
Surveillance of Antibacterial Usage during the COVID-19 Pandemic in England, 2020

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
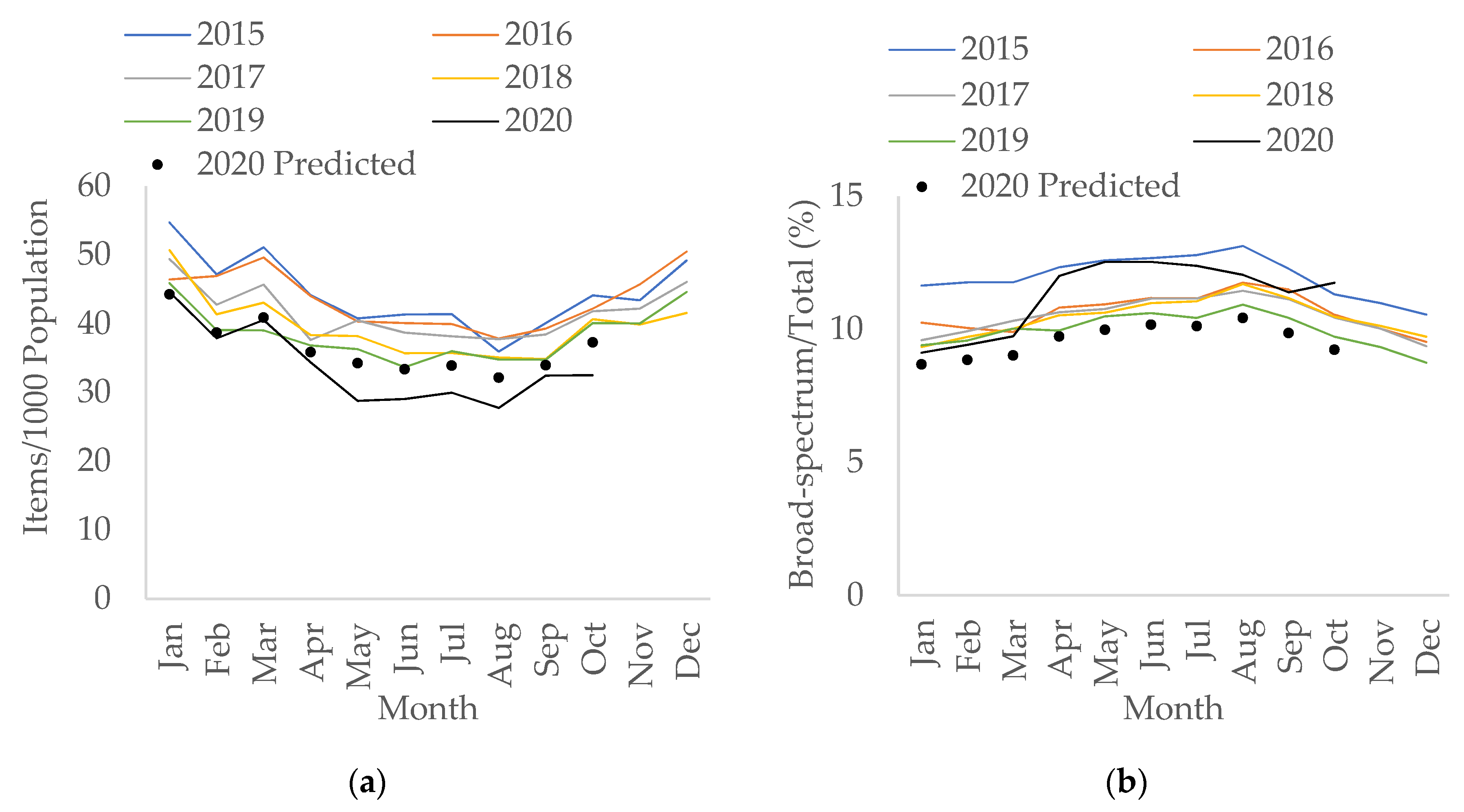
2.1. Primary Care
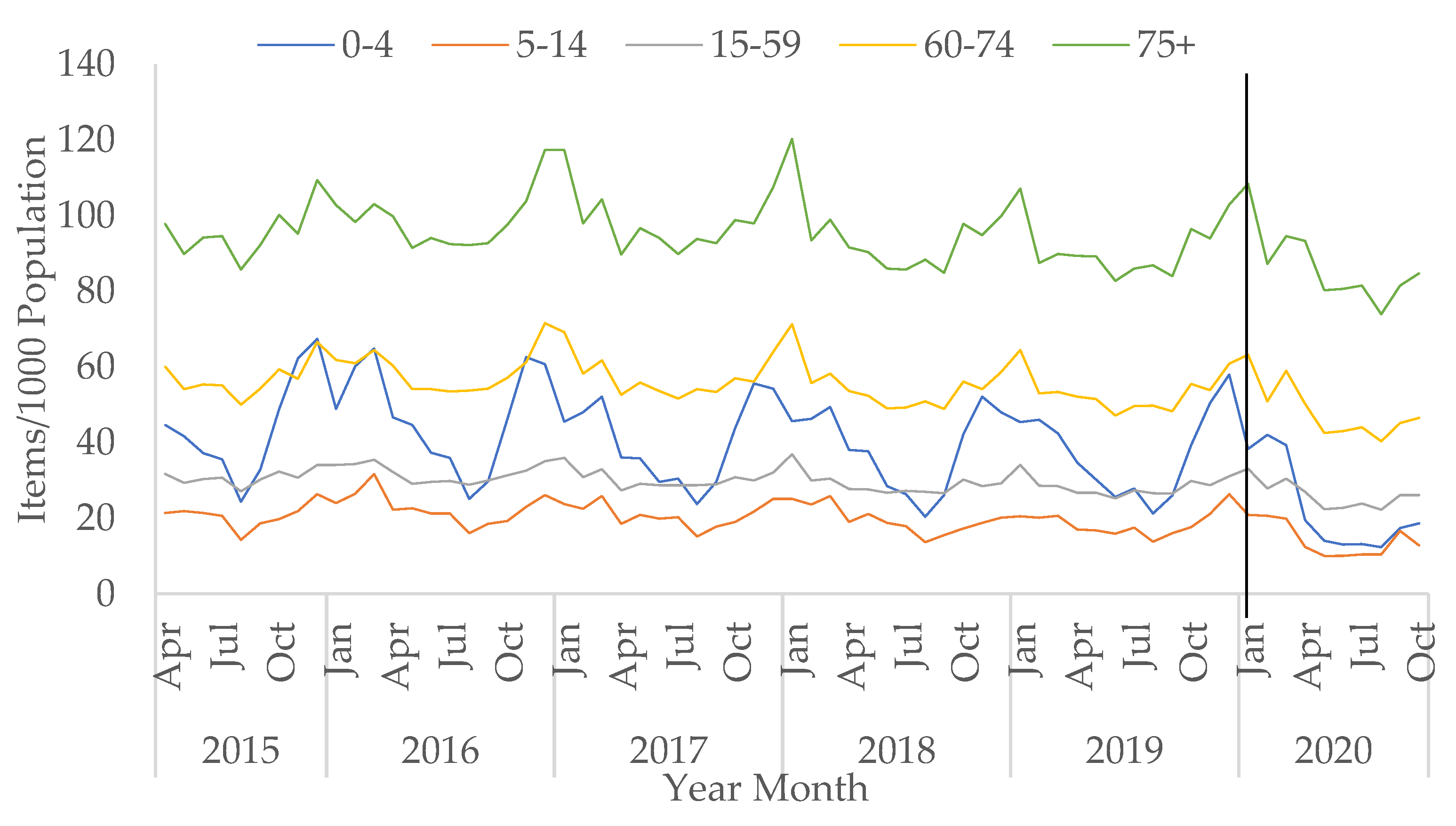
2.2. Primary Care by Age Group
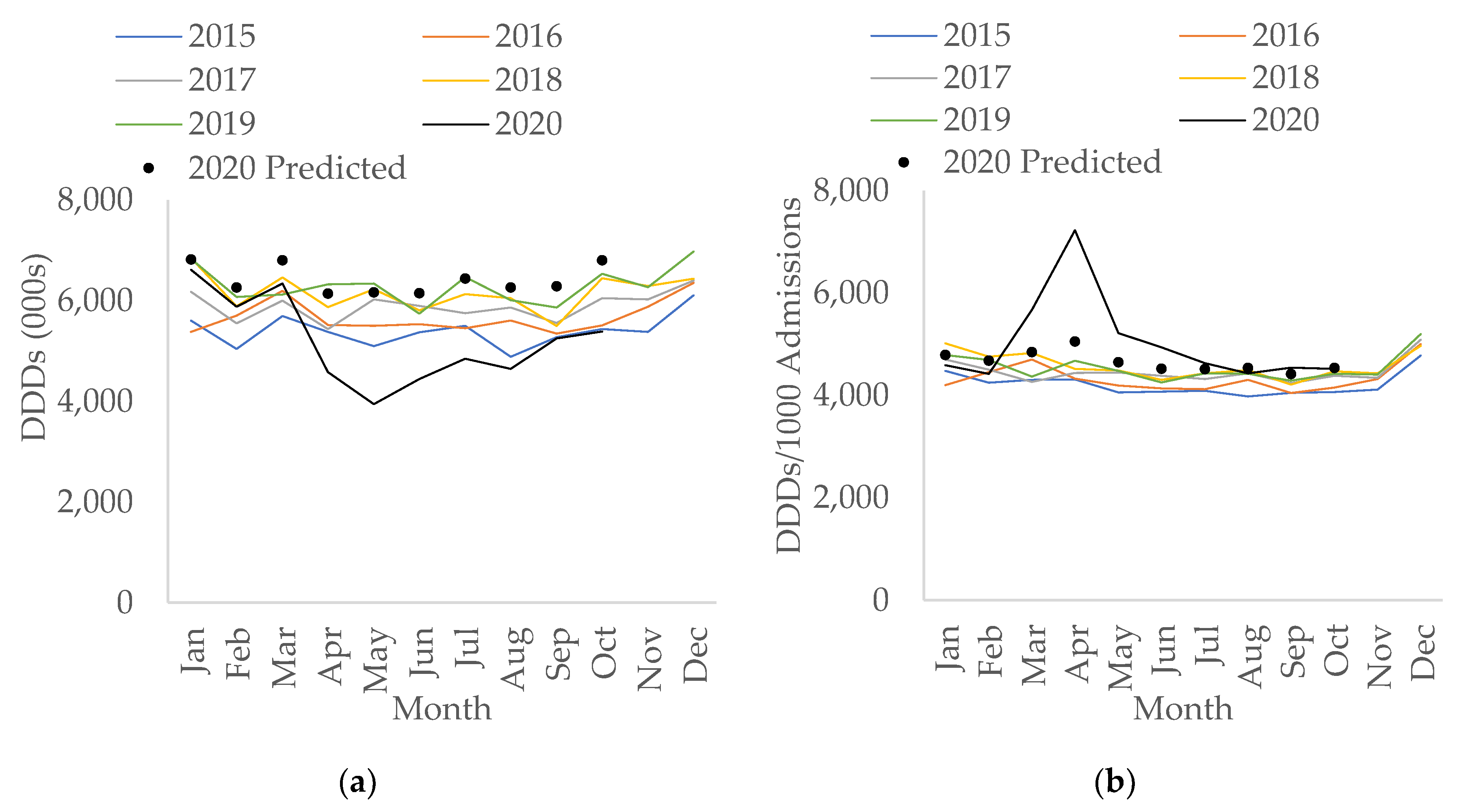
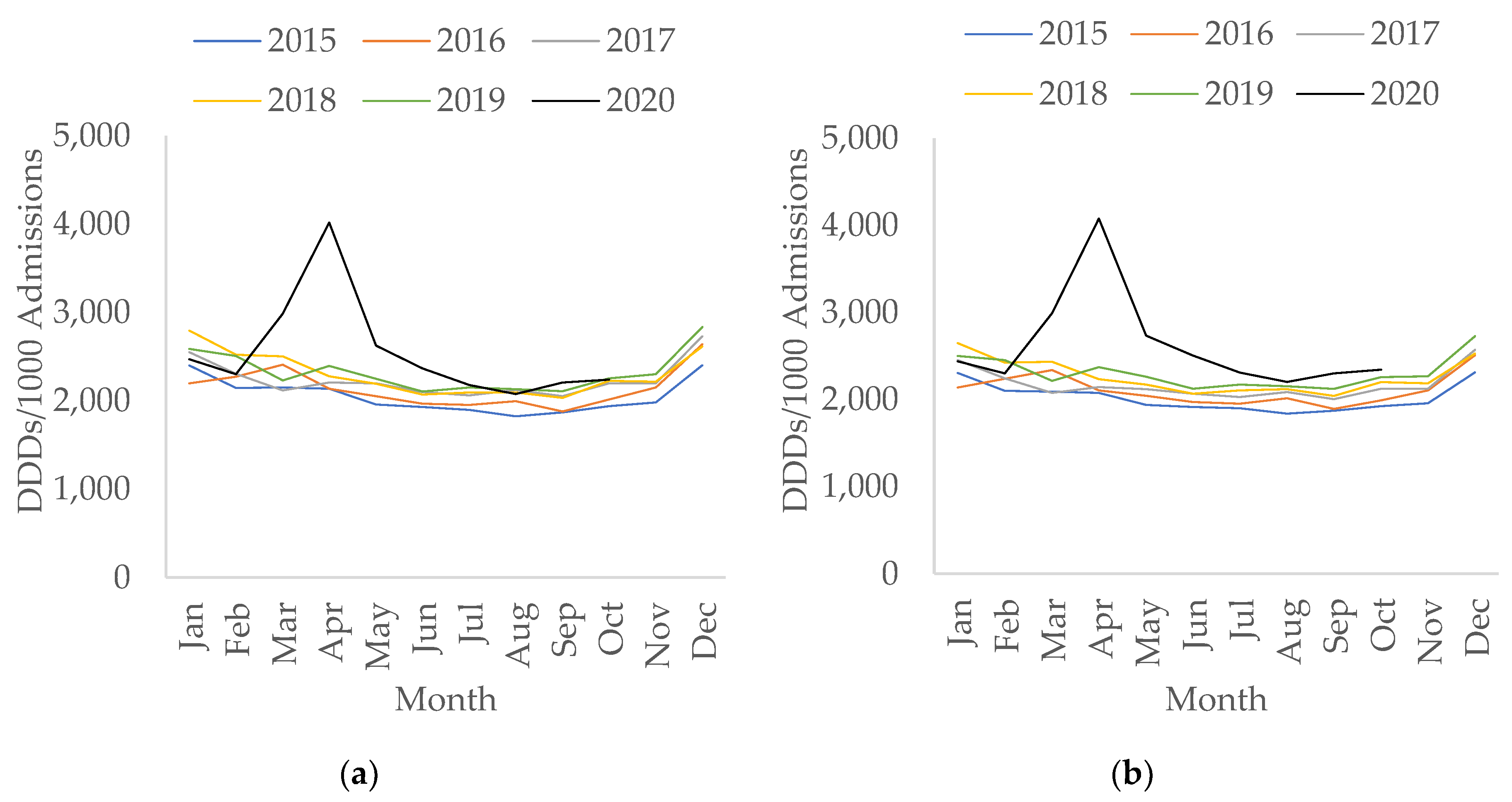
2.3. Secondary Care
3. Discussion
4. Materials and Methods
4.1. Data Sources
4.2. Descriptive and Statistical Analysis
4.3. Antibacterials Selection
- Total antibacterial use in both primary and secondary care settings;
- ‘Broad-spectrum antibacterials’, which included amoxicillin/clavulanic acid (co-amoxiclav), cephalosporins, and fluoroquinolones for primary care;
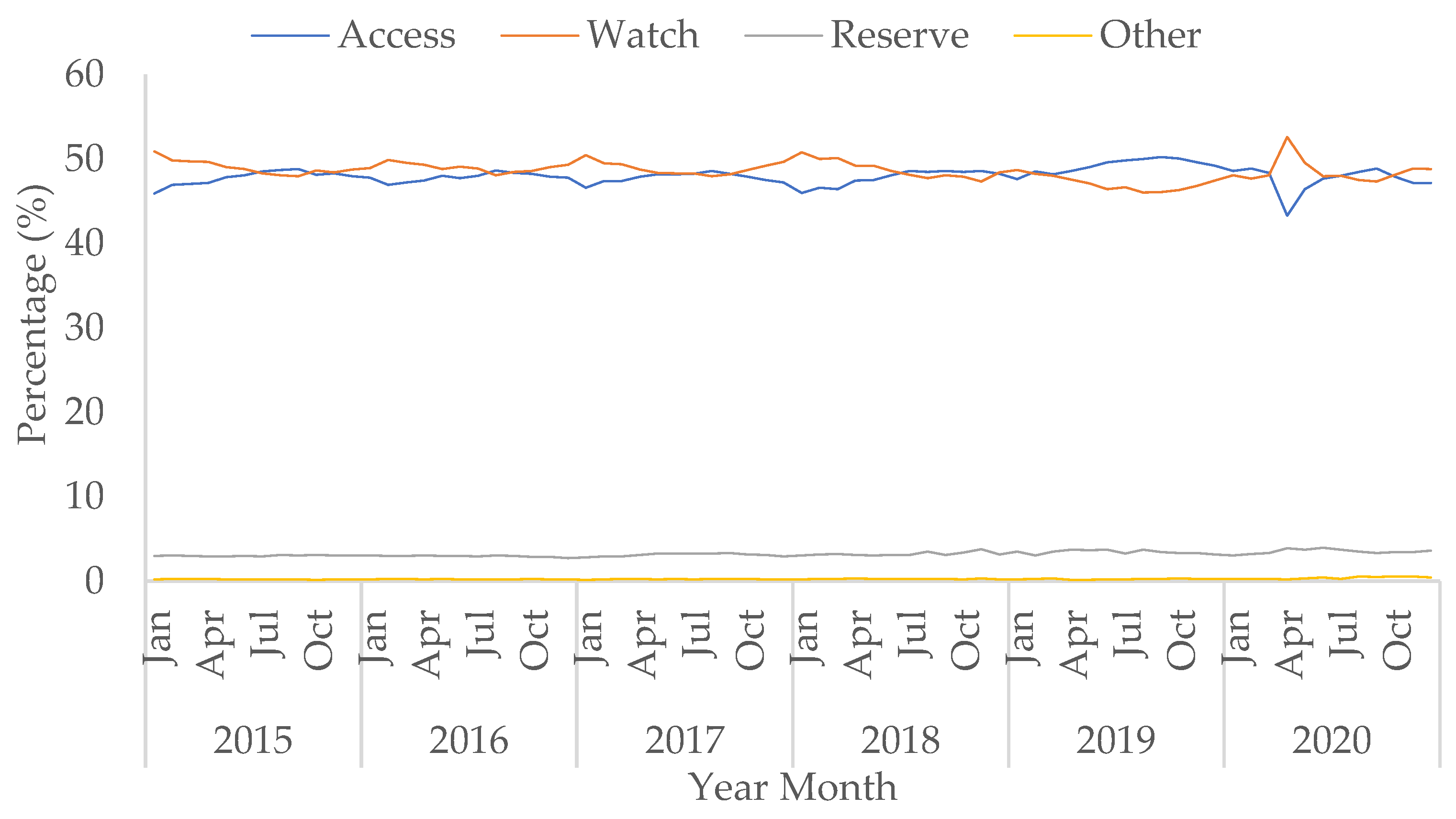
- AWaRe categories from the WHO Essential Medicine List adopted in England for hospital settings: antibacterials to improve access to (Access, predominantly narrow-spectrum), to monitor (Watch, predominantly broad-spectrum), and for ‘last resort’ or new antibacterials (Reserve) [51];
- Antibacterials for treatment of pneumonia; community-acquired pneumonia (CAP) and hospital-associated pneumonia (HAP) now for children and young people only [31,52], and secondary pneumonia with COVID-19 infection for adults [7,19], were defined using the NICE guidelines and the UK Advisory Committee on Antimicrobial Prescribing and Resistance and Healthcare Associated Infection survey (personal communication);
- Antibacterials for treatment of respiratory tract infections (besides tuberculosis) including treatments for ventilator-associated Gram-negative infections;
- Specific groups of antibacterials were also investigated; second- and third-generation cephalosporins for treatment of secondary bacterial infections and macrolide antibacterials undergoing clinical trials in hospitals; azithromycin for hospital inpatients in RECOVERY [53], and macrolides for ICU patients in REMAP-CAP [54].
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 9 February 2021).
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef]
- Public Health England. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2019–2020. Available online: https://www.gov.uk/government/publications/english-surveillance-programme-antimicrobial-utilisation-and-resistance-espaur-report (accessed on 9 February 2021).
- Public Health England. Keep Antibiotics Working. Available online: https://antibioticguardian.com/keep-antibiotics-working/ (accessed on 9 February 2021).
- NHS England. NHS Standard Contract. Available online: https://www.england.nhs.uk/nhs-standard-contract/ (accessed on 9 February 2021).
- NHS England. Commissioning for Quality and Innovation. Available online: https://www.england.nhs.uk/nhs-standard-contract/cquin/ (accessed on 9 February 2021).
- National Institute for Health and Care Excellence. COVID Rapid Guideline: Antibiotics for Pneumonia in Adults in Hospital. Available online: https://www.nice.org.uk/guidance/ng173 (accessed on 22 October 2020).
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.; Dugas, A. The frequency of influenza and bacterial coin-fection: A systematic review and meta-analysis. Influ. Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.; Togawa, Y.; Shindo, N. Bacterial and viral infections associated with influenza. Influ. Other Respir. Viruses 2013, 7, 105–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gerver, S.M.; Guy, R.; Wilson, K.; Thelwall, S.; Nsonwu, O.; Rooney, G.; Brown, C.S.; Muller-Pebody, B.; Russell, H.; Hall, V. National surveillance of bacterial and fungal co- and secondary infection in COVID-19 patients in England – Lessons from the first wave. Clin. Microbiol. Infect. 2021. [Google Scholar] [CrossRef]
- Baillie, J.K.; Beane, A.; Blumberg, L.; Bozza, F.; Fowler, R.A.; Garcia Barrio, N.; Hashmi, M.; Jassat, W.; Laouenan, C.; Mentre, F.; et al. ISARIC Clinical Data Report 8 April 2021. medRxiv 2021, 17.20155218. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.-P.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.a.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Yang, B.; Li, Q.; Wen, L.; Zhang, R. Clinical Features of 69 Cases With Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Malcolm, W.; Seaton, R.A.; Haddock, G.; Baxter, L.; Thirlwell, S.; Russell, P.; Cooper, L.; Thomson, A.; Sneddon, J. Impact of the COVID-19 pandemic on community antibiotic prescribing in Scotland. JAC Antimicrob. Resist. 2020, 2, dlaa105. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19. Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 9 November 2020).
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing Suspected or Confirmed Pneumonia in Adults in the Community. Available online: https://www.nice.org.uk/guidance/ng165/chapter/4-Managing-suspected-or-confirmed-pneumonia (accessed on 22 October 2020).
- Ashiru-Oredope, D.; Kerr, F.; Hughes, S.; Urch, J.; Lanzman, M.; Yau, T.; Cockburn, A.; Patel, R.; Sheikh, A.; Gormley, C.; et al. Assessing the Impact of COVID-19 on Antimicrobial Stewardship Activities/Programs in the United Kingdom. Antibiotics 2021, 10, 110. [Google Scholar] [CrossRef]
- Huttner, B.D.; Catho, G.; Pano-Pardo, J.R.; Pulcini, C.; Schouten, J. COVID-19: Don’t neglect antimicrobial stewardship principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Clostridium Difficile Infection: Risk with Broad-Spectrum Antibiotics. Available online: https://www.nice.org.uk/advice/esmpb1/chapter/key-points-from-the-evidence (accessed on 9 February 2021).
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef]
- Mamun, A.A.; Saatchi, A.; Xie, M.; Lishman, H.; Blondel-Hill, E.; Marra, F.; Patrick, D.M. Community Antibiotic Use at the Population Level During the SARS-CoV-2 Pandemic in British Columbia, Canada. Open Forum Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Cabinet Office. Guidance: Staying at Home and Away From Others (Social Distancing). Available online: https://www.gov.uk/government/publications/full-guidance-on-staying-at-home-and-away-from-others/full-guidance-on-staying-at-home-and-away-from-others (accessed on 9 November 2020).
- NHS England. Quality Premium. Available online: https://www.england.nhs.uk/ccg-out-tool/qual-prem/ (accessed on 9 November 2020).
- Balinskaite, V.; Johnson, A.P.; Holmes, A.; Aylin, P. The impact of a national antimicrobial stewardship programme on antibiotic prescribing in primary care: An interrupted time series analysis. Clin. Infect. Dis. 2018, 69, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Royal College of General Practitioners Research and Surveillance Centre. Public Health Data. Available online: https://www.rcgp.org.uk/clinical-and-research/our-programmes/research-and-surveillance-centre/public-health-data.aspx (accessed on 17 May 2021).
- Zhu, N.; Aylin, P.; Rawson, T.; Gilchrist, M.; Majeed, A.; Holmes, A. Investigating the impact of COVID-19 on primary care antibiotic prescribing in North West London across two epidemic waves. Clin. Microbiol. Infect. 2021, 27, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. MRSA, MSSA, Gram-Negative Bacteraemia and CDI: Quarterly Report. Available online: https://www.gov.uk/government/statistics/mrsa-mssa-and-e-coli-bacteraemia-and-c-difficile-infection-quarterly-epidemiological-commentary (accessed on 9 February 2021).
- National Institute for Health and Care Excellence. Pneumonia (Community-Acquired): Antimicrobial Prescribing. Available online: https://www.nice.org.uk/guidance/ng138/chapter/Recommendations#choice-of-antibiotic (accessed on 22 October 2020).
- NHS Digital. Appointments in General Practice. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/appointments-in-general-practice (accessed on 9 February 2021).
- Dolk, F.C.K.; Pouwels, K.B.; Smith, D.R.M.; Robotham, J.V.; Smieszek, T. Antibiotics in primary care in England: Which antibiotics are prescribed and for which conditions? J. Antimicrob. Chemother. 2018, 73, ii2–ii10. [Google Scholar] [CrossRef]
- Rezel-Potts, E.; L’Esperance, V.; Gulliford, M.C. Antimicrobial stewardship in the UK during the COVID-19 pandemic: A population-based cohort study and interrupted time-series analysis. Br. J. Gen. Pract. 2021, 71, e331–e338. [Google Scholar] [CrossRef]
- Zhu, N.J.; McLeod, M.; McNulty, C.A.M.; Lecky, D.M.; Holmes, A.H.; Ahmad, R. Trends in Antibiotic Prescribing in Out-of-Hours Primary Care in England from January 2016 to June 2020 to Understand Behaviours during the First Wave of COVID-19. Antibiotics 2021, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Iacobucci, G. Covid-19: All non-urgent elective surgery is suspended for at least three months in England. BMJ 2020, 368, m1106. [Google Scholar] [CrossRef] [Green Version]
- McCabe, R.; Schmit, N.; Christen, P.; D’Aeth, J.C.; Løchen, A.; Rizmie, D.; Nayagam, S.; Miraldo, M.; Aylin, P.; Bottle, A.; et al. Adapting hospital capacity to meet changing demands during the COVID-19 pandemic. BMC Med. 2020, 18, 329. [Google Scholar] [CrossRef] [PubMed]
- Beović, B.; Doušak, M.; Ferreira-Coimbra, J.; Nadrah, K.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Ayoade, F.; Rello, J.; Erdem, H. Antibiotic use in patients with COVID-19: A ‘snapshot’ Infectious Diseases International Research Initiative (ID-IRI) survey. J. Antimicrob. Chemother. 2020, 75, 3386–3390. [Google Scholar] [CrossRef] [PubMed]
- University of Oxford. Azithromycin and Doxycycline Are Not Generally Effective Against COVID-19 in Patients Treated at Home, Shows PRINCIPLE Trial. Available online: https://www.principletrial.org/news/azithromycin-and-doxycycline-are-not-generally-effective-treatments-for-covid-19-shows-principle-trial (accessed on 25 January 2021).
- Furtado, R.H.M.; Berwanger, O.; Fonseca, H.A.; Corrêa, T.D.; Ferraz, L.R.; Lapa, M.G.; Zampieri, F.G.; Veiga, V.C.; Azevedo, L.C.P.; Rosa, R.G.; et al. Azithromycin in addition to standard of care versus standard of care alone in the treatment of patients admitted to the hospital with severe COVID-19 in Brazil (COALITION II): A randomised clinical trial. Lancet 2020, 396, 959–967. [Google Scholar] [CrossRef]
- Abaleke, E.; Abbas, M.; Abbasi, S.; Abbott, A.; Abdelaziz, A.; Abdelbadiee, S.; Abdelfattah, M.; Abdul, B.; Abdul Rasheed, A.; Abdul-Kadir, R.; et al. Azithromycin in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021. [Google Scholar] [CrossRef]
- Public Health England. Weekly National Influenza and COVID-19 Surveillance Report: Week 51 Report (Up to Week 50 Data) 17 December 2020. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/945502/Weekly_Flu_and_COVID-19_report_w51_FINAL.pdf (accessed on 21 April 2021).
- National Institute for Health Research. NIHR COVID Recovery and Learning Research Committee Public Minutes August 2020 Meeting. Available online: https://www.nihr.ac.uk/documents/nihr-covid-recovery-and-learning-research-committee-public-minutes-august-2020-meeting/25665 (accessed on 4 December 2020).
- NHS Business Service Authority. ePACT2. Available online: https://www.nhsbsa.nhs.uk/epact2 (accessed on 9 February 2021).
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2019. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 21 April 2020).
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Corrigendum to: Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2020, 49, 1414. [Google Scholar] [CrossRef] [PubMed]
- Christou, V.; Fokianos, K. Quasi-Likelihood Inference for Negative Binomial Time Series Models. J. Time Ser. Anal. 2014, 35, 55–78. [Google Scholar] [CrossRef]
- UCLA: Statistical Consulting Group. Negative Binomial Regression, Stata Annotated Output. Available online: https://stats.idre.ucla.edu/stata/output/negative-binomial-regression/ (accessed on 7 June 2021).
- StataCorp LLC. Stata Statistical Software: Release 15; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Public Health England. Public Health Profiles-AMR Local Indicators. Available online: https://fingertips.phe.org.uk/profile/amr-local-indicators (accessed on 21 April 2020).
- Budd, E.; Cramp, E.; Sharland, M.; Hand, K.; Howard, P.; Wilson, P.; Wilcox, M.; Muller-Pebody, B.; Hopkins, S. Adaptation of the WHO Essential Medicines List for national antibiotic stewardship policy in England: Being AWaRe. J. Antimicrob. Chemother. 2019, 74, 3384–3389. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Pneumonia (Hospital-Acquired): Antimicrobial Prescribing. Available online: https://www.nice.org.uk/guidance/ng139/chapter/Recommendations (accessed on 22 October 2020).
- University of Oxford. Randomised Evaluation of COVID-19 Therapy (RECOVERY) Protocol. Available online: https://www.recoverytrial.net/files/recovery-protocol-v9-1-2020-09-18.pdf (accessed on 9 November 2020).
- REMAP-CAP. REMAP-CAP Response to the COVID-19 Pandemic. Available online: https://www.remapcap.org/coronavirus (accessed on 21 April 2020).





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrews, A.; Budd, E.L.; Hendrick, A.; Ashiru-Oredope, D.; Beech, E.; Hopkins, S.; Gerver, S.; Muller-Pebody, B.; the AMU COVID-19 Stakeholder Group. Surveillance of Antibacterial Usage during the COVID-19 Pandemic in England, 2020. Antibiotics 2021, 10, 841. https://doi.org/10.3390/antibiotics10070841
Andrews A, Budd EL, Hendrick A, Ashiru-Oredope D, Beech E, Hopkins S, Gerver S, Muller-Pebody B, the AMU COVID-19 Stakeholder Group. Surveillance of Antibacterial Usage during the COVID-19 Pandemic in England, 2020. Antibiotics. 2021; 10(7):841. https://doi.org/10.3390/antibiotics10070841
Chicago/Turabian StyleAndrews, Amelia, Emma L. Budd, Aoife Hendrick, Diane Ashiru-Oredope, Elizabeth Beech, Susan Hopkins, Sarah Gerver, Berit Muller-Pebody, and the AMU COVID-19 Stakeholder Group. 2021. "Surveillance of Antibacterial Usage during the COVID-19 Pandemic in England, 2020" Antibiotics 10, no. 7: 841. https://doi.org/10.3390/antibiotics10070841
APA StyleAndrews, A., Budd, E. L., Hendrick, A., Ashiru-Oredope, D., Beech, E., Hopkins, S., Gerver, S., Muller-Pebody, B., & the AMU COVID-19 Stakeholder Group. (2021). Surveillance of Antibacterial Usage during the COVID-19 Pandemic in England, 2020. Antibiotics, 10(7), 841. https://doi.org/10.3390/antibiotics10070841