
Evaluation of a Meropenem and Piperacillin Monitoring Program in Intensive Care Unit Patients Calls for the Regular Assessment of Empirical Targets and Easy-to-Use Dosing Decision Tools

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Antimicrobial Treatment
2.3. Pathogen Susceptibility
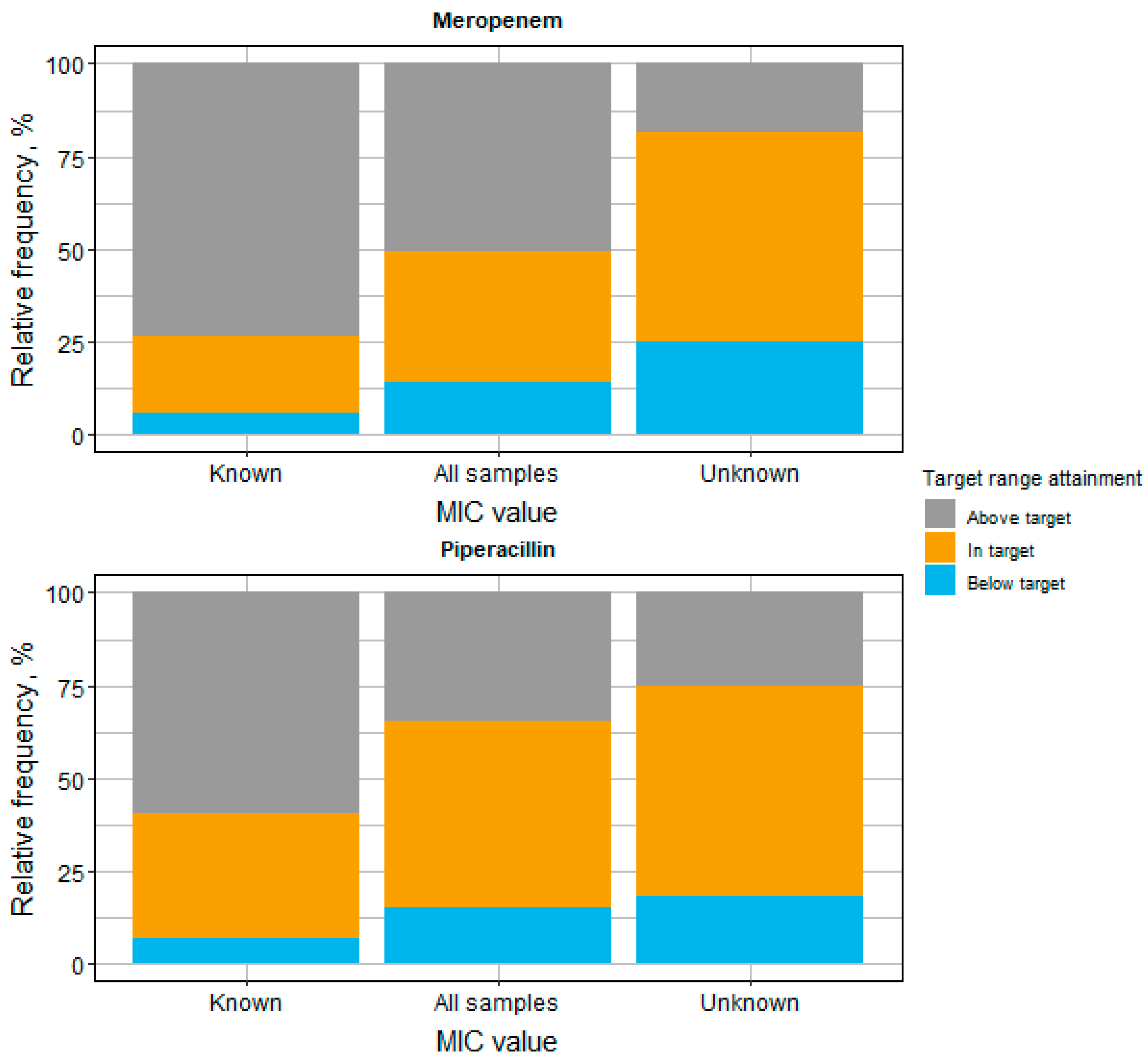
2.4. Target Attainment Assessment
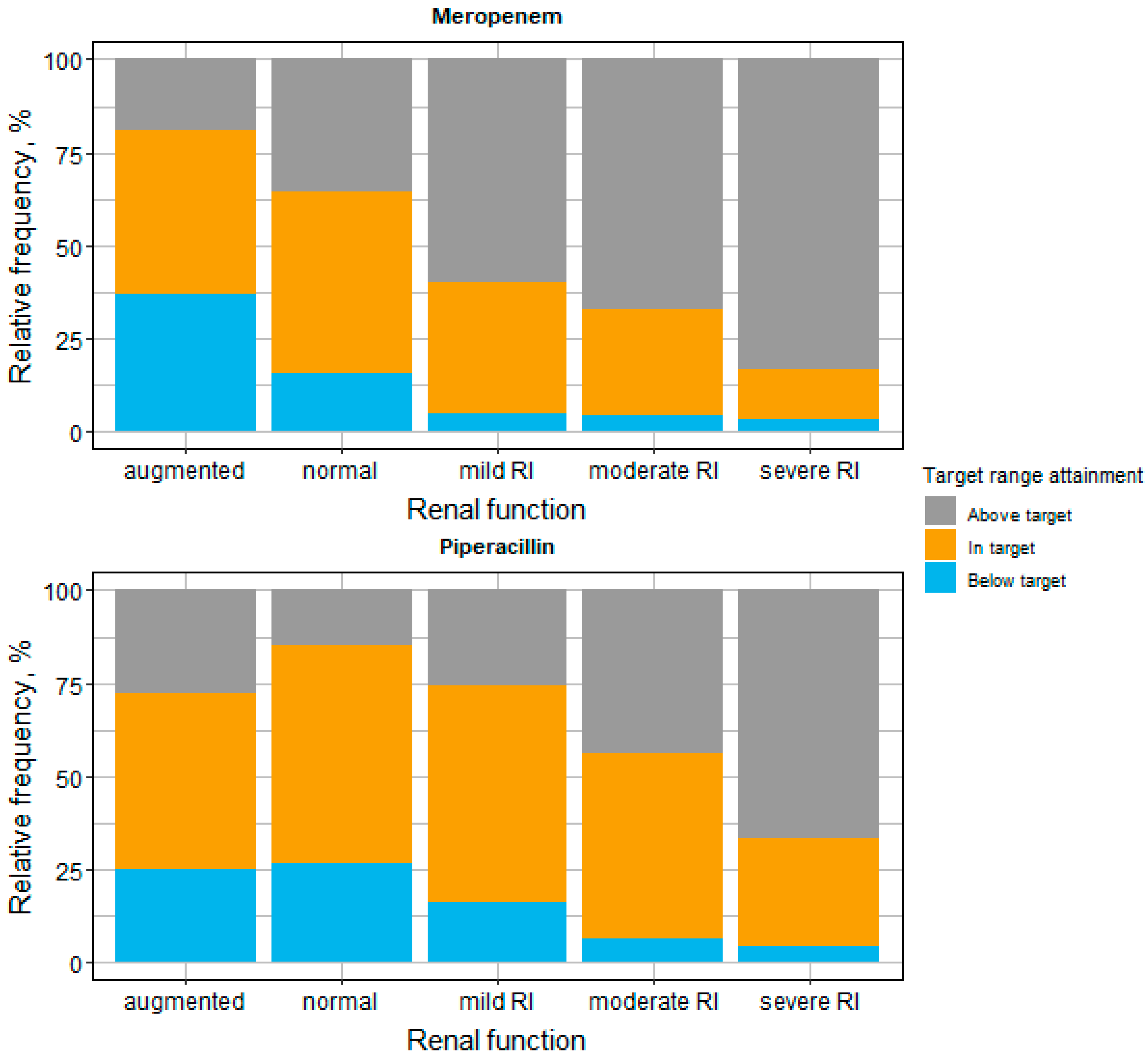
2.5. Target Attainment Assessment in Different Renal Function Groups
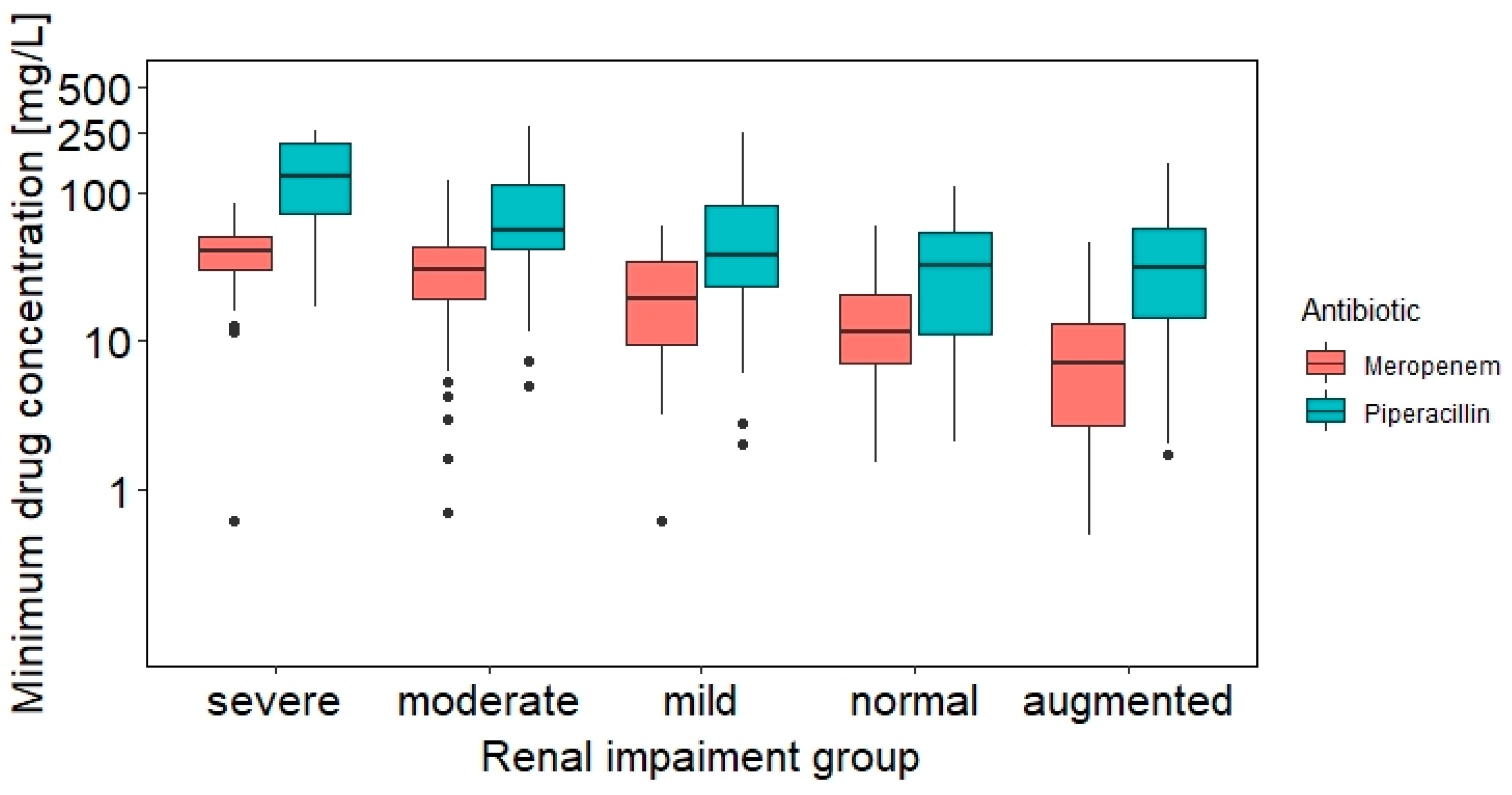
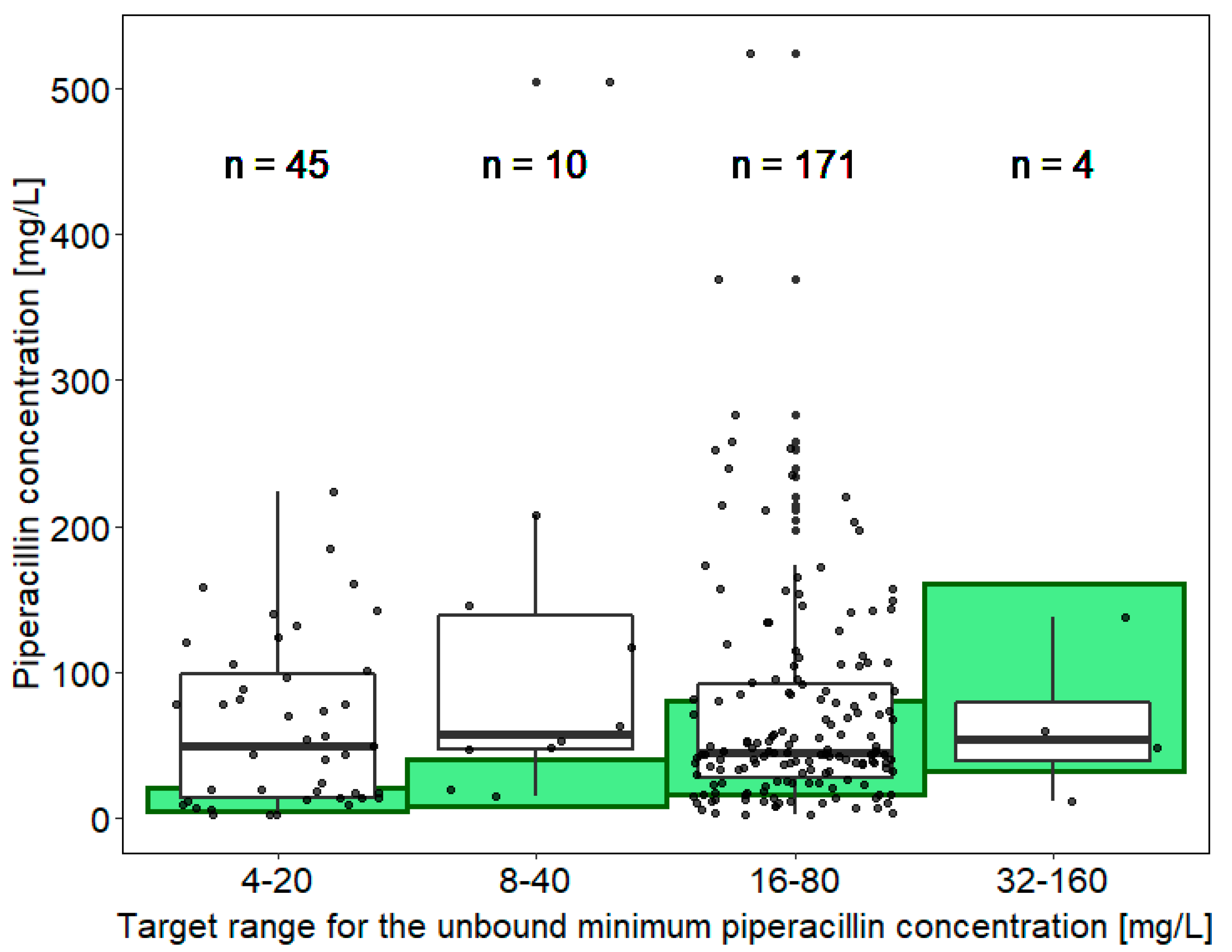
2.6. Drug Concentration Assessment between Different Target Range Groups
2.7. Dosing Adaptations
3. Discussion
4. Materials and Methods
4.1. Study Design, Data Collection and Bioanalytical Method
4.2. Pharmacokinetic/Pharmacodynamic Targets
4.3. Antimicrobial Treatment
4.4. Data Analysis
4.5. Target Attainment Assessment
4.6. Target Attainment Assessment in Different Renal Function Groups
4.7. Drug Concentration Assessment between Different Target Range Groups
4.8. Dosing Adaptations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



Appendix B
Instrumentation and LC-MS/MS Conditions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time [min] | Eluent A [%] | Eluent B [%] |
|---|---|---|
| 0.01 | 99 | 1 |
| 0.35 | 45 | 55 |
| 1.30 | 45 | 55 |
| 1.65 | 1 | 99 |
| 2.10 | 1 | 99 |
| 2.70 | 99 | 1 |
| 3.70 | 99 | 1 |
| Compound | Precursor Ion m/z | Product Ion m/z | Dwell Time [ms] | Collision Energy [V] | Declustering Potential [V] | Entrance Potential [V] | Collision Cell Exit Potential [V] |
|---|---|---|---|---|---|---|---|
| Meropenem 1 | 384.1 | 340.2 | 30 | 11 | 231 | 10 | 24 |
| Meropenem 2 | 384.1 | 298.3 | 20 | 21 | 1 | 10 | 24 |
| Piperacillin 1 | 518.2 | 160.2 | 30 | 9 | 280 | 10 | 22 |
| Piperacillin 2 | 518.2 | 143.3 | 30 | 51 | 191 | 10 | 16 |
| Curtain Gas [psi] | Collision Gas [psi] | Ionspray Voltage [V] | Temperature of Ion Source [°C] | Nebulizing Gas [psi] | Drying Gas [psi] |
|---|---|---|---|---|---|
| 40 | 9 | 4000 | 500 | 45 | 70 |
References
- Morrison, L.; Zembower, T.R. Antimicrobial Resistance. Gastrointest. Endosc. Clin. N. Am. 2020, 30, 619–635. [Google Scholar] [CrossRef] [PubMed]
- Nadimpalli, M.; Delarocque-Astagneau, E.; Love, D.C.; Price, L.B.; Huynh, B.T.; Collard, J.M.; Lay, K.S.; Borand, L.; Ndir, A.; Walsh, T.R.; et al. Combating Global Antibiotic Resistance: Emerging One Health Concerns in Lower-and Middle-Income Countries. Clin. Infect. Dis. 2018, 66, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Zaman, S.B.; Hussain, M.A.; Nye, R.; Mehta, V.; Mamun, K.T.; Hossain, N. A Review on Antibiotic Resistance: Alarm Bells Are Ringing. Cureus 2017, 9, e1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Framework for Development & Stewardship to Combat Antimicrobial Resistance. 2018. Available online: https://Www.Who.Int/Antimicrobial-Resistance/En/ (accessed on 24 April 2022).
- Roberts, J.A.; Kruger, P.; Paterson, D.L.; Lipman, J. Antibiotic Resistance-What’s Dosing Got to Do with It? Crit. Care Med. 2008, 36, 2433–2440. [Google Scholar] [CrossRef] [PubMed]
- Levy Hara, G.; Kanj, S.S.; Pagani, L.; Abbo, L.; Endimiani, A.; Wertheim, H.F.L.; Amábile-Cuevas, C.; Tattevin, P.; Mehtar, S.; Lopes Cardoso, F.; et al. Ten Key Points for the Appropriate Use of Antibiotics in Hospitalised Patients: A Consensus from the Antimicrobial Stewardship and Resistance Working Groups of the International Society of Chemotherapy. Int. J. Antimicrob. Agents 2016, 48, 239–246. [Google Scholar] [CrossRef]
- Lambrini, K. The Rational Use of Antibiotics Medicine. J. Healthc. Commun. 2017, 2, 36. [Google Scholar] [CrossRef]
- Slama, T.G.; Amin, A.; Brunton, S.A.; File, T.M.; Milkovich, G.; Rodvold, K.A.; Sahm, D.F.; Varon, J.; Weiland, D. A Clinician’s Guide to the Appropriate and Accurate Use of Antibiotics: The Council for Appropriate and Rational Antibiotic Therapy (CARAT) Criteria. Am. J. Med. 2005, 118, 1S–6S. [Google Scholar] [CrossRef]
- Gonçalves-Pereira, J.; Póvoa, P. Antibiotics in Critically Ill Patients: A Systematic Review of the Pharmacokinetics of β-Lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining Antibiotic Levels in Intensive Care Unit Patients: Are Current ß-Lactam Antibiotic Doses Sufficient for Critically Ill Patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef]
- Sime, F.B.; Roberts, M.S.; Warner, M.S.; Hahn, U.; Robertson, T.A.; Yeend, S.; Phay, A.; Lehman, S.; Lipman, J.; Peake, S.L.; et al. Altered Pharmacokinetics of Piperacillin in Febrile Neutropenic Patients with Hematological Malignancy. Antimicrob. Agents Chemother. 2014, 58, 3533–3537. [Google Scholar] [CrossRef] [Green Version]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Maier, B.; Schmitt, M.V.; Hartung, N.; Huisinga, W.; Vogeser, M.; Frey, L.; et al. Role of Renal Function in Risk Assessment of Target Non-Attainment after Standard Dosing of Meropenem in Critically Ill Patients: A Prospective Observational Study. Crit. Care 2017, 21, 263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minichmayr, I.K.; Schaeftlein, A.; Kuti, J.L.; Zeitlinger, M.; Kloft, C. Clinical Determinants of Target Non-Attainment of Linezolid in Plasma and Interstitial Space Fluid: A Pooled Population Pharmacokinetic Analysis with Focus on Critically Ill Patients. Clin. Pharmacokinet. 2017, 56, 617–633. [Google Scholar] [CrossRef] [PubMed]
- Minichmayr, I.K.; Roberts, J.A.; Frey, O.R.; Roehr, A.C.; Kloft, C.; Brinkmann, A. Development of a Dosing Nomogram for Continuous-Infusion Meropenem in Critically Ill Patients Based on a Validated Population Pharmacokinetic Model. J. Antimicrob. Chemother. 2018, 73, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Huisinga, W.; Zander, J.; Kloft, C. Development of a Dosing Algorithm for Meropenem in Critically Ill Patients Based on a Population Pharmacokinetic/Pharmacodynamic Analysis. Int. J. Antimicrob. Agents 2019, 54, 309–317. [Google Scholar] [CrossRef]
- Brusselaers, N.; Vogelaers, D.; Blot, S. The Rising Problem of Antimicrobial Resistance in the Intensive Care Unit. Ann. Intensive Care 2011, 1, 47. [Google Scholar] [CrossRef] [Green Version]
- Llor, C.; Bjerrum, L. Antimicrobial Resistance: Risk Associated with Antibiotic Overuse and Initiatives to Reduce the Problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.; Briscoe, S.; McWhinney, B.; Ally, M.; Ungerer, J.; Lipman, J.; Roberts, J.A. Therapeutic Drug Monitoring of B-Lactam Antibiotics in the Critically Ill: Direct Measurement of Unbound Drug Concentrations to Achieve Appropriate Drug Exposures. J. Antimicrob. Chemother. 2018, 73, 3087–3094. [Google Scholar] [CrossRef] [Green Version]
- Muller, A.E.; Huttner, B.; Huttner, A. Therapeutic Drug Monitoring of Beta-Lactams and Other Antibiotics in the Intensive Care Unit: Which Agents, Which Patients and Which Infections? Drugs 2018, 78, 439–451. [Google Scholar] [CrossRef]
- Buyle, F.M.; Decruyenaere, J.; De Waele, J.; Tulkens, P.M.; Van Audenrode, T.; Depuydt, P.; Claeys, G.; Robays, H.; Vogelaers, D. A Survey of Beta-Lactam Antibiotics and Vancomycin Dosing Strategies in Intensive Care Units and General Wards in Belgian Hospitals. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 763–768. [Google Scholar] [CrossRef]
- Baldwin, C.M.; Lyseng-Williamson, K.A.; Keam, S.J. Meropenem: A Review of Its Use in the Treatment of Serious Bacterial Infections. Drugs 2008, 68, 803–838. [Google Scholar] [CrossRef]
- Mltsuyama, J.; Takahata, M.; Yasuda, T.; Saikawa, I. The Mechanism of Action of Piperacillin-Analogues in Vitro; Effect of the Carbon Number at the N-4 Position of 2,3-Dioxopiperazine on the Outer Membrane Permeability, Stability to Beta-Lactamase and Binding Affinity to Penicillin-Binding Proteins. J. Antibiot. (Tokyo) 1987, 40, 868–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolau, D.P. Pharmacokinetic and Pharmacodynamic Properties of Meropenem. Clin. Infect. Dis. 2008, 47, S32–S40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gin, A.; Dilay, L.; Karlowsky, J.A.; Walkty, A.; Rubinstein, E.; Zhanel, G.G. Piperacillin-Tazobactam: A β-Lactam/β-Lactamase Inhibitor Combination. Expert Rev. Anti-Infect. Ther. 2007, 5, 365–383. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Du, X.; Kuti, J.L.; Nicolau, D.P. Clinical Pharmacodynamics of Meropenem in Patients with Lower Respiratory Tract Infections. Antimicrob. Agents Chemother. 2007, 51, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the Treatment with Beta-Lactam Antibiotics in Critically Ill Patients—Guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique—SFPT) and the French Society of Anaesthesia. Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Waele, J.J.; Carrette, S.; Carlier, M.; Stove, V.; Boelens, J.; Claeys, G.; Leroux-Roels, I.; Hoste, E.; Depuydt, P.; Decruyenaere, J.; et al. Therapeutic Drug Monitoring-Based Dose Optimisation of Piperacillin and Meropenem: A Randomised Controlled Trial. Intensive Care Med. 2014, 40, 380–387. [Google Scholar] [CrossRef]
- Liebchen, U.; Paal, M.; Scharf, C.; Schroeder, I.; Grabein, B.; Zander, J.; Siebers, C.; Zoller, M. The ONTAI Study—A Survey on Antimicrobial Dosing and the Practice of Therapeutic Drug Monitoring in German Intensive Care Units. J. Crit. Care 2020, 60, 260–266. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 8.1; 2018. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_8.1_Breakpoint_Tables.xlsx (accessed on 24 April 2022).
- Meronem IV 500 mg & 1 g; Pfizer: New York, NY, USA, 2018; pp. 1–11.
- Pfizer Inc. Tazocin® (Piperacillin and Tazobactam Powder for Injection)—Summary of Product Characteristics. 2014. Available online: https://www.ema.europa.eu/en/documents/referral/tazocin-article-30-referral-annex-iii_en.pdf (accessed on 24 April 2022).
- Vieillard-Baron, A.; Prin, S.; Chergui, K.; Dubourg, O.; Jardin, F. Hemodynamic Instability in Sepsis: Bedside Assessment by Doppler Echocardiography. Am. J. Respir. Crit. Care Med. 2003, 168, 1270–1276. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, M.H. Prediction of Creatinine Clearance from Serum Creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Esteve-Pitarch, E.; Gumucio-Sanguino, V.D.; Cobo-Sacristán, S.; Shaw, E.; Maisterra-Santos, K.; Sabater-Riera, J.; Pérez-Fernandez, X.L.; Rigo-Bonnin, R.; Tubau-Quintano, F.; Carratalà, J.; et al. Continuous Infusion of Piperacillin/Tazobactam and Meropenem in ICU Patients Without Renal Dysfunction: Are Patients at Risk of Underexposure? Eur. J. Drug Metab. Pharmacokinet. 2021, 46, 527–538. [Google Scholar] [CrossRef]
- Mouton, J.W.; Muller, A.E.; Canton, R.; Giske, C.G.; Kahlmeter, G.; Turnidge, J. MIC-Based Dose Adjustment: Facts and Fables. J. Antimicrob. Chemother. 2018, 73, 564–568. [Google Scholar] [CrossRef] [Green Version]
- Zander, J.; Döbbeler, G.; Nagel, D.; Scharf, C.; Huseyn-Zada, M.; Jung, J.; Frey, L.; Vogeser, M.; Zoller, M. Variability of Piperacillin Concentrations in Relation to Tazobactam Concentrations in Critically Ill Patients. Int. J. Antimicrob. Agents 2016, 48, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Scharf, C.; Paal, M.; Schroeder, I.; Vogeser, M.; Draenert, R.; Irlbeck, M.; Zoller, M.; Liebchen, U. Therapeutic Drug Monitoring of Meropenem and Piperacillin in Critical Illness—Experience and Recommendations from One Year in Routine Clinical Practice. Antibiotics 2020, 9, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imani, S.; Buscher, H.; Marriott, D.; Gentili, S.; Sandaradura, I. Too much of a good thing: A retrospective study of β-lactam concentration-toxicity relationships. J. Antimicrob. Chemother. 2017, 72, 2891–2897. [Google Scholar] [CrossRef] [PubMed]
- Quinton, M.-C.; Bodeau, S.; Kontar, L.; Zerbib, Y.; Maizel, J.; Slama, M.; Masmoudi, K.; Lemaire-Hurtel, A.-S.; Bennis, Y. Neurotoxic Concentration of Piperacillin during Continuous Infusion in Critically Ill Patients. Antimicrob. Agents Chemother. 2017, 61, e00654-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharf, C.; Liebchen, U.; Paal, M.; Taubert, M.; Vogeser, M.; Irlbeck, M.; Zoller, M.; Schroeder, I. The higher the better? Defining the optimal beta-lactam target for critically ill patients to reach infection resolution and improve outcome. J. Intensive Care 2020, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Hagel, S.; Bach, F.; Brenner, T.; Bracht, H.; Brinkmann, A.; Annecke, T.; Hohn, A.; Weigand, M.; Michels, G.; Kluge, S.; et al. Effect of therapeutic drug monitoring-based dose optimization of piperacillin/tazobactam on sepsis-related organ dysfunction in patients with sepsis: A randomized controlled trial. Intensive Care Med. 2022, 48, 311–321. [Google Scholar] [CrossRef]
- Carlier, M.; Carrette, S.; Roberts, J.A.; Stove, V.; Verstraete, A.; Hoste, E.; Depuydt, P.; Decruyenaere, J.; Lipman, J.; Wallis, S.C.; et al. Meropenem and Piperacillin/Tazobactam Prescribing in Critically Ill Patients: Does Augmented Renal Clearance Affect Pharmacokinetic/Pharmacodynamic Target Attainment When Extended Infusions Are Used? Crit. Care 2013, 17, R84. [Google Scholar] [CrossRef] [Green Version]
- Chimata, M.; Nagase, M.; Suzuki, Y.; Shimomura, M.; Kakuta, S. Pharmacokinetics of Meropenem in Patients with Various Degrees of Renal Function, Including Patients with End-Stage Renal Disease. Antimicrob. Agents Chemother. 1993, 37, 229–233. [Google Scholar] [CrossRef] [Green Version]
- Tamatsukuri, T.; Ohbayashi, M.; Kohyama, N.; Kobayashi, Y.; Yamamoto, T.; Fukuda, K.; Nakamura, S.; Miyake, Y.; Dohi, K.; Kogo, M. The Exploration of Population Pharmacokinetic Model for Meropenem in Augmented Renal Clearance and Investigation of Optimum Setting of Dose. J. Infect. Chemother. 2018, 24, 834–840. [Google Scholar] [CrossRef]
- Udy, A.A.; Lipman, J.; Jarrett, P.; Klein, K.; Wallis, S.C.; Patel, K.; Kirkpatrick, C.M.J.; Kruger, P.S.; Paterson, D.L.; Roberts, M.S.; et al. Are Standard Doses of Piperacillin Sufficient for Critically Ill Patients with Augmented Creatinine Clearance? Crit. Care 2015, 19, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukarnjanaset, W.; Jaruratanasirikul, S.; Wattanavijitkul, T. Population Pharmacokinetics and Pharmacodynamics of Piperacillin in Critically Ill Patients during the Early Phase of Sepsis. J. Pharmacokinet. Pharmacodyn. 2019, 46, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Masterton, R.; Drusano, G.; Paterson, D.L.; Park, G. Appropriate Antimicrobial Treatment in Nosocomial Infections—The Clinical Challenges. J. Hosp. Infect. 2003, 55, 1–12. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised Antibiotic Dosing for Patients Who Are Critically Ill: Challenges and Potential Solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Lopez, E.; Biran, V.; Durrmeyer, X.; Fakhoury, M.; Jacqz-Aigrain, E. Vancomycin Continuous Infusion in Neonates: Dosing Optimisation and Therapeutic Drug Monitoring. Arch. Dis. Child. 2013, 98, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Leroux, S.; Jacqz-Aigrain, E.; Biran, V.; Lopez, E.; Madeleneau, D.; Wallon, C.; Zana-Taïeb, E.; Virlouvet, A.L.; Rioualen, S.; Zhao, W. Clinical Utility and Safety of a Model-Based Patient-Tailored Dose of Vancomycin in Neonates. Antimicrob. Agents Chemother. 2016, 60, 2039–2042. [Google Scholar] [CrossRef] [Green Version]
- McCune, J.S.; Batchelder, A.; Guthrie, K.A.; Witherspoon, R.; Appelbaum, F.R.; Phillips, B.; Vicini, P.; Salinger, D.H.; McDonald, G.B. Personalized Dosing of Cyclophosphamide in the Total Body Irradiation-Cyclophosphamide Conditioning Regimen: A Phase II Trial in Patients with Hematologic Malignancy. Clin. Pharmacol. Ther. 2009, 85, 615–622. [Google Scholar] [CrossRef] [Green Version]
- Marsousi, N.; Samer, C.F.; Fontana, P.; Reny, J.L.; Rudaz, S.; Desmeules, J.A.; Daali, Y. Coadministration of Ticagrelor and Ritonavir: Toward Prospective Dose Adjustment to Maintain an Optimal Platelet Inhibition Using the PBPK Approach. Clin. Pharmacol. Ther. 2016, 100, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Weinelt, F.A.; Stegemann, M.S.; Theloe, A.; Pfäfflin, F.; Achterberg, S.; Schmitt, L.; Huisinga, W.; Michelet, R.; Hennig, S.; Kloft, C. Development of a model-informed dosing tool to optimise initial antibiotic dosing—A translational example for intensive care units. Pharmaceutics 2021, 13, 2128. [Google Scholar] [CrossRef]
- Liebchen, U.; Weinelt, F.; Scharf, C.; Schroeder, I.; Paal, M.; Zoller, M.; Kloft, C.; Jung, J.; Michelet, R. Combination of Pharmacokinetic and Pathogen Susceptibility Information to Optimize Meropenem Treatment of Gram- Negative Infections in Critically Ill Patients. Antimicrob. Agents Chemother. 2022, 66, e0183121. [Google Scholar] [CrossRef]
- Wicha, S.G.; Kees, M.G.; Solms, A.; Minichmayr, I.K.; Kratzer, A.; Kloft, C. TDMx: A novel web-based open-access support tool for optimising antimicrobial dosing regimens in clinical routine. Int. J. Antimicrob. Agents 2015, 45, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 33, 1159–1164. [Google Scholar] [CrossRef]
- Bassetti, M.; De Waele, J.J.; Eggimann, P.; Garnacho-Montero, J.; Kahlmeter, G.; Menichetti, F.; Nicolau, D.P.; Paiva, J.A.; Tumbarello, M.; Welte, T.; et al. Preventive and Therapeutic Strategies in Critically Ill Patients with Highly Resistant Bacteria. Intensive Care Med. 2015, 41, 776–795. [Google Scholar] [CrossRef] [PubMed]
- Eagye, K.J.; Banevicius, M.A.; Nicolau, D.P. Pseudomonas Aeruginosa Is Not Just in the Intensive Care Unit Any More: Implications for Empirical Therapy. Crit. Care Med. 2012, 40, 1329–1332. [Google Scholar] [CrossRef]
- Craig, W.A. The Pharmacology of Meropenem, A New Carbapenem Antibiotic. Clin. Infect. Dis. 1997, 24, S266–S275. [Google Scholar] [CrossRef] [Green Version]
- Colman, S.; Stove, V.; De Waele, J.J.; Verstraete, A.G. Measuring Unbound Versus Total Piperacillin Concentrations in Plasma of Critically Ill Patients: Methodological Issues and Relevance. Ther. Drug Monit. 2019, 41, 325–330. [Google Scholar] [CrossRef]
- Food and Drug Administration. Briefing Document Pharmaceutical Science and Clinical Pharmacology Advisory Committee Meeting. 2019. Available online: https://www.fda.gov/media/124495/download (accessed on 24 April 2022).


| Characteristic | Meropenem | Piperacillin/Tazobactam |
|---|---|---|
| Patient level | ||
| Categorical | n(%) | n(%) |
| Patients | 108 | 96.0 |
| Male | 70.0 (64.8) | 61.0 (63.5) |
| Continuous [unit] | Median (5th–95th percentile) | Median (5th–95th percentile) |
| Age (years) | 62.0 (36.0–80.0) | 65.0 (36.081.0) |
| Weight (kg) | 76.0 (49.0–126.0) | 76.0 (49.6–128.3) |
| Sample level | ||
| Categorical | n(%) | n(%) |
| Samples | 375 | 230 |
| 143 (38.1) | 53 (23.0) |
| 33 (8.80) | 12 (5.22) |
| Location of infection: | ||
| 166 (44.6) | 101 (43.9) |
| 131 (35.2) | 102 (44.3) |
| 60 (16.1) | 18 (7.83) |
| 15 (4.00) | 4 (1.74) |
| 0 (0) | 5 (2.17) |
| 3 (0.80) | 0 (0) |
| Continuous [unit] | Median (5th–95th percentile) | Median (5th–95th percentile) |
| Samples per patient | 2.00 (1.00–9.60) | 2.00 (1.00–5.20) |
| Creatinine clearance # (mL/min) | 76.6 (24.8–241) | 71.1 (17.8–171) |
| Serum albumin conc. (g/dL) | 2.68 (1.99–3.58) | 2.70 (2.00–3.50) |
| SOFA score | 8.00 (1.90–17.0) | 6.00 (1.00–14.0) |
| APACHE score | 23.0 (12.0–37.0) | 20.0 (11.0–34.0) |
| Meropenem n (%) | Piperacillin/Tazobactam n (%) | |
|---|---|---|
| Patients with determined MIC | 53 (49.1) | 33 (34.4) |
| Unique MIC determinations | 60 | 33 |
| MIC values (mg/L): | ||
| ≤0.25 | 45 (75.0 *) | 2 (6.06 *) |
| 0.5 | 2 (3.33 *) | - |
| 1 | 2 (3.33 *) | - |
| 2 | 2 (3.33 *) | - |
| 4 | 3 (5.00 *) | 24 (72.7 *) |
| 8 | 2 (3.33 *) | 5 (15.2 *) |
| 16 | 4 (6.67 *) | 1 (3.03 *) |
| 32 | - | 1 (3.03 *) |
| Samples | Dosing Adaptations, n (%) | |||
|---|---|---|---|---|
| All | Below Target Range | In Target Range | Above Target Range | |
| Meropenem | ||||
| Total | 22 (6.18 *) | 3 (6.12 *) | 7 (5.51 *) | 12 (6.67 *) |
| Dose reduction | 7 (31.8 #) | 0 (0 #) | 0 (0 #) | 7 (58.0 #) |
| Dose increase | 8 (36.4 #) | 3 (100 #) | 3 (43.0 #) | 2 (17.0 #) |
| Dosing interval reduction | 2 (9.09 #) | 0 (0 #) | 1 (14.0 #) | 1 (8.3 #) |
| Dosing interval increase | 2 (9.09 #) | 0 (0 #) | 1 (14.0 #) | 1 (8.3 #) |
| Infusion duration reduction | 2 (9.09 #) | 0 (0 #) | 1 (14.0 #) | 1 (8.3 #) |
| Infusion duration increase | 1 (4.54 #) | 0 (0 #) | 1 (14.0 #) | 0 (0 #) |
| Piperacillin | ||||
| Total | 10 (4.63 *) | 4 (12.5 *) | 0 (0 *) | 6 (8.00 *) |
| Dose reduction | 0 (0 #) | 0 (0 #) | 0 (0 #) | 0 (0 #) |
| Dose increase | 0 (0 #) | 0 (0 #) | 0 (0 #) | 0 (0 #) |
| Interval reduction | 4 (40.0 #) | 3 (75.0 #) | 0 (0 #) | 1 (17.0 #) |
| Interval increase | 5 (50.0 #) | 0 (0 #) | 0 (0 #) | 5 (83.0 #) |
| Infusion duration reduction | 1 (10.0 #) | 1 (25.0 #) | 0 (0 #) | 0 (0 #) |
| Infusion duration increase | 0 (0 #) | 0 (0 #) | 0 (0 #) | 0 (0 #) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinelt, F.A.; Stegemann, M.S.; Theloe, A.; Pfäfflin, F.; Achterberg, S.; Weber, F.; Dübel, L.; Mikolajewska, A.; Uhrig, A.; Kiessling, P.; et al. Evaluation of a Meropenem and Piperacillin Monitoring Program in Intensive Care Unit Patients Calls for the Regular Assessment of Empirical Targets and Easy-to-Use Dosing Decision Tools. Antibiotics 2022, 11, 758. https://doi.org/10.3390/antibiotics11060758
Weinelt FA, Stegemann MS, Theloe A, Pfäfflin F, Achterberg S, Weber F, Dübel L, Mikolajewska A, Uhrig A, Kiessling P, et al. Evaluation of a Meropenem and Piperacillin Monitoring Program in Intensive Care Unit Patients Calls for the Regular Assessment of Empirical Targets and Easy-to-Use Dosing Decision Tools. Antibiotics. 2022; 11(6):758. https://doi.org/10.3390/antibiotics11060758
Chicago/Turabian StyleWeinelt, Ferdinand Anton, Miriam Songa Stegemann, Anja Theloe, Frieder Pfäfflin, Stephan Achterberg, Franz Weber, Lucas Dübel, Agata Mikolajewska, Alexander Uhrig, Peggy Kiessling, and et al. 2022. "Evaluation of a Meropenem and Piperacillin Monitoring Program in Intensive Care Unit Patients Calls for the Regular Assessment of Empirical Targets and Easy-to-Use Dosing Decision Tools" Antibiotics 11, no. 6: 758. https://doi.org/10.3390/antibiotics11060758
APA StyleWeinelt, F. A., Stegemann, M. S., Theloe, A., Pfäfflin, F., Achterberg, S., Weber, F., Dübel, L., Mikolajewska, A., Uhrig, A., Kiessling, P., Huisinga, W., Michelet, R., Hennig, S., & Kloft, C. (2022). Evaluation of a Meropenem and Piperacillin Monitoring Program in Intensive Care Unit Patients Calls for the Regular Assessment of Empirical Targets and Easy-to-Use Dosing Decision Tools. Antibiotics, 11(6), 758. https://doi.org/10.3390/antibiotics11060758