Upper-Arm Photoplethysmographic Sensor with One-Time Calibration for Long-Term Blood Pressure Monitoring

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
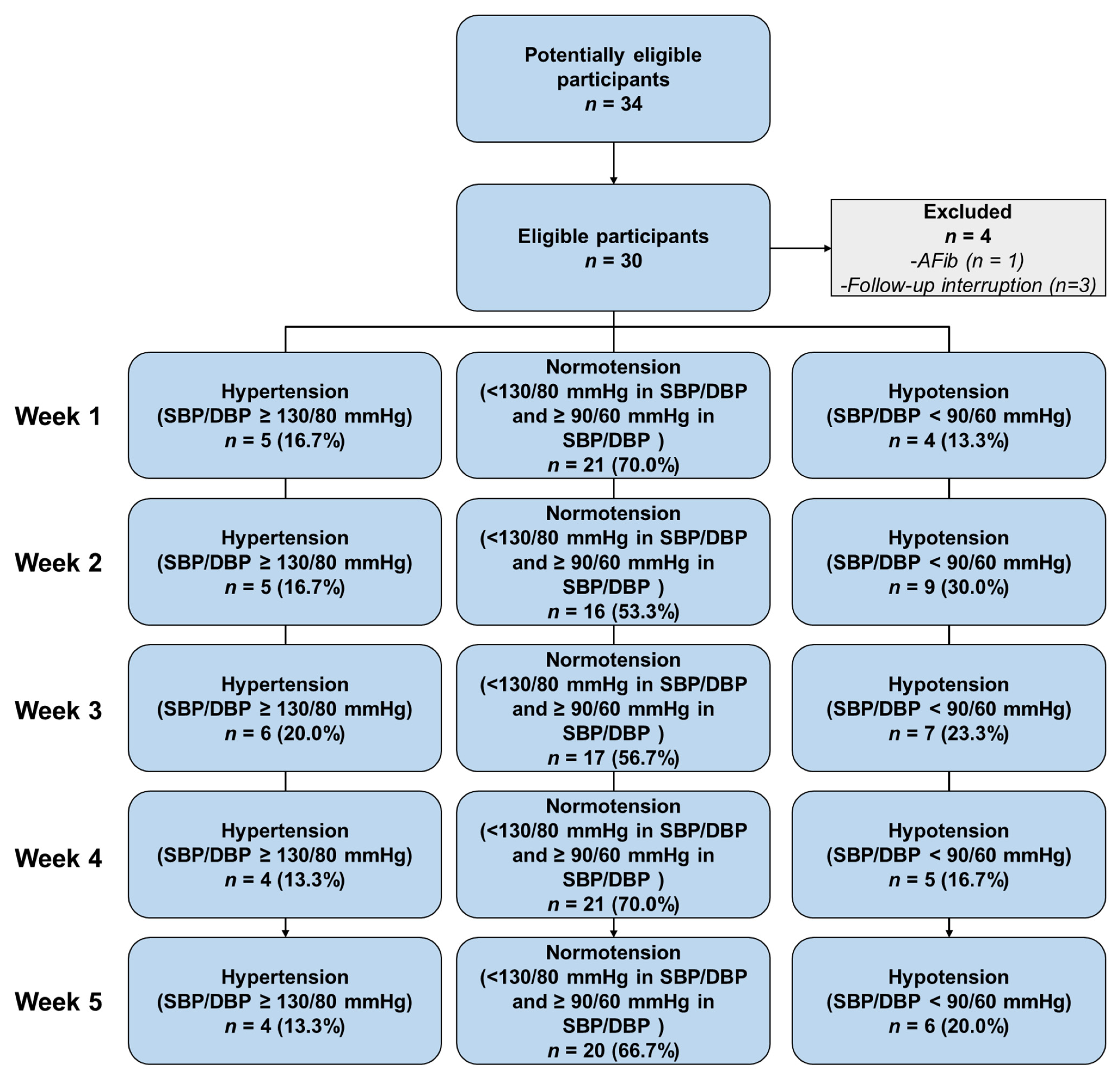
2.1. Participants from Clinical Trial
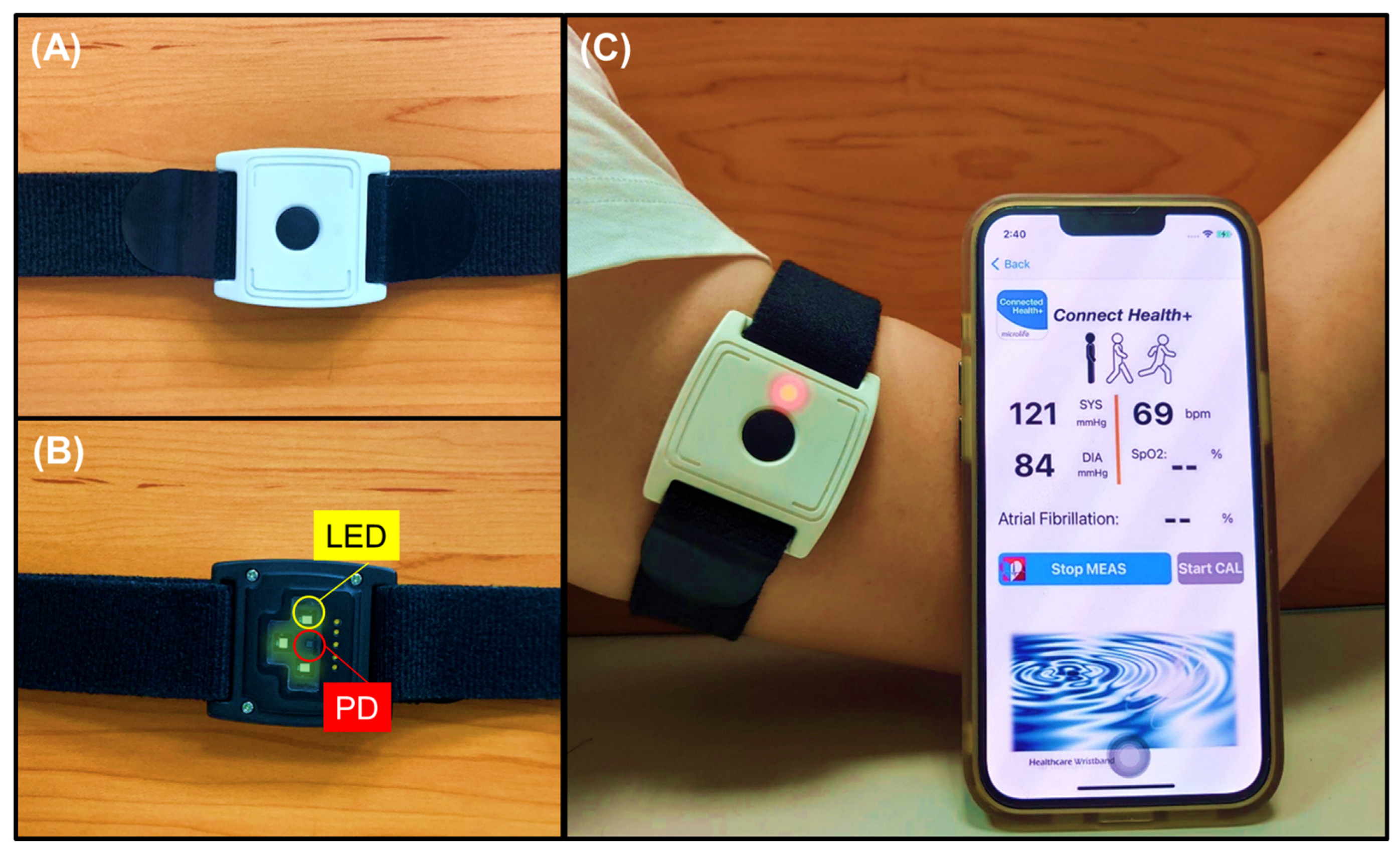
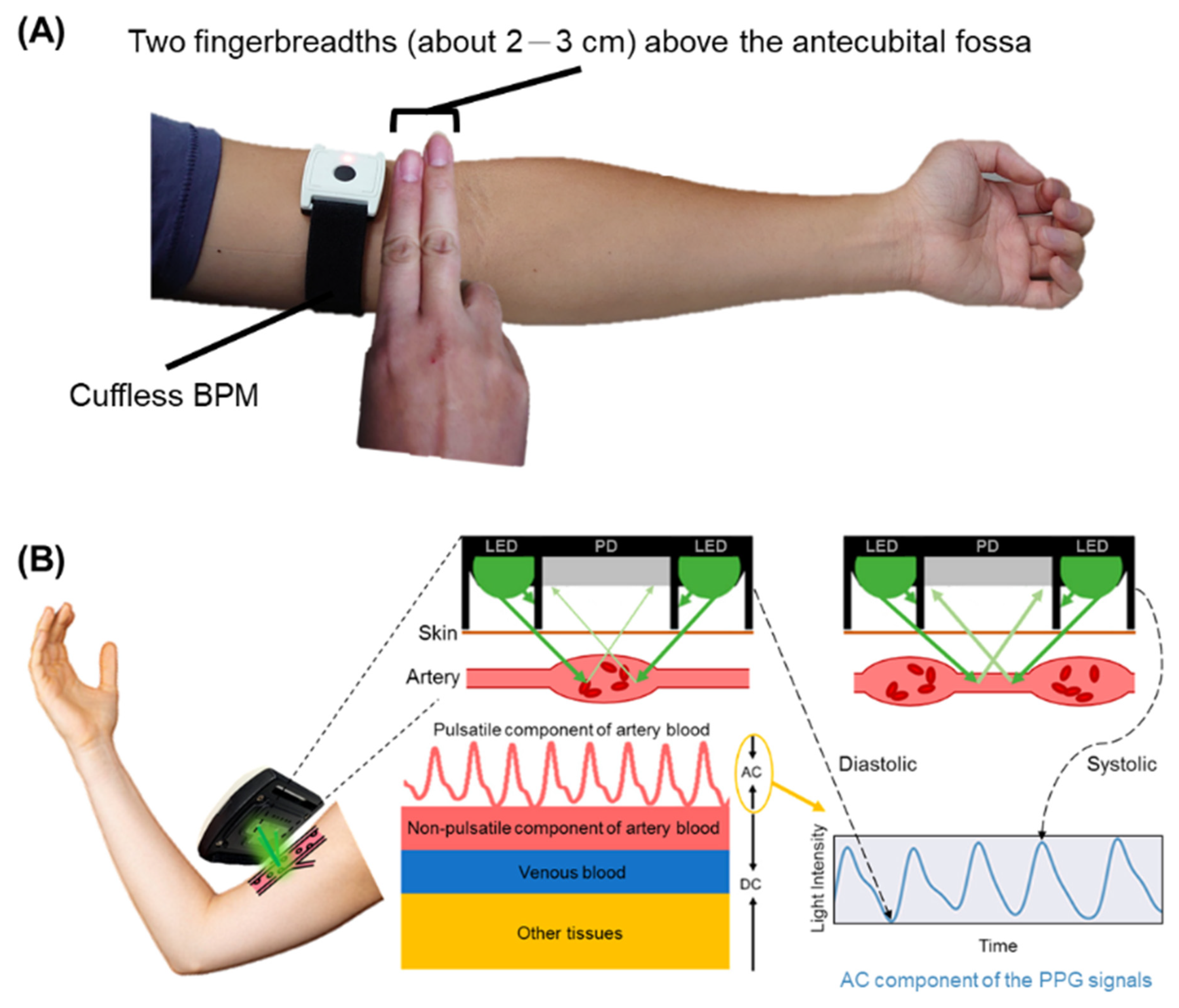
2.2. Upper-Arm Photoplethysmographic Sensor as a Cuffless Blood Pressure Monitor
2.3. Machine-Learning Framework for an Embedded Optimal Design on the Fine-Tuning Method
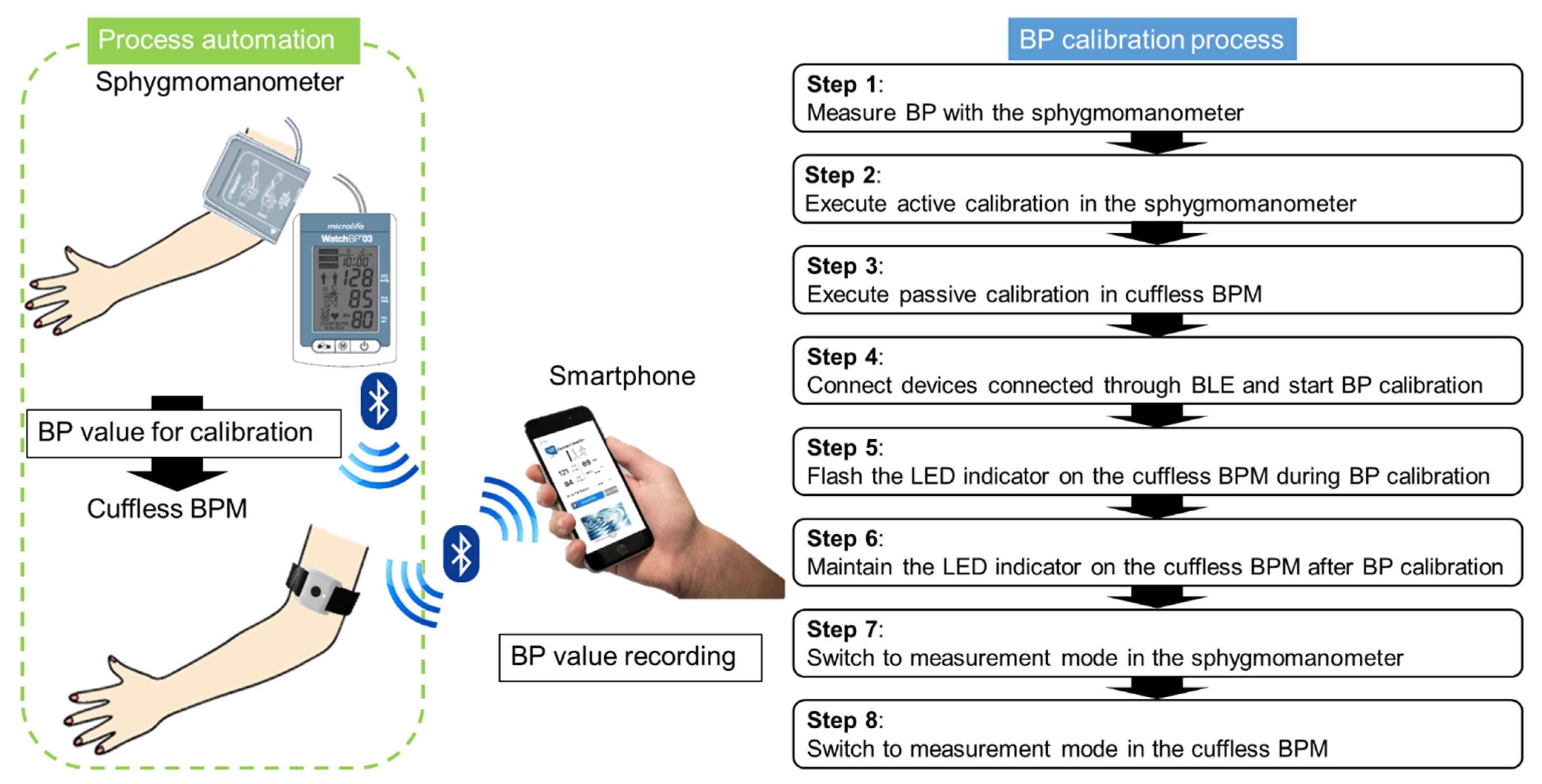
2.4. Integration of an Autocalibrated System for a Cuff-Based and Cuffless Blood Pressure Monitor through a Smartphone
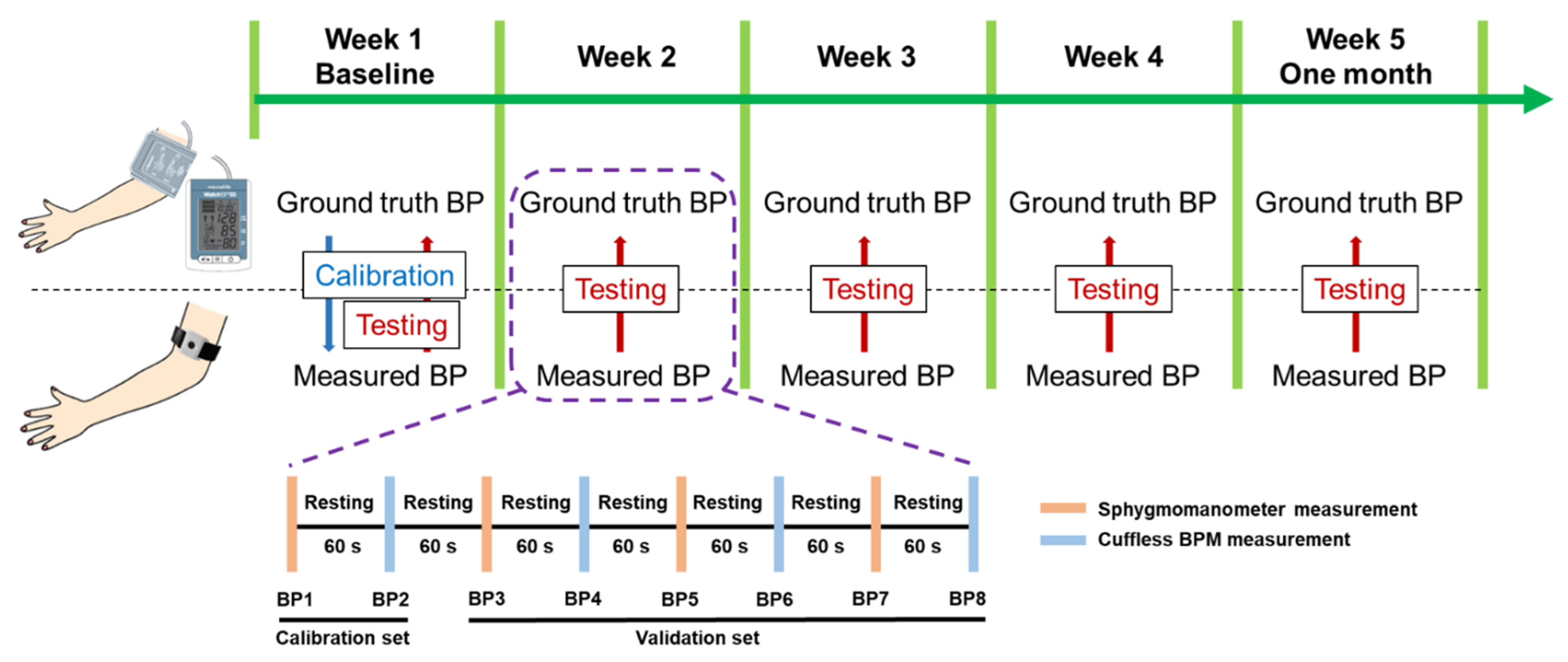
2.5. Validation of ISO Protocol Based on One-Time Calibration for Long-Term Blood Pressure Monitoring
2.6. Statistical Analysis of Blood Pressure Estimations
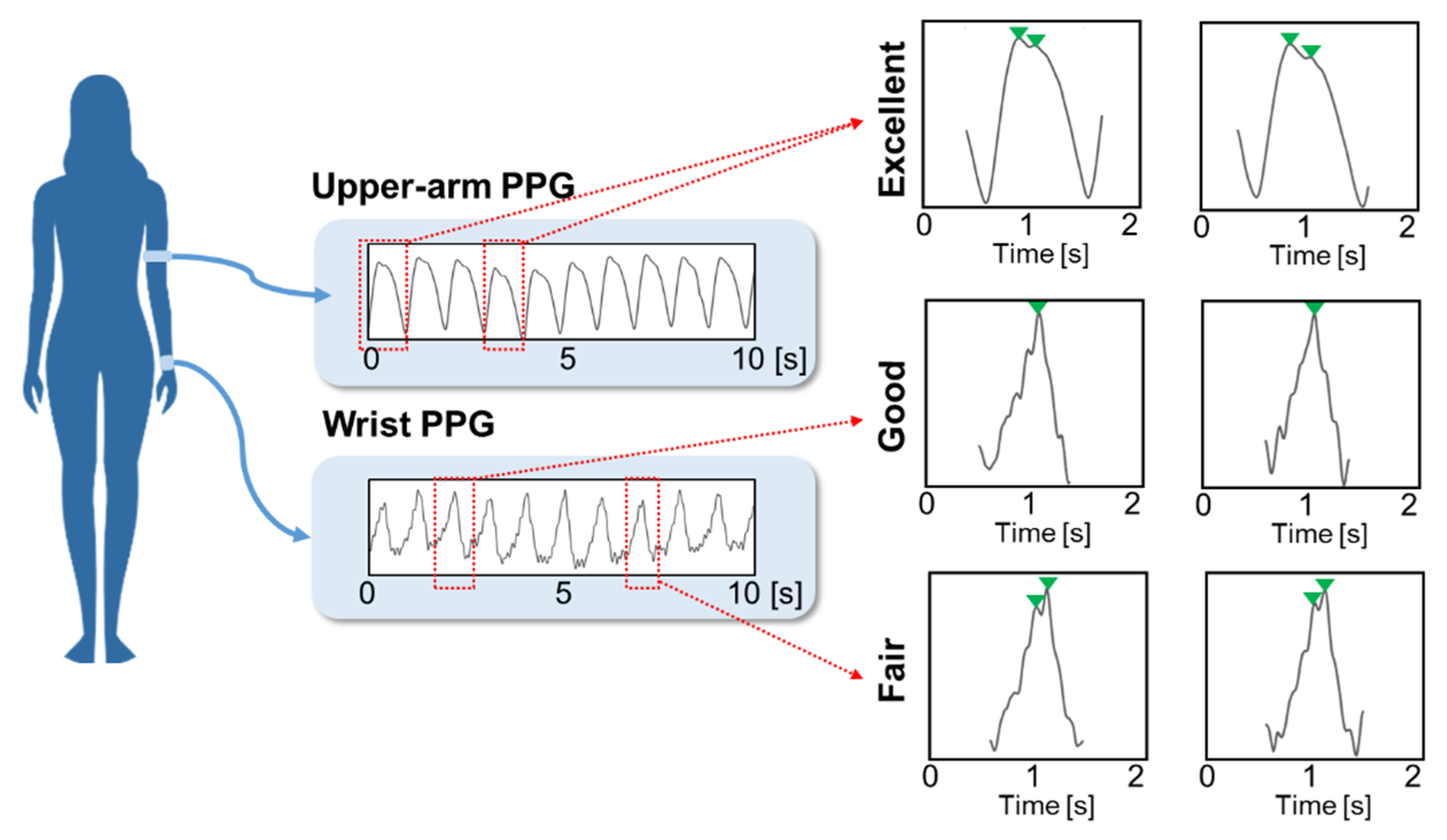
- Fair—systolic and diastolic peaks cannot be easily distinguished from noise.
- Good—the systolic peak is clearly detectable, but the diastolic peak is not.
- Excellent—systolic and diastolic peaks are both clearly detectable.
3. Results
3.1. Participant Demographic
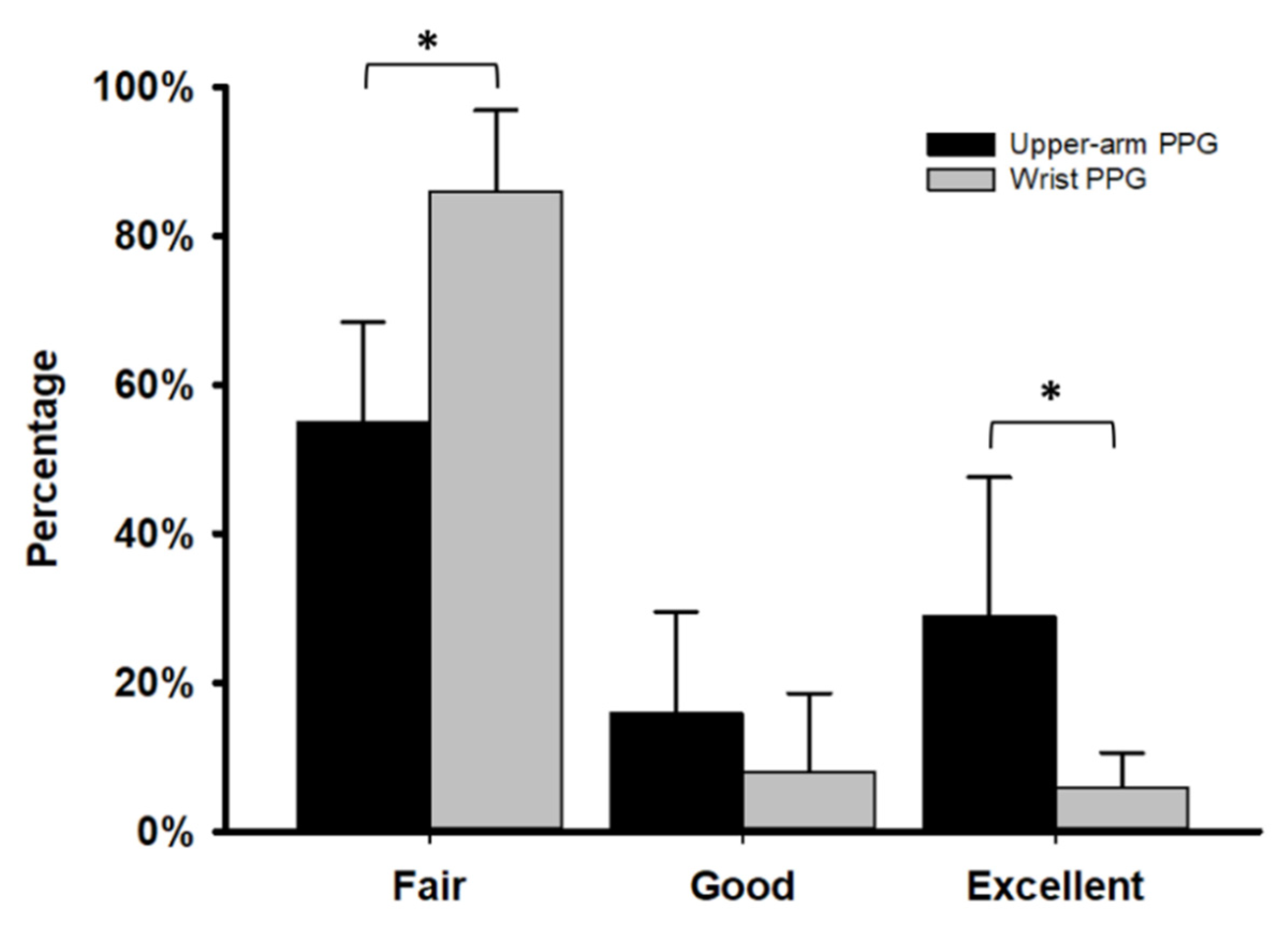
3.2. Comparison of PPG Signals from Upper-Arm, Cuffless PPG BPM and Wrist-Type PPG BPM
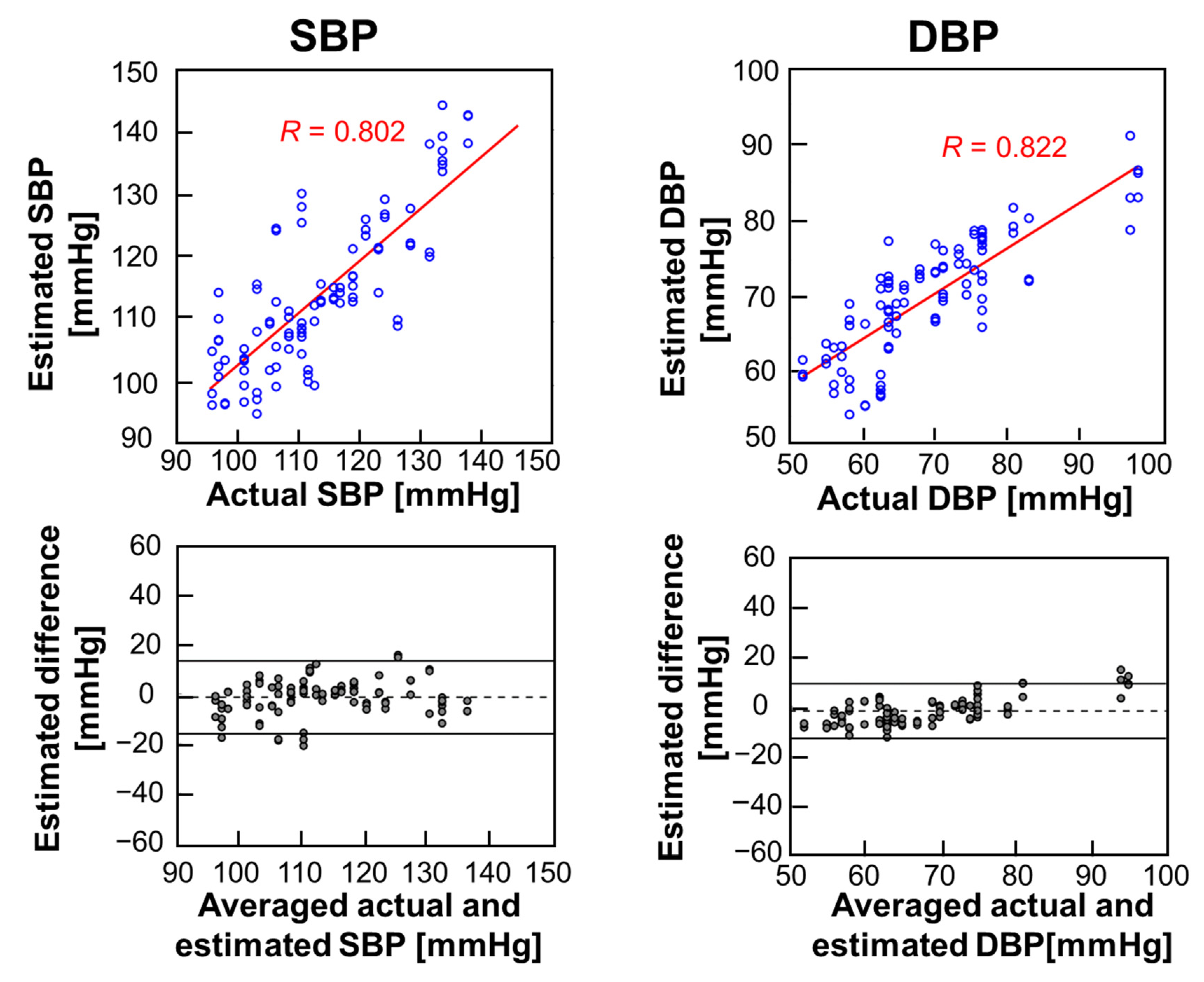
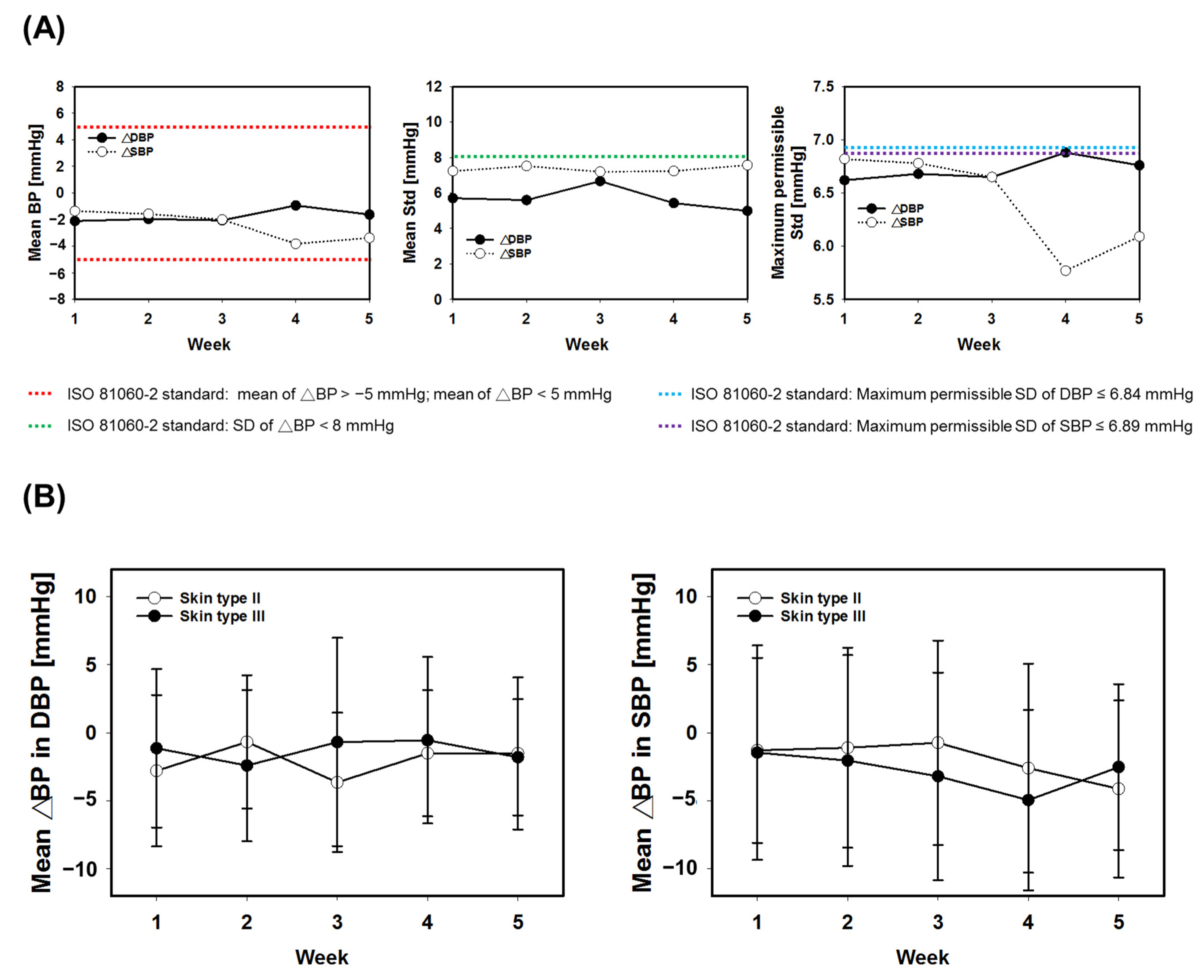
3.3. Baseline and Long-Term Performance Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [PubMed] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosendorff, C.; Lackland, D.T.; Allison, M.; Aronow, W.S.; Black, H.R.; Blumenthal, R.S.; Cannon, C.P.; de Lemos, J.A.; Elliott, W.J.; Findeiss, L.; et al. Treatment of hypertension in patients with coronary artery disease: A scientific statement from the American Heart Association, American College of Cardiology, and American Society of Hypertension. Circulation 2015, 131, e435–e470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Hypertension. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 23 December 2022).
- Wang, T.D.; Chiang, C.E.; Chao, T.H.; Cheng, H.M.; Wu, Y.W.; Wu, Y.J.; Lin, Y.H.; Chen, M.Y.; Ueng, K.C.; Chang, W.T.; et al. 2022 Guidelines of the Taiwan Society of Cardiology and the Taiwan Hypertension Society for the Management of Hypertension. Acta Cardiol. Sin. 2022, 38, 225–325. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Palatini, P.; Asmar, R.; Ioannidis, J.P.; Kollias, A.; Lacy, P.; McManus, R.J.; Myers, M.G.; Parati, G.; Shennan, A.; et al. Recommendations and Practical Guidance for performing and reporting validation studies according to the Universal Standard for the validation of blood pressure measuring devices by the Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO). J. Hypertens. 2019, 37, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Muntner, P.; Shimbo, D.; Carey, R.M.; Charleston, J.B.; Gaillard, T.; Misra, S.; Myers, M.G.; Ogedegbe, G.; Schwartz, J.E.; Townsend, R.R.; et al. Measurement of Blood Pressure in Humans: A Scientific Statement From the American Heart Association. Hypertension 2019, 73, e35–e66. [Google Scholar] [CrossRef]
- Casey, D.E., Jr.; Thomas, R.J.; Bhalla, V.; Commodore-Mensah, Y.; Heidenreich, P.A.; Kolte, D.; Muntner, P.; Smith, S.C., Jr.; Spertus, J.A.; Windle, J.R.; et al. 2019 AHA/ACC Clinical Performance and Quality Measures for Adults With High Blood Pressure: A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J. Am. Coll. Cardiol. 2019, 74, 2661–2706. [Google Scholar] [CrossRef]
- Vybornova, A.; Polychronopoulou, E.; Wurzner-Ghajarzadeh, A.; Fallet, S.; Sola, J.; Wuerzner, G. Blood pressure from the optical Aktiia Bracelet: A 1-month validation study using an extended ISO81060-2 protocol adapted for a cuffless wrist device. Blood Press. Monit. 2021, 26, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Burkard, T. The Advent of Cuffless Mobile Device Blood Pressure Measurement: Remaining Challenges and Pitfalls. Korean Circ. J. 2022, 52, 198–204. [Google Scholar] [CrossRef]
- Desebbe, O.; Tighenifi, A.; Jacobs, A.; Toubal, L.; Zekhini, Y.; Chirnoaga, D.; Collange, V.; Alexander, B.; Knebel, J.F.; Schoettker, P.; et al. Evaluation of a novel mobile phone application for blood pressure monitoring: A proof of concept study. J. Clin. Monit. Comput. 2022, 36, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Sola, J.; Cortes, M.; Perruchoud, D.; De Marco, B.; Lobo, M.D.; Pellaton, C.; Wuerzner, G.; Fisher, N.D.; Shah, J. Guidance for the Interpretation of Continual Cuffless Blood Pressure Data for the Diagnosis and Management of Hypertension. Front. med. technol. 2022, 4, 899143. [Google Scholar] [CrossRef] [PubMed]
- Vischer, A.S.; Rosania, J.; Socrates, T.; Blaschke, C.; Eckstein, J.; Proust, Y.M.; Bonnier, G.; Proenca, M.; Lemay, M.; Burkard, T. Comparability of a Blood-Pressure-Monitoring Smartphone Application with Conventional Measurements-A Pilot Study. Diagnostics 2022, 12, 749. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.-H.; Kim, J.; Lee, K.J.; Cho, D.; Oh, J.K.; Kim, M.S.; Roh, J.-H.; Park, H.-W.; Lee, J.-H. Blood Pressure Measurement Based on the Camera and Inertial Measurement Unit of a Smartphone. Research Square. 2022, 1–16. [Google Scholar] [CrossRef]
- Degott, J.; Ghajarzadeh-Wurzner, A.; Hofmann, G.; Proenca, M.; Bonnier, G.; Lemkaddem, A.; Lemay, M.; Christen, U.; Knebel, J.F.; Durgnat, V.; et al. Smartphone based blood pressure measurement: Accuracy of the OptiBP mobile application according to the AAMI/ESH/ISO universal validation protocol. Blood Press. Monit. 2021, 26, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Nachman, D.; Gepner, Y.; Goldstein, N.; Kabakov, E.; Ishay, A.B.; Littman, R.; Azmon, Y.; Jaffe, E.; Eisenkraft, A. Comparing blood pressure measurements between a photoplethysmography-based and a standard cuff-based manometry device. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Dorr, M.; Weber, S.; Birkemeyer, R.; Leonardi, L.; Winterhalder, C.; Raichle, C.J.; Brasier, N.; Burkard, T.; Eckstein, J. iPhone App compared with standard blood pressure measurement -The iPARR trial. Am. Heart J. 2021, 233, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekhar, A.; Kim, C.S.; Naji, M.; Natarajan, K.; Hahn, J.O.; Mukkamala, R. Smartphone-based blood pressure monitoring via the oscillometric finger-pressing method. Sci. Transl. Med. 2018, 10, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sagirova, Z.; Kuznetsova, N.; Gogiberidze, N.; Gognieva, D.; Suvorov, A.; Chomakhidze, P.; Omboni, S.; Saner, H.; Kopylov, P. Cuffless Blood Pressure Measurement Using a Smartphone-Case Based ECG Monitor with Photoplethysmography in Hypertensive Patients. Sensors 2021, 21, 3525. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, Z.; Liu, G.; Elgendi, M. A new, short-recorded photoplethysmogram dataset for blood pressure monitoring in China. Sci. Data 2018, 5, 180020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez, G.; Howard, N.; Abbott, D.; Lim, K.; Ward, R.; Elgendi, M. Can photoplethysmography replace arterial blood pressure in the assessment of blood pressure? J. Clin. Med. 2018, 7, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguirre, N.; Grall-Maes, E.; Cymberknop, L.J.; Armentano, R.L. Blood Pressure Morphology Assessment from Photoplethysmogram and Demographic Information Using Deep Learning with Attention Mechanism. Sensors 2021, 21, 2167. [Google Scholar] [CrossRef] [PubMed]
- Athaya, T.; Choi, S. An Estimation Method of Continuous Non-Invasive Arterial Blood Pressure Waveform Using Photoplethysmography: A U-Net Architecture-Based Approach. Sensors 2021, 21, 1867. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Chen, Z.; Ward, R.; Elgendi, M. Photoplethysmography and Deep Learning: Enhancing Hypertension Risk Stratification. Biosensors 2018, 8, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, V.; Liu, H.; Chen, F.; Qiu, Q.; Hughes, S.; Zheng, D. Quantitative Comparison of Photoplethysmographic Waveform Characteristics: Effect of Measurement Site. Front. Physiol. 2019, 10, 198. [Google Scholar] [CrossRef] [PubMed]
- Maeda, Y.; Sekine, M.; Tamura, T. Relationship between measurement site and motion artifacts in wearable reflected photoplethysmography. J. Med. Syst. 2011, 35, 969–976. [Google Scholar] [CrossRef]
- O’Brien, E.; Pickering, T.; Asmar, R.; Myers, M.; Parati, G.; Staessen, J.; Mengden, T.; Imai, Y.; Waeber, B.; Palatini, P.; et al. Working Group on Blood Pressure Monitoring of the European Society of Hypertension International Protocol for validation of blood pressure measuring devices in adults. Blood Press. Monit. 2002, 7, 3–17. [Google Scholar] [CrossRef]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1–R39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beevers, G.; Lip, G.Y.; O’Brien, E. Blood pressure measurement: Part I—Sphygmomanometry: Factors common to all techniques. Bmj 2001, 322, 981–985. [Google Scholar] [CrossRef]
- Chen, J.W.; Huang, H.K.; Fang, Y.T.; Lin, Y.T.; Li, S.Z.; Chen, B.W.; Lo, Y.C.; Chen, P.C.; Wang, C.F.; Chen, Y.Y. A Data-Driven Model with Feedback Calibration Embedded Blood Pressure Estimator Using Reflective Photoplethysmography. Sensors 2022, 22, 1873. [Google Scholar] [CrossRef]
- Dash, R.K.; Nguyen, T.N.; Cengiz, K.; Sharma, A. Fine-tuned support vector regression model for stock predictions. Neural. Comput. Appl. 2021, 1–15. [Google Scholar] [CrossRef]
- Pintea, S.L.; Karaoğlu, S.; van Gemert, J.C.; Smeulders, A.W. Large scale Gaussian Process for overlap-based object proposal scoring. Comput. Vis. Image. Underst. 2016, 150, 95–108. [Google Scholar] [CrossRef]
- Standardization, I.O.f. ISO 81060-2:2018 Non-invasive Sphygmomanometers—Part 2: Clinical Investigation of Intermittent Automated Measurement Type. 2018. Available online: https://www.doc88.com/p-8189127379736.html. (accessed on 23 December 2022).
- Kuwabara, M.; Harada, K.; Hishiki, Y.; Kario, K. Validation of two watch-type wearable blood pressure monitors according to the ANSI/AAMI/ISO81060-2: 2013 guidelines: Omron HEM-6410T-ZM and HEM-6410T-ZL. J. Clin. Hypertens 2019, 21, 853–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, J.H.; Kang, M.K.; Choi, C.E.; Min, J.; Lee, H.Y.; Lim, S. Validation of a wearable cuff-less wristwatch-type blood pressure monitoring device. Sci. Rep. 2020, 10, 19015. [Google Scholar] [CrossRef]
- Lapum, J.L.; Verkuyl, M.; Garcia, W. Vital Sign Measurement Across the Lifespan–1st Canadian Edition; OpenStax Anatomy and Physiology, eCampusOntario: Toronto, ON, Canada, 2017. [Google Scholar]
- Teng, X.; Zhang, Y.-T. The effect of contacting force on photoplethysmographic signals. Physiol. Meas. 2004, 25, 1323. [Google Scholar] [CrossRef] [PubMed]
- Scardulla, F.; D’Acquisto, L.; Colombarini, R.; Hu, S.; Pasta, S.; Bellavia, D. A study on the effect of contact pressure during physical activity on photoplethysmographic heart rate measurements. Sensors 2020, 20, 5052. [Google Scholar] [CrossRef]
- Moscato, S.; Giudice, S.L.; Massaro, G.; Chiari, L. Wrist Photoplethysmography Signal Quality Assessment for Reliable Heart Rate Estimate and Morphological Analysis. Sensors 2022, 22, 5831. [Google Scholar] [CrossRef]
- Miao, F.; Fu, N.; Zhang, Y.T.; Ding, X.R.; Hong, X.; He, Q.; Li, Y. A Novel Continuous Blood Pressure Estimation Approach Based on Data Mining Techniques. IEEE J. Biomed. Health Inform. 2017, 21, 1730–1740. [Google Scholar] [CrossRef] [PubMed]
- Gratz, I.; Deal, E.; Spitz, F.; Baruch, M.; Allen, I.E.; Seaman, J.E.; Pukenas, E.; Jean, S. Continuous non-invasive finger cuff CareTaker® comparable to invasive intra-arterial pressure in patients undergoing major intra-abdominal surgery. BMC Anesthesiol. 2017, 17, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Barvik, D.; Cerny, M.; Penhaker, M.; Noury, N. Noninvasive Continuous Blood Pressure Estimation From Pulse Transit Time: A Review of the Calibration Models. IEEE Rev. Biomed. Eng. 2022, 15, 138–151. [Google Scholar] [CrossRef]
- Mol, A.; Meskers, C.G.; Niehof, S.P.; Maier, A.B.; van Wezel, R.J. Pulse transit time as a proxy for vasoconstriction in younger and older adults. Exp. Gerontol. 2020, 135, 110938. [Google Scholar] [CrossRef]
- Lee, H.Y.; Lee, D.-J.; Seo, J.; Ihm, S.-H.; Kim, K.-i.; Cho, E.J.; Kim, H.C.; Shin, J.; Park, S.; Sohn, I.-S. Smartphone/smartwatch-based cuffless blood pressure measurement: A position paper from the Korean Society of Hypertension. Clin. Hypertens 2021, 27, 1–8. [Google Scholar] [CrossRef]
- Branan, K.L.; Reyes, G.O.F.; Abel, J.A.; Erraguntla, M.; Gutierrez-Osuna, R.; Cote, G.L. Multi-modal physiological sensing on the upper arm. In Proceedings of the Biophotonics in Exercise Science, Sports Medicine, Health Monitoring Technologies, and Wearables III, San Francisco, CA, USA, 2 March 2022; pp. 49–54. [Google Scholar]
- DeMeulenaere, S.J.T.J.f.N.P. Pulse oximetry: Uses and limitations. J. Nurse Pract. 2007, 3, 312–317. [Google Scholar] [CrossRef]
- Clement, M.; Daniel, G.; Trelles, M.J.J.o.C.; Therapy, L. Optimising the design of a broad-band light source for the treatment of skin. J. Cosmet. Laser Ther. 2005, 7, 177–189. [Google Scholar] [CrossRef]
- Spigulis, J.; Gailite, L.; Lihachev, A.; Erts, R.J.A.o. Simultaneous recording of skin blood pulsations at different vascular depths by multiwavelength photoplethysmography. Appl. Opt. 2007, 46, 1754–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ash, C.; Dubec, M.; Donne, K.; Bashford, T.J.L.i.m.s. Effect of wavelength and beam width on penetration in light-tissue interaction using computational methods. Lasers Med. Sci. 2017, 32, 1909–1918. [Google Scholar] [CrossRef] [PubMed]
- Almarshad, M.A.; Islam, M.S.; Al-Ahmadi, S.; BaHammam, A.S. Diagnostic Features and Potential Applications of PPG Signal in Healthcare: A Systematic Review. Healthcare 2022, 10, 547. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Hu, S.; Alzahrani, A.; Alharbi, S.; Blanos, P.J.B. A multi-wavelength opto-electronic patch sensor to effectively detect physiological changes against human skin types. Biosensors 2017, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Han, S.; Roh, D.; Park, J.; Shin, H.J.S. Design of multi-wavelength optical sensor module for depth-dependent photoplethysmography. Sensors 2019, 19, 5441. [Google Scholar] [CrossRef] [Green Version]
- Stergiou, G.S.; Alpert, B.; Mieke, S.; Asmar, R.; Atkins, N.; Eckert, S.; Frick, G.; Friedman, B.; Grassl, T.; Ichikawa, T.; et al. A Universal Standard for the Validation of Blood Pressure Measuring Devices: Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) Collaboration Statement. Hypertension 2018, 71, 368–374. [Google Scholar] [CrossRef]
- Ibrahim, B.; Jafari, R. Cuffless blood pressure monitoring from a wristband with calibration-free algorithms for sensing location based on bio-impedance sensor array and autoencoder. Sci. Rep. 2022, 12, 319. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n [%] | Mean ± SD | Range | |
|---|---|---|---|
| Age [year] | 30 [100%] | 26.3 ± 5.3 | 20.0–42.0 |
| Female gender | 11 [36.67%] | ||
| Male gender | 19 [63.33%] | ||
| Arm circumference [cm] | 30 | 27.2 ± 2.8 | 22.0–31.0 |
| Cuff size M–L [22–31 cm] | 30 [100%] | ||
| Skin phototype [Fitzpatrick skin type] | II, Ivory = 16 [53.33%] III, Beige = 14 [46.67%] | ||
| Long-term BP distribution [n = 90] | SBP, mmHg [Mean ± SD] | DBP, mmHg [Mean ± SD] | |
| Week 1 | 112.2 ± 11.6 | 67.7 ± 9.8 | |
| Week 2 | 110.7 ± 12.1 | 65.7 ± 9.5 | |
| Week 3 | 110.3 ± 13.8 | 66.8 ± 11.1 | |
| Week 4 | 110.4 ± 12.5 | 67.6 ± 10.0 | |
| Week 5 | 109.8 ± 12.0 | 66.7 ± 8.7 | |
| Total | 110.7 ± 12.4 | 66.9 ± 9.8 | |
| Cumulative Percentage of ∆BP [%] | |||||
|---|---|---|---|---|---|
| Grading Criteria | ≤5 [%] | ≤10 [%] | ≤15 [%] | ∆BP [mmHg] | |
| Week 1 (baseline) | DBP | 57.29† | 92.71# | 98.96# | −1.86 ± 5.50 |
| SBP | 60.42† | 82.29† | 92.70† | −1.37 ± 7.35 | |
| Week 2 | DBP | 65.59# | 91.40# | 95.70# | −1.96 ± 5.60 |
| SBP | 56.99† | 81.72† | 91.40† | −1.58 ± 7.52 | |
| Week 3 | DBP | 53.76† | 88.17† | 96.77# | −2.06 ± 6.67 |
| SBP | 50.54† | 79.57† | 91.40# | −2.00 ± 7.20 | |
| Week 4 | DBP | 64.52# | 93.55† | 98.92# | −0.94 ± 5.43 |
| SBP | 53.76† | 80.65† | 90.32† | −3.82 ± 7.24 | |
| Week 5 (1 month) | DBP | 66.67# | 93.55# | 100.0† | −1.62 ± 4.99 |
| SBP | 36.56* | 74.19* | 93.55† | −3.38 ± 7.57 | |
| Reference | Devices | Subjects [n] | Max. Calibration Interval | Estimation Errors [Mean ± SD] | |
|---|---|---|---|---|---|
| SBP | DBP | ||||
| Current Study | Microlife WatchBP O3 wearable | 30 | 1 month | −3.38 ± 7.57 | −1.62 ± 4.99 |
| Yoon et al. (2022) [14] | AlwaysBP | 15 | 1 month | 0.1 ± 8.8 | −2.4 ± 7.6 |
| Vybornova et al. (2021) [9] | Aktiia bracelet | 86 | 1 month | 0.46 ± 7.75 | 0.39 ± 6.86 |
| Miao et al. (2017) [40] | MLR- and SVR-based BP models | 10 | 6 months | −1.267 ± 5.98 (MLR) −1.148 ± 5.79 (SVR) | −1.38 ± 5.49 (MLR) −1.194 ± 5.29 (SVR) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.-F.; Wang, T.-Y.; Kuo, P.-H.; Wang, H.-L.; Li, S.-Z.; Lin, C.-M.; Chan, S.-C.; Liu, T.-Y.; Lo, Y.-C.; Lin, S.-H.; et al. Upper-Arm Photoplethysmographic Sensor with One-Time Calibration for Long-Term Blood Pressure Monitoring. Biosensors 2023, 13, 321. https://doi.org/10.3390/bios13030321
Wang C-F, Wang T-Y, Kuo P-H, Wang H-L, Li S-Z, Lin C-M, Chan S-C, Liu T-Y, Lo Y-C, Lin S-H, et al. Upper-Arm Photoplethysmographic Sensor with One-Time Calibration for Long-Term Blood Pressure Monitoring. Biosensors. 2023; 13(3):321. https://doi.org/10.3390/bios13030321
Chicago/Turabian StyleWang, Ching-Fu, Ting-Yun Wang, Pei-Hsin Kuo, Han-Lin Wang, Shih-Zhang Li, Chia-Ming Lin, Shih-Chieh Chan, Tzu-Yu Liu, Yu-Chun Lo, Sheng-Huang Lin, and et al. 2023. "Upper-Arm Photoplethysmographic Sensor with One-Time Calibration for Long-Term Blood Pressure Monitoring" Biosensors 13, no. 3: 321. https://doi.org/10.3390/bios13030321
APA StyleWang, C. -F., Wang, T. -Y., Kuo, P. -H., Wang, H. -L., Li, S. -Z., Lin, C. -M., Chan, S. -C., Liu, T. -Y., Lo, Y. -C., Lin, S. -H., & Chen, Y. -Y. (2023). Upper-Arm Photoplethysmographic Sensor with One-Time Calibration for Long-Term Blood Pressure Monitoring. Biosensors, 13(3), 321. https://doi.org/10.3390/bios13030321