
Influence of Anti-Infective Periodontal Therapy on Subgingival Microbiota Evaluated by Chair-Side Test Compared to qPCR—A Clinical Follow-Up Study

 ,
,  and
and
Abstract
:1. Introduction
2. Results
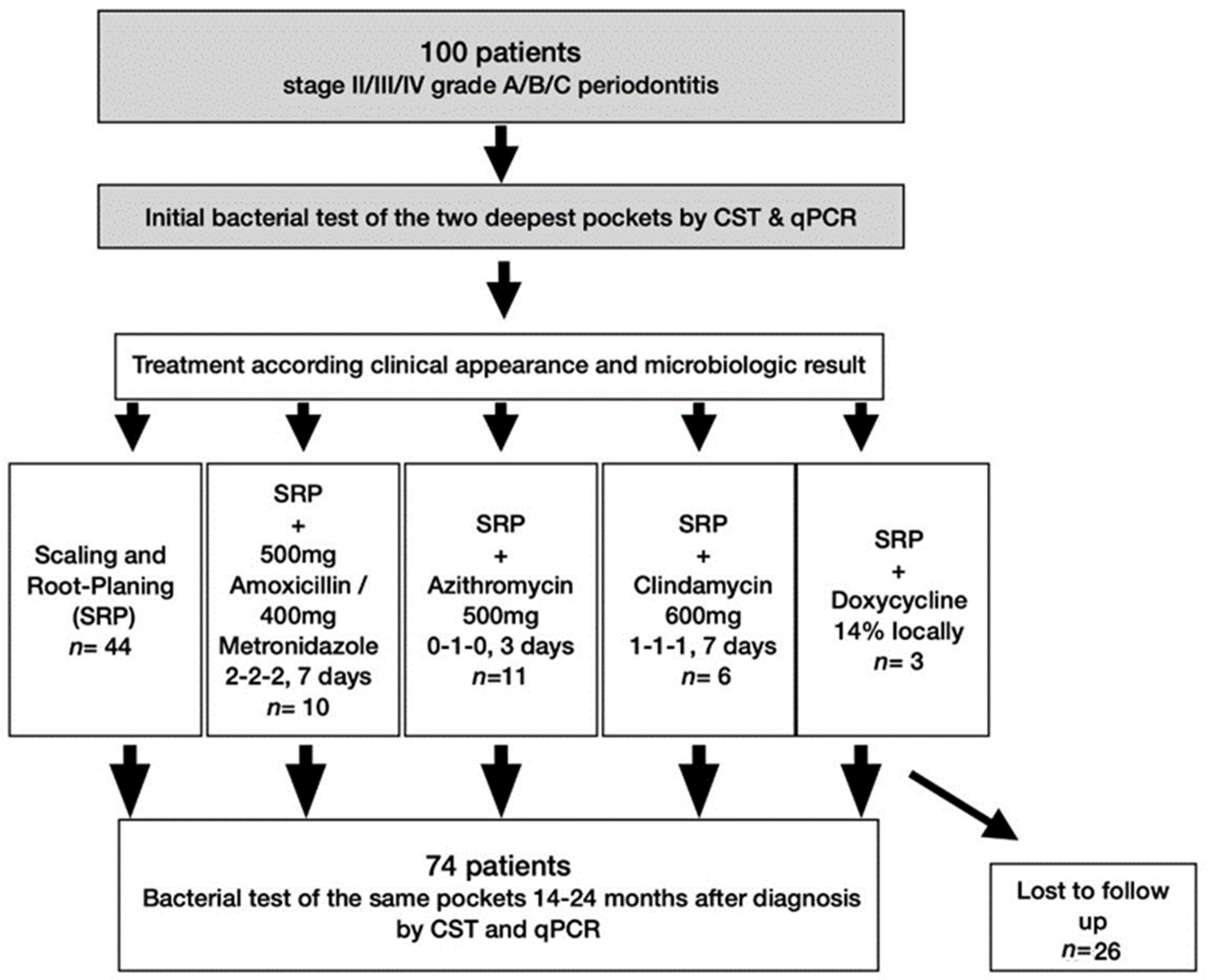
2.1. Patients and Periodontal Therapy
2.2. Bacterial Elimination (in %) Depending on Treatment Modalities
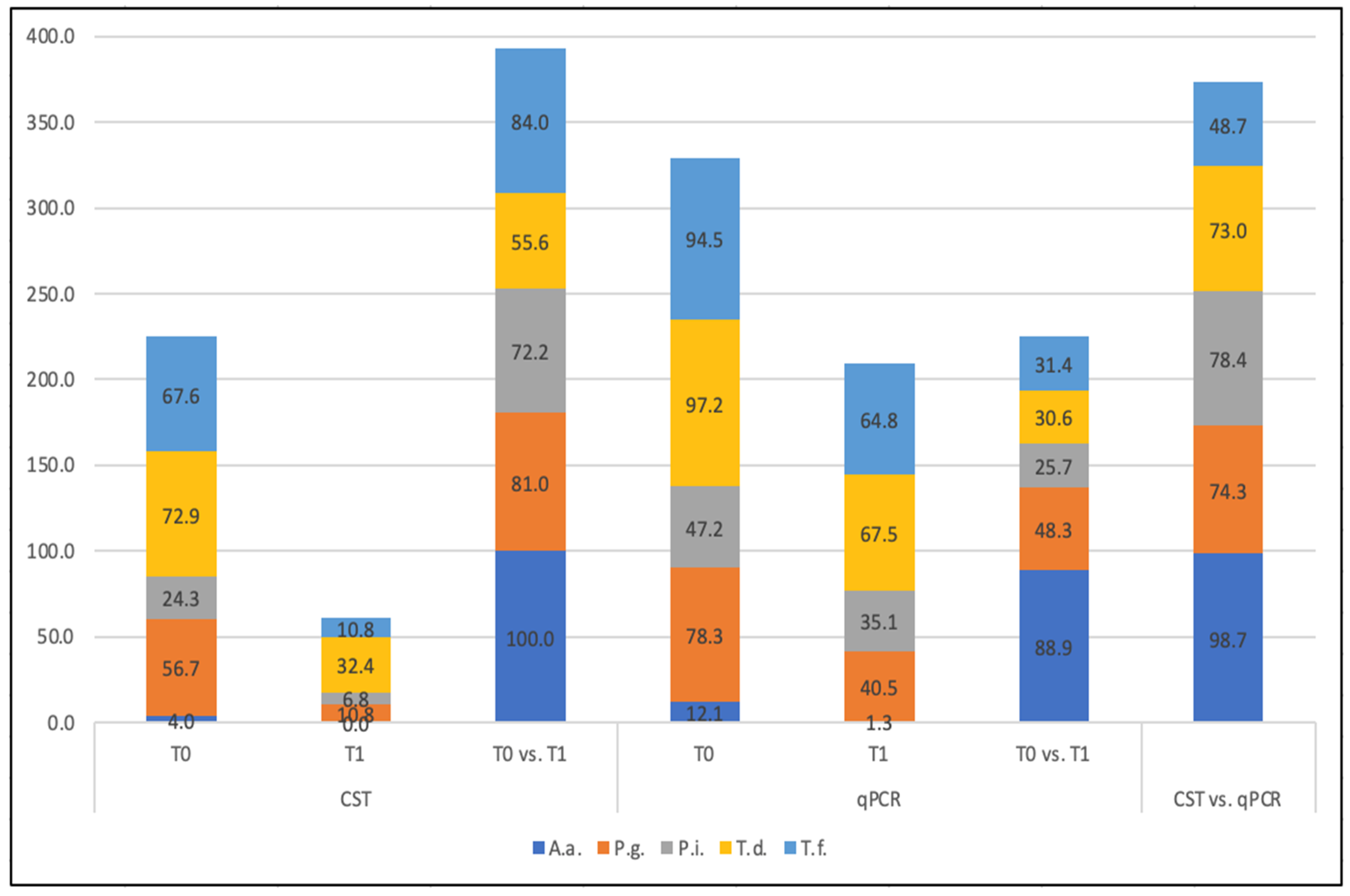
2.3. Elimination Rate of Single Species
2.4. Comparison of CST with qPCR
3. Discussion
4. Materials and Methods
4.1. Study Center and Subjects
4.2. Study Design and Procedure
4.3. Previous Systemic Periodontal Therapy
- SRP only (n = 44): when no P. gingivalis and no A. actinomycetemcomitans were detected, possible detection of T. denticola, T. forsythia and/or P. intermedia;
- SRP + M/A (n = 10): when P. gingivalis and A. actinomycetemcomitans and possibly T. denticola, T. forsythia, and/or P. intermedia were detected, administration of Amoxicillin 500 mg and Metronidazole 400 mg, each 3 times per day for 7 days.
- SRP + A (n = 11): When P. gingivalis, but no A. actinomycetemcomitans and possibly T. denticola, T. forsythia, and/or P. intermedia, was detected [34], administration of 500 mg, once per day (for 3 days) Azithromycin;
- SRP + local D (n = 3): when only 4–5 pockets were present and no A. actinomycetemcomitans was detected, 14% Doxycycline gel (Ligosan® slow release, Heraeus Kulzer, Hanau, Germany) was locally administered [41].
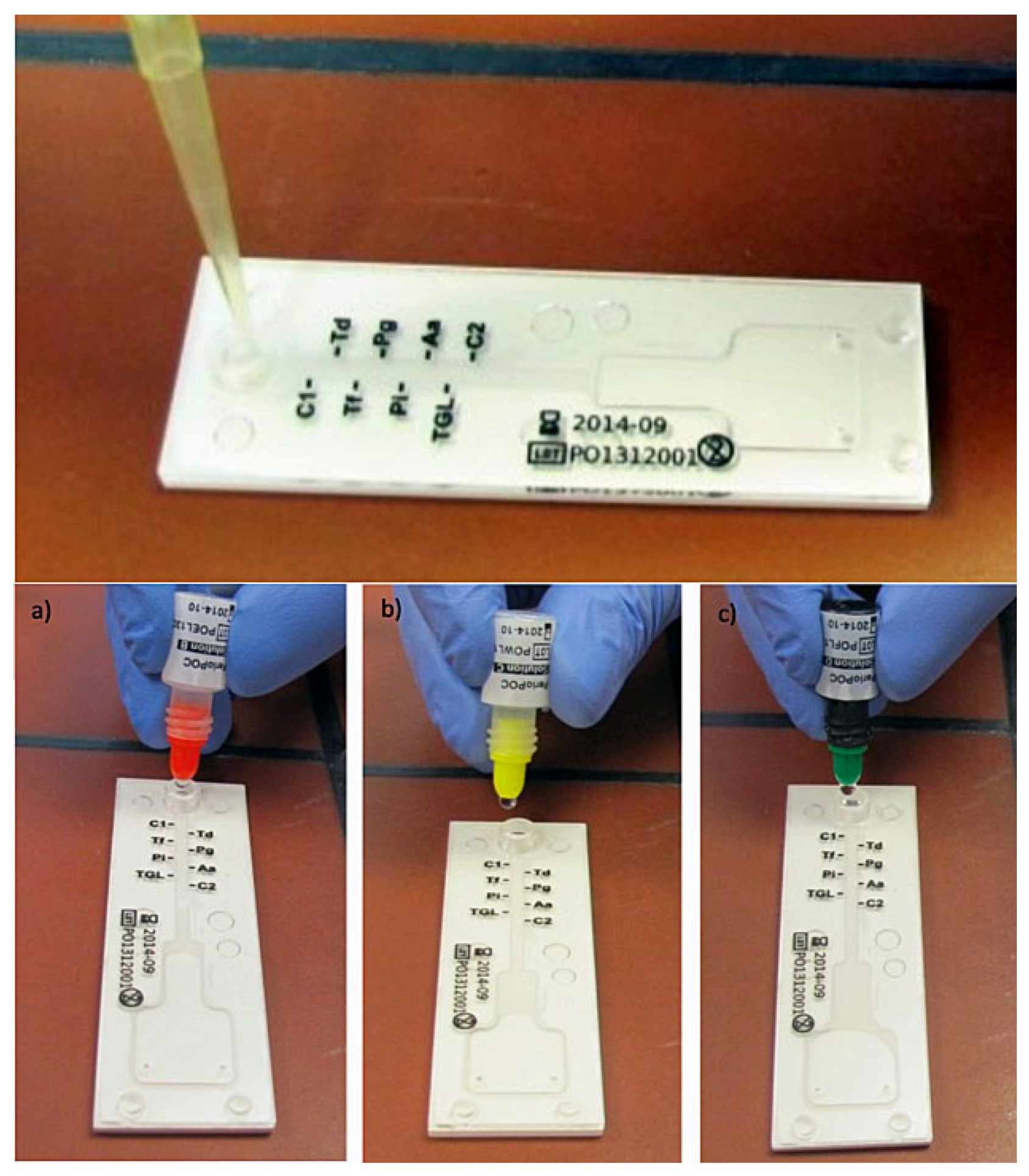
4.4. Sample Collection for CST and qPCR
4.5. Sample Size, Data Management and Data Collection Forms
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Sanz, M. Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontol. 2000 2020, 83, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Arweiler, N.B.; Netuschil, L. The Oral Microbiota. Adv. Exp. Med. Biol. 2016, 902, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Arweiler, N.B.; Marx, V.K.; Laugisch, O.; Sculean, A.; Auschill, T.M. Clinical evaluation of a newly developed chairside test to determine periodontal pathogens. J. Periodontol. 2020, 91, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Mombelli, A.; Cionca, N.; Almaghlouth, A.; Decaillet, F.; Courvoisier, D.S.; Giannopoulou, C. Are there specific benefits of amoxicillin plus metronidazole in Aggregatibacter actinomycetemcomitans-associated periodontitis? Double-masked, randomized clinical trial of efficacy and safety. J. Periodontol. 2013, 84, 715–724. [Google Scholar] [CrossRef]
- Mombelli, A.; Almaghlouth, A.; Cionca, N.; Cancela, J.; Courvoisier, D.S.; Giannopoulou, C. Microbiologic Response to Periodontal Therapy and Multivariable Prediction of Clinical Outcome. J. Periodontol. 2017, 88, 1253–1262. [Google Scholar] [CrossRef]
- Nibali, L.; Koidou, V.P.; Hamborg, T.; Donos, N. Empirical or microbiologically guided systemic antimicrobials as adjuncts to non-surgical periodontal therapy? A systematic review. J. Clin. Periodontol. 2019, 46, 999–1012. [Google Scholar] [CrossRef]
- Falkenstein, S.; Stein, J.M.; Henne, K.; Conrads, G. Trends in antibiotic use and microbial diagnostics in periodontal treatment: Comparing surveys of German dentists in a ten-year period. Clin. Oral Investig. 2016, 20, 2203–2210. [Google Scholar] [CrossRef]
- Eick, S.; Nydegger, J.; Burgin, W.; Salvi, G.E.; Sculean, A.; Ramseier, C. Microbiological analysis and the outcomes of periodontal treatment with or without adjunctive systemic antibiotics-a retrospective study. Clin. Oral Investig. 2018, 22, 3031–3041. [Google Scholar] [CrossRef]
- Guerrero, A.; Nibali, L.; Lambertenghi, R.; Ready, D.; Suvan, J.; Griffiths, G.S.; Wilson, M.; Tonetti, M.S. Impact of baseline microbiological status on clinical outcomes in generalized aggressive periodontitis patients treated with or without adjunctive amoxicillin and metronidazole: An exploratory analysis from a randomized controlled clinical trial. J. Clin. Periodontol. 2014, 41, 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, G.N.; Bostanci, N.; Marsh, P.D.; Zaura, E. Applications of the oral microbiome in personalized dentistry. Arch. Oral Biol. 2019, 104, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Preus, H.R.; Gjermo, P.; Scheie, A.A.; Baelum, V. The effect of metronidazole on the presence of P. gingivalis and T. forsythia at 3 and 12 months after different periodontal treatment strategies evaluated in a randomized, clinical trial. Acta Odontol. Scand. 2015, 73, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Cosgarea, R.; Juncar, R.; Heumann, C.; Tristiu, R.; Lascu, L.; Arweiler, N.; Stavropoulos, A.; Sculean, A. Non-surgical periodontal treatment in conjunction with 3 or 7 days systemic administration of amoxicillin and metronidazole in severe chronic periodontitis patients. A placebo-controlled randomized clinical study. J. Clin. Periodontol. 2016, 43, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Slots, J.; Jorgensen, M.G. Effective, safe, practical and affordable periodontal antimicrobial therapy: Where are we going, and are we there yet? Periodontol. 2000 2002, 28, 298–312. [Google Scholar] [CrossRef]
- Zandbergen, D.; Slot, D.E.; Cobb, C.M.; Van der Weijden, F.A. The clinical effect of scaling and root planing and the concomitant administration of systemic amoxicillin and metronidazole: A systematic review. J. Periodontol. 2013, 84, 332–351. [Google Scholar] [CrossRef] [Green Version]
- Paster, B.J.; Boches, S.K.; Galvin, J.L.; Ericson, R.E.; Lau, C.N.; Levanos, V.A.; Sahasrabudhe, A.; Dewhirst, F.E. Bacterial diversity in human subgingival plaque. J. Bacteriol. 2001, 183, 3770–3783. [Google Scholar] [CrossRef] [Green Version]
- Jervoe-Storm, P.M.; Koltzscher, M.; Falk, W.; Dorfler, A.; Jepsen, S. Comparison of culture and real-time PCR for detection and quantification of five putative periodontopathogenic bacteria in subgingival plaque samples. J. Clin. Periodontol. 2005, 32, 778–783. [Google Scholar] [CrossRef]
- Cosgarea, R.; Baumer, A.; Pretzl, B.; Zehaczek, S.; Kim, T.S. Comparison of two different microbiological test kits for detection of periodontal pathogens. Acta Odontol. Scand. 2010, 68, 115–121. [Google Scholar] [CrossRef]
- Eick, S.; Straube, A.; Guentsch, A.; Pfister, W.; Jentsch, H. Comparison of real-time polymerase chain reaction and DNA-strip technology in microbiological evaluation of periodontitis treatment. Diagn. Microbiol. Infect. Dis. 2011, 69, 12–20. [Google Scholar] [CrossRef]
- Loozen, G.; Boon, N.; Pauwels, M.; Quirynen, M.; Teughels, W. Live/dead real-time polymerase chain reaction to assess new therapies against dental plaque-related pathologies. Mol. Oral Microbiol. 2011, 26, 253–261. [Google Scholar] [CrossRef]
- Polonyi, M.; Prenninger, N.; Arweiler, N.B.; Haririan, H.; Winklehner, P.; Kierstein, S. Assessment of viable periodontal pathogens by reverse transcription quantitative polymerase chain reaction. J. Periodontal. Res. 2013, 48, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Untch, M.; Schlagenhauf, U. Inter- and intra-test agreement of three commercially available molecular diagnostic tests for the identification of periodontal pathogens. Clin. Oral Investig. 2015, 19, 2045–2052. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G., Jr. Compliance and its role in periodontal therapy. Periodontol. 2000 1996, 12, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Bollen, C.M.; Vandekerckhove, B.N.; Dekeyser, C.; Papaioannou, W.; Eyssen, H. Full- vs. partial-mouth disinfection in the treatment of periodontal infections: Short-term clinical and microbiological observations. J. Dent. Res. 1995, 74, 1459–1467. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D.; Teles, R.; Wennstrom, J.L.; Lindhe, J.; Bogren, A.; Hasturk, H.; van Dyke, T.; Wang, X.; Goodson, J.M. Effect of periodontal therapy on the subgingival microbiota over a 2-year monitoring period. I. Overall effect and kinetics of change. J. Clin. Periodontol. 2013, 40, 771–780. [Google Scholar] [CrossRef] [Green Version]
- Fenol, A.; Mathew, S. Compliance to recall visits by patients with periodontitis-Is the practitioner responsible? J. Indian Soc. Periodontol. 2010, 14, 106–108. [Google Scholar] [CrossRef]
- Novaes, A.B., Jr.; de Lima, F.R.; Novaes, A.B. Compliance with supportive periodontal therapy and its relation to the bleeding index. J. Periodontol. 1996, 67, 976–980. [Google Scholar] [CrossRef]
- Famili, P.; Short, E. Compliance with periodontal maintenance at the University of Pittsburgh: Retrospective analysis of 315 cases. Gen. Dent. 2010, 58, e42–e47. [Google Scholar]
- Demetriou, N.; Tsami-Pandi, A.; Parashis, A. Compliance with supportive periodontal treatment in private periodontal practice. A 14-year retrospective study. J. Periodontol. 1995, 66, 145–149. [Google Scholar] [CrossRef]
- De Wet, L.M.; Slot, D.E.; Van der Weijden, G.A. Supportive periodontal treatment: Pocket depth changes and tooth loss. Int. J. Dent. Hyg. 2018, 16, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, H.F.; Buchmann, A.; Friedrich, A.; Eick, S. Nonsurgical therapy of chronic periodontitis with adjunctive systemic azithromycin or amoxicillin/metronidazole. Clin. Oral Investig. 2016, 20, 1765–1773. [Google Scholar] [CrossRef] [PubMed]
- Muniz, F.W.; de Oliveira, C.C.; de Sousa Carvalho, R.; Moreira, M.M.; de Moraes, M.E.; Martins, R.S. Azithromycin: A new concept in adjuvant treatment of periodontitis. Eur. J. Pharmacol. 2013, 705, 135–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oteo, A.; Herrera, D.; Figuero, E.; O’Connor, A.; Gonzalez, I.; Sanz, M. Azithromycin as an adjunct to scaling and root planing in the treatment of Porphyromonas gingivalis-associated periodontitis: A pilot study. J. Clin. Periodontol. 2010, 37, 1005–1015. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms 2022, 10, 337. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Taccardi, D.; Scribante, A. Home Oral Care of Periodontal Patients Using Antimicrobial Gel with Postbiotics, Lactoferrin, and Aloe Barbadensis Leaf Juice Powder vs. Conventional Chlorhexidine Gel: A Split-Mouth Randomized Clinical Trial. Antibiotics 2022, 11, 118. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef]
- Meier, K. Guidance for Industry and FDA Staff-Statistical Guidance on Reporting Results from Studies Evaluating Diagnostic Tests; Food and Drug Administration: Silver Spring, MD, USA, 2007.
- Garrett, P.E.; Lasky, F.D.; Meier, K.L.; Clark, L.W. User Protocol for Evaluating of Qualitative Test Performance: Approved Guideline, 2nd ed.; Clinical and Laboratory Standars Institute: Wayne, PA, USA, 2008. [Google Scholar]
- van Winkelhoff, A.J.; Winkel, E.G. Microbiological diagnostics in periodontics: Biological significance and clinical validity. Periodontol. 2000 2005, 39, 40–52. [Google Scholar] [CrossRef]
- Eickholz, P.; Kim, T.S.; Burklin, T.; Schacher, B.; Renggli, H.H.; Schaecken, M.T.; Holle, R.; Kubler, A.; Ratka-Kruger, P. Non-surgical periodontal therapy with adjunctive topical doxycycline: A double-blind randomized controlled multicenter study. J. Clin. Periodontol. 2002, 29, 108–117. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Therapy | CST | qPCR | CST vs. qPCR | ||
|---|---|---|---|---|---|
| Elimination% | T1/T0 | Elimination% | T1/T0 | Agreement% | |
| SRP | 59.1 | 18/44 | 29.6 | 31/44 | 75.5 |
| SRP + A/M | 90.0 | 1/10 | 30.0 | 7/10 | 82.2 |
| SRP + A | 72.8 | 3/11 | 9.1 | 10/11 | 65.5 |
| SRP + C | 66.7 | 2/6 | 33.3 | 4/6 | 90.0 |
| SRP + D | 66.7 | 1/3 | 33.3 | 2/3 | 40.0 |
| CST | qPCR | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A.a. | P.g. | P.i. | T.d. | T.f. | A.a. | P.g. | P.i. | T.d. | T.f. | |||||||||||
| % | T1/T0 | % | T1/T0 | % | T1/T0 | % | T1/T0 | % | T1/T0 | % | T1/T0 | % | T1/T0 | % | T1/T0 | % | T1/T0 | % | T1/T0 | |
| SRP | n.a | 0/0 | 80.7 | 5/26 | 77.8 | 2/9 | 43.3 | 17/30 | 78.8 | 7/33 | 100 | 0/1 | 33.3 | 20/30 | 22.2 | 14/18 | 26.2 | 31/42 | 22.5 | 31/40 |
| SRP + A/M | 100 | 0/3 | 100 | 0/6 | 80.0 | 1/5 | 80.7 | 5/26 | 77.8 | 2/9 | 80.0 | 1/5 | 77.8 | 2/9 | 50.0 | 3/6 | 60.0 | 4/10 | 50.0 | 5/10 |
| SRP + A | n.a | 0/0 | 40.0 | 3/5 | 100 | 0/2 | 80.7 | 5/26 | 77.8 | 2/9 | 100 | 0/1 | 45.4 | 6/11 | 100 | 8/8 | 18.1 | 9/11 | 36.3 | 7/11 |
| SRP + C | n.a | 0/0 | 100 | 0/5 | 100 | 0/2 | 80.7 | 5/26 | 77.8 | 2/9 | 100 | 0/2 | 100 | 0/6 | 66.6 | 1/3 | 33.3 | 4/6 | 66.6 | 2/6 |
| SRP + D | n.a | 0/0 | n.a | 0/0 | n.a | 0/0 | 50.0 | 1/2 | n.a | 0/0 | n.a | 0/0 | 0 | 2/2 | n.a | 0/0 | 33.3 | 2/3 | 0 | 3/3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laugisch, O.; Auschill, T.M.; Tumbrink, A.; Sculean, A.; Arweiler, N.B. Influence of Anti-Infective Periodontal Therapy on Subgingival Microbiota Evaluated by Chair-Side Test Compared to qPCR—A Clinical Follow-Up Study. Antibiotics 2022, 11, 577. https://doi.org/10.3390/antibiotics11050577
Laugisch O, Auschill TM, Tumbrink A, Sculean A, Arweiler NB. Influence of Anti-Infective Periodontal Therapy on Subgingival Microbiota Evaluated by Chair-Side Test Compared to qPCR—A Clinical Follow-Up Study. Antibiotics. 2022; 11(5):577. https://doi.org/10.3390/antibiotics11050577
Chicago/Turabian StyleLaugisch, Oliver, Thorsten M. Auschill, Anne Tumbrink, Anton Sculean, and Nicole B. Arweiler. 2022. "Influence of Anti-Infective Periodontal Therapy on Subgingival Microbiota Evaluated by Chair-Side Test Compared to qPCR—A Clinical Follow-Up Study" Antibiotics 11, no. 5: 577. https://doi.org/10.3390/antibiotics11050577
APA StyleLaugisch, O., Auschill, T. M., Tumbrink, A., Sculean, A., & Arweiler, N. B. (2022). Influence of Anti-Infective Periodontal Therapy on Subgingival Microbiota Evaluated by Chair-Side Test Compared to qPCR—A Clinical Follow-Up Study. Antibiotics, 11(5), 577. https://doi.org/10.3390/antibiotics11050577