
The Impact of the COVID-19 Pandemic on Antibiotic Prescribing Trends in Outpatient Care: A Nationwide, Quasi-Experimental Approach

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Results
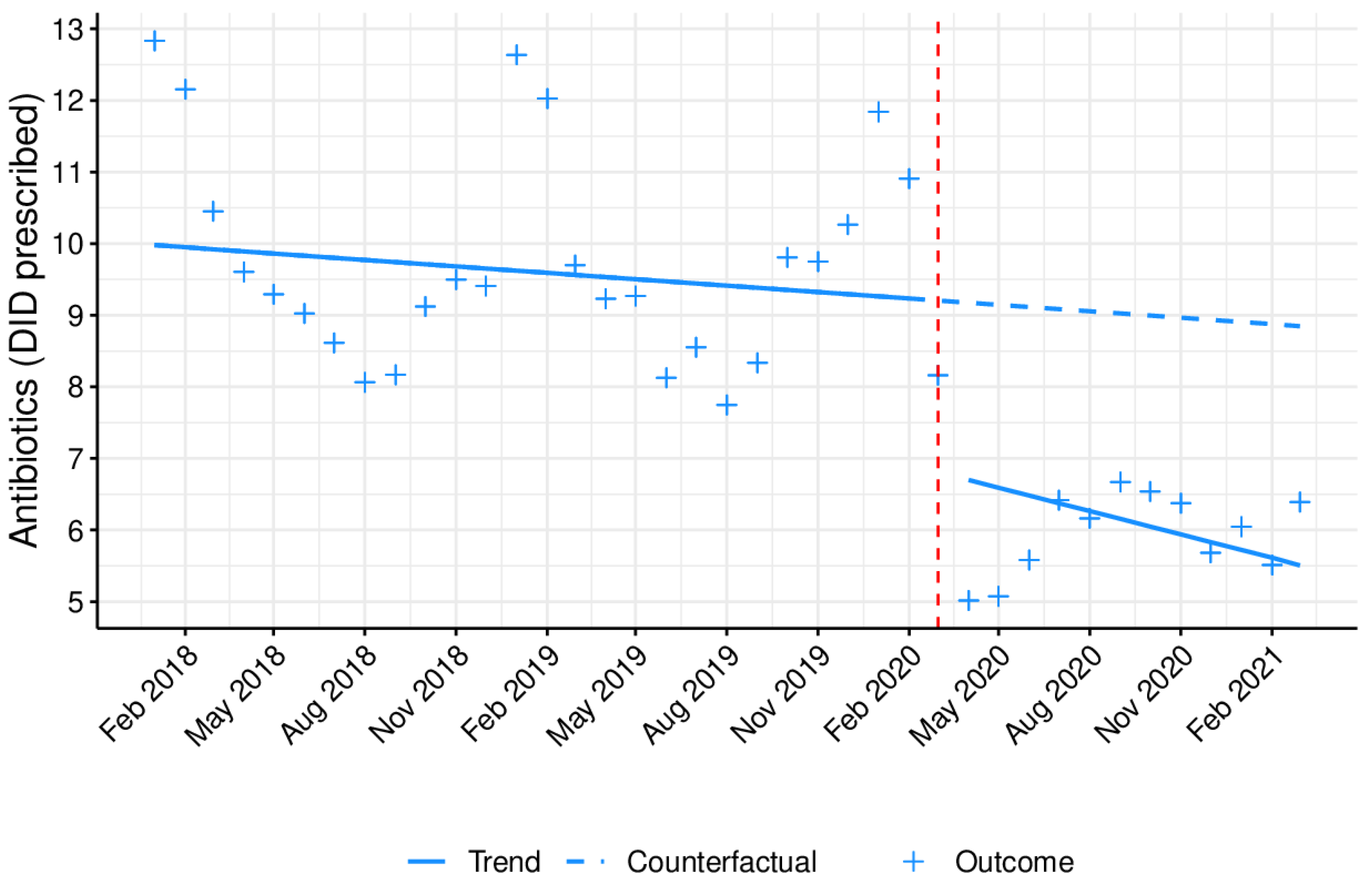
2.1. The Impact of the COVID-19 Pandemic on the Prescription of Antibiotics in Outpatient Care
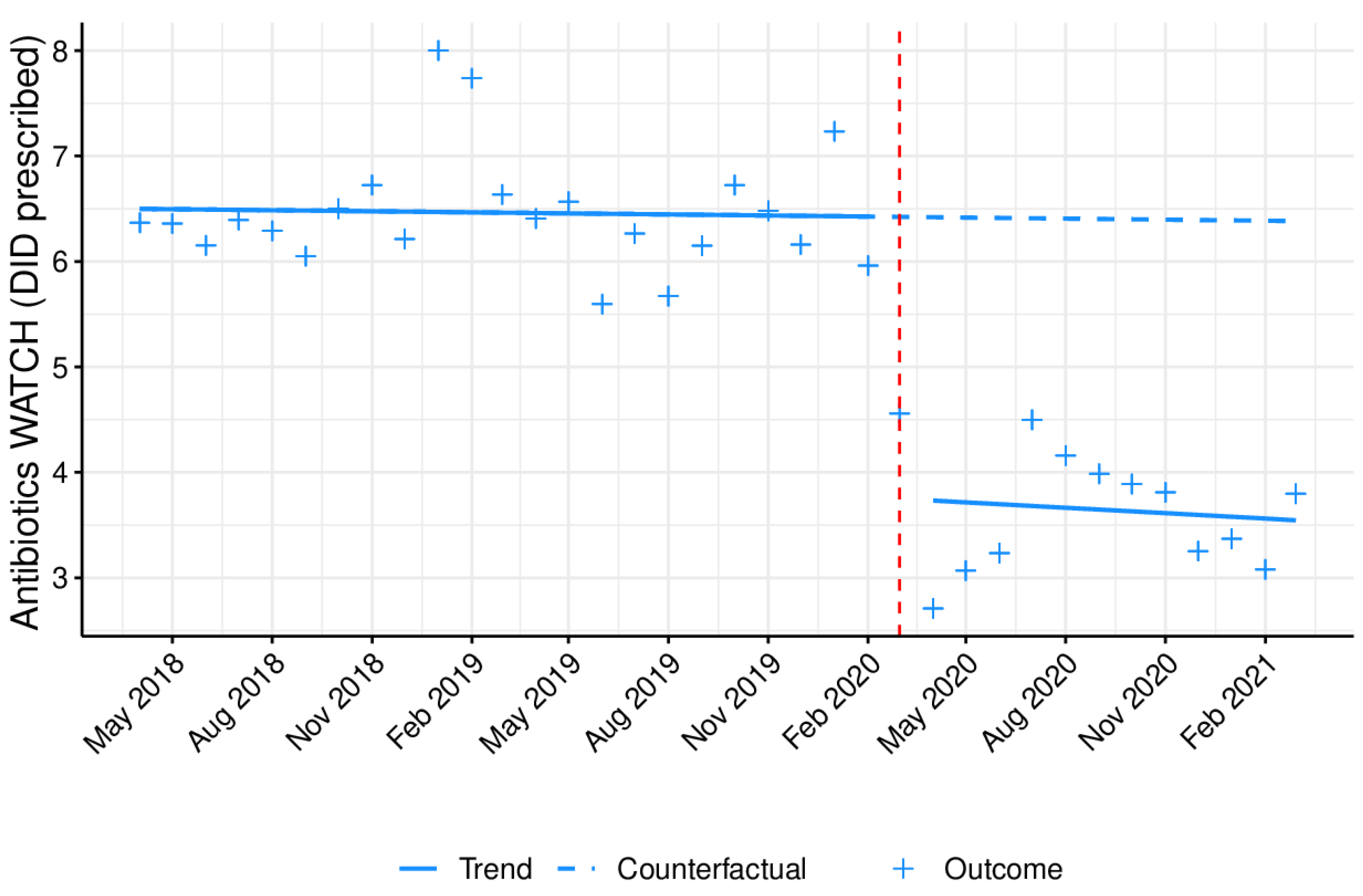
2.2. The Impact of the COVID-19 Pandemic on the Prescription of Antibiotics Associated with Increased Antibiotic Resistance in Outpatient Care—Antibiotics from the WHO’s Watch Group
2.3. Sensitivity Analysis: The Effect of the COVID-19 Pandemic on the Prescription of Oral Antidiabetics
3. Discussion
3.1. Most Relevant Results of the Study
3.2. Interpretation of the Main Results
3.3. Secondary Outcomes
3.4. Comparison with Other Studies
3.5. Strengths and Weaknesses of the Study
4. Materials and Methods
4.1. Setting
4.2. Study Drugs
4.3. Study Design and Data Source
4.4. Statistical Analysis
4.5. Sensitivity Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Xie, M.; Chen, Q. Insight into 2019 novel coronavirus—An updated interim review and lessons from SARS-CoV and MERS-CoV. Int. J. Infect. Dis. 2020, 94, 119–124. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 23 November 2020).
- European Centre for Disease Prevention and Control. COVID-19 Situation Update Worldwide, as of Week 17, Updated 6 May 2021. 2021. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 7 May 2021).
- Presidência do Conselho de Ministros. Decreto do Presidente da República n.o 14-A/2020. Diário da República. 18 March 2020. Available online: https://dre.pt/pesquisa/-/search/130399862/details/maximized (accessed on 7 May 2021).
- Presidência do Conselho de Ministros. Decreto no. 2-A/2020—Regulamenta a aplicação do estado de emergência decretado pelo Presidente da República. Diário da República. 20 March 2020. Available online: https://dre.pt/home/-/dre/130473161/details/maximized (accessed on 7 May 2021).
- Güner, R.; Hasanoğlu, İ.; Aktaş, F. COVID-19: Prevention and control measures in community. TURKISH J. Med. Sci. 2020, 50, 571–577. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. COVID-19 Situation Update for the EU/EEA, as of 7 May 2021. 2021. Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 7 May 2021).
- World Health Organization. Clinical Management of COVID-19 Interim Guidance—May 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Abelenda-Alonso, G.; Padullés, A.; Rombauts, A.; Gudiol, C.; Pujol, M.; Alvarez-Pouso, C.; Jodar, R.; Carratalà, J. Antibiotic prescription during the COVID-19 pandemic: A biphasic pattern. Infect. Control Hosp. Epidemiol. 2020, 41, 1371–1372. [Google Scholar] [CrossRef] [PubMed]
- Beović, B.; Doušak, M.; Ferreira-Coimbra, J.; Nadrah, K.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Ayoade, F.; Rello, J.; Erdem, H. Antibiotic use in patients with COVID-19: A ‘snapshot’ Infectious Diseases International Research Initiative (ID-IRI) survey. J. Antimicrob. Chemother. 2020, 75, 3386–3390. [Google Scholar] [CrossRef]
- Chedid, M.; Waked, R.; Haddad, E.; Chetata, N.; Saliba, G.; Choucair, J. Antibiotics in treatment of COVID-19 complications: A review of frequency, indications, and efficacy. J. Infect. Public Health 2021, 14, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Baño, J.; Rossolini, G.M.; Schultsz, C.; Tacconelli, E.; Murthy, S.; Ohmagari, N.; Holmes, A.; Bachmann, T.; Goossens, H.; Canton, R.; et al. Key considerations on the potential impacts of the COVID-19 pandemic on antimicrobial resistance research and surveillance. Trans. R. Soc. Trop. Med. Hyg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bleyzac, N.; Goutelle, S.; Bourguignon, L.; Tod, M. Azithromycin for COVID-19: More Than Just an Antimicrobial? Clin. Drug Investig. 2020, 40, 683–686. [Google Scholar] [CrossRef] [PubMed]
- Oldenburg, C.E.; Doan, T. Azithromycin for severe COVID-19. Lancet 2020, 396, 936–937. [Google Scholar] [CrossRef]
- Demsie, D.G.; Gebre, A.K.; Yimer, E.M.; Alema, N.M.; Araya, E.M.; Bantie, A.T.; Allene, M.D.; Gebremedhin, H.; Yehualaw, A.; Tafere, C.; et al. Glycopeptides as Potential Interventions for COVID-19. Biol. Targets Ther. 2020, 14, 107–114. [Google Scholar] [CrossRef]
- Baron, S.A.; Devaux, C.; Colson, P.; Raoult, D.; Rolain, J.-M. Teicoplanin: An alternative drug for the treatment of COVID-19? Int. J. Antimicrob. Agents 2020, 55, 105944. [Google Scholar] [CrossRef]
- World Health Organization. The 2019 WHO AWaRe Classification of Antibiotics for Evaluation and Monitoring of Use; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Jornal Publico. Quase 1,4 Milhões de Consultas Ficaram por Fazer no SNS por Causa da Pandemia. 2020. Available online: https://www.publico.pt/2020/05/20/sociedade/noticia/quase-14-milhoes-consultas-ficaram-sns-causa-pandemia-1917448 (accessed on 10 December 2020).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19). JAMA 2020, 324, 782. [Google Scholar] [CrossRef] [PubMed]
- Ohannessian, R.; Duong, T.A.; Odone, A. Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action. JMIR Public Heal. Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef]
- Haynes, L. GPs Call for Suspension of Routine Appointments during Coronavirus Outbreak. 2020. Available online: https://www.gponline.com/gps-call-suspension-routine-appointments-during-coronavirus-outbreak/article/1676337 (accessed on 10 December 2020).
- World Health Organization—Europe Preventing the COVID-19 Pandemic from Causing an Antibiotic Resistance Catastrophe. 2020. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/antimicrobial-resistance/news/news/2020/11/preventing-the-covid-19-pandemic-from-causing-an-antibiotic-resistance-catastrophe (accessed on 12 January 2020).
- Butler, C.C.; Dorward, J.; Yu, L.-M.; Gbinigie, O.; Hayward, G.; Saville, B.R.; Van Hecke, O.; Berry, N.; Detry, M.; Saunders, C.; et al. Azithromycin for community treatment of suspected COVID-19 in people at increased risk of an adverse clinical course in the UK (PRINCIPLE): A randomised, controlled, open-label, adaptive platform trial. Lancet 2021, 397, 1063–1074. [Google Scholar] [CrossRef]
- Han, S.M.; Greenfield, G.; Majeed, A.; Hayhoe, B. Impact of Remote Consultations on Antibiotic Prescribing in Primary Health Care: Systematic Review. J. Med. Internet Res. 2020, 22, e23482. [Google Scholar] [CrossRef] [PubMed]
- Miranda, C.; Silva, V.; Capita, R.; Alonso-Calleja, C.; Igrejas, G.; Poeta, P. Implications of antibiotics use during the COVID-19 pandemic: Present and future. J. Antimicrob. Chemother. 2020, 75, 3413–3416. [Google Scholar] [CrossRef] [PubMed]
- Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. Vital surveillances: The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19)—China, 2020. China CDC Wkly. 2020, 2, 113–122. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Castro-Sanchez, E.; Charani, E.; Davies, F.; Satta, G.; Ellington, M.J.; Holmes, A.H. COVID-19 and the potential long-term impact on antimicrobial resistance. J. Antimicrob. Chemother. 2020, 75, 1681–1684. [Google Scholar] [CrossRef]
- Bai, Y.-X.; Xu, Y.-H.; Wang, X.; Sun, C.; Guo, Y.; Qiu, S.; Ma, K.-W. Advances in SARS-CoV-2: A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9208–9215. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Rapid Risk Assessment: Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK—Eighth Update; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020. [Google Scholar]
- Martin, A.J.; Shulder, S.; Dobrzynski, D.; Quartuccio, K.; Pillinger, K.E. Risk Factors Associated with Increased Antibiotic Use in COVID-19 Hospitalized Patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Getahun, H.; Smith, I.; Trivedi, K.; Paulin, S.; Balkhy, H.H. Tackling antimicrobial resistance in the COVID-19 pandemic. Bull. World Health Organ. 2020, 98, 442–442A. [Google Scholar] [CrossRef]
- Zhu, N.; Aylin, P.; Rawson, T.; Gilchrist, M.; Majeed, A.; Holmes, A. Investigating the impact of COVID-19 on primary care antibiotic prescribing in North West London across two epidemic waves. Clin. Microbiol. Infect. 2021, 27, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.M.; Glover, R.E.; McQuaid, C.F.; Olaru, I.D.; Gallandat, K.; Leclerc, Q.J.; Fuller, N.M.; Willcocks, S.J.; Hasan, R.; van Kleef, E.; et al. Antimicrobial resistance and COVID-19: Intersections and implications. Elife 2021, 10, e64139. [Google Scholar] [CrossRef] [PubMed]
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef]
- Infarmed, I.P. Comunicado de Imprensa: Dia Europeu do Antibiótico; Assessoria de Imprensa do Infarmed, I.P.: Lisbon, Portugal, 2020. [Google Scholar]
- Malcolm, W.; Seaton, R.A.; Haddock, G.; Baxter, L.; Thirlwell, S.; Russell, P.; Cooper, L.; Thomson, A.; Sneddon, J. Impact of the COVID-19 pandemic on community antibiotic prescribing in Scotland. JAC-Antimicrobial Resist. 2020, 2, dlaa105. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA—Annual Epidemiological Report for 2019; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2019. [Google Scholar]
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Ewusie, J.E.; Blondal, E.; Soobiah, C.; Beyene, J.; Thabane, L.; Straus, S.E.; Hamid, J.S. Methods, applications, interpretations and challenges of interrupted time series (ITS) data: Protocol for a scoping review. BMJ Open 2017, 7, e016018. [Google Scholar] [CrossRef]
- Fundação Francisco Manuel dos Santos. Pordata n.d. Available online: https://www.pordata.pt/Portugal (accessed on 18 December 2020).
- Simões, J.d.A.; Augusto, G.F.; Fronteira, I.; Hernandez-Quevedo, C. Portugal: Health system review. Health Syst. Transit. 2017, 19, 1–184. [Google Scholar]
- Ministério da Saúde. Portaria n.o 195-D/2015 de 30 de junho—Regimes de comparticipação de medicamentos. Diário da República, 30 June 2015; 4542-(11) a 4542-(15). [Google Scholar]
- WHO Collaborating Centre for Drug Statistics Methodology—Norwegian Institute of Public Health. Antibacterials for Systemic Use 2019. Available online: https://www.whocc.no/atc_ddd_index/?code=J01&showdescription=no (accessed on 10 December 2020).
- World Health Organization. Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for Drug Resistant Bacterial Infections, Including Tuberculosis; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Sruamsiri, R.; Wagner, A.K.; Ross-Degnan, D.; Lu, C.Y.; Dhippayom, T.; Ngorsuraches, S.; Chaiyakunapruk, N. Expanding access to high-cost medicines through the E2 access program in Thailand: Effects on utilisation, health outcomes and cost using an interrupted time-series analysis. BMJ Open 2016, 6, e008671. [Google Scholar] [CrossRef] [Green Version]
- Kontopantelis, E.; Doran, T.; Springate, D.A.; Buchan, I.; Reeves, D. Regression based quasi-experimental approach when randomisation is not an option: Interrupted time series analysis. BMJ 2015, 350, h2750. [Google Scholar] [CrossRef] [Green Version]
- Serviços Partilhados do Ministério da Saúde (SPMS). System of Information and Monitoring of the Portuguese National Health System (SIM@SNS) n.d. Available online: https://bicsp.min-saude.pt/pt/investigacao/Paginas/medicamentoprescritor_publico.aspx?isdlg=1 (accessed on 24 March 2021).
- Instituto Nacional de Estatística—Portugal. 2019 Annual Provisional Resident Population Estimates 2020. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&contecto=pi&indOcorrCod=0008273&selTab=tab0&xlang=en (accessed on 24 March 2021).
- Sax, C.; Eddelbuettel, D. Seasonal Adjustment by X-13ARIMA-SEATS in R. J. Stat. Softw. 2018, 87, 1–17. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 31 July 2020).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2018 | 2019 | Mean 2018 and 2019 | 2020 | Change in Percentage | ||
|---|---|---|---|---|---|---|
| Antibiotic Prescribing (DID) | JANUARY | 12.8 | 12.6 | 12.7 | 11.8 | −7.0 |
| FEBRUARY | 12.2 | 12.0 | 12.1 | 10.9 | −9.8 | |
| MARCH | 10.5 | 9.7 | 10.1 | 8.2 | −19.0 | |
| APRIL | 9.6 | 9.2 | 9.4 | 5.0 | −46.7 | |
| MAY | 9.3 | 9.3 | 9.3 | 5.1 | −45.3 | |
| JUNE | 9.0 | 8.1 | 8.6 | 5.6 | −34.9 | |
| JULY | 8.6 | 8.6 | 8.6 | 6.4 | −25.2 | |
| AUGUST | 8.1 | 7.8 | 7.9 | 6.2 | −22.0 | |
| SEPTEMBER | 8.2 | 8.3 | 8.3 | 6.7 | −19.2 | |
| OCTOBER | 9.1 | 9.8 | 9.5 | 6.5 | −30.9 | |
| NOVEMBER | 9.5 | 9.8 | 9.6 | 6.4 | −33.8 | |
| DECEMBER | 9.4 | 10.3 | 9.8 | 5.7 | −42.2 | |
| WATCH Antibiotics Group Prescribing (DID) | JANUARY * | - | 8.0 | 8.0 | 7.2 | 9.6 |
| FEBRUARY * | - | 7.7 | 7.7 | 6.0 | −23.0 | |
| MARCH * | - | 6.6 | 6.6 | 4.6 | −31.3 | |
| APRIL | 6.4 | 6.4 | 6.4 | 2.7 | −57.6 | |
| MAY | 6.4 | 6.6 | 6.5 | 3.1 | −52.5 | |
| JUNE | 6.2 | 5.6 | 5.9 | 3.2 | −44.9 | |
| JULY | 6.4 | 6.3 | 6.3 | 4.5 | −28.9 | |
| AUGUST | 6.3 | 5.7 | 6.0 | 4.2 | −30.5 | |
| SEPTEMBER | 6.1 | 6.2 | 6.1 | 4.0 | −34.6 | |
| OCTOBER | 6.5 | 6.7 | 6.6 | 3.9 | −41.2 | |
| NOVEMBER | 6.7 | 6.5 | 6.6 | 3.8 | −42.3 | |
| DECEMBER | 6.2 | 6.2 | 6.2 | 3.3 | −47.4 |
| Time: January 2018 to March 2021 | Immediate Effect | Long Term Effect | ||||
|---|---|---|---|---|---|---|
| B | 95%CI | B | 95%CI | B | 95%CI | |
| Antibiotic prescribing (DID) | −0.009 | (−0.043; 0.024) | −1.6 * | (−2.5; −0.70) | 0.011 | (−0.094; 0.12) |
| Third-generation cephalosporins prescribing (DID) | 8.02 × 10−5 | (−2.5 × 10−4; 4.1 × 10−4) | −0.010 * | (−0.019; −0.002) | 1.5 × 10−4 | (−0.001; 0.001) |
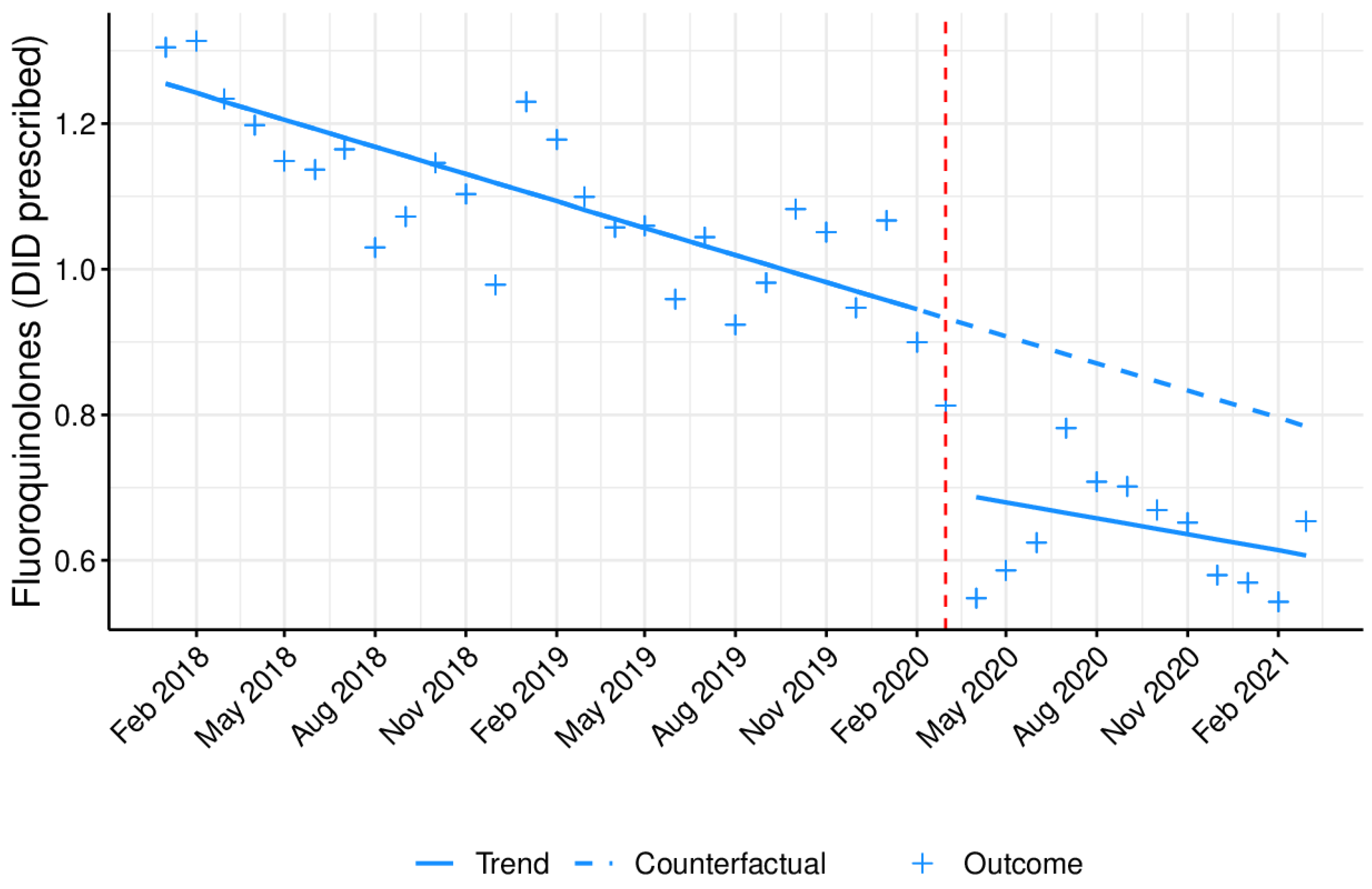
| Fluoroquinolone prescribing (DID) | −0.012 * | (−0.017; −0.008) | −0.24 * | (−0.37; −0.11) | 0.005 | (−0.010; 0.020) |
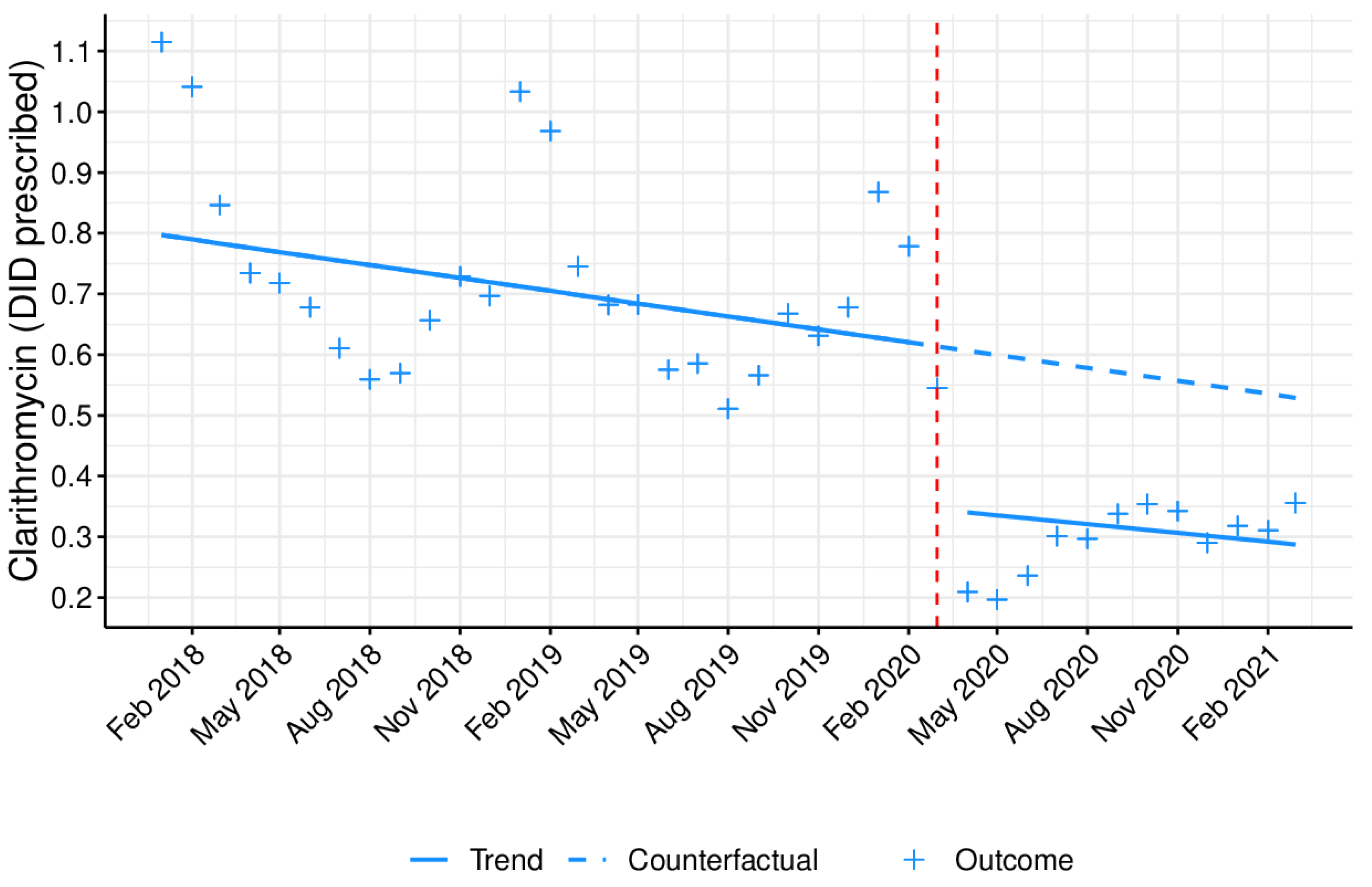
| Clarithromycin prescribing (DID) | −0.003 | (−0.006; 0.001) | −0.18 * | (−0.27; −0.095) | 0.006 | (−0.002; 0.015) |
| Time: April 2018 to March 2021 | Immediate Effect | Long Term Effect | ||||
|---|---|---|---|---|---|---|
| B | 95%CI | B | 95%CI | B | 95%CI | |
| Watch antibiotics group prescribing (DID) | −0.020 | (−0.056; 0.016) | −2.2 * | (−3.0; −1.3) | −0.043 | (−0.13; 0.046) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, T.M.; Estrela, M.; Gomes, E.R.; Piñeiro-Lamas, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. The Impact of the COVID-19 Pandemic on Antibiotic Prescribing Trends in Outpatient Care: A Nationwide, Quasi-Experimental Approach. Antibiotics 2021, 10, 1040. https://doi.org/10.3390/antibiotics10091040
Silva TM, Estrela M, Gomes ER, Piñeiro-Lamas M, Figueiras A, Roque F, Herdeiro MT. The Impact of the COVID-19 Pandemic on Antibiotic Prescribing Trends in Outpatient Care: A Nationwide, Quasi-Experimental Approach. Antibiotics. 2021; 10(9):1040. https://doi.org/10.3390/antibiotics10091040
Chicago/Turabian StyleSilva, Tânia Magalhães, Marta Estrela, Eva Rebelo Gomes, Maria Piñeiro-Lamas, Adolfo Figueiras, Fátima Roque, and Maria Teresa Herdeiro. 2021. "The Impact of the COVID-19 Pandemic on Antibiotic Prescribing Trends in Outpatient Care: A Nationwide, Quasi-Experimental Approach" Antibiotics 10, no. 9: 1040. https://doi.org/10.3390/antibiotics10091040
APA StyleSilva, T. M., Estrela, M., Gomes, E. R., Piñeiro-Lamas, M., Figueiras, A., Roque, F., & Herdeiro, M. T. (2021). The Impact of the COVID-19 Pandemic on Antibiotic Prescribing Trends in Outpatient Care: A Nationwide, Quasi-Experimental Approach. Antibiotics, 10(9), 1040. https://doi.org/10.3390/antibiotics10091040