
Antimicrobial Use in COVID-19 Patients in the First Phase of the SARS-CoV-2 Pandemic: A Scoping Review

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Study Selection
2.2. Description of Included Studies
2.3. Antibiotic Prescribing and Illness Severity
2.4. Antibiotic Prescribing and Health Outcomes
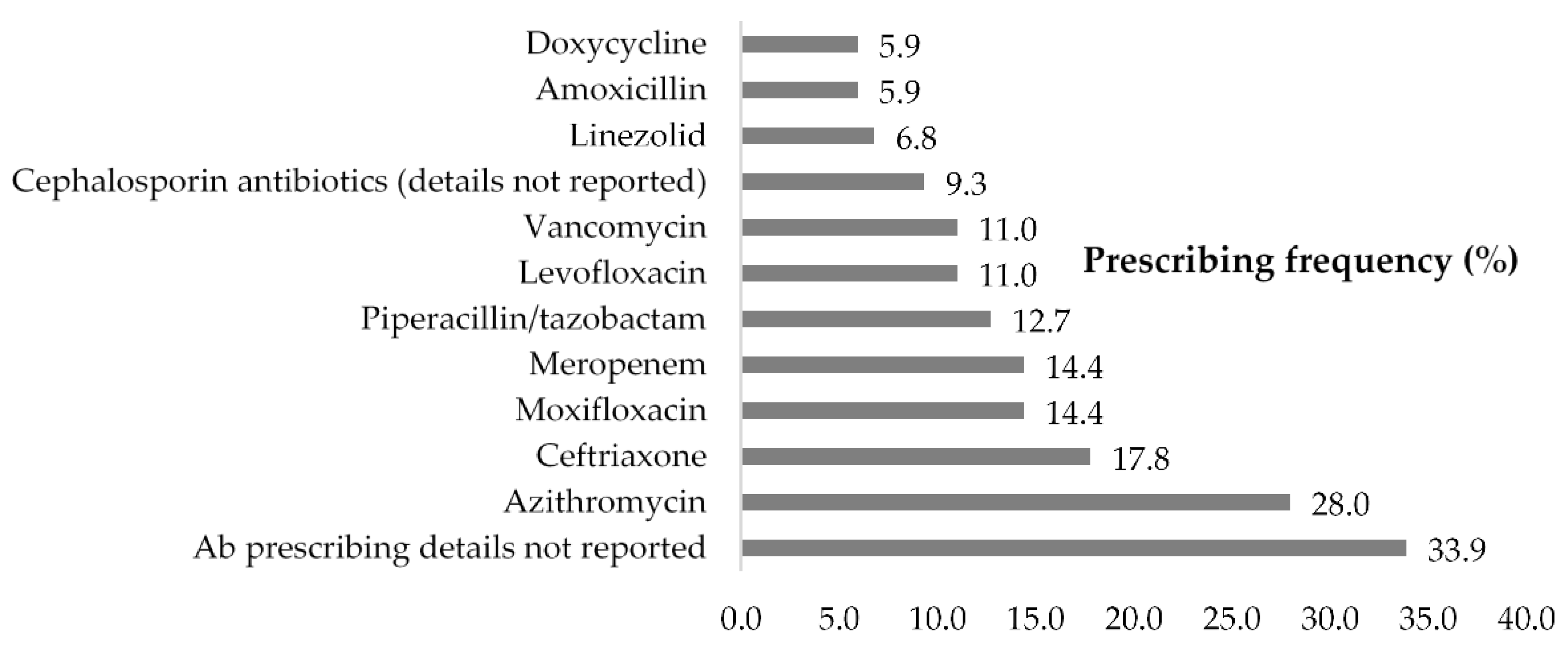
2.5. Frequently Prescribed Antibiotics
2.6. Antibiotic Prescribing Scenarios
2.7. Severity of Illness, Antibiotic Prescribing Justifications, and Health Outcomes
2.8. Secondary Infections and Health Outcomes
2.9. Gender and Health Outcomes
2.10. Study Design and Country Economic Status
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.1.1. Web of Science
4.1.2. PubMed
4.1.3. Embase
4.1.4. CNKI and VIP
4.2. Inclusion, Exclusion Criteria, and Study Selection Process
4.2.1. Inclusion criteria
- All types of clinical studies (randomized control trial (RCT), cohort, case report including case series, other observational studies (except cohort)) about the use of antibiotics to treat patients with COVID-19.
- Studies reporting patients diagnosed with COVID-19 and receiving antibiotic treatment, without restrictions on age, race, gender, geographical location.
- Studies which had mentioned antibiotic treatment and also reporting treatment outcomes.
- Studies reporting COVID-19 patients with bacterial co-infections.
4.2.2. Exclusion Criteria
- Animal studies, in vitro experiments, in silico screening/drug modeling, molecular mechanism, and other aspects of COVID-19 research where not related to or mentioned antibiotic use (ABU).
- Conference abstracts.
- Commentaries and editorial letters not reporting ABU.
- Literature review not reporting ABU.
- Trial protocol.
- Case report and case series not reporting ABU.
- Full-text articles not available in English or Chinese.
- Studies reporting suspected or asymptomatic COVID-19 patients.
- Studies reporting COVID- 19 patients in primary care settings such as GP and community health center.
4.3. Data Extraction
4.4. Data Synthesis and Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. No Time to Wait: Securing the Future from Drug-Resistant Infections. Report to the Secretary-General of the United Nations (IACG). Available online: https://www.who.int/publications/i/item/no-time-to-wait-securing-the-future-from-drug-resistant-infections (accessed on 4 December 2020).
- O’Neill, J.; Bretagne, B. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations; Wellcome Trust: London, UK, 2014. [Google Scholar]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Coinfections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal co-infection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar]
- Vaughn, V.M.; Gandhi, T.; Petty, L.A.; Patel, P.K.; Prescott, H.C.; Malani, A.N.; Ratz, D.; McLaughlin, E.; Chopra, V.; Flanders, S.A. Empiric Antibacterial Therapy and Community-onset Bacterial Coinfection in Patients Hospitalized with COVID-19: A Multi-Hospital Cohort Study. Clin. Infect. Dis. 2021, 72, e533–e541. [Google Scholar] [CrossRef]
- Beović, B.; Doušak, M.; Ferreira-Coimbra, J.; Nadrah, K.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Ayoade, F.; Rello, J.; Erdem, H. Antibiotic use in patients with COVID-19: A ‘snapshot’ Infectious Diseases International Research Initiative (ID-IRI) survey. J. Antimicrob. Chemother. 2020, 75, 3386–3390. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Huttner, B.D.; Catho, G.; Pano-Pardo, J.R.; Pulcini, C.; Schouten, J. COVID-19: Don’t neglect antimicrobial stewardship principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of coinfections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442–442A. [Google Scholar] [CrossRef]
- Hsu, J. How covid-19 is accelerating the threat of antimicrobial resistance. BMJ 2020, 369, m1983. [Google Scholar] [CrossRef]
- Murray, A.K. The Novel Coronavirus COVID-19 Outbreak: Global Implications for Antimicrobial Resistance. Front. Microbiol. 2020, 11, 1020. [Google Scholar] [CrossRef]
- Hu, X.-Y.; Logue, M.; Robinson, N. Antimicrobial resistance is a global problem—A UK perspective. Eur. J. Integr. Med. 2020, 36, 101136. [Google Scholar] [CrossRef]
- Antimicrobial resistance in the age of COVID-19. Nat. Microbiol. 2020, 5, 779. [CrossRef]
- Martin, E.; Philbin, M.; Hughes, G.; Bergin, C.; Talento, A.F. Antimicrobial stewardship challenges and innovative initiatives in the acute hospital setting during the COVID-19 pandemic. J. Antimicrob. Chemother. 2021, 76, 272–275. [Google Scholar] [CrossRef]
- Sieswerda, E.; De Boer, M.G.; Bonten, M.M.; Boersma, W.G.; Jonkers, R.E.; Aleva, R.M.; Kullberg, B.J.; Schouten, J.A.; van de Garde, E.M.; Verheij, T.J.; et al. Recommendations for antibacterial therapy in adults with COVID-19—An evidence based guideline. Clin. Microbiol. Infect. 2020, 27, 61–66. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19 Interim Guidance; World Health Organization: Geneva, Switzerland, May 2020; Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 4 December 2020).
- National Institute for Health and Care Excellence. COVID-19 Rapid Guideline: Managing COVID-19: March 2021. Available online: https://www.nice.org.uk/guidance/ng191 (accessed on 21 May 2021).
- Group SAP. SAPG Response to COVID-19. Available online: https://www.sapg.scot/about-us/latest-updates/sapg-response-to-covid-19/ (accessed on 4 December 2020).
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Scully, E.P.; Haverfield, J.; Ursin, R.L.; Tannenbaum, C.; Klein, S.L. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Antibiotic Use at Veterans Affairs’ Hospitals Increases During COVID-19 Pandemic, Reversing A Four-Year Downward Trend. Available online: https://www.idsociety.org/news--publications-new/articles/2020/antibiotic-use-at-veterans-affairs-hospitals-increases-during-covid-19-pandemic-reversing-a-four-year-downward-trend/ (accessed on 4 December 2020).
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R.; Higgs, E.; Randolph, A.; Smoot, B.E.; Thompson, B.T. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States*. Crit. Care Med. 2012, 40, 1487–1498. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.S.; Greenberg, J.A.; McNulty, M.C.; Gregg, K.S.; Riddell, J.; Mangino, J.E.; Weber, D.M.; Hebert, C.L.; Marzec, N.S.; Barron, M.A.; et al. Bacterial and viral co-infections complicating severe influenza: Incidence and impact among 507 U.S. patients, 2013–14. J. Clin. Virol. 2016, 80, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Critically Important Antimicrobials for Human Medicine. Available online: https://apps.who.int/iris/bitstream/handle/10665/312266/9789241515528-eng.pdf?ua=1 (accessed on 4 December 2020).
- Miranda, C.; Silva, V.; Capita, R.; Alonso-Calleja, C.; Igrejas, G.; Poeta, P. Implications of antibiotics use during the COVID-19 pandemic: Present and future. J. Antimicrob. Chemother. 2020, 75, 3413–3416. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.-A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- O’Brien, K.S.; Emerson, P.; Hooper, P.; Reingold, A.L.; Dennis, E.G.; Keenan, J.D.; Lietman, T.M.; Oldenburg, C.E. Antimicrobial resistance following mass azithromycin distribution for trachoma: A systematic review. Lancet Infect. Dis. 2019, 19, e14–e25. [Google Scholar] [CrossRef]
- Muller, A.; Lopez-Lozano, J.M.; Bertrand, X.; Talon, D. Relationship between ceftriaxone use and resistance to third-generation cephalosporins among clinical strains of Enterobacter cloacae. J. Antimicrob. Chemother. 2004, 54, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Pereira, L.M.P.; Phillips, M.; Ramlal, H.; Teemul, K.; Prabhakar, P. Third generation cephalosporin use in a tertiary hospital in Port of Spain, Trinidad: Need for an antibiotic policy. BMC Infect. Dis. 2004, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, K.L.; Cohen, S.H.; Inciardi, J.F.; King, J.H.; Lippert, W.E.; Iglesias, T.; VanCouwenberghe, C.J. The relationship between antecedent antibiotic use and resistance to extend-ed-spectrum cephalosporins in group I beta-lactamase-producing organisms. Clin. Infect. Dis. 1995, 21, 1107–1113. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Wen, Y.; Wan, W.; Lei, J.; Jiang, X. Clinical characteristics and antibiotics treatment in suspected bacterial infection patients with COVID-19. Int. Immunopharmacol. 2021, 90, 107157. [Google Scholar] [CrossRef] [PubMed]
- Buetti, N.; Mazzuchelli, T.; Priore, E.L.; Balmelli, C.; Llamas, M.; Pallanza, M.; Elzi, L.; Consonni, V.; Trimboli, P.; Forni-Ogna, V.; et al. Early administered antibiotics do not impact mortality in critically ill patients with COVID-19. J. Infect. 2020, 81, e148–e149. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 4 August 2020).



{kind=link}
{kind=link}
| Illness Severity of COVID-19 Patients | Patient Size n (%) | Mean Antibiotic Prescribing (%) |
|---|---|---|
| Severe and critical patients | 2630 (41.9) | 75.4 |
| Mild and moderate | 3649 (58.1) | 75.1 |
| Total | 6279 (100.0) | 75.2 |
| SN | Category of Antibiotic Prescribing | LOS (Mean Days) | Discharge (Mean%) | Mortality (Mean%) |
|---|---|---|---|---|
| 1 | All given abs (58 studies) | 12.5 | 76.2 | 26.5 |
| 2 | Majority are given abs (37 studies) | 14.3 | 57.9 | 13.1 |
| 3 | Majority not given abs (11 studies) | 10.3 | 73.2 | 2.3 |
| Antimicrobial Prescribing Scenarios with Clinical Justifications (A) | Antimicrobial Prescribing Scenarios without Clinical Justifications (B) | Antimicrobial Prescribing Scenarios not Sure whether with or Without Clinical Justifications (C) |
|---|---|---|
| Scenario 1: Microbiological analysis such as blood, stool, urine, or sputum culture was tested positive. | Scenario 4: Respiratory failure such as acute respiratory distress syndrome (ARDS) | Scenario 9: Patients are older or frail, or have a pre-existing comorbidity such as immunosuppression (Solid organ transplant recipients who remain on long term immune suppression therapy), HIV patients, or significant heart or lung disease (for example bronchiectasis or COPD, systemic lupus erythematosus), or have a history of severe illness following previous lung infection |
| Scenario 2: Pulmonary aspergillosis | Scenario 7: C reactive protein higher (around 30 mg/L, normal range 0–8 mg/L) | Scenario 10: Elder patient with other type of cancer not listed above, diabetes, hypertension |
| Scenario 3: Septic shock or sepsis | Scenario 8: Patients received ventilation or mechanical ventilation | Scenario 12: Azithromycin was used as a combination therapy with hydroxychloroquine |
| Scenario 5: Procalcitonin >0.5 ng/mL | Scenario 11: Pregnant woman for caesarean section, or with suspected bronchitis | Scenario 14: Mentioned that “Abs were used as an empirical treatment when it was very difficult to exclude bacterial co-infection”; or “abs were used if needed and this decision was based on health care providers’ discretion” or “abs were initialled at the beginning but was discontinued after COVID-19 was confirmed or after microbiological culture analysis tested negative” or “abs were empirically used and patient developed bacterial infection later (case report) or a high percentage of patients developed bacterial co-infections later |
| Scenario 6: a high percentage of neutrophils (neutrophilia), WBC count | Scenario 13: Antimicrobial treatment was given without any justifications (Not reporting any suspected bacterial/fungal co-infection symptoms, or any lab test results indicating possible bacterial/fungal infections) | Scenario 15: Abs were used for most patients (higher prescribing rate) to cover possible bacterial co-infections; however only a minor percentage of patients developed bacterial/fungal infections |
| Scenario 18: Paediatric patient (infant, preterm neonate) with abnormal blood cell test or CRP levels; or suspected sepsis etc | Scenario 16: Abs were reported to be used as an empirical/adjuvant/concomitant/standard treatment; and patients were given abs on admission, or before randomization into different trial groups for some trials) | Scenario 17: Dual or triple antibiotics used |
| Scenario 19: Patient with acute appendicitis | ||
| Scenario 20: Patient with digestive symptoms |
| Severity of Illness (Categories) | LOS (Mean Days) | Discharge (Mean%) | Mortality (Mean%) |
|---|---|---|---|
| All severe/critical (16 studies) | 17.4 | 36.6 | 53.1 |
| Majority were severe/critical (4 studies) | 18.0 | 77.9 | 5.8 |
| Majority were mild/moderate (33 studies) | 12.0 | 60.5 | 4.8 |
| All mild/moderate (20 studies) | 8.7 | 96.2 | 0.2 |
| Antibiotic Prescribing Justified or Not | LOS (Mean Days) | Discharge (Mean%) | Mortality (Mean%) |
|---|---|---|---|
| A-with clinical justifications” (n = 14) | 9.3 | 80.9 | 9.5 |
| B-without clinical justifications (n = 49) | 12.2 | 69.3 | 13.1 |
| C-not sure (n = 47) | 14.1 | 61.1 | 24.8 |
| Descriptions | Severe/Critical n (%) | Mild/Moderate n (%) | Mean Length of Stay (Days) | Mean Discharge Rate (%) | Mean Mortality Rate (%) |
|---|---|---|---|---|---|
| Total patients with secondary infections (n = 610) | 313 (51.3%) | 297 (48.7%) | 20.4 | 54.8 | 43.7 |
| Total sample size (n = 6279) | 2630 (41.9%) | 3649 (58.1%) | 12.4 | 65.6 | 16.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cong, W.; Poudel, A.N.; Alhusein, N.; Wang, H.; Yao, G.; Lambert, H. Antimicrobial Use in COVID-19 Patients in the First Phase of the SARS-CoV-2 Pandemic: A Scoping Review. Antibiotics 2021, 10, 745. https://doi.org/10.3390/antibiotics10060745
Cong W, Poudel AN, Alhusein N, Wang H, Yao G, Lambert H. Antimicrobial Use in COVID-19 Patients in the First Phase of the SARS-CoV-2 Pandemic: A Scoping Review. Antibiotics. 2021; 10(6):745. https://doi.org/10.3390/antibiotics10060745
Chicago/Turabian StyleCong, Wenjuan, Ak Narayan Poudel, Nour Alhusein, Hexing Wang, Guiqing Yao, and Helen Lambert. 2021. "Antimicrobial Use in COVID-19 Patients in the First Phase of the SARS-CoV-2 Pandemic: A Scoping Review" Antibiotics 10, no. 6: 745. https://doi.org/10.3390/antibiotics10060745
APA StyleCong, W., Poudel, A. N., Alhusein, N., Wang, H., Yao, G., & Lambert, H. (2021). Antimicrobial Use in COVID-19 Patients in the First Phase of the SARS-CoV-2 Pandemic: A Scoping Review. Antibiotics, 10(6), 745. https://doi.org/10.3390/antibiotics10060745