Peptide-Coated Bacteriorhodopsin-Based Photoelectric Biosensor for Detecting Rheumatoid Arthritis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Clinical Samples
2.3. Chip Preparation, Characterization, and Serum Detection
3. Results and Discussion
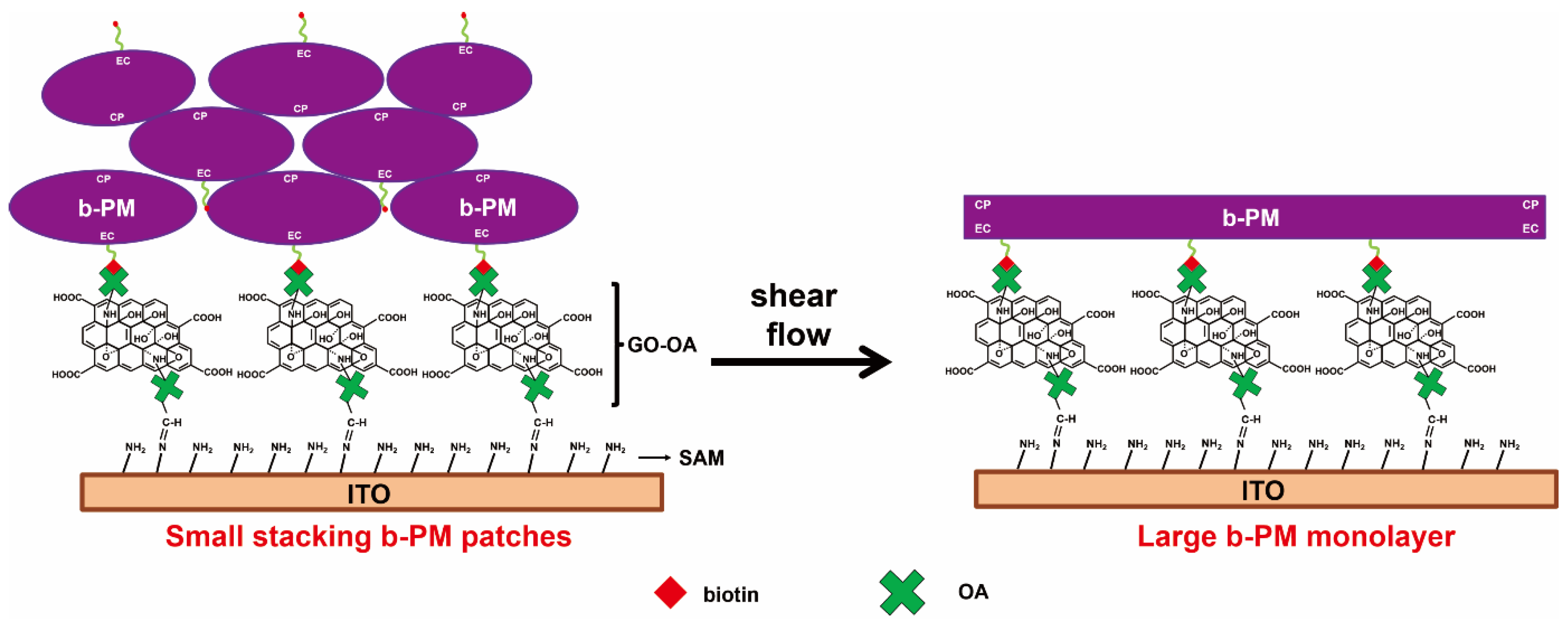
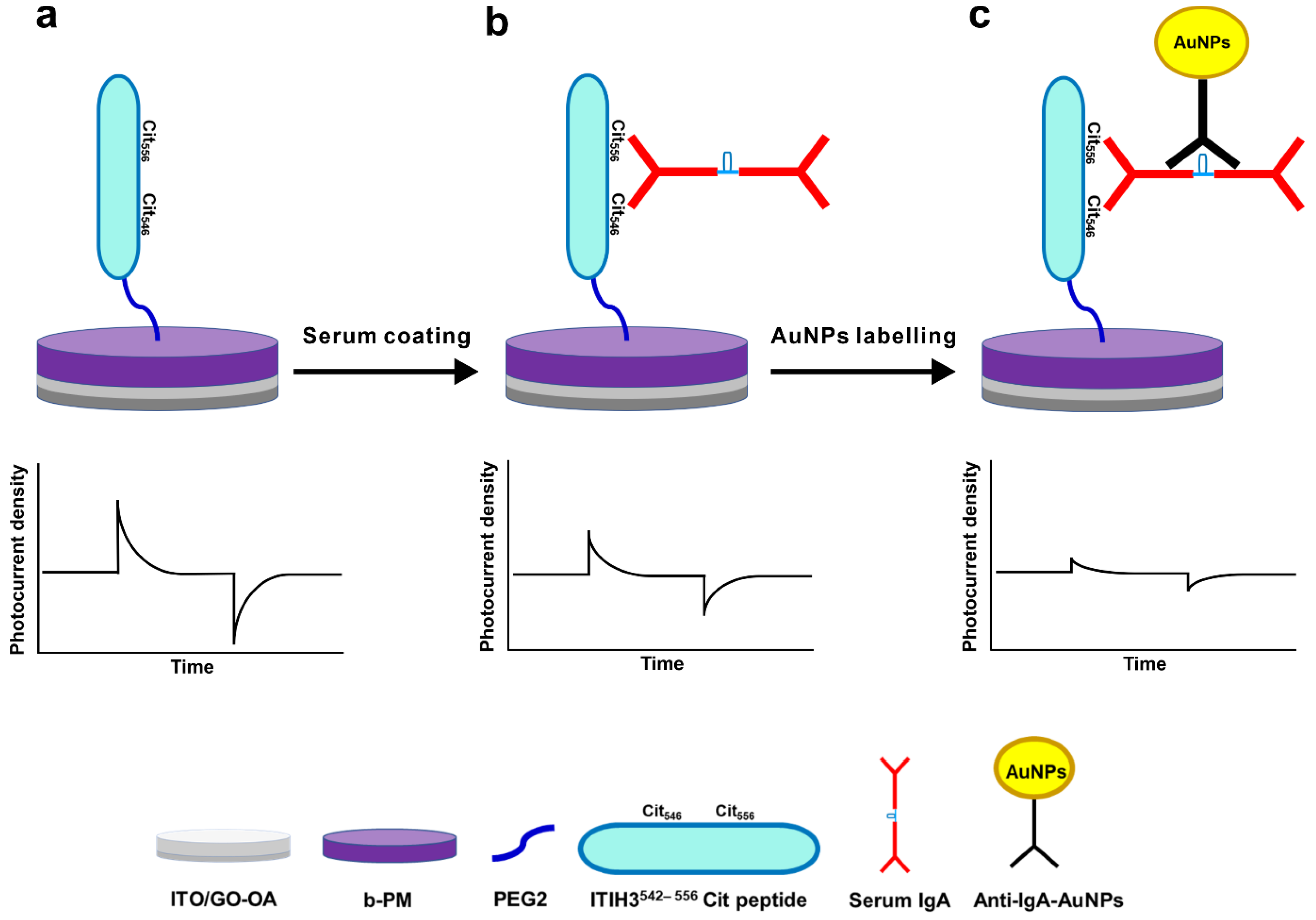
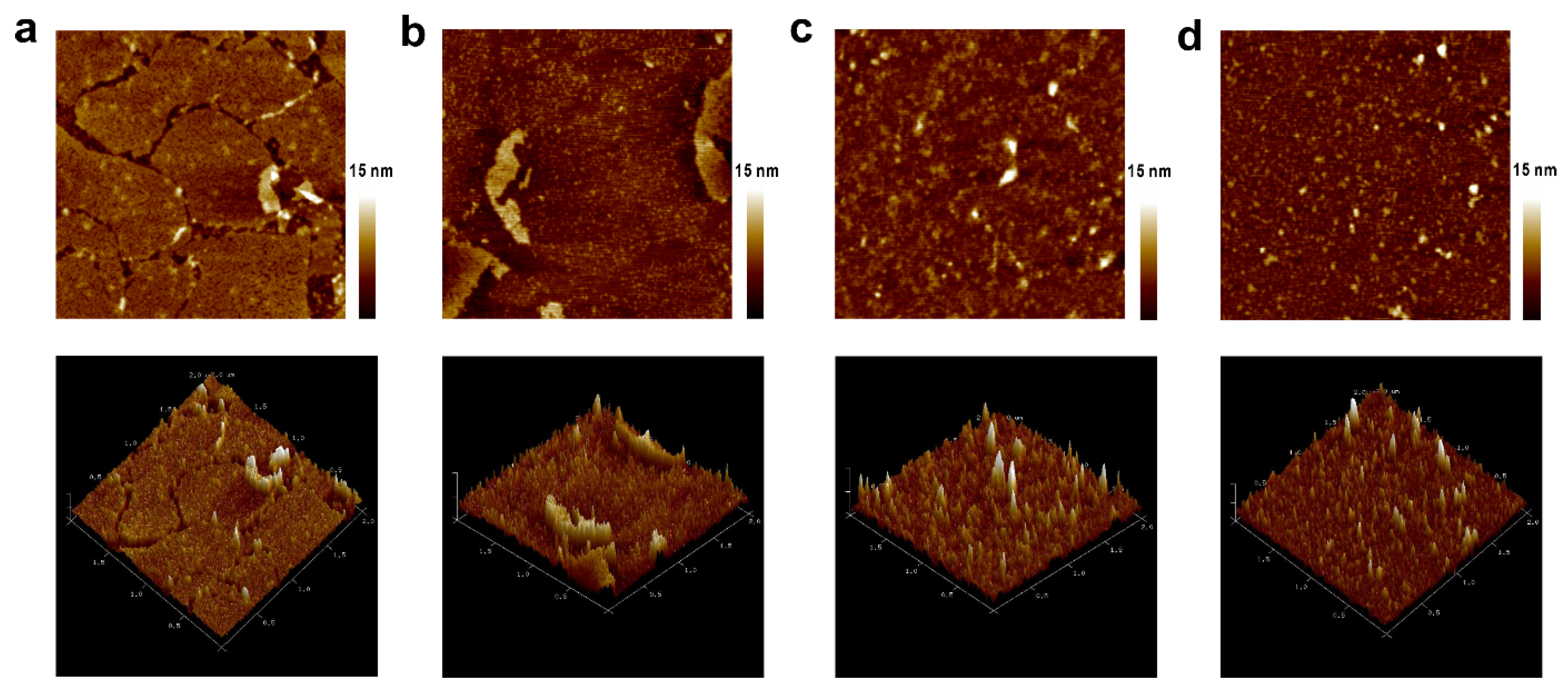
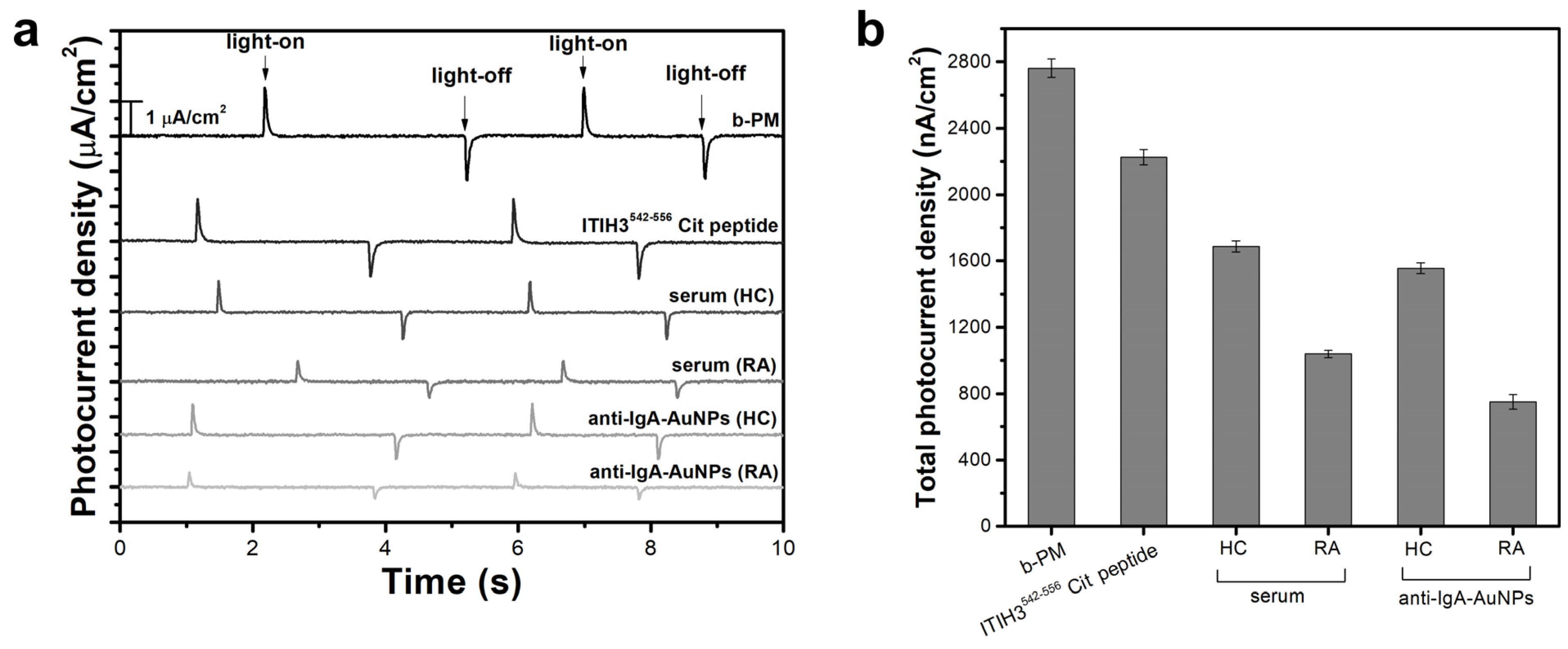
3.1. Fabrication, Characterization, and Detection
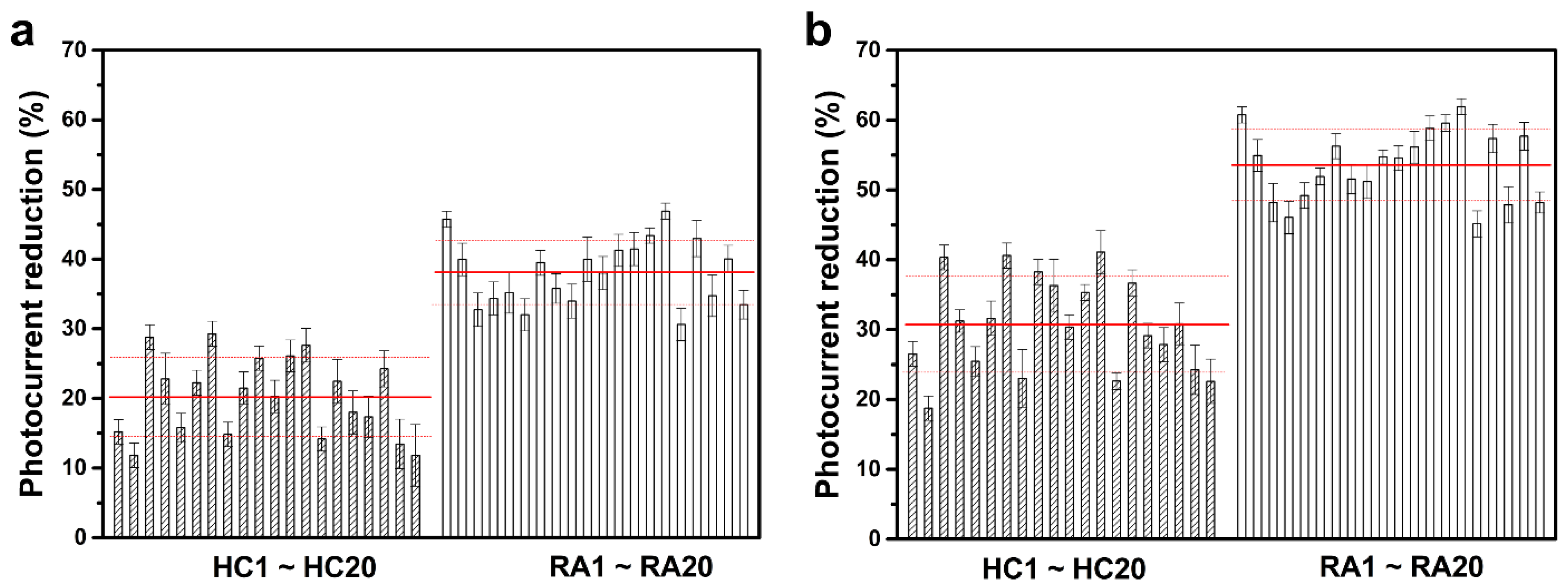
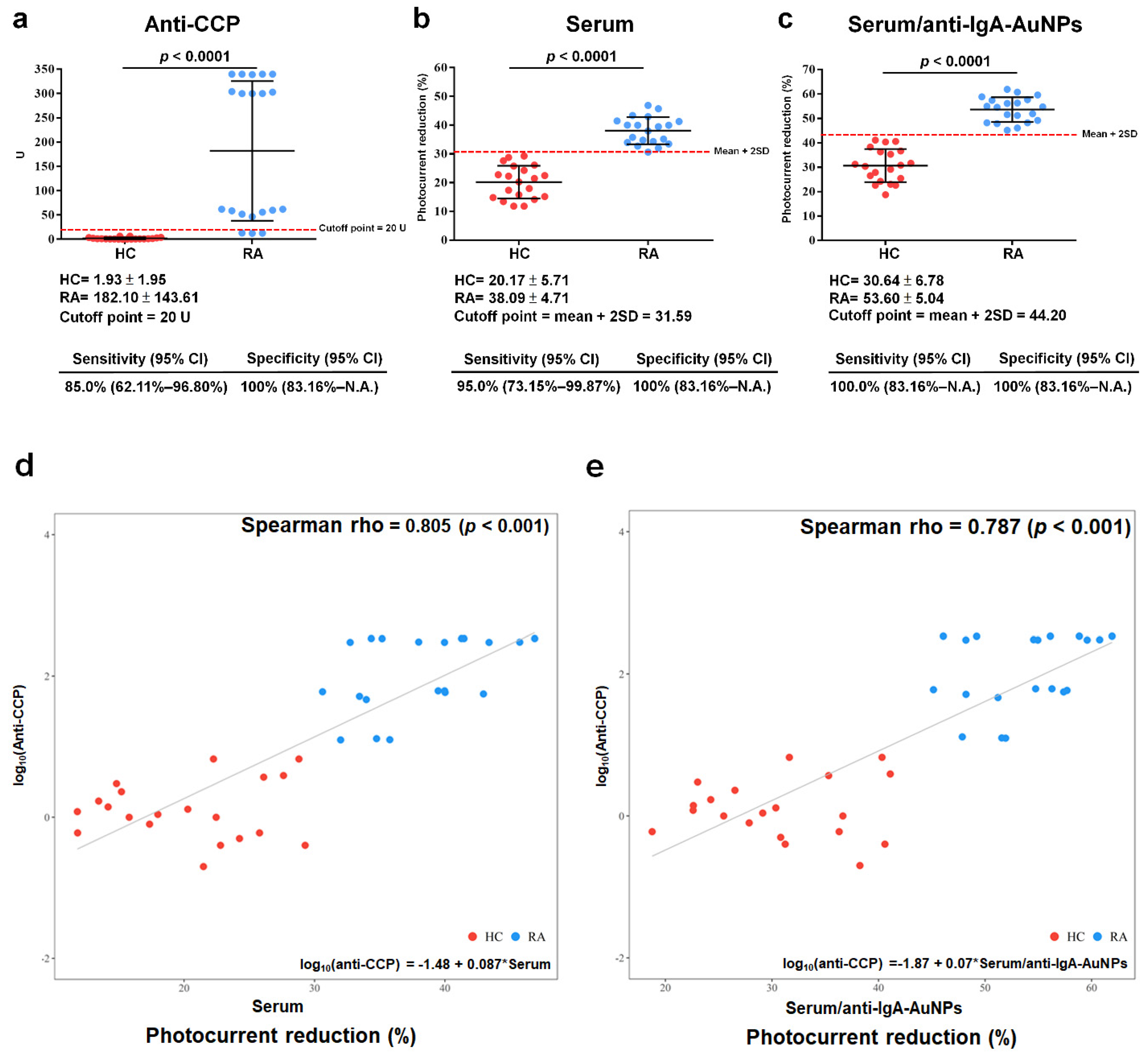
3.2. Clinical Samples

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
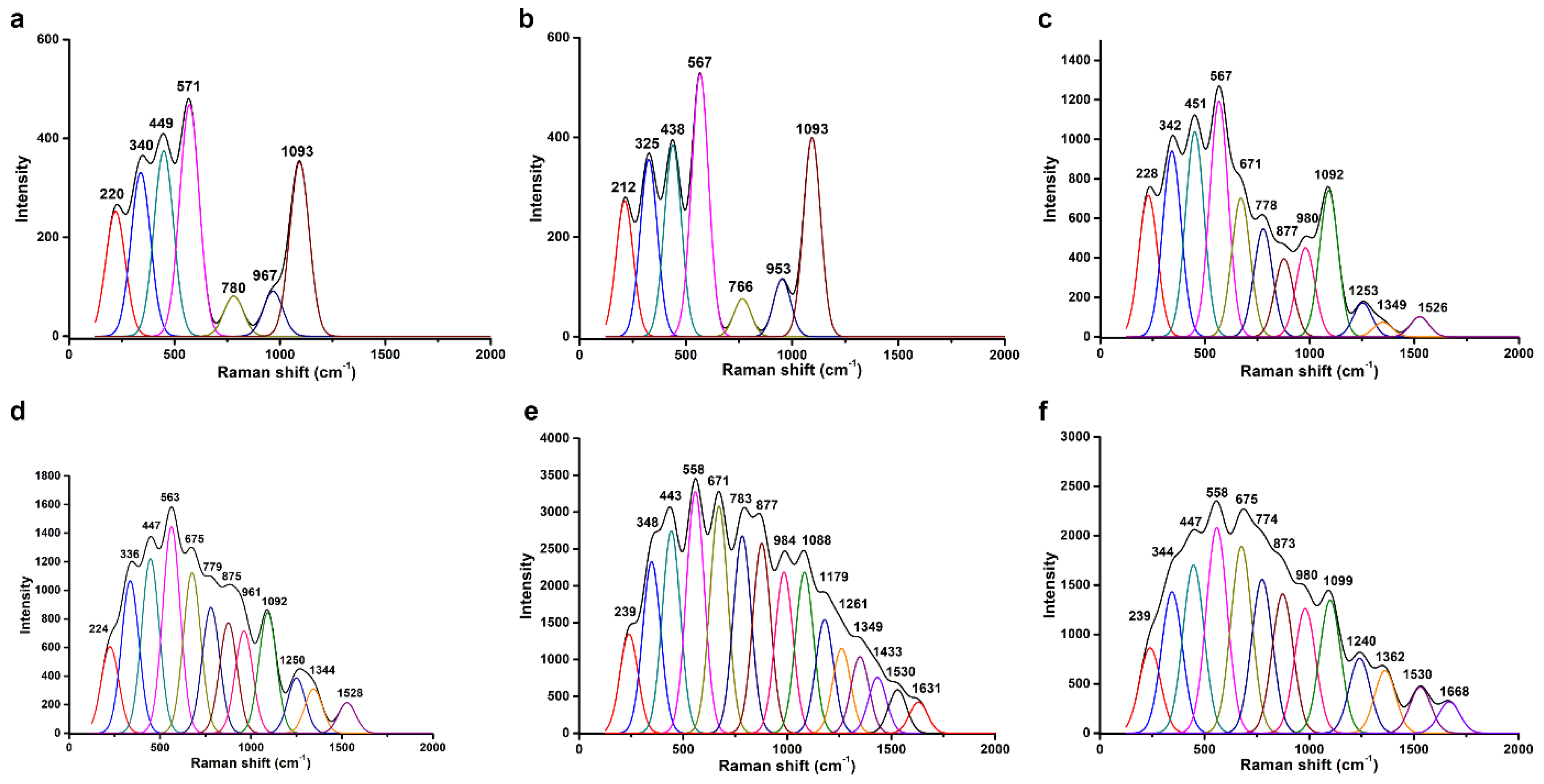
| APPA | GO-OA | b-PM | Peptide | HC Serum | Anti-IgA-AuNPs | Band Assignment | References |
|---|---|---|---|---|---|---|---|
| 220 | 212 | 228 | 224 | 239 | 239 | ITO | - |
| 340 | 325 | 342 | 336 | 348 | 344 | ITO | - |
| 449 | 438 | 451 | 447 | 443 | 447 | ITO | - |
| 571 | 567 | 567 | 563 | 558 | 558 | ITO | - |
| 671 | 675 | 671 | 675 | C-S stretching/Tyr | [31,32] | ||
| 780 | 766 | 778 | 779 | 783 | 774 | ITO/Trp | [31,32,33] |
| 877 | 875 | 877 | 873 | Tyr | [31,32,33] | ||
| 967 | 953 | 980 | 961 | 984 | 980 | ITO | - |
| 1093 | 1093 | 1092 | 1092 | 1088 | 1099 | ITO | - |
| 1179 | Trp/Phe | [31] | |||||
| 1253 | 1250 | 1261 | 1240 | Amide III/retinal | [34,35] | ||
| 1349 | 1344 | 1349 | 1362 | Amide III/retinal | [34,35] | ||
| 1433 | CH2 deformation | [34] | |||||
| 1526 | 1528 | 1530 | 1530 | C=C stretching, retinal | [35] | ||
| 1631 | 1668 | Trp/Phe | [31] |
| Characteristic a | HC b | RA c |
|---|---|---|
| n = 20 | n = 20 | |
| Age (years) | 51.10 ± 13.46 | 50.80 ± 13.01 |
| Gender | ||
| Female | 20 | 20 |
| Disease duration (median in years) | N.A. c | 5.4 ± 6.41 |
| DAS 28 | N.A. | 4.4 ± 1.67 |
| Clinical tests | ||
| RF-positive (%) | 0 | 94.7 |
| Anti-CCP-positive (%) | 0 | 85.0 |
| CRP-positive (%) | N.A. | 35.0 |
| ESR-positive (%) | N.A. | 90.0 |
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van der Woude, D.; van der Helm-van Mil, A.H.M. Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.F.; Luo, S.F.; See, L.C.; Chou, I.J.; Chang, H.C.; Yu, K.H. Rheumatoid arthritis prevalence, incidence, and mortality rates: A nationwide population study in Taiwan. Rheumatol. Int. 2013, 33, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Scott, I.C.; Mangat, N.; MacGregor, A.; Raza, K.; Mallen, C.D.; Hider, S.L. Primary care challenges in diagnosing and referring patients with suspected rheumatoid arthritis: A national cross-sectional GP survey. Rheumatol. Adv. Pract. 2018, 2, rky012. [Google Scholar] [CrossRef] [PubMed]
- Farid, S.; Azizi, G.; Mirshafiey, A. Anti-citrullinated protein antibodies and their clinical utility in rheumatoid arthritis. Int. J. Rheum. Dis. 2013, 16, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Liao, K.; Nair, R.; Ringold, S.; Costenbader, K.H. Anti-citrullinated peptide antibody assays and their role in the diagnosis of rheumatoid arthritis. Arthritis Rheum. 2009, 61, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- Arnoux, F.; Mariot, C.; Peen, E.; Lambert, N.C.; Balandraud, N.; Roudier, J.; Auger, I. Peptidyl arginine deiminase immunization induces anticitrullinated protein antibodies in mice with particular MHC types. Proc. Natl. Acad. Sci. USA 2017, 114, E10169–E10177. [Google Scholar] [CrossRef]
- Liao, C.C.; Chou, P.L.; Cheng, C.W.; Chang, Y.S.; Chi, W.M.; Tsai, K.L.; Chen, W.J.; Kung, T.S.; Tai, C.C.; Lee, K.W.; et al. Comparative analysis of novel autoantibody isotypes against citrullinated-inter-alpha-trypsin inhibitor heavy chain 3 (ITIH3)(542–556) peptide in serum from Taiwanese females with rheumatoid arthritis, primary Sjogren’s syndrome and secondary Sjogren’s syndrome in rheumatoid arthritis. J. Proteom. 2016, 141, 1–11. [Google Scholar] [CrossRef]
- Lin, C.Y.; Nhat Nguyen, U.T.; Hsieh, H.Y.; Tahara, H.; Chang, Y.S.; Wang, B.Y.; Gu, B.C.; Dai, Y.H.; Wu, C.C.; Tsai, I.J.; et al. Peptide-based electrochemical sensor with nanogold enhancement for detecting rheumatoid arthritis. Talanta 2022, 236, 122886. [Google Scholar] [CrossRef]
- Dutta, P.; Su, T.-Y.; Fu, A.-Y.; Chang, M.-C.; Guo, Y.-J.; Tsai, I.-J.; Wei, P.-K.; Chang, Y.-S.; Lin, C.-Y.; Fan, Y.-J. Combining portable solar-powered centrifuge to nanoplasmonic sensing chip with smartphone reader for rheumatoid arthritis detection. Chem. Eng. J. 2022, 434, 133864. [Google Scholar] [CrossRef]
- Szarka, E.; Aradi, P.; Huber, K.; Pozsgay, J.; Vegh, L.; Magyar, A.; Gyulai, G.; Nagy, G.; Rojkovich, B.; Kiss, E.; et al. Affinity Purification and Comparative Biosensor Analysis of Citrulline-Peptide-Specific Antibodies in Rheumatoid Arthritis. Int. J. Mol. Sci. 2018, 19, 326. [Google Scholar] [CrossRef]
- Rodovalho, V.R.; Araujo, G.R.; Vaz, E.R.; Ueira-Vieira, C.; Goulart, L.R.; Madurro, J.M.; Brito-Madurro, A.G. Peptide-based electrochemical biosensor for juvenile idiopathic arthritis detection. Biosens. Bioelectron. 2018, 100, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Fang, C.; Yan, J.; Li, H.; Tu, Y. A sensitive electrochemiluminescent biosensor based on AuNP-functionalized ITO for a label-free immunoassay of C-peptide. Bioelectrochemistry 2018, 123, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Sun, H.; Huang, Y.; Tang, Y.; Chen, Q.; Miao, P. Peptide cleavage-based electrochemical biosensor coupling graphene oxide and silver nanoparticles. Anal. Chim. Acta 2019, 1047, 45–51. [Google Scholar] [CrossRef]
- Xing, Y.; Feng, X.Z.; Zhang, L.; Hou, J.; Han, G.C.; Chen, Z. A sensitive and selective electrochemical biosensor for the determination of beta-amyloid oligomer by inhibiting the peptide-triggered in situ assembly of silver nanoparticles. Int. J. Nanomed. 2017, 12, 3171–3179. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Choi, J.S.; Guruprasath, P.; Lee, B.H.; Cho, Y.W. An Electrochemical Biosensor Based on a Myoglobin-specific Binding Peptide for Early Diagnosis of Acute Myocardial Infarction. Anal. Sci. 2015, 31, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Drouvalakis, K.A.; Bangsaruntip, S.; Hueber, W.; Kozar, L.G.; Utz, P.J.; Dai, H. Peptide-coated nanotube-based biosensor for the detection of disease-specific autoantibodies in human serum. Biosens. Bioelectron. 2008, 23, 1413–1421. [Google Scholar] [CrossRef]
- de Gracia Villa, M.; Jiménez-Jorquera, C.; Haro, I.; Gomara, M.J.; Sanmartí, R.; Fernández-Sánchez, C.; Mendoza, E. Carbon nanotube composite peptide-based biosensors as putative diagnostic tools for rheumatoid arthritis. Biosens. Bioelectron. 2011, 27, 113–118. [Google Scholar] [CrossRef]
- Hampp, N. Bacteriorhodopsin as a Photochromic Retinal Protein for Optical Memories. Chem. Rev. 2000, 100, 1755–1776. [Google Scholar] [CrossRef]
- Li, Y.T.; Tian, Y.; Tian, H.; Tu, T.; Gou, G.Y.; Wang, Q.; Qiao, Y.C.; Yang, Y.; Ren, T.L. A Review on Bacteriorhodopsin-Based Bioelectronic Devices. Sensors 2018, 18, 1368. [Google Scholar] [CrossRef]
- Singh, P.; Singh, S.; Jaggi, N.; Kim, K.H.; Devi, P. Recent advances in bacteriorhodopsin-based energy harvesters and sensing devices. Nano Energy 2021, 79, 105482. [Google Scholar] [CrossRef]
- Chen, H.M.; Jheng, K.R.; Yu, A.D. Direct, label-free, selective, and sensitive microbial detection using a bacteriorhodopsin-based photoelectric immunosensor. Biosens. Bioelectron. 2017, 91, 24–31. [Google Scholar] [CrossRef]
- Wu, H.H.; Liao, X.Q.; Wu, X.Y.; Lin, C.D.; Jheng, K.R.; Chen, H.R.; Wang, Y.Y.; Chen, H.M. Versatile Protein-A Coated Photoelectric Immunosensors with a Purple-Membrane Monolayer Transducer Fabricated by Affinity-Immobilization on a Graphene-Oxide Complexed Linker and by Shear Flow. Sensors 2018, 18, 4493. [Google Scholar] [CrossRef]
- Lin, Y.C.; Lin, C.Y.; Chen, H.M.; Kuo, L.P.; Hsieh, C.E.; Wang, X.H.; Cheng, C.W.; Wu, C.Y.; Chen, Y.S. Direct and Label-Free Determination of Human Glycated Hemoglobin Levels Using Bacteriorhodopsin as the Biosensor Transducer. Sensors 2020, 20, 7274. [Google Scholar] [CrossRef]
- Chen, H.M.; Wang, W.C.; Chen, H.R. Small-Molecule Analysis Based on DNA Strand Displacement Using a Bacteriorhodopsin Photoelectric Transducer: Taking ATP as an Example. Sensors 2023, 23, 7453. [Google Scholar] [CrossRef]
- Chen, H.M.; Lin, C.J.; Jheng, K.R.; Kosasih, A.; Chang, J.Y. Effect of graphene oxide on affinity-immobilization of purple membranes on solid supports. Colloids Surf B Biointerfaces 2014, 116, 482–488. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Voitchovsky, K.; Antoranz Contera, S.; Kamihira, M.; Watts, A.; Ryan, J.F. Differential stiffness and lipid mobility in the leaflets of purple membranes. Biophys. J. 2006, 90, 2075–2085. [Google Scholar] [CrossRef]
- Kuhlbrandt, W. Bacteriorhodopsin—The movie. Nature 2000, 406, 569–570. [Google Scholar] [CrossRef] [PubMed]
- Chinnadayyala, S.R.; Cho, S. Electrochemical Immunosensor for the Early Detection of Rheumatoid Arthritis Biomarker: Anti-Cyclic Citrullinated Peptide Antibody in Human Serum Based on Avidin-Biotin System. Sensors 2020, 21, 124. [Google Scholar] [CrossRef] [PubMed]
- Painter, P.C.; Koenig, J.L. Raman spectroscopic study of the structure of antibodies. Biopolymers 1975, 14, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Rygula, A.; Majzner, K.; Marzec, K.M.; Kaczor, A.; Pilarczyk, M.; Baranska, M. Raman spectroscopy of proteins: A review. J. Raman Spectrosc. 2013, 44, 1061–1076. [Google Scholar] [CrossRef]
- Fagnano, C.; Fini, G.; Torreggiani, A. Raman spectroscopic study of the avidin—Biotin complex. J. Raman Spectrosc. 1995, 26, 991–995. [Google Scholar] [CrossRef]
- Kengne-Momo, R.P.; Daniel, P.; Lagarde, F.; Jeyachandran, Y.L.; Pilard, J.F.; Durand-Thouand, M.J.; Thouand, G. Protein Interactions Investigated by the Raman Spectroscopy for Biosensor Applications. Int. J. Spectrosc. 2012, 2012, 462901. [Google Scholar] [CrossRef]
- Braiman, M.; Mathies, R. Resonance Raman spectra of bacteriorhodopsin’s primary photoproduct: Evidence for a distorted 13-cis retinal chromophore. Proc. Natl. Acad. Sci. USA 1982, 79, 403–407. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-M.; Tsai, Y.-H.; Hsu, C.-Y.; Wang, Y.-Y.; Hsieh, C.-E.; Chen, J.-H.; Chang, Y.-S.; Lin, C.-Y. Peptide-Coated Bacteriorhodopsin-Based Photoelectric Biosensor for Detecting Rheumatoid Arthritis. Biosensors 2023, 13, 929. https://doi.org/10.3390/bios13100929
Chen H-M, Tsai Y-H, Hsu C-Y, Wang Y-Y, Hsieh C-E, Chen J-H, Chang Y-S, Lin C-Y. Peptide-Coated Bacteriorhodopsin-Based Photoelectric Biosensor for Detecting Rheumatoid Arthritis. Biosensors. 2023; 13(10):929. https://doi.org/10.3390/bios13100929
Chicago/Turabian StyleChen, Hsiu-Mei, Yi-Hsuan Tsai, Chien-Yi Hsu, Yong-Yi Wang, Cheng-En Hsieh, Jin-Hua Chen, Yu-Sheng Chang, and Ching-Yu Lin. 2023. "Peptide-Coated Bacteriorhodopsin-Based Photoelectric Biosensor for Detecting Rheumatoid Arthritis" Biosensors 13, no. 10: 929. https://doi.org/10.3390/bios13100929
APA StyleChen, H. -M., Tsai, Y. -H., Hsu, C. -Y., Wang, Y. -Y., Hsieh, C. -E., Chen, J. -H., Chang, Y. -S., & Lin, C. -Y. (2023). Peptide-Coated Bacteriorhodopsin-Based Photoelectric Biosensor for Detecting Rheumatoid Arthritis. Biosensors, 13(10), 929. https://doi.org/10.3390/bios13100929