
The Serum Concentration of Vancomycin as a Diagnostic Predictor of Nephrotoxic Acute Kidney Injury in Critically Ill Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lentini, P.; De Cal, M.; Clementi, A.; Angel, A.; Ronco, C. Sepsis and AKI in ICU patients: The Role of plasma biomarkers. Crit. Care Res. Pract. 2012, 2012, 856401. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Schrier, R.W.; Wang, W. Acute Renal Failure and Sepsis. N. Engl. J. Med. 2004, 351, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Zarjou, A.; Agarwal, A. Sepsis and Acute Kidney Injury. J. Am. Soc. Nephrol. 2011, 22, 999–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar] [CrossRef] [Green Version]
- Eyler, R.F.; Mueller, B. Antibiotic dosing in critically ill patients with acute kidney injury. Nat. Rev. Nephrol. 2011, 7, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.J.; Mueller, B.A. Antibiotic Dosing in Patients with Acute Kidney Injury. J. Intensiv. Care Med. 2014, 31, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Zamoner, W.; Freitas, F.M.; Garms, D.S.S.; Oliveira, M.G.; Balbi, A.L.; Ponce, D. Pharmacokinetics and pharmacodynamics of antibiotics in critically ill acute kidney injury patients. Pharmacol. Nothing Perspect. 2016, 4, e00280. [Google Scholar] [CrossRef] [Green Version]
- Hiramatsu, K. Vancomycin resistance in Staphylococci. Drug Resist. Updates 1998, 1, 135–150. [Google Scholar] [CrossRef]
- Rybak, M.J.; Lomaestro, B.M.; Rotschafer, J.C.; Moellering, R., Jr.; Craig, W.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Therapeutic monitoring of vancomycin in adults summary of consensus recommendations from the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Pharmacotherapy 2009, 29, 1275–1279. [Google Scholar] [CrossRef]
- Fisherman, M.; Lomaestro, B.; Rotschafer, J.C.; Moellering, R., Jr.; Craig, W.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am. J. Health-Syst. Pharm. 2009, 66, 82–98. [Google Scholar] [CrossRef]
- Alvarez, R.; López Cortés, L.E.; Molina, J.; Cisneros, J.M.; Pachón, J. Optimizing the clinical use of vancomycin. Antimicrob. Agents Chemother. 2016, 60, 2601–2609. [Google Scholar] [CrossRef] [Green Version]
- Iwamoto, T.; Kagawa, Y.; Kojima, M. Clinical Efficacy of Therapeutic Drug Monitoring in Patients Receiving Vancomycin. Biol. Pharm. Bull. 2003, 26, 876–879. [Google Scholar] [CrossRef] [Green Version]
- Davis, S.L.; Scheetz, M.H.; Bosso, J.A.; Goff, D.A.; Rybak, M.J. Adherence to the 2009 Consensus Guidelines for Vancomycin Dosing and Monitoring Practices: A Cross-Sectional Survey of U.S. Hospitals. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2013, 33, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Bosso, J.A.; Nappi, J.; Rudisill, C.; Wellein, M.; Bookstaver, P.B.; Swindler, J.; Mauldin, P.D. Relationship between vancomycin trough concentrations and nephrotoxicity: A prospective multicentertrial. Antimicrob. Agents Chemother. 2011, 55, 5475–5479. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.Y.; Yoshihara Dias, J.C.; Taguti, P.; Sacon, M.F.; Cup, I.A.M.; Carrilho, C.M.D.M.; Cardoso, L.T.Q.; Grion, C.M.C.; Matsuo, T. Acute renal injury in patients with severe sepsis: Prognostic factors. Sci. Med. 2012, 22, 138–141. [Google Scholar]
- Ponce, D.; Zorzenon, C.d.P.F.; Santos, N.Y.; Teixeira, U.A.; Balbi, A.L. Acute kidney injury in intensive care unit patients: A prospective study on incidence, risk factors and mortality. Rev. Bras. Ter. Intensiva 2011, 23, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Elyasi, S.; Khalili, H.; Dashti-Khavidaki, S.; Mohammadpour, A. Vancomycin-induced nephrotoxicity: Mechanism, incidence, risk factors and special populations. A literature review. Eur. J. Clin. Pharmacol. 2012, 68, 1243–1255. [Google Scholar] [CrossRef]
- Gupta, A.; Biyani, M.; Khaira, A. Vancomycin nephrotoxicity: Myths and facts. Neth. J. Med. 2011, 69, 379–383. [Google Scholar] [PubMed]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [Green Version]
- Liangos, O.; Wald, R.; O’ Bell, J.W.; Prince, L.; Pereira, B.J.; Jaber, B.l. Epidemiology and outcomes of acute renal failure in hospitalized patients: A national survey. Clin. J. Am. Soc. Nephrol. 2006, 1, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villacorta, H.; Masetto, A.C.; Mosque, E.T. C-Reactive Protein: An Inflammatory Marker with Prognostic Value in Patients with Decompensated Heart Failure. Arq. Bras. Cardiol. 2007, 88, 585–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am. J. Health Syst. Pharm. 2020, 19, 835–864. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | General | With AKI | Without AKI | p-Value |
|---|---|---|---|---|
| (N = 63) | (N = 28) | (N = 35) | ||
| Age (years) * | 54.6 ± 18.7 | 58.1 ± 17.2 | 51.9 ± 19.7 | 0.19 |
| Male | 42 (66.7) | 19 (67.8) | 23 (65.7) | 0.89 |
| Weight (kg) * | 72.6 ± 18.6 | 71.4 ± 17.05 | 73.5 ± 19.9 | 0.66 |
| GFR baseline—CKD-EPI (mL/min) * | 108.9 ± 28.9 | 98.4 ± 29.3 | 117.3 ± 26.1 | 0.009 |
| Urinary Output (mL/kg/h) * | 1.1 ± 0.5 | 1.08 ± 0.5 | 1.1 ± 0.5 | 0.50 |
| CPR (mg/dL) ** | 16.4 (11.2–25.9) | 16.2 (11.7–25.8) | 12.94 (6.4–23.6) | 0.13 |
| Mean arterial pressure * | 105.9 ± 11.9 | 78.7 ± 8.7 | 80.8 ± 9.3 | 0.37 |
| Albumin (g/dL) * | 2.25 ± 0.38 | 2.18 ± 0.3 | 2.32 ± 0.44 | 0.027 |
| SOFA | 8.5 ± 5.95 | 9.5 ± 5.54 | 7.0 ± 7.07 | 0.81 |
| Hospitalization days * | 36.1 ± 21.1 | 33.5 ± 20.5 | 30 ± 20.2 | 0.71 |
| Arterial hypertension (%) | 32 (50.8) | 14 (40) | 18 (51.4) | 0.88 |
| Diabetes Mellitus (%) | 18 (28.6) | 8 (28.5) | 10 (28.5) | 0.77 |
| Chronic kidney disease (%) | 3 (4.8) | 2 (7.1) | 1 (2.8) | 0.58 |
| Cardiovascular disease (%) | 7 (11.1) | 4 (14.2) | 3 (8.5) | 0.69 |
| Mechanical Ventilation (%) | 51 (81) | 25 (89.2) | 26 (74.2) | 0.24 |
| Vasoactive drug (%) | 35 (55.6) | 20 (71.4) | 15 (42.8) | 0.04 |
| Contrast (%) | 7 (11.1) | 3 (10.7) | 4 (11.4) | 1.00 |
| Diuretic (%) | 24 (38.1) | 15 (53.5) | 9 (25.7) | 0.04 |
| Other nephrotoxic drugs (%) # | 5 (7.9) | 3 (10.7) | 2 (5.7) | 0.65 |
| Diagnosis of hospitalization (%) | ||||
| Infection | 22 (34.9) | 12 (42.8) | 10 (28.5) | 0.36 |
| Cardiovascular | 4 (6.3) | 3 (10.7) | 1 (2.8) | 0.31 |
| Postoperative | 22 (34.9) | 7 (25) | 15 (42.8) | 0.22 |
| Other | 15 (23.8) | 6 (21.43) | 9 (25.7) | 0.92 |
| Death (%) | 29 (46) | 15 (53.5) | 14 (40) | 0.34 |
| Variables | General | With AKI | Without AKI | p-Value |
|---|---|---|---|---|
| (N = 63) | (N = 28) | (N = 35) | ||
| Vancomycin use time (days) ** | 11.4 (8.1–15.2) | 10 (7.5–15) | 9 (6–13.7) | 0.25 |
| Attack dose (mg/kg) * | 24.8 ± 5 | 24.42 ± 5.15 | 25.13 ± 4.93 | 0.58 |
| Vancomycin doses (First) (mg/kg) ** | 15.3 (12.9–19.4) | 15.2 (13.3–18.3) | 15.7 (14.6–19.2) | 0.21 |
| Number of doses adjustments ** | 1.8 (0–3) | 1 (0.5–3) | 2 (0–3) | 0.88 |
| Toxic serum level (%) | 34 (54) | 22 (78.5) | 15 (42.8) | 0.009 |
| Subtherapeutic level (%) | 32 (50.7) | 12 (42.8) | 30 (85.7) | <0.001 |
| Vancomycin T0-T2 (mg/L) * | 16.08 ± 8.3 | 17.4 ± 11.7 | 14.7 ± 5.5 | 0.73 |
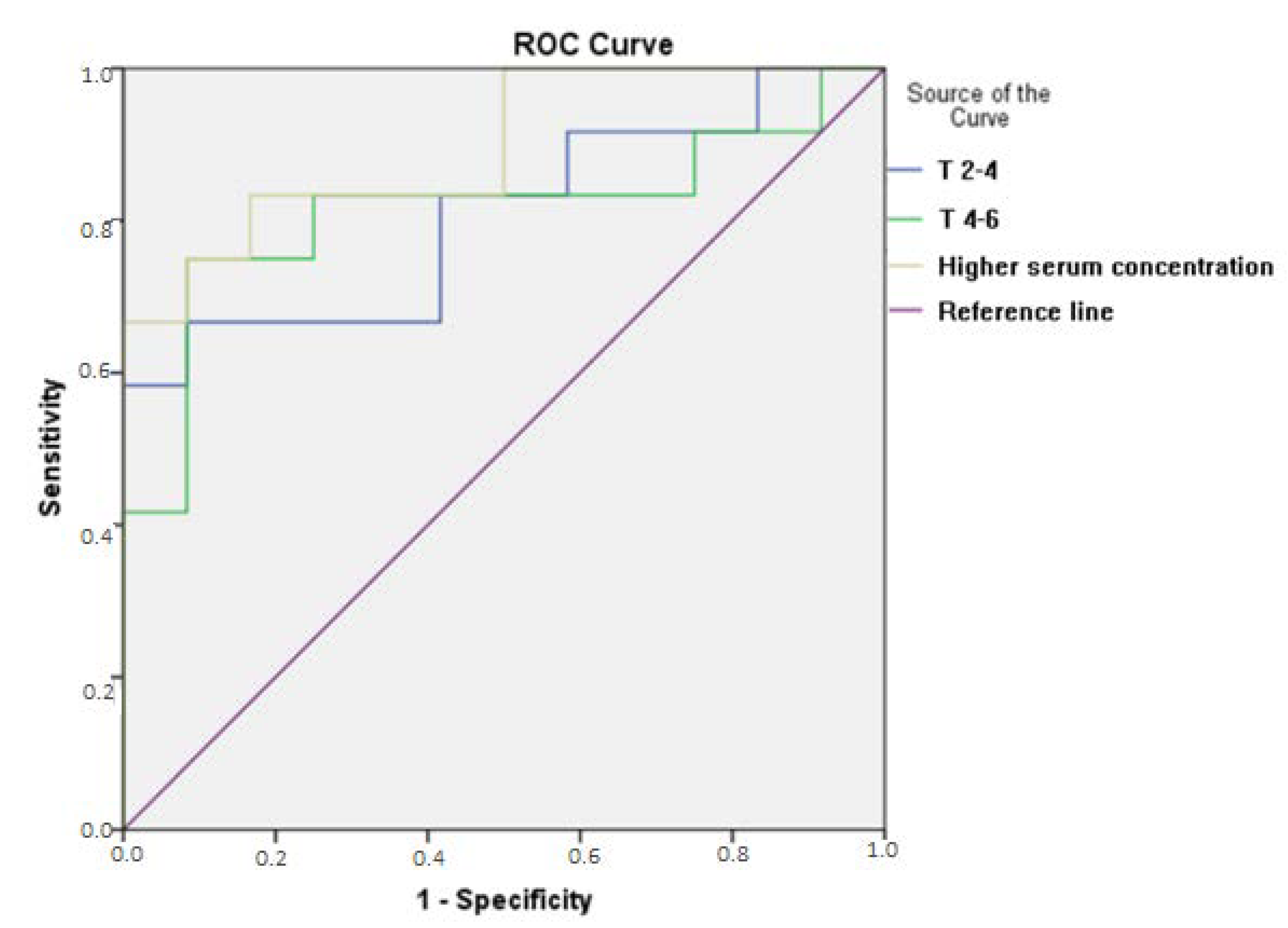
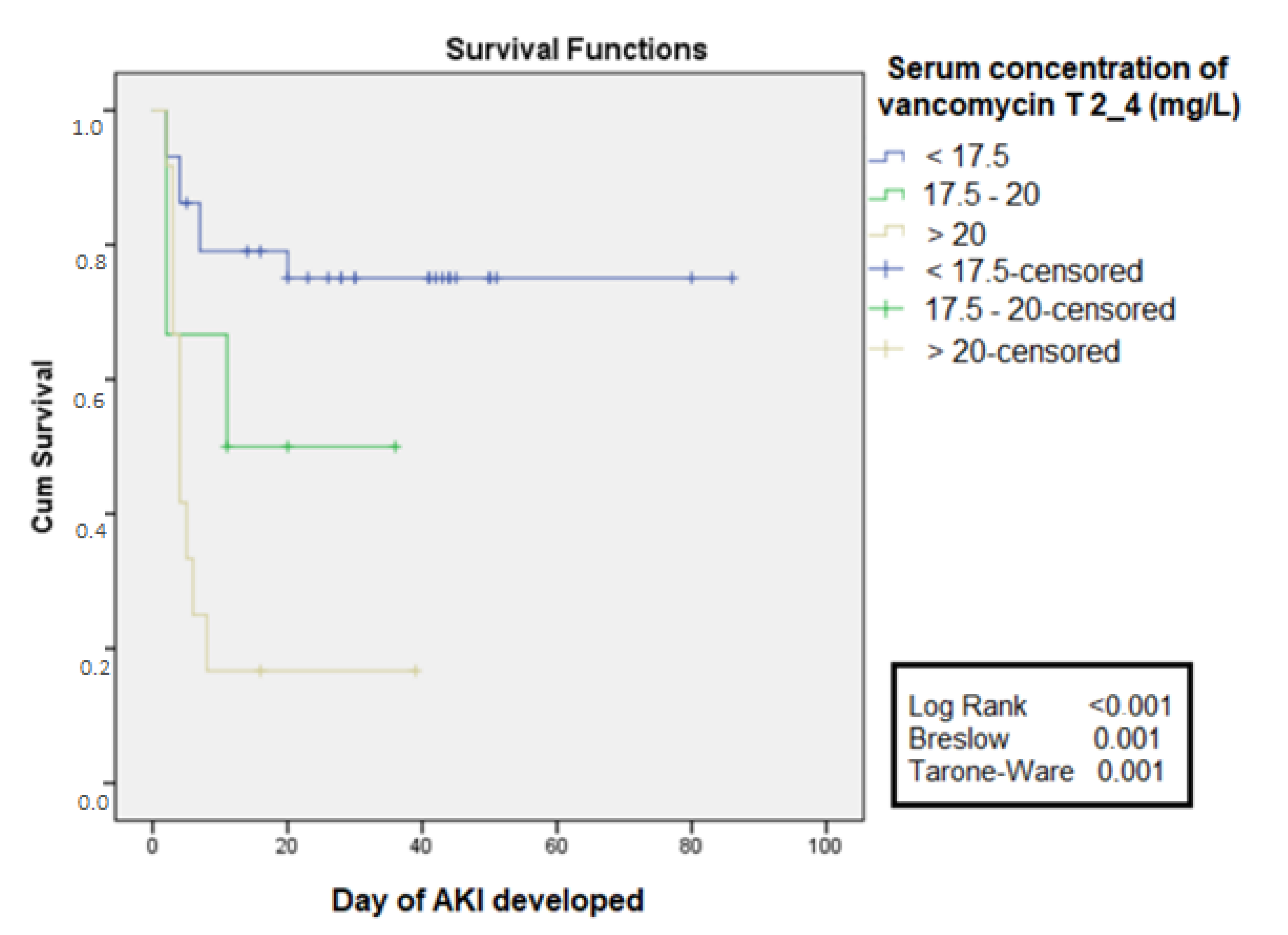
| Vancomycin T2-T4 (mg/L) ** | 19.1 (7.1–26.6) | 22.1 (9.1–29.6) | 9.1 (6.03–13.4) | 0.002 |
| Vancomycin T4-T6 (mg/L) * | 17.1 ± 8.9 | 20.4 ± 11.04 | 14.02 ± 5.08 | 0.051 |
| Variables | HR | Confidence Interval | p-Value |
|---|---|---|---|
| Albumin (g/dL) | 0.49 | 0.12–1.91 | 0.3 |
| Estimated GFR (mL/min) | 0.99 | 0.97–1.017 | 0.74 |
| Vasoactive drug | 0.59 | 0.16–2.2 | 0.43 |
| Diuretic use | 1.004 | 0.27–3.71 | 0.99 |
| Serum concentration T2-T4 (mg/L) | 1.086 | 1.02–1.15 | 0.009 |
| Variables | General | Death | No Death | p-Value |
|---|---|---|---|---|
| (N = 63) | (N = 29) | (N = 34) | ||
| Age (years) * | 54.6 ± 18.7 | 64.5 ± 17.04 | 46.2 ± 15.9 | 0.0001 |
| Male sex (%) | 42 (66.7) | 19 (65.5) | 23 (67.6) | 1 |
| Weight (kg) * | 72.6 ± 18.6 | 69.1 ± 15.5 | 75.5 ± 20.6 | 0.17 |
| GFR baseline—CKD-EPI (mL/min) * | 108.9 ± 28.9 | 96.08 ± 31.7 | 119.9 ± 21.3 | 0.001 |
| Diuresis mL/kg/h * | 1.1 ± 0.5 | 1.04 ± 0.5 | 1.2 ± 0.5 | 0.17 |
| CPR (mg/dL) * | 16.4 ± 9.8 | 20.6 ± 10.8 | 12.8 ± 7.3 | 0.002 |
| Mean arterial pressure (mmHg) * | 105.9 ± 11.9 | 103.6 ± 12.3 | 107.8 ± 11.4 | 0.16 |
| Albumin (g/dL) * | 2.25 ± 0.38 | 2.19 ± 0.32 | 2.31 ± 0.43 | 0.19 |
| SOFA | 8.5 ± 5.95 | 8.88 ± 6.68 | 7.0 ± 0.00 | 0.008 |
| Hospitalization days * | 36.1 ± 21.1 | 30.28 ± 23.6 | 41.09 ± 17.6 | 0.04 |
| Arterial hypertension (%) | 32 (50.8) | 17 (58.6) | 15 (44.1) | 0.37 |
| Diabetes mellitus (%) | 18 (28.6) | 9 (31) | 9 (26.5) | 0.90 |
| Chronic kidney disease (%) | 3 (4.8) | 3 (10.3) | 0 (0) | 0.18 |
| Cardiovascular disease (%) | 7 (11.1) | 4 (13.8) | 3 (8.8) | 0.82 |
| Mechanical ventilation (%) | 51 (81) | 24 (82.8) | 27 (79.4) | 0.98 |
| Vasoactive drug (%) | 35 (55.6) | 17 (58.6) | 18 (52.9) | 0.84 |
| Contrast (%) | 7 (11.1) | 4 (13.8) | 3 (8.8) | 0.82 |
| Diuretic use (%) | 24 (38.1) | 16 (55.2) | 8 (23.5) | 0.02 |
| Other nephrotoxic drugs (%)# | 5 (7.9) | 1 (3.4) | 4 (11.8) | 0.45 |
| Hospitalization Diagnosis: | ||||
| Infection (%) | 22 (34.9) | 13 (44.8) | 9 (26.4) | 0.21 |
| Cardiovascular (%) | 4 (6.3) | 3 (10.3) | 1 (2.9) | 0.32 |
| Infection Focus (%) | ||||
| Urinary + bloodstream | 4 (13.79) | 4 (13.79) | 0 (0) | 0.04 |
| Pulmonary | 32 (50.8) | 12 (41.38) | 21 (61.76) | 0.17 |
| AKI (%) | 28 (44.4) | 15 (51.7) | 13 (38.12) | 0.34 |
| KDIGO (%) | ||||
| 1 | 5 (17.8) | 3 (20) | 2 (15) | 0.99 |
| 2 | 10 (35.7) | 6 (40) | 4 (30) | 0.76 |
| 3 | 13 (46.4) | 6 (40) | 7 (53) | 0.72 |
| Variables | General | Death | No Death | p-Value |
|---|---|---|---|---|
| (N = 63) | (N = 29) | (N = 34) | ||
| Vancomycin use time (days) * | 11.4 ± 7.3 | 9.4 ± 5.9 | 13.1 ± 8.05 | 0.04 |
| Attack dose mg/kg * | 24.8 ± 5 | 24.9 ± 4.4 | 24.7 ± 5.5 | 0.33 |
| Vancomycin dose (First) mg/kg * | 15.3 ± 3.5 | 14.8 ± 2.6 | 18.1 ± 4.1 | 0.90 |
| Number of doses adjustments ** | 1.84 (1.8) | 1.07 (1.2) | 2.50 (2.07) | 0.002 |
| Toxic serum level (%) | 34 (54) | 16 (55.2) | 18 (52.9) | 1.00 |
| Subtherapeutic level (%) | 39 (61.9) | 14 (48.3) | 25 (73.5) | 0.07 |
| Vancomycin T0-T2 (mg/L) * | 16.08 ± 8.3 | 17.91 ± 11.02 | 14.2 ± 6.5 | 0.65 |
| Vancomycin T2-T4 (mg/L) * | 17.6 ± 9.5 | 20.0 ± 9.76 | 11.3 ± 7.81 | 0.02 |
| Vancocycin T4-T6 (mg/L) * | 17.1 ±8.9 | 20 ± 9.07 | 14.08 ± 8.05 | 0.07 |
| Variables | HR | Confidence Interval | p-Value |
|---|---|---|---|
| Age (years) | 1.13 | 1.02–1.26 | 0.018 |
| Estimated GFR (mL/min) | 1.23 | 1.04–1.45 | 0.015 |
| Number of doses adjustments | 3.21 | 0.94–10.9 | 0.06 |
| Vasoactive drug | 30.68 | 0.37–2502.8 | 0.127 |
| Vancomycin T2-T4 (mg/L) | 1.60 | 1.07–2.4 | 0.021 |
| Diuretic use | 0.153 | 0.005–4.25 | 0.26 |
| CPR (mg/dL) | 1.26 | 1.05–1.51 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamoner, W.; Eid, K.Z.C.; de Almeida, L.M.B.; Pierri, I.G.; Santos, A.d.; Balbi, A.L.; Ponce, D. The Serum Concentration of Vancomycin as a Diagnostic Predictor of Nephrotoxic Acute Kidney Injury in Critically Ill Patients. Antibiotics 2022, 11, 112. https://doi.org/10.3390/antibiotics11010112
Zamoner W, Eid KZC, de Almeida LMB, Pierri IG, Santos Ad, Balbi AL, Ponce D. The Serum Concentration of Vancomycin as a Diagnostic Predictor of Nephrotoxic Acute Kidney Injury in Critically Ill Patients. Antibiotics. 2022; 11(1):112. https://doi.org/10.3390/antibiotics11010112
Chicago/Turabian StyleZamoner, Welder, Karina Zanchetta Cardoso Eid, Lais Maria Bellaver de Almeida, Isabella Gonçalves Pierri, Adriano dos Santos, André Luis Balbi, and Daniela Ponce. 2022. "The Serum Concentration of Vancomycin as a Diagnostic Predictor of Nephrotoxic Acute Kidney Injury in Critically Ill Patients" Antibiotics 11, no. 1: 112. https://doi.org/10.3390/antibiotics11010112
APA StyleZamoner, W., Eid, K. Z. C., de Almeida, L. M. B., Pierri, I. G., Santos, A. d., Balbi, A. L., & Ponce, D. (2022). The Serum Concentration of Vancomycin as a Diagnostic Predictor of Nephrotoxic Acute Kidney Injury in Critically Ill Patients. Antibiotics, 11(1), 112. https://doi.org/10.3390/antibiotics11010112