
Factors Associated with Inadequate Intravenous Colistin Dosages: Post Hoc Analysis of a Multicenter, Cross-Sectional Study

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
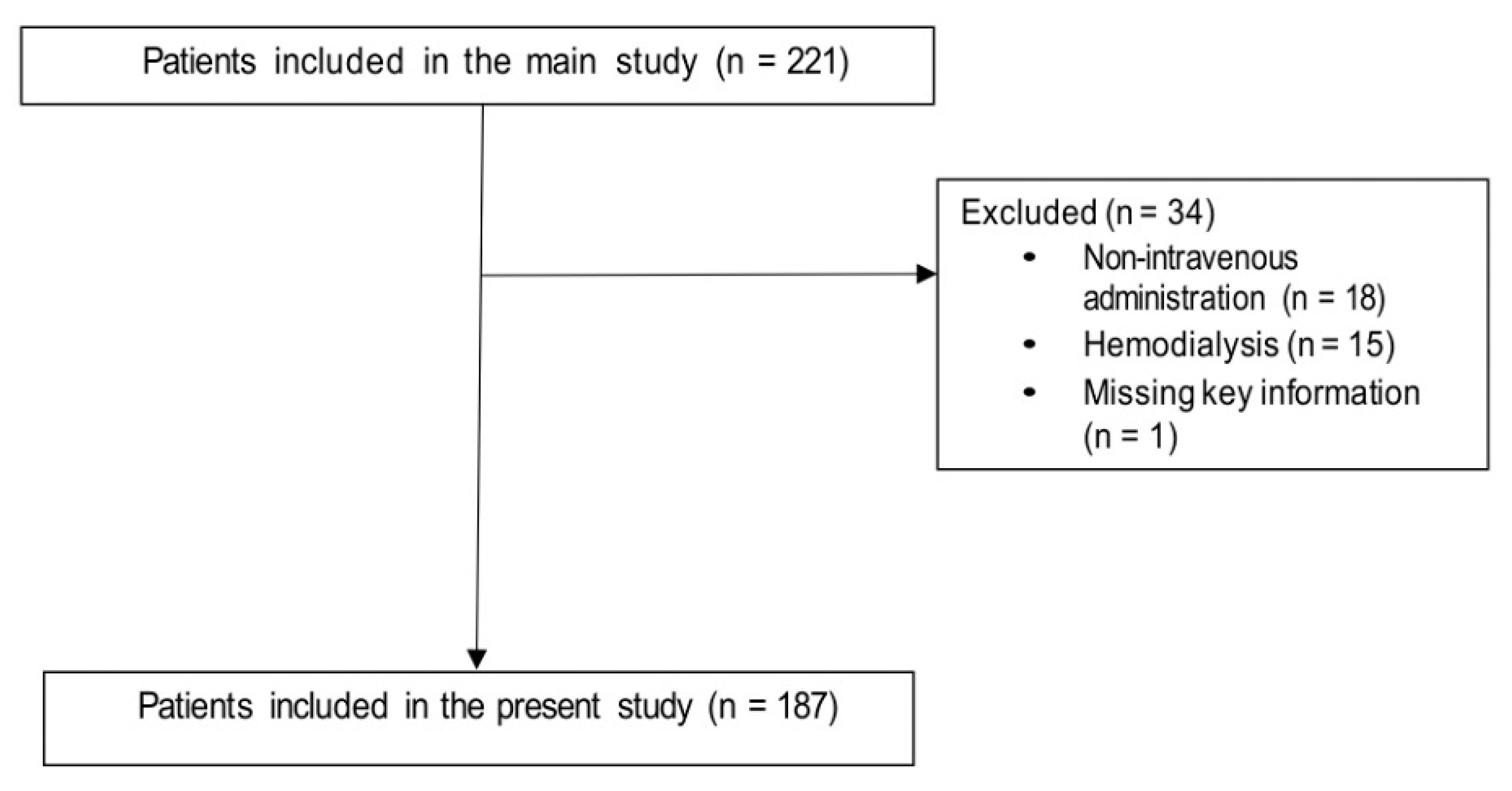
2. Methods
Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giacobbe, D.R.; Mikulska, M.; Viscoli, C. Recent advances in the pharmacological management of infections due to multidrug-resistant Gram-negative bacteria. Expert Rev. Clin. Pharmacol. 2018, 11, 1219–1236. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Souli, M.; Galani, I.; Giamarellou, H. Colistin: Still a lifesaver for the 21st century? Expert Opin. Drug Metab. Toxicol. 2017, 13, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Nang, S.C.; Azad, M.A.K.; Velkov, T.; Zhou, Q.T.; Li, J. Rescuing the Last-Line Polymyxins: Achievements and Challenges. Pharmacol. Rev. 2021, 73, 679–728. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, B.T.; Pogue, J.M.; Zavascki, A.P.; Paul, M.; Daikos, G.L.; Forrest, A.; Giacobbe, D.R.; Viscoli, C.; Giamarellou, H.; Karaiskos, I.; et al. International Consensus Guidelines for the Optimal Use of the Polymyxins: Endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy 2019, 39, 10–39. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; di Masi, A.; Leboffe, L.; Del Bono, V.; Rossi, M.; Cappiello, D.; Coppo, E.; Marchese, A.; Casulli, A.; Signori, A.; et al. Hypoalbuminemia as a predictor of acute kidney injury during colistin treatment. Sci. Rep. 2018, 8, 11968. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Labate, L.; Russo, C.; Vena, A.; Giacobbe, D.R. Therapeutic options for difficult-to-treat Acinetobacter baumannii infections: A 2020 perspective. Expert Opin. Pharm. 2021, 22, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Galani, I.; Papoutsaki, V.; Galani, L.; Giamarellou, H. Carbapenemase producing Klebsiella pneumoniae: Implication on future therapeutic strategies. Expert Rev. Anti. Infect. Ther. 2021, 19, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Nation, R.L.; Forrest, A. Clinical Pharmacokinetics, Pharmacodynamics and Toxicodynamics of Polymyxins: Implications for Therapeutic Use. Adv. Exp. Med. Biol. 2019, 1145, 219–249. [Google Scholar] [CrossRef] [PubMed]
- Nation, R.L.; Garonzik, S.M.; Thamlikitkul, V.; Giamarellos-Bourboulis, E.J.; Forrest, A.; Paterson, D.L.; Li, J.; Silveira, F.P. Dosing guidance for intravenous colistin in critically-ill patients. Clin. Infect. Dis. 2017, 64, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Nation, R.L.; Rigatto, M.H.P.; Falci, D.R.; Zavascki, A.P. Polymyxin Acute Kidney Injury: Dosing and Other Strategies to Reduce Toxicity. Antibiotics 2019, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacobbe, D.R.; Saffioti, C.; Losito, A.R.; Rinaldi, M.; Aurilio, C.; Bolla, C.; Boni, S.; Borgia, G.; Carannante, N.; Cassola, G.; et al. Use of colistin in adult patients: A cross-sectional study. J. Glob. Antimicrob. Resist. 2020, 20, 43–49. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency Completes Review of Polymyxin-Based Medicines. Recommendations Issued for Safe Use in Patients with Serious Infections Resistant to Standard Antibiotics. Annex III. Available online: https://www.ema.europa.eu/documents/referral/polymyxin-article-31-referral-annex-iii_en.pdf (accessed on 21 November 2021).
- Giacobbe, D.R.; Karaiskos, I.; Bassetti, M. How do we optimize the prescribing of intravenous polymyxins to increase their longevity and efficacy in critically ill patients? Expert Opin. Pharm. 2021, 10, 1961743. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Patients Receiving Inadequate Dosage (%) (n = 50) | Patients Receiving Adequate Dosage (%) (n = 137) | OR (95% CI) | p |
|---|---|---|---|---|
| Age in years, median IQR | 69 (53–80) | 61 (48–71) | 1.03 (1.00–1.05) | 0.021 |
| Male gender | 32 (64) | 81 (59) | 1.23 (0.63–2.40) | 0.547 |
| Previous treatment with colistin | 8 (16) | 20 (15) | 1.11 (0.46–2.72) | 0.812 |
| Hospital stay before colistin initiation in days, median (IQR) | 17 (4–40) | 23 (13–50) | 1.00 (0.99–1.01) | 0.960 |
| ICU stay | 22 (44) | 56 (41) | 1.13 (0.59–2.19) | 0.701 |
| Diabetes mellitus | 15 (30) | 27 (20) | 1.75 (0.84–3.65) | 0.138 |
| Chronic renal failure | 5 (10) | 3 (2) | 4.96 (1.14–21.60) | 0.033 |
| Solid neoplasm | 10 (20) | 23 (17) | 1.24 (0.54–2.83) | 0.611 |
| Hematological malignancy | 2 (4) | 13 (9) | 0.40 (0.09–1.83) | 0.236 |
| Charlson score, median (IQR) | 2 (1–3) | 2 (1–3) | 1.12 (0.97–1.29) | 0.136 |
| Presence of CVC | 30 (60) | 109 (80) | 0.39 (0.19–0.78) | 0.008 |
| Presence of urinary catheter | 39 (78) | 113 (82) | 0.75 (0.34–1.68) | 0.488 |
| Mechanical ventilation | 18 (36) | 37 (27) | 1.52 (0.76–3.03) | 0.234 |
| Neutropenia | 2 (4) | 11 (8) | 0.48 (0.10–2.23) | 0.347 |
| Septic shock | 12 (24) | 27 (20) | 1.29 (0.59–2.79) | 0.523 |
| Pulmonary infection | 15 (30) | 44 (32) | 0.91 (0.45–1.83) | 0.783 |
| KDIGO stage of AKI | 0.002 | |||
| No AKI | 31 (62) | 120 (88) | (ref) | |
| Stage 1 | 10 (20) | 10 (7) | 3.87 (1.48–10.12) | |
| Stage 2 | 5 (10) | 5 (4) | 3.87 (1.05–14.22) | |
| Stage 3 | 4 (8) | 2 (1) | 7.74 (1.36–44.23) | |
| Type of prescriber § | 0.346 | |||
| Infectious diseases specialist | 36 (72) | 109 (81) | (ref) | |
| Intensive care specialist | 10 (20) | 16 (12) | 1.89 (0.79–4.54) | |
| Others §§ | 4 (8) | 9 (7) | 1.35 (0.39–4.63) | |
| Targeted therapy §§§ | 40 (80) | 101 (74) | 1.43 (0.65–3.14) | 0.379 |
| Combination therapy | 42 (84) | 108 (79) | 1.41 (0.60–3.33) | 0.434 |
| Model A (AIC 204.5) | OR (95% CI) | p |
| Presence of CVC | 0.34 (0.16–0.72) | 0.004 § |
| KDIGO stage of AKI | 0.001 § | |
| No AKI | (ref) | |
| Stage 1 | 3.98 (1.48–10.74) | |
| Stage 2 | 4.44 (1.17–16.93) | |
| Stage 3 | 9.41 (1.59–55.70) | |
| Model B ** (AIC 199.4) | OR (95% CI) | p |
| Presence of CVC | 0.33 (0.15–0.75) | 0.008 § |
| KDIGO stage of AKI | 0.002 § | |
| No AKI | (ref) | |
| Stage 1 | 4.73 (1.56–14.37) | |
| Stage 2 | 4.83 (105–22.22) | |
| Stage 3 | 8.23 (1.20–56.64) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giacobbe, D.R.; Mirabella, M.; Rinaldi, M.; Losito, A.R.; Raffaelli, F.; Del Puente, F.; Saffioti, C.; Mikulska, M.; Giannella, M.; Viale, P.; et al. Factors Associated with Inadequate Intravenous Colistin Dosages: Post Hoc Analysis of a Multicenter, Cross-Sectional Study. Antibiotics 2021, 10, 1554. https://doi.org/10.3390/antibiotics10121554
Giacobbe DR, Mirabella M, Rinaldi M, Losito AR, Raffaelli F, Del Puente F, Saffioti C, Mikulska M, Giannella M, Viale P, et al. Factors Associated with Inadequate Intravenous Colistin Dosages: Post Hoc Analysis of a Multicenter, Cross-Sectional Study. Antibiotics. 2021; 10(12):1554. https://doi.org/10.3390/antibiotics10121554
Chicago/Turabian StyleGiacobbe, Daniele Roberto, Michele Mirabella, Matteo Rinaldi, Angela Raffaella Losito, Francesca Raffaelli, Filippo Del Puente, Carolina Saffioti, Malgorzata Mikulska, Maddalena Giannella, Pierluigi Viale, and et al. 2021. "Factors Associated with Inadequate Intravenous Colistin Dosages: Post Hoc Analysis of a Multicenter, Cross-Sectional Study" Antibiotics 10, no. 12: 1554. https://doi.org/10.3390/antibiotics10121554
APA StyleGiacobbe, D. R., Mirabella, M., Rinaldi, M., Losito, A. R., Raffaelli, F., Del Puente, F., Saffioti, C., Mikulska, M., Giannella, M., Viale, P., Tumbarello, M., Bassetti, M., & on behalf of SITA GIOVANI (Young Investigators Group of the Società Italiana Terapia Antinfettiva) and the COLI-CROSS Study Group. (2021). Factors Associated with Inadequate Intravenous Colistin Dosages: Post Hoc Analysis of a Multicenter, Cross-Sectional Study. Antibiotics, 10(12), 1554. https://doi.org/10.3390/antibiotics10121554