
Impact of Prior Antibiotic Use in Primary Care on Escherichia coli Resistance to Third Generation Cephalosporins: A Case-Control Study

 , , and
, , and
Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Summary of Main Findings
3.2. Comparison to Existing Literature
3.3. Strengths and Limitations
4. Materials and Methods
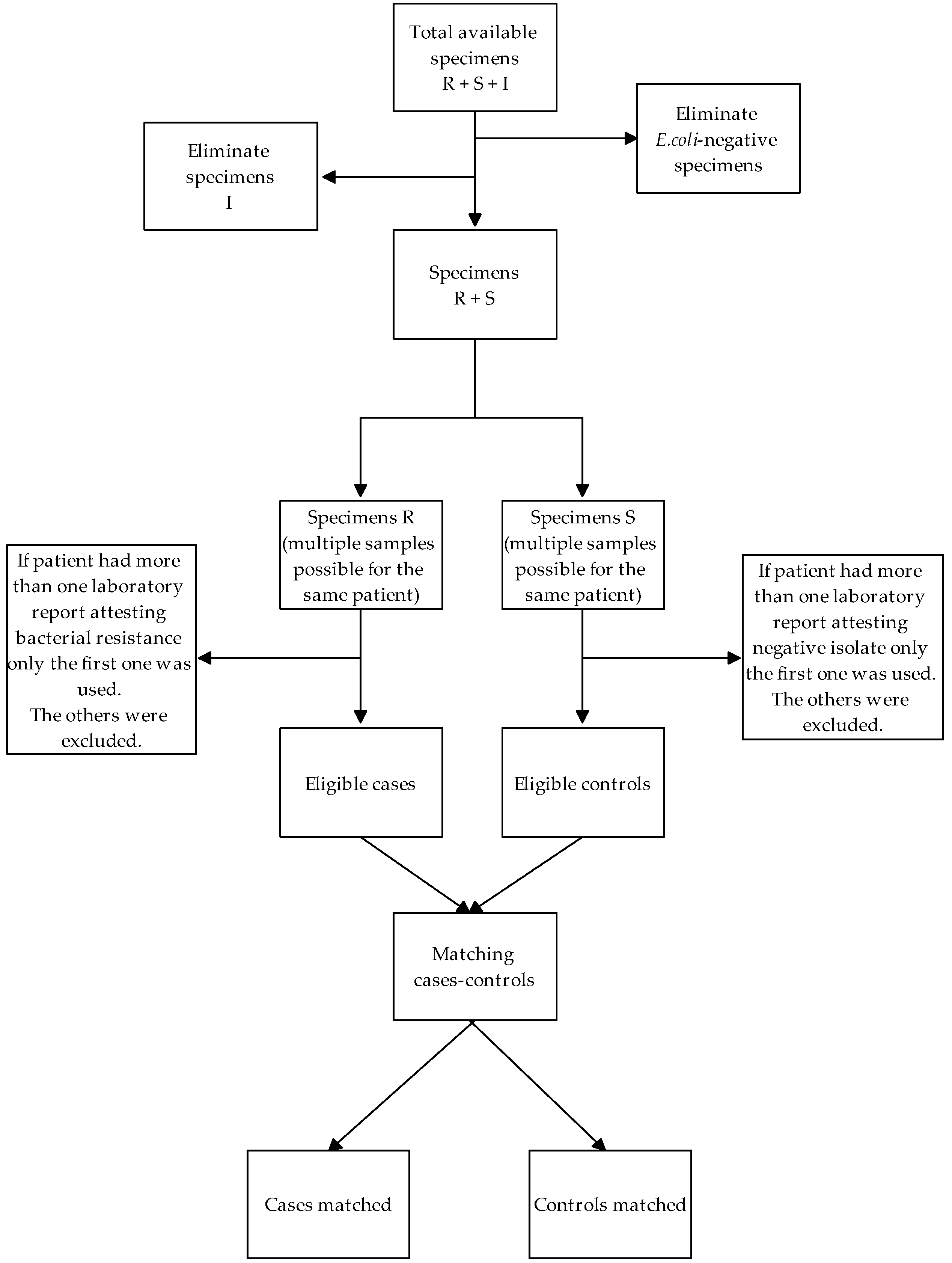
4.1. Study Design, Setting and Data Sources
- The database of hospital laboratories of the Autonomous Province of Bolzano/Bozen that was used to define cases and controls.
- The database of outpatient pharmaceutical prescriptions of the Bolzano/Bozen Local Health Trust, that was used to define the exposure.
- The hospital discharge record database of the Autonomous Province of Bolzano/Bozen, that was used to identify potential risk factors.
4.2. Definition of Exposure
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aminov, R.I. A brief history of the antibiotic era: Lessons learned and challenges for the future. Front. Microbiol. 2010, 1, 134. [Google Scholar] [CrossRef] [Green Version]
- Sykes, R. The 2009 Garrod Lecture: The evolution of antimicrobial resistance: A Darwinian perspective. J. Antimicrob. Chemother. 2010, 65, 1842–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiltunen, T.; Virta, M.; Laine, A.L. Antibiotic resistance in the wild: An eco-evolutionary perspective. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372. [Google Scholar] [CrossRef] [PubMed]
- Hollis, A.; Ahmed, Z. Preserving Antibiotics, Rationally. N. Engl. J. Med. 2013, 369, 2474–2476. [Google Scholar] [CrossRef] [Green Version]
- Biswas, R.; Halder, U.; Kabiraj, A.; Mondal, A.; Bandopadhyay, R. Overview on the role of heavy metals tolerance on developing antibiotic resistance in both Gram-negative and Gram-positive bacteria. Arch. Microbiol. 2021. [Google Scholar] [CrossRef]
- Cassini, A.; Hogberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption Surveillance in Europe 2018; Annual Report of the European Antimicrobial Consumption Surveillance Network (ESAC-Net); ECDC: Stockholm, Sweden, 2019. [Google Scholar]
- Osservatorio Nazionale Sull’Impiego dei Medicinali. L’uso degli antibiotici in Italia. Rapporto Nazionale 2019; Agenzia Italiana del Farmaco (AIFA): Roma, Italy, 2020.
- MacKinnon, M.C.; Sargeant, J.M.; Pearl, D.L.; Reid-Smith, R.J.; Carson, C.A.; Parmley, E.J.; McEwen, S.A. Evaluation of the health and healthcare system burden due to antimicrobial-resistant Escherichia coli infections in humans: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2020, 9, 200. [Google Scholar] [CrossRef]
- ECDC. Antimicrobial Resistance Surveillance in Europe 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2019 (accessed on 26 December 2020).
- Peñalva, G.; Högberg, L.D.; Weist, K.; Vlahović-Palčevski, V.; Heuer, O.; Monnet, D.L. Decreasing and stabilising trends of antimicrobial consumption and resistance in Escherichia coli and Klebsiella pneumoniae in segmented regression analysis, European Union/European Economic Area, 2001 to 2018. Eurosurveillance 2019, 24, 1900656. [Google Scholar] [CrossRef]
- Alvarez-Uria, G.; Gandra, S.; Mandal, S.; Laxminarayan, R. Global forecast of antimicrobial resistance in invasive isolates of Escherichia coli and Klebsiella pneumoniae. Int. J. Infect. Dis. 2018, 68, 50–53. [Google Scholar] [CrossRef] [Green Version]
- Bellino, S.; Iacchini, S.; Monaco, M.; Del Grosso, M.; Camilli, R.; Errico, G.; D’Ancona, F.; Pantosti, A.; Pezzotti, P.; Maraglino, F.; et al. AR-ISS: Sorveglianza Nazionale Dell’antibiotico-Resistenza. Dati 2019; Rapporti ISS Sorveglianza RIS-1/2020; Istituto Superiore di Sanità: Roma, Italy, 2020; Available online: https://www.epicentro.iss.it/antibiotico-resistenza/ar-iss (accessed on 26 December 2020).
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakhit, M.; Hoffmann, T.; Scott, A.M.; Beller, E.; Rathbone, J.; Del Mar, C. Resistance decay in individuals after antibiotic exposure in primary care: A systematic review and meta-analysis. BMC Med. 2018, 16, 126. [Google Scholar] [CrossRef]
- Kurotschka, P.K.; Serafini, A.; Massari, M.; Da Cas, R.; Figueiras, A.; Forte, V.; Moro, M.F.; Massidda, M.; Contu, F.; Minerba, L.; et al. Broad Spectrum project: Factors determining the quality of antibiotic use in primary care: An observational study protocol from Italy. BMJ Open 2020, 10, e038843. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Marotta, C.; Amicone, M.; Bavaro, D.F.; Bernaudo, F.; Frisicale, E.M.; Kurotschka, P.K.; Mazzari, A.; Veronese, N.; Murri, R.; et al. Italian Young Doctors’ knowledge, attitude and practices on antibiotic use and resistance: A national cross-sectional survey. J. Glob. Antimicrob. Resist. 2020. [Google Scholar] [CrossRef]
- Yang, P.; Chen, Y.; Jiang, S.; Shen, P.; Lu, X.; Xiao, Y. Association between the rate of third generation cephalosporin-resistant Escherichia coli and Klebsiella pneumoniae and antibiotic consumption based on 143 Chinese tertiary hospitals data in 2014. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1495–1502. [Google Scholar] [CrossRef]
- Donnan, P.T.; Wei, L.; Steinke, D.T.; Phillips, G.; Clarke, R.; Noone, A.; Sullivan, F.M.; MacDonald, T.M.; Davey, P.G. Presence of bacteriuria caused by trimethoprim resistant bacteria in patients prescribed antibiotics: Multilevel model with practice and individual patient data. BMJ 2004, 328, 1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, A.D.; Thomas, M.; Montgomery, A.; Wetherell, M.; Lovering, A.; McNulty, C.; Lewis, D.; Carron, B.; Henderson, E.; MacGowan, A. The relationship between primary care antibiotic prescribing and bacterial resistance in adults in the community: A controlled observational study using individual patient data. J. Antimicrob. Chemother. 2005, 56, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.; Roberts, Z.; Dunstan, F.; Butler, C.; Howard, A.; Palmer, S. Prior antibiotics and risk of antibiotic-resistant community-acquired urinary tract infection: A case-control study. J. Antimicrob. Chemother. 2007, 60, 92–99. [Google Scholar] [CrossRef]
- Lin, W.-P.; Huang, Y.-S.; Wang, J.-T.; Chen, Y.-C.; Chang, S.-C. Prevalence of and risk factor for community-onset third-generation cephalosporin-resistant Escherichia coli bacteremia at a medical center in Taiwan. BMC Infect. Dis. 2019, 19, 245. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, M.C.; Oliveira, C.R.A.; Gonçalves, K.V.; Santos, M.S.; Tardelli, A.C.S.; Nobre, V.A., Jr. Enterobacteriaceae resistant to third generation cephalosporins upon hospital admission: Risk factors and clinical outcomes. Braz. J. Infect. Dis. 2015, 19, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Kraker, M.E.A.; Wolkewitz, M.; Davey, P.G.; Koller, W.; Berger, J.; Nagler, J.; Icket, C.; Kalenic, S.; Horvatic, J.; Seifert, H.; et al. Burden of antimicrobial resistance in European hospitals: Excess mortality and length of hospital stay associated with bloodstream infections due to Escherichia coli resistant to third-generation cephalosporins. J. Antimicrob. Chemother. 2010, 66, 398–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chervet, D.; Lortholary, O.; Zahar, J.R.; Dufougeray, A.; Pilmis, B.; Partouche, H. Antimicrobial resistance in community-acquired urinary tract infections in Paris in 2015. Med. Mal. Infect. 2018, 48, 188–192. [Google Scholar] [CrossRef]
- McDanel, J.; Schweizer, M.; Crabb, V.; Nelson, R.; Samore, M.; Khader, K.; Blevins, A.E.; Diekema, D.; Chiang, H.Y.; Nair, R.; et al. Incidence of Extended-Spectrum β-Lactamase (ESBL)-Producing Escherichia coli and Klebsiella Infections in the United States: A Systematic Literature Review. Infect. Control Hosp. Epidemiol. 2017, 38, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Brolund, A.; Edquist, P.J.; Mäkitalo, B.; Olsson-Liljequist, B.; Söderblom, T.; Wisell, K.T.; Giske, C.G. Epidemiology of extended-spectrum β-lactamase-producing Escherichia coli in Sweden 2007-2011. Clin. Microbiol. Infect. 2014, 20, O344–O352. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Baño, J.; Navarro, M.D.; Romero, L.; Martínez-Martínez, L.; Muniain, M.A.; Perea, E.J.; Pérez-Cano, R.; Pascual, A. Epidemiology and clinical features of infections caused by extended-spectrum beta-lactamase-producing Escherichia coli in nonhospitalized patients. J. Clin. Microbiol. 2004, 42, 1089–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Baño, J.; Alcalá, J.C.; Cisneros, J.M.; Grill, F.; Oliver, A.; Horcajada, J.P.; Tórtola, T.; Mirelis, B.; Navarro, G.; Cuenca, M.; et al. Community Infections Caused by Extended-Spectrum β-Lactamase–Producing Escherichia coli. Arch. Intern. Med. 2008, 168, 1897–1902. [Google Scholar] [CrossRef] [Green Version]
- Latry, P.; Molimard, M.; Bégaud, B.; Martin-Latry, K. How reimbursement databases can be used to support drug utilisation studies: Example using the main French national health insurance system database. Eur. J. Clin. Pharm. 2010, 66, 743–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ISTAT—Direzione Centrale Per le Statistiche e le Indagini Sulle Istituzioni Sociali, Popolazione Residente al 1° Gennaio 2019. Available online: http://demo.istat.it (accessed on 10 March 2021).
- WHO Collaborating Centre for Drug Statistics Methodology. Anatomical Therapeutic Chemical (ATC) Classification System: Guidelines for ATC Classification and DDD Assignment; Norwegian Institute of Public Health: Oslo, Norway, 2020; Available online: https://www.whocc.no/filearchive/publications/2020_guidelines_web.pdf (accessed on 6 September 2020).
- Geraci, J.M.; Ashton, C.M.; Kuykendall, D.H.; Johnson, M.L.; Wu, L. International Classification of Diseases. 9th Revision, 5th ed.; Clinical Modification; Medicode: Salt Lake City, UT, USA, 1995. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LLC: College Station, TX, USA, 2013; Available online: https://www.stata.com/support/faqs/resources/citing-software-documentation-faqs/ (accessed on 15 April 2021).
- R Core Team. R: A Language and Environment for Statistical Computing [Internet]. 2016. Available online: https://www.R-project.org/ (accessed on 27 February 2021).




{kind=link}
{kind=link}
{kind=link}
| Variable | Cases a | Controls a | Crude OR (95% CI) | p |
|---|---|---|---|---|
| Age, Median (IQ) | 79 (68–85) | 76 (61–84) | 1.11 b (1.04–1.20) | 0.003 |
| Gender | ||||
| Male (%) | 106 (43.98) | 530 (34.13) | 1.49 (1.14–1.98) | 0.004 |
| Hospitalization ward | ||||
| Other (%) | 4 (1.66) | 12 (0.77) | - | |
| Surgery (%) | 82 (34.02) | 597 (38.44) | 0.44 (0.14–1.41) | 0.167 |
| Intensive care unit (%) | 12 (4.98) | 78 (5.02) | 0.47 (0.13–1.71) | 0.252 |
| Medicine unit (%) | 143 (59.34) | 866 (55.76) | 0.54 (0.17–1.71) | 0.296 |
| Drug’s DDD taken in previous 5 years, Median (IQ) | 4334.15 (1092.92–7802.62) | 3117.01 (414.83–6392.25) | 1.04 c (1.01–1.06) | 0.016 |
| Number of active ingredients taken in previous 5 years, Median (IQ) | 16 (9–24) | 12 (5–19) | 1.04 (1.03–1.05) | <0.0001 |
| At least one cortisone drug’s DDD taken in previous 5 years (%) | 29 (12.03) | 139 (8.95) | 1.38 (0.90–2.13) | 0.144 |
| Number of antibiotics taken in previous 5 years, Median (IQ) | 3 (1–4) | 2 (0–3) | 1.27 (1.19–1.35) | <0.0001 |
| At least one J01 prescription taken in previous period (%) | ||||
| I year | 161 (66.80) | 681 (43.85) | 2.69 (2.00–3.61) | <0.0001 |
| II year | 127 (52.70) | 626 (40.31) | 1.65 (1.26–2.17) | <0.0001 |
| III–V years | 161 (66.80) | 879 (56.60) | 1.59 (1.19–2.12) | 0.002 |
| At least one 3GC prescription in previous year (%) | ||||
| 0 | 212 (87.97) | 1437 (92.53) | - | - |
| 1 | 12 (4.98) | 78 (5.02) | 1.04 (0.56–1.95) | 0.898 |
| 2+ | 17 (7.05) | 38 (2.45) | 3.23 (1.78–5.87) | <0.0001 |
| Hospitalization days, Median (IQ) | 47 (8–97) | 12 (0–46) | 1.05 d (1.04–1.07) | <0.0001 |
| Hospitalization with surgery (%) | 177 (48.55) | 642 (41.34) | 1.32 (1.01–1.73) | 0.044 |
| Hospitalization with device implantation (%) | 29 (12.03) | 127 (8.18) | 1.52 (0.98–2.34) | 0.059 |
| Hospitalization with organ transplant (%) | 6 (2.49) | 26 (1.67) | 1.59 (0.65–3.88) | 0.305 |
| Diagnosis of chronic diseases | ||||
| Cancer (%) | 59 (24.48) | 270 (17.51) | 1.52 (1.10–2.11) | 0.012 |
| Diabetes (%) | 61 (25.31) | 251 (16.16) | 1.79 (1.29–2.47) | <0.0001 |
| AIDS (%) | 0 (0.00) | 2 (0.13) | NA | NA |
| COPD (%) | 86 (35.68) | 461 (29.68) | 1.39 (1.03–1.87) | 0.031 |
| Immunosuppression (%) | 0 (0.00) | 2 (0.13) | NA | NA |
| Haemodialysis (%) | 7 (2.90) | 29 (1.87) | 1.22 (1.06–1.40) | 0.005 |
| Variables | Cases a | Controls a | Adj OR (95% CI) | p |
|---|---|---|---|---|
| Age, Median (IQ) | 79 (68–85) | 76 (61–84) | 1.11 b (1.02–1.21) | <0.0001 |
| Gender, Male (%) | 106 (43.98) | 530 (34.13) | 1.49 (1.10–2.01) | 0.009 |
| Drug’s DDD taken in previous 5 years, Median (IQ) | 4334.15 (1092.92–7802.62) | 3117.01 (414.83–6392.25) | 0.95 c (0.91–0.99) | 0.013 |
| Number of antibiotics taken in previous 5 years, Median (IQ) | 3 (1–4) | 2 (0–3) | 1.20 (1.08–1.33) | 0.001 |
| At least one J01 prescription taken in previous period (%) | ||||
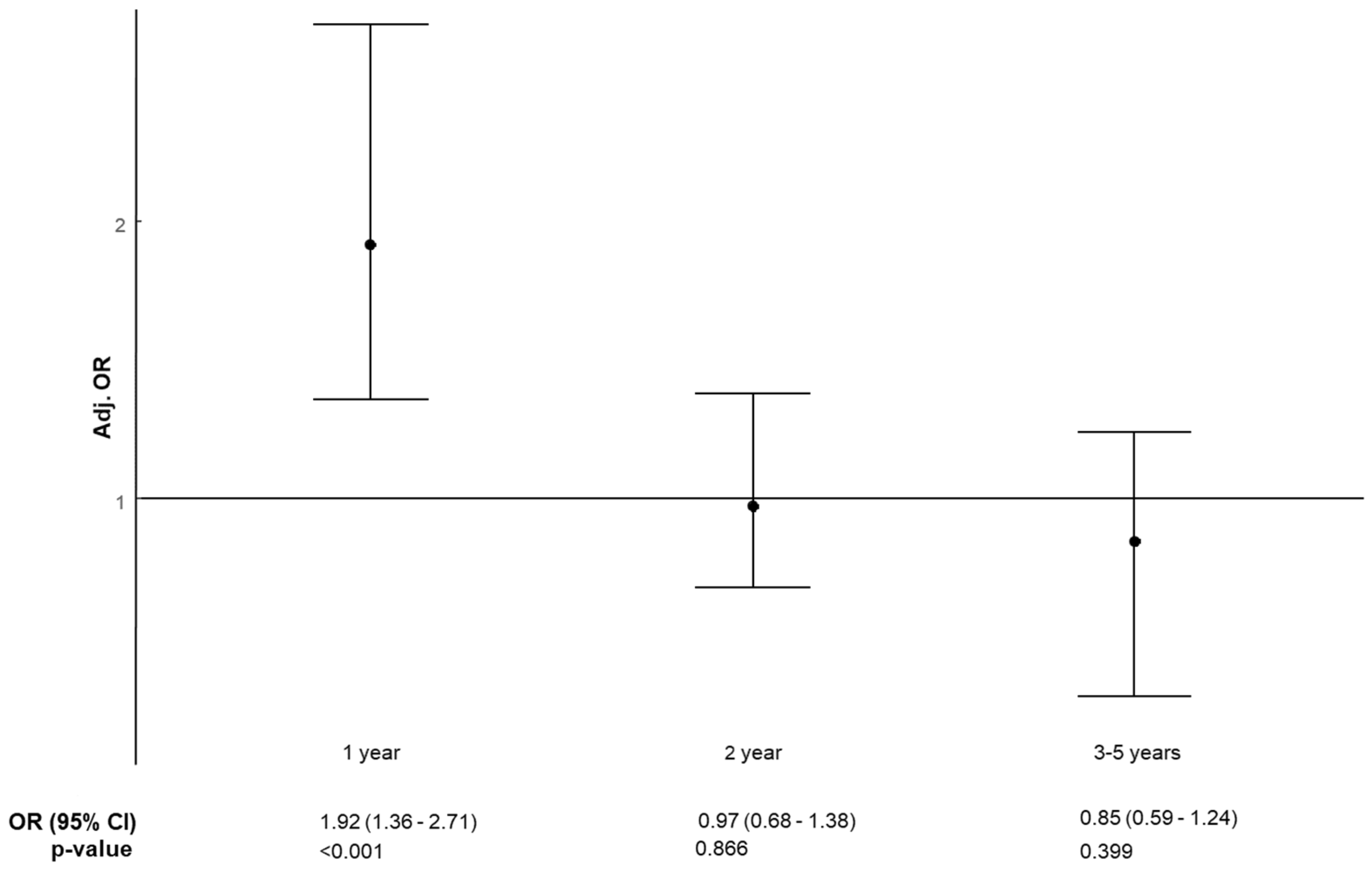
| I year | 161 (66.80) | 681 (43.85) | 1.92 (1.36–2.71) | <0.0001 |
| II year | 127 (52.70) | 626 (40.31) | 0.97 (0.68–1.38) | 0.866 |
| III—V years | 161 (66.80) | 879 (56.60) | 0.85 (0.59–1.24) | 0.399 |
| Hospitalization days, Median (IQ) | 47 (8–97) | 12 (0–46) | 1.06 d (1.03–1.08) | <0.0001 |
| Hospitalizations with surgery (%) | 177 (48.55) | 642 (41.34) | 0.89 (0.82–0.98) | 0.012 |
| Diabetes (%) | 61 (25.31) | 251 (16.16) | 1.57 (1.08–2.30) | 0.019 |
| Variables | Cases a | Controls a | Adj OR (95% CI) | p |
|---|---|---|---|---|
| Age, Median (IQ) | 79 (68–85) | 76 (61–84) | 1.11 b (1.02–1.21) | 0.012 |
| Gender, Male (%) | 106 (43.98) | 530 (34.13) | 1.49 (1.10–2.02) | 0.010 |
| Drug’s DDD taken in previous 5 years, Median (IQ) | 4334.15 (1092.92–7802.62) | 3117.01 (414.83–6392.25) | 0.95 c (0.91–0.99) | 0.009 |
| Number of antibiotics taken in previous 5 years, Median (IQ) | 3 (1–4) | 2 (0–3) | 1.15 (1.05–1.25) | 0.002 |
| At least one other J01 prescription in previous year (%) | 156 (64.73) | 640 (41.21) | 2.03 (1.45–2.85) | <0.0001 |
| 3GC prescriptions in the previous year (%) | ||||
| 0 | 212 (87.97) | 1437 (92.53) | - | - |
| 1 | 12 (4.98) | 78 (5.02) | 0.73 (0.37–1.40) | 0.345 |
| 2+ | 17 (7.05) | 38 (2.45) | 2.08 (1.07–4.08) | 0.030 |
| Hospitalization days, Median (IQ) | 47 (8–97) | 12 (0–46) | 1.06 (1.03–1.08) | <0.0001 |
| Hospitalization with surgery (%) | 177 (48.55) | 642 (41.34) | 0.89 d (0.82–0.99) | 0.010 |
| Diabetes (%) | 61 (25.31) | 251 (16.16) | 1.6 (1.09–2.34) | 0.016 |
| Potential Confounding Factor | Data Source |
|---|---|
| Age | |
| Gender | hospital discharge records database |
| Hospitalization ward | hospital discharge records database |
| Surgery | hospital discharge records database |
| Intensive care unit | |
| Internal Medicine | |
| Other | |
| Drug’s DDD taken in previous 5 years | |
| Number of active ingredients taken in previous 5 years | database of drug prescription records |
| One or more cortisone drug DDDs taken in previous 5 years | database of drug prescription records |
| Number of antibiotics taken in previous 5 years | database of drug prescription records |
| One or more J01 prescription taken in previous 5,4,3 years | |
| One or more J01 prescription taken in previous 2 years | database of drug prescription records |
| Hospitalization days | database of drug prescription records |
| Hospitalizations with surgery | |
| Hospitalizations with device implantation | database of drug prescription records |
| Hospitalizations with organ transplant | hospital discharge records database |
| Diagnosis of chronic diseases | hospital discharge records database |
| Cancer | hospital discharge records database |
| Diabetes Mellitus | hospital discharge records database |
| AIDS | hospital discharge records database |
| COPD | |
| Immunosuppression | |
| Hemodialysis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulgenzio, C.; Massari, M.; Traversa, G.; Da Cas, R.; Ferrante, G.; Aschbacher, R.; Moser, V.; Pagani, E.; Vestri, A.R.; Massidda, O.; et al. Impact of Prior Antibiotic Use in Primary Care on Escherichia coli Resistance to Third Generation Cephalosporins: A Case-Control Study. Antibiotics 2021, 10, 451. https://doi.org/10.3390/antibiotics10040451
Fulgenzio C, Massari M, Traversa G, Da Cas R, Ferrante G, Aschbacher R, Moser V, Pagani E, Vestri AR, Massidda O, et al. Impact of Prior Antibiotic Use in Primary Care on Escherichia coli Resistance to Third Generation Cephalosporins: A Case-Control Study. Antibiotics. 2021; 10(4):451. https://doi.org/10.3390/antibiotics10040451
Chicago/Turabian StyleFulgenzio, Chiara, Marco Massari, Giuseppe Traversa, Roberto Da Cas, Gianluigi Ferrante, Richard Aschbacher, Verena Moser, Elisabetta Pagani, Anna Rita Vestri, Orietta Massidda, and et al. 2021. "Impact of Prior Antibiotic Use in Primary Care on Escherichia coli Resistance to Third Generation Cephalosporins: A Case-Control Study" Antibiotics 10, no. 4: 451. https://doi.org/10.3390/antibiotics10040451
APA StyleFulgenzio, C., Massari, M., Traversa, G., Da Cas, R., Ferrante, G., Aschbacher, R., Moser, V., Pagani, E., Vestri, A. R., Massidda, O., & Kurotschka, P. K. (2021). Impact of Prior Antibiotic Use in Primary Care on Escherichia coli Resistance to Third Generation Cephalosporins: A Case-Control Study. Antibiotics, 10(4), 451. https://doi.org/10.3390/antibiotics10040451