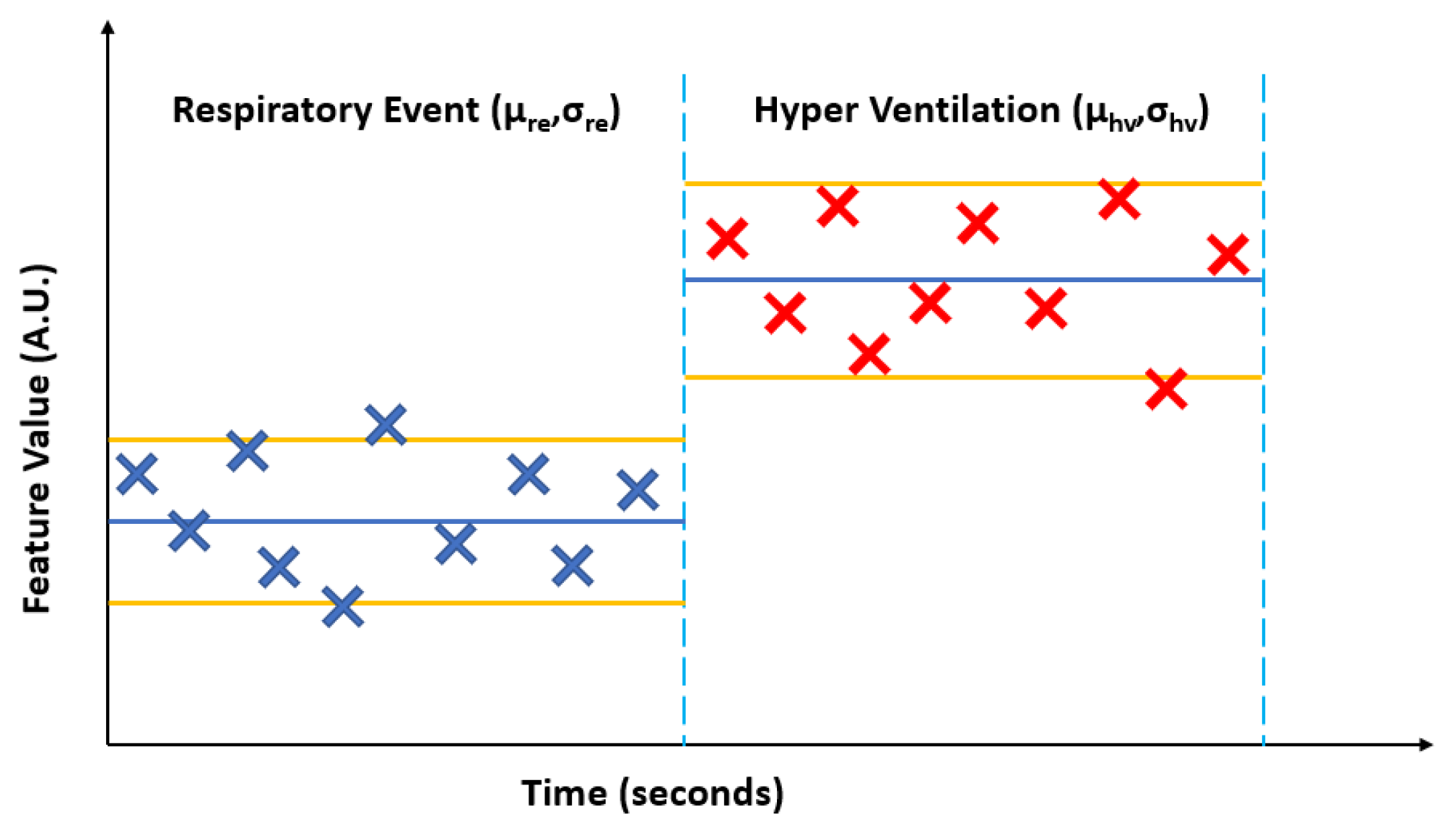
2.8. Respiratory Event Epoch Clipping
2.9. Hypothesis Formulation
2.10. Statistical Analysis and Hypothesis Testing
- Normalizing each feature for the subsequent breathing period to the preceding respiratory event, allowing for normalized intra- and inter-subject comparisons.
- Introduction of two-tail null-hypothesis testing: If there are no changes in the calculated features between the preceding and succeeding breathing periods in each clip, then the logarithm of the ratio is expected to be equal to zero. If there are changes, then the logarithm of the ratio will be ≠ 0.
3. Results
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Fifth Edition. 2016. Available online: https://apps.who.int/iris/handle/10665/246208 (accessed on 15 August 2022).
- Broderick, M.; Guilleminault, C. Neurological aspects of Obstructive Sleep Apnea. Ann. N. Y. Acad. Sci. 2008, 1142, 44–57. [Google Scholar] [CrossRef]
- Eckert, D.J.; Malhotra, A. Pathophysiology of adult Obstructive Sleep Apnea. Proc. Am. Thorac. Soc. 2008, 5, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J. International classification of sleep disorders. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Fogel, R.B.; Malhotra, A.; White, D.P. Sleep 2: Pathophysiology of Obstructive Sleep Apnoea/Hypopnoea syndrome. Thorax 2004, 59, 159–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, R.; Watenpaugh, D.E. Obesity and obstructive sleep apnea: Or is it OSA and obesity? Pathophysiology 2008, 15, 71–77. [Google Scholar] [CrossRef]
- Peppard, P.E.; Young, T.; Palta, M.; Dempsey, J.; Skatrud, J. Longitudinal study of moderate weight change and sleep-disordered breathing. J. Am. Med. Assoc. 2000, 284, 3015–3021. [Google Scholar] [CrossRef] [Green Version]
- Punjabi, N.M. The epidemiology of adult Obstructive Sleep Apnea. Proc. Am. Thorac. Soc. 2008, 5, 136–143. [Google Scholar] [CrossRef]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of Obstructive Sleep Apnea: A population health perspective. Am. J. Respir. Crit. Care Med. 2002, 165, 1217–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, B.A.; Wellman, A.; Owens, R.L. Psgs: More than just the ahi. J. Clin. Sleep. Med. 2013, 9, 527–528. [Google Scholar] [CrossRef] [Green Version]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef]
- Flemons, W.W.; Douglas, N.J.; Kuna, S.T.; Rodenstein, D.O.; Wheatley, J. Access to diagnosis and treatment of patients with suspected sleep apnea. Am. J. Respir. Crit. Care Med. 2004, 169, 668–672. [Google Scholar] [CrossRef]
- Young, T.; Palta, M.; Dempsey, J.; Peppard, P.E.; Nieto, F.J.; Hla, K.M. Burden of Sleep Apnea: Rationale, design, and major findings of the Wisconsin Sleep Cohort Study. Wis. Med. J. 2009, 108, 246–249. [Google Scholar]
- White, D.P. Sleep Apnea. Proc. Am. Thoraic Soc. 2006, 3, 124–128. [Google Scholar] [CrossRef]
- Agur, A.M.R.; Lee, M.J. Grant’s Atlas of Anatomy, 10th ed.; Kelly, P.J., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1999. [Google Scholar]
- Rodenstein, D.O.; Dooms, G.; Thomas, Y.; Liistro, G.; Stanescu, D.C.; Culee, C.; Aubert-Tulkens, G. Pharyngeal shape and dimensions in healthy subjects, snorers, and patients with Obstructive Sleep Apnoea. Thorax 1990, 45, 722–727. [Google Scholar] [CrossRef] [Green Version]
- Schwab, R.J.; Pasirstein, M.; Pierson, R.; Mackley, A.; Hachadoorian, R.; Arens, R.; Maislin, G.; Pack, A.I. Identification of upper airway anatomic risk factors for Obstructive Sleep Apnea with volumetric magnetic resonance imaging. Am. J. Respir. Crit. Care Med. 2003, 168, 522–530. [Google Scholar] [CrossRef]
- Martins, A.B.; Tufik, S.; Moura, S.M.G.P.T. Physiopathology of Obstructive Sleep Apnea-Hypopnea Syndrome. J. Bras. De Pneumol. 2007, 33, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Rama, A.N.; Tekwani, S.H.; Kushida, C.A. Sites of obstruction in Obstructive Sleep Apnea. Chest 2002, 122, 1139–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faber, C.E.; Grymer, L. Available techniques for objective assessment of upper airway narrowing in snoring and Sleep Apnea. Sleep Breath. 2003, 7, 77–86. [Google Scholar] [CrossRef]
- Maturo, S.C.; Mair, E.A. Submucosal minimally invasive lingual excision: An effective, novel surgery for pediatric tongue base reduction. Ann. Otol. Rhinol. Laryngol. 2006, 115, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Lewis, R.; Norton, A.; McPeake, S. Ultrasound-guided radiofrequency submucosal tongue-base excision for Sleep Apnoea: A preliminary report. Clin. Otolaryngol. Allied Sci. 2003, 28, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Quistgaard, J. Signal acquisition and processing in medical diagnostic ultrasound. IEEE Signal Process. Mag. 1997, 14, 67–74. [Google Scholar] [CrossRef]
- Hedrick, W.R.; Hykes, D.L.; Starchman, D.E. Ultrasound Physics and Instrumentation, 4th ed.; Elsevier Mosby: St. Louis, MO, USA, 2005. [Google Scholar]
- Cobbold, R.S. Foundations of Biomedical Ultrasound, 1st ed.; Biomedical Engineering; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Al-Abed, M.; Antich, P.; Watenpaugh, D.E.; Behbehani, K.E. Detection of airway occlusion in simulated Obstructive Sleep Apnea/Hypopnea using ultrasound: An in vitro study. In Proceedings of the 32nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010. [Google Scholar]
- Al-Abed, M.; Behbehani, K.; Antich, P.; Watenpaugh, D.; Burk, J. Systems and Methods for Detecting Airway Occlusion. U.S. Patent Application No 13/588,819, 19 October 2013. [Google Scholar]
- Boudewyns, A.; Sforza, E.; Zamagni, M.; Krieger, J. Respiratory effort during Sleep Apneas after interruption of long-term Cpap treatment in patients with Obstructive Sleep Apnea. Chest 1996, 110, 120–127. [Google Scholar] [CrossRef]
- Al-Abed, M.; Antich, P.; Watenpaugh, D.E.; Behbehani, K. In Vivo characterization of ultrasonic sensors for the detection of airway occlusion in sleep disordered breathing. In Proceedings of the 33rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011. [Google Scholar]
- Al-Abed, M.A. Non-Invasive Detection of Upper Airway Occlusion Using Piezoelectric Ultrasonic Sensors in Sleep Apnea Patients. Ph.D. Thesis, The University of Texas at Arlington, Arlington, TX, USA, 2011. [Google Scholar]
- Al-Abed, M.; Antich, P.; Watenpaugh, D.E.; Behbehani, K. Phantom study evaluating detection of simulated upper airway occlusion using piezoelectric ultrasound transducers. Comput. Biol. Med. 2017, 89, 325–336. [Google Scholar] [CrossRef]
- Al-Abed, M.A.; Antich, P.; Watenpaugh, D.E.; Behbehani, K. Upper airway occlusion detection using a novel ultrasound technique. In Proceedings of the Engineering in Medicine and Biology Society (EMBC), 2012 Annual International Conference of the IEEE, San Diego, CA, USA, 28 August–1 September 2012. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Stats |
|---|---|
| Patients (Number, Gender) | 2 Females, 7 Males |
| Age (years) (mean ± SD) | 41.9 ± 10.6 |
| Height (m) (mean ± SD) | 1.75 ± 0.14 |
| Weight (kg) (mean ± SD) | 114.8 ± 25.5 |
| Neck measurement (cm, coronal) (mean ± SD) | 15.2 ± 1.1 |
| BMI (kg/m2) (mean ± SD) | 37.6 ± 6.6 |
| Total Sleep Period (min) (mean ± SD) | 368.7 ± 75.7 |
| Total Sleep Time (min) (mean ± SD) | 270.3 ± 68.3 |
| Sleep Efficiency Index (%) (mean ± SD) | 70.9% ± 13.4% |
| Total Sleep Time Mean SaO2 (%) (mean ± SD) | 93.4% ± 3.3% |
| Obstructive Apnea Index (mean ± SD) | 29.2 ± 26.9 |
| Hypopnea Index (mean ± SD) | 41.7 ± 30.3 |
| Mixed Apnea Index (mean ± SD) | 5.5 ± 9.8 |
| Central Apnea Index (mean ± SD) | 1.0 ± 1.65 |
| Apnea/Hypopnea Index (AHI) (mean ± SD) | 78.6 ± 39.2 |
| Feature Index (m) | Feature | Description | Classification |
|---|---|---|---|
| 1 | PEAK | Maximum value of the envelope | Temporal |
| 2 | LOC | Temporal location of peak | Temporal |
| 3 | AREA | Total area under the curve | Temporal |
| 4 | AREA-25 | Area under the curve bounded by the first crossing of the 25% threshold to left and right of peak | Temporal |
| 5 | SPAN-25 | Duration of the waveform between the first crossing of the 25% of peak threshold to left and right of peak | Temporal |
| 6 | AREA-50 | The area under the curve bounded by the first crossing of the 50% threshold to left and right of peak | Temporal |
| 7 | SPAN-50 | Duration of the waveform between the first crossing of the 50% of peak threshold to left and right of peak | Temporal |
| 8 | AREA-70 | The area under the curve bounded by the first crossing of the 70% threshold to left and right of peak | Temporal |
| 9 | SPAN-70 | Duration of the waveform between the first crossing of the 70% of peak threshold to left and right of peak | Temporal |
| 10 | VLSB | Very Low Spectral Band (10–230 kHz) | Spectral |
| 11 | LSB | Low Spectral Band (230–487 kHz) | Spectral |
| 12 | HSB | High Spectral Band (487–770 kHz) | Spectral |
| 13 | VHSB | Very High Spectral Band (770–1000 kHz) | Spectral |
| Event Epoch Classification | Number of Clipped Epochs |
|---|---|
| Control normal breathing of 10 s followed by normal breathing for 10 s (NB:NB) | 603 |
| Apneic respiratory event followed by at least 10 s of hyperventilation (ARE:HV) | 693 |
| Hypopnea respiratory event followed by at least 10 s of hyperventilation (HRE:HV) | 801 |
| Combine respiratory event (apnea and hypopnea) followed by at least 10 s of hyperventilation (RE:HV) = (ARE:HV) + (HRE:HV) | 1494 |
| Statistical Parameter | Description |
|---|---|
| Feature m mean for apneic respiratory event (ARE) | |
| Feature m mean for hypopnea respiratory event (HRE) | |
| Feature m mean for all respiratory events (RE) | |
| Feature m mean for succeeding hyperventilation period (HV) | |
| Feature m mean for the first 10 s controlling normal breathing (NBx) | |
| Feature m mean for the second 10 s controlling normal breathing (NBy) | |
| Feature m standard deviation for apneic respiratory event (ARE) | |
| Feature m standard deviation for hypopnea respiratory event (HRE) | |
| Feature m standard deviation for all respiratory events (RE) | |
| Feature m standard deviation for succeeding hyperventilation period (HV) | |
| Feature m standard deviation for the first 10 s controlling normal breathing (NBx) | |
| Feature m standard deviation for the second 10 s controlling normal breathing (NBy) |
| Feature Index (m) | Feature | Ratio of Means (RM) | Ratio of Standard Deviations (RS) |
|---|---|---|---|
| p-Value | p-Value | ||
| 1 | PEAK | 0.527 | 0.163 |
| 2 | LOC | 0.946 | 0.443 |
| 3 | AREA | 0.731 | 0.781 |
| 4 | AREA-25 | 0.857 | 0.160 |
| 5 | SPAN-25 | 0.621 | 0.353 |
| 6 | AREA-50 | 0.339 | 0.994 |
| 7 | SPAN-50 | 0.551 | 0.929 |
| 8 | AREA-70 | 0.111 | 0.067 |
| 9 | SPAN-70 | 0.123 | 0.074 |
| 10 | VLSB | 0.757 | 0.877 |
| 11 | LSB | 0.657 | 0.863 |
| 12 | HSB | 0.831 | 0.520 |
| 13 | VHSB | 0.949 | 0.998 |
| Feature Index (m) | Feature | Ratio of Means (RM) | Ratio of Standard Deviations (RS) |
|---|---|---|---|
| p-Value | p-Value | ||
| 1 | PEAK | 0.117 | 0.591 |
| 2 | LOC | <0.001 | 0.017 |
| 3 | AREA | <0.001 | 0.027 |
| 4 | AREA-25 | <0.001 | 0.834 |
| 5 | SPAN-25 | <0.001 | 0.895 |
| 6 | AREA-50 | <0.001 | 0.052 |
| 7 | SPAN-50 | <0.001 | 0.188 |
| 8 | AREA-70 | <0.001 | <0.001 |
| 9 | SPAN-70 | <0.001 | 0.002 |
| 10 | VLSB | <0.001 | 0.008 |
| 11 | LSB | <0.001 | <0.001 |
| 12 | HSB | <0.001 | <0.001 |
| 13 | VHSB | <0.001 | <0.001 |
| Feature Index (m) | Feature | Ratio of Means (RM) | Ratio of Standard Deviations (RS) |
|---|---|---|---|
| p-Value | p-Value | ||
| 1 | PEAK | <0.001 | <0.001 |
| 2 | LOC | 0.014 | 0.258 |
| 3 | AREA | 0.325 | 0.126 |
| 4 | AREA-25 | <0.001 | 0.496 |
| 5 | SPAN-25 | <0.001 | 0.161 |
| 6 | AREA-50 | 0.004 | 0.094 |
| 7 | SPAN-50 | <0.001 | 0.050 |
| 8 | AREA-70 | <0.001 | 0.009 |
| 9 | SPAN-70 | <0.001 | 0.001 |
| 10 | VLSB | <0.001 | <0.001 |
| 11 | LSB | <0.001 | <0.001 |
| 12 | HSB | <0.001 | <0.001 |
| 13 | VHSB | <0.001 | <0.001 |
| Feature Index (m) | Feature | Ratio of Means (RM) | Ratio of Standard Deviations (RS) |
|---|---|---|---|
| p-Value | p-Value | ||
| 1 | PEAK | <0.001 | 0.001 |
| 2 | LOC | <0.001 | 0.012 |
| 3 | AREA | <0.001 | 0.544 |
| 4 | AREA-25 | <0.001 | 0.538 |
| 5 | SPAN-25 | <0.001 | 0.284 |
| 6 | AREA-50 | <0.001 | 0.010 |
| 7 | SPAN-50 | <0.001 | 0.021 |
| 8 | AREA-70 | <0.001 | <0.001 |
| 9 | SPAN-70 | <0.001 | <0.001 |
| 10 | VLSB | 0.864 | 0.231 |
| 11 | LSB | <0.001 | <0.001 |
| 12 | HSB | <0.001 | <0.001 |
| 13 | VHSB | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Abed, M.; Watenpaugh, D.; Behbehani, K. In Situ Investigation of Upper Airway Occlusion in Sleep Disordered Breathing Using Ultrasonic Transducer Arrays. Biosensors 2023, 13, 121. https://doi.org/10.3390/bios13010121
Al-Abed M, Watenpaugh D, Behbehani K. In Situ Investigation of Upper Airway Occlusion in Sleep Disordered Breathing Using Ultrasonic Transducer Arrays. Biosensors. 2023; 13(1):121. https://doi.org/10.3390/bios13010121
Chicago/Turabian StyleAl-Abed, Mohammad, Donald Watenpaugh, and Khosrow Behbehani. 2023. "In Situ Investigation of Upper Airway Occlusion in Sleep Disordered Breathing Using Ultrasonic Transducer Arrays" Biosensors 13, no. 1: 121. https://doi.org/10.3390/bios13010121
APA StyleAl-Abed, M., Watenpaugh, D., & Behbehani, K. (2023). In Situ Investigation of Upper Airway Occlusion in Sleep Disordered Breathing Using Ultrasonic Transducer Arrays. Biosensors, 13(1), 121. https://doi.org/10.3390/bios13010121