
Experimental Validation of a Mathematical Framework to Simulate Antibiotics with Distinct Half-Lives Concurrently in an In Vitro Model

 , and
, and
Abstract
:1. Introduction
2. Results
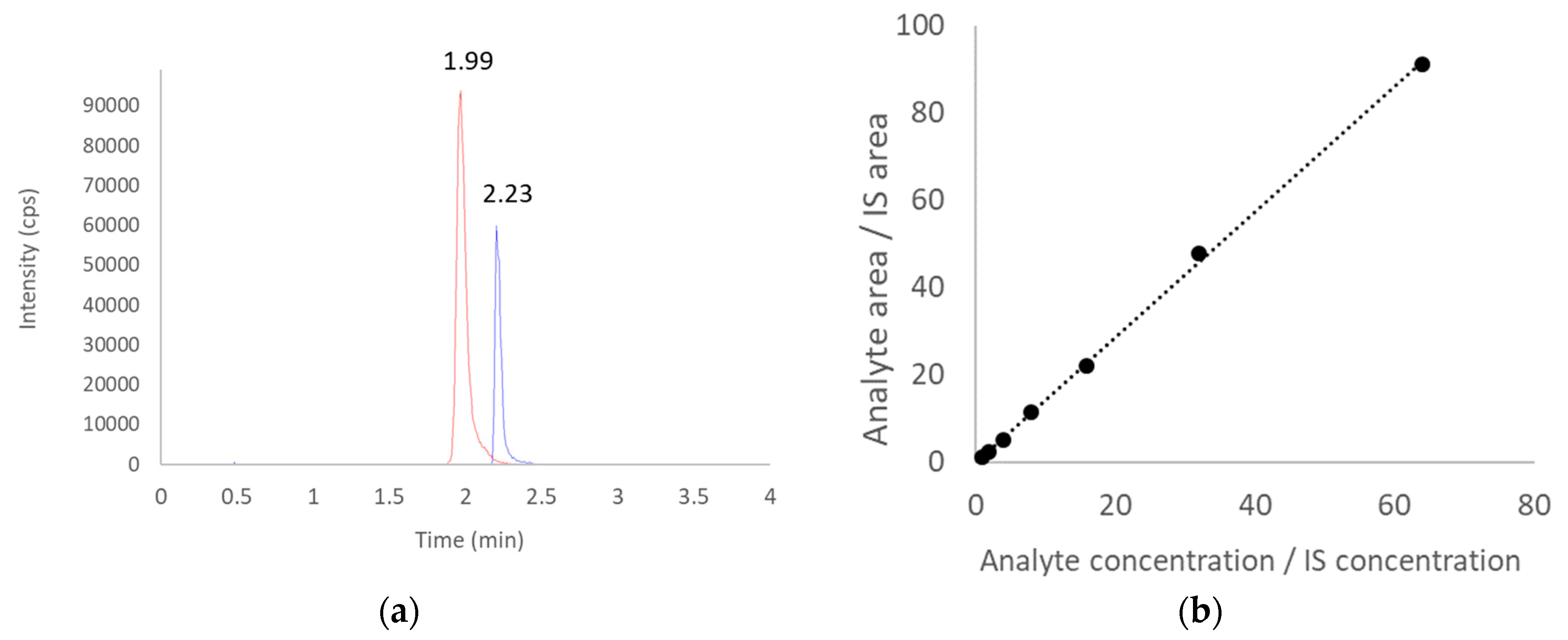
2.1. Ceftriaxone Assay Performance
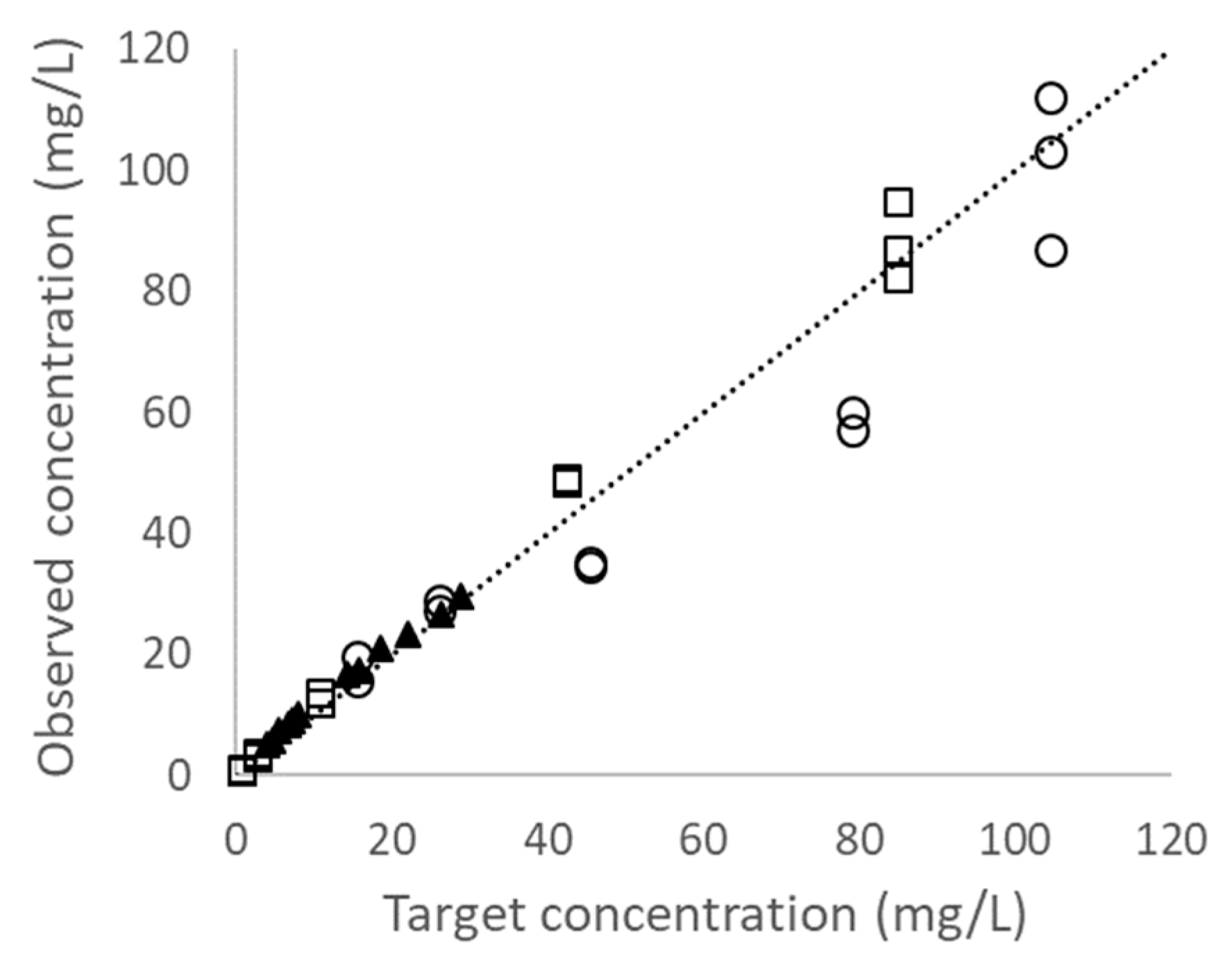
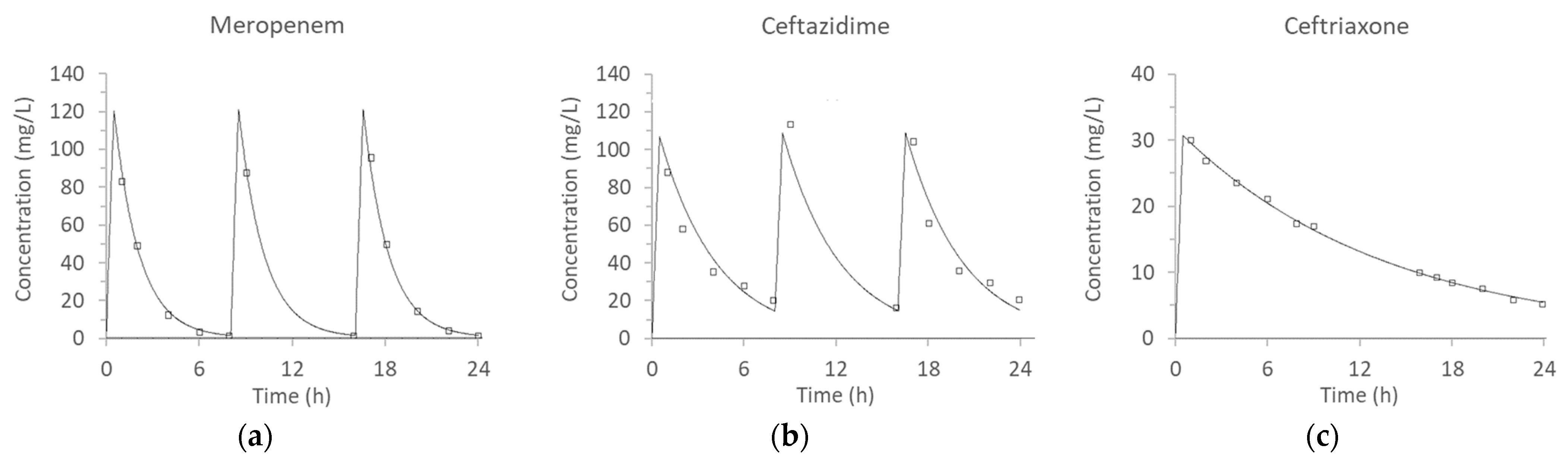
2.2. Pharmacokinetic Simulations
3. Discussion
4. Materials and Methods
4.1. Antibiotics and Chemical Reagents
4.2. Experimental Setup
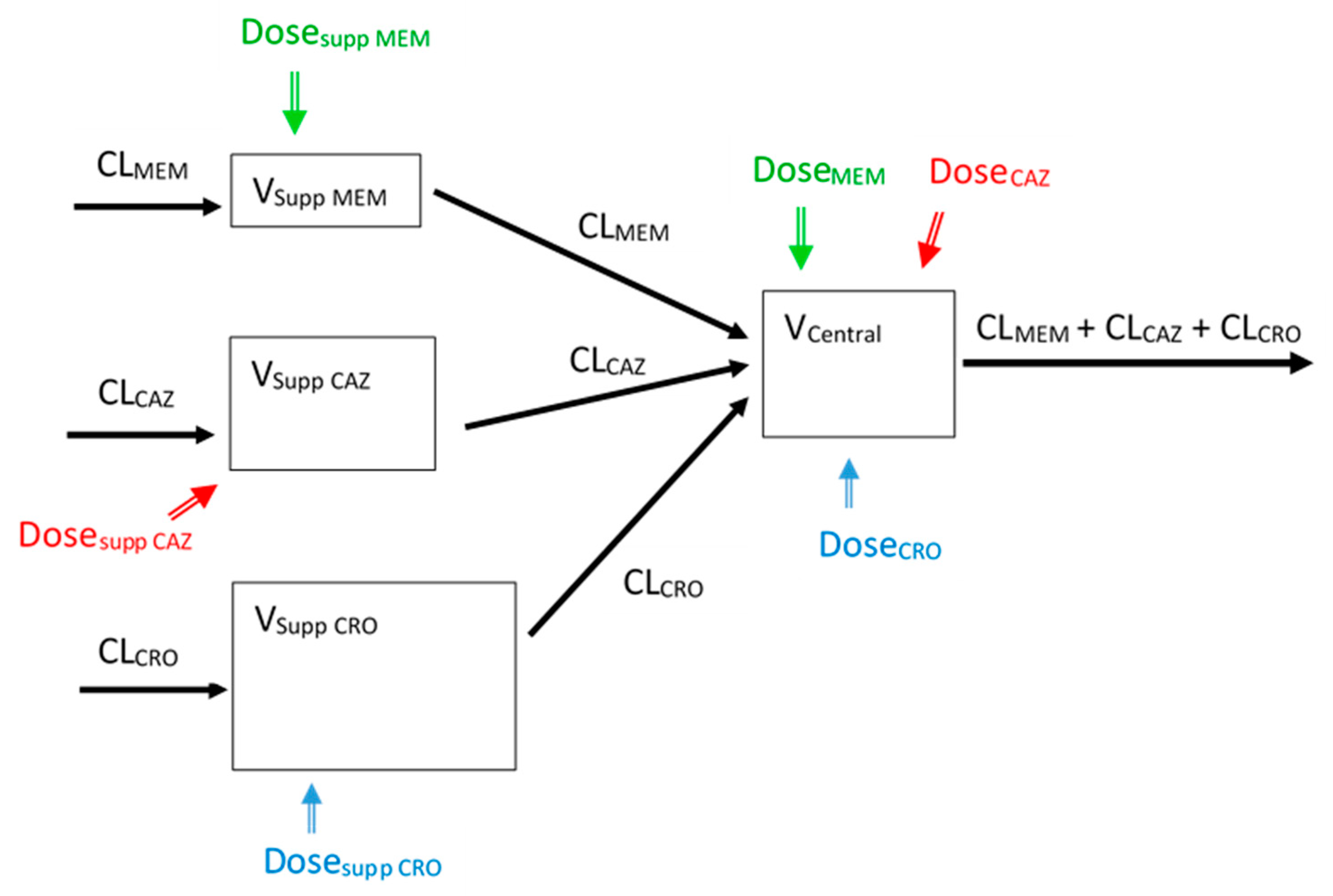
4.3. Drug Assays and Pharmacokinetic Modeling
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States; CDC: Atlanta, GA, USA, 2019.
- O’Neill, J. Review on Antimicrobial Resistance Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; Wellcome Trust: London, UK, 2014. [Google Scholar]
- Bulitta, J.B.; Hope, W.W.; Eakin, A.E.; Guina, T.; Tam, V.H.; Louie, A.; Drusano, G.L.; Hoover, J.L. Generating robust and informative nonclinical in vitro and in vivo bacterial infection model efficacy data to support translation to humans. Antimicrob. Agents Chemother. 2019, 63, e02307-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaser, J. In-vitro model for simultaneous simulation of the serum kinetics of two drugs with different half-lives. J. Antimicrob. Chemother. 1985, 15 (Suppl A), 125–130. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, B.T.; Rybak, M.J. Short-course gentamicin in combination with daptomycin or vancomycin against Staphylococcus aureus in an in vitro pharmacodynamic model with simulated endocardial vegetations. Antimicrob. Agents Chemother. 2005, 49, 2735–2745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, T.P.; Ledesma, K.R.; Chang, K.T.; Hou, J.G.; Kwa, A.L.; Nikolaou, M.; Quinn, J.P.; Prince, R.A.; Tam, V.H. Quantitative assessment of combination antimicrobial therapy against multidrug-resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2008, 52, 2898–2904. [Google Scholar] [CrossRef] [Green Version]
- Tam, V.H.; Abodakpi, H.; Wang, W.; Ledesma, K.R.; Merlau, P.R.; Chan, K.; Altman, R.; Tran, T.T.; Nikolaou, M.; Sofjan, A.K. Optimizing pharmacokinetics/pharmacodynamics of beta-lactam/beta-lactamase inhibitor combinations against high inocula of ESBL-producing bacteria. J. Antimicrob. Chemother. 2021, 76, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Lim, T.P.; Teo, J.Q.; Sasikala, S.; Chan, E.C.; Hong, Y.J.; Lee, W.; Tan, T.Y.; Tan, T.T.; Koh, T.H.; et al. Evaluating polymyxin B-based combinations against carbapenem-resistant escherichia coli in time-kill studies and in a hollow-fiber infection model. Antimicrob. Agents Chemother. 2017, 61, e01509-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steed, M.E.; Werth, B.J.; Ireland, C.E.; Rybak, M.J. Evaluation of the novel combination of high-dose daptomycin plus trimethoprim-sulfamethoxazole against daptomycin-nonsusceptible methicillin-resistant Staphylococcus aureus using an in vitro pharmacokinetic/pharmacodynamic model of simulated endocardial vegetations. Antimicrob. Agents Chemother. 2012, 56, 5709–5714. [Google Scholar] [PubMed] [Green Version]
- Drusano, G.L.; Neely, M.N.; Yamada, W.M.; Duncanson, B.; Brown, D.; Maynard, M.; Vicchiarelli, M.; Louie, A. The combination of fosfomycin plus meropenem is synergistic for Pseudomonas aeruginosa PAO1 in a hollow-fiber infection model. Antimicrob. Agents Chemother. 2018, 62, e01682-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloprogge, F.; Hammond, R.; Kipper, K.; Gillespie, S.H.; Della Pasqua, O. Mimicking in-vivo exposures to drug combinations in-vitro: Anti-tuberculosis drugs in lung lesions and the hollow fiber model of infection. Sci. Rep. 2019, 9, 13228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulman, Z.P.; Satlin, M.J.; Chen, L.; Kreiswirth, B.N.; Shin, B.S.; Walsh, T.J.; Holden, P.N.; Forrest, A.; Nation, R.L.; Li, J.; et al. New polymyxin B dosing strategies to fortify old allies in the war against KPC-2-producing Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2017, 61, e02023-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beganovic, M.; Daffinee, K.E.; Luther, M.K.; LaPlante, K.L. Minocycline alone and in combination with polymyxin B, meropenem, and sulbactam against carbapenem-susceptible and -resistant Acinetobacter baumannii in an in vitro pharmacodynamic model. Antimicrob. Agents Chemother. 2021, 65, e01680-20. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Li, X.; He, X.; Jian, L. Levofloxacin-ceftazidime administration regimens combat Pseudomonas aeruginosa in the hollow-fiber infection model simulating abnormal renal function in critically ill patients. BMC Pharmacol. Toxicol. 2020, 21, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenhard, J.R.; Smith, N.M.; Bulman, Z.P.; Tao, X.; Thamlikitkul, V.; Shin, B.S.; Nation, R.L.; Li, J.; Bulitta, J.B.; Tsuji, B.T. High-dose ampicillin-sulbactam combinations combat polymyxin-resistant Acinetobacter baumannii in a hollow-fiber infection model. Antimicrob. Agents Chemother. 2017, 61, e01268-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abodakpi, H.; Chang, K.T.; Zhou, J.; Byerly, C.; Tam, V.H. A novel framework to compare the effectiveness of beta-lactamase inhibitors against extended-spectrum beta-lactamase-producing Enterobacteriaceae. Clin. Microbiol. Infect. 2019, 25, 1154.e9–1154.e14. [Google Scholar] [CrossRef] [PubMed]
- Satta, G.; Cornaglia, G.; Foddis, G.; Pompei, R. Evaluation of ceftriaxone and other antibiotics against Escherichia coli, Pseudomonas aeruginosa, and Streptococcus pneumoniae under in vitro conditions simulating those of serious infections. Antimicrob. Agents Chemother. 1988, 32, 552–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesisoglou, I.; Eales, B.M.; Ledesma, K.R.; Merlau, P.R.; Tam, V.H.; Wang, W.; Nikolaou, M. Simultaneous in vitro simulation of multiple antimicrobial agents with different elimination half-lives in a pre-clinical infection model. Comput. Chem. Eng. 2021, 155, 107540. [Google Scholar] [CrossRef]
- Tam, V.H.; Chang, K.-T.; Zhou, J.; Ledesma, K.R.; Phe, K.; Gao, S.; Van Bambeke, F.; Sánchez-Díaz, A.M.; Zamorano, L.; Oliver, A.; et al. Determining β-lactam exposure threshold to suppress resistance development in Gram-negative bacteria. J. Antimicrob. Chemother. 2017, 72, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- D’Argenio, D.Z.; Schumitzky, A.; Wang, X. ADAPT 5 User’s Guide: Pharmacokinetic/Pharmacodynamic Systems Analysis Software; Biomedical Simulations Resource: Los Angeles, CA, USA, 2009. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotics | Cmax (mg/L) 1 | Half-Life (h) | AUC24 (mg·h/L) 2 | Equivalent Human Dosing |
|---|---|---|---|---|
| Meropenem | 120 | 1.0 | 519.5 | 2 g |
| Ceftazidime | 120 | 2.5 | 1298.7 | 2 g |
| Ceftriaxone | 30 | 8.0 | 346.3 | 2 g |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eales, B.M.; Hudson, C.S.; Kesisoglou, I.; Wang, W.; Nikolaou, M.; Tam, V.H. Experimental Validation of a Mathematical Framework to Simulate Antibiotics with Distinct Half-Lives Concurrently in an In Vitro Model. Antibiotics 2021, 10, 1256. https://doi.org/10.3390/antibiotics10101256
Eales BM, Hudson CS, Kesisoglou I, Wang W, Nikolaou M, Tam VH. Experimental Validation of a Mathematical Framework to Simulate Antibiotics with Distinct Half-Lives Concurrently in an In Vitro Model. Antibiotics. 2021; 10(10):1256. https://doi.org/10.3390/antibiotics10101256
Chicago/Turabian StyleEales, Brianna M., Cole S. Hudson, Iordanis Kesisoglou, Weiqun Wang, Michael Nikolaou, and Vincent H. Tam. 2021. "Experimental Validation of a Mathematical Framework to Simulate Antibiotics with Distinct Half-Lives Concurrently in an In Vitro Model" Antibiotics 10, no. 10: 1256. https://doi.org/10.3390/antibiotics10101256
APA StyleEales, B. M., Hudson, C. S., Kesisoglou, I., Wang, W., Nikolaou, M., & Tam, V. H. (2021). Experimental Validation of a Mathematical Framework to Simulate Antibiotics with Distinct Half-Lives Concurrently in an In Vitro Model. Antibiotics, 10(10), 1256. https://doi.org/10.3390/antibiotics10101256