
Mortality in Thai Nursing Homes Based on Antimicrobial-Resistant Enterobacterales Carriage and COVID-19 Lockdown Timing: A Prospective Cohort Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Characteristics and Factors Associated EC Carriage
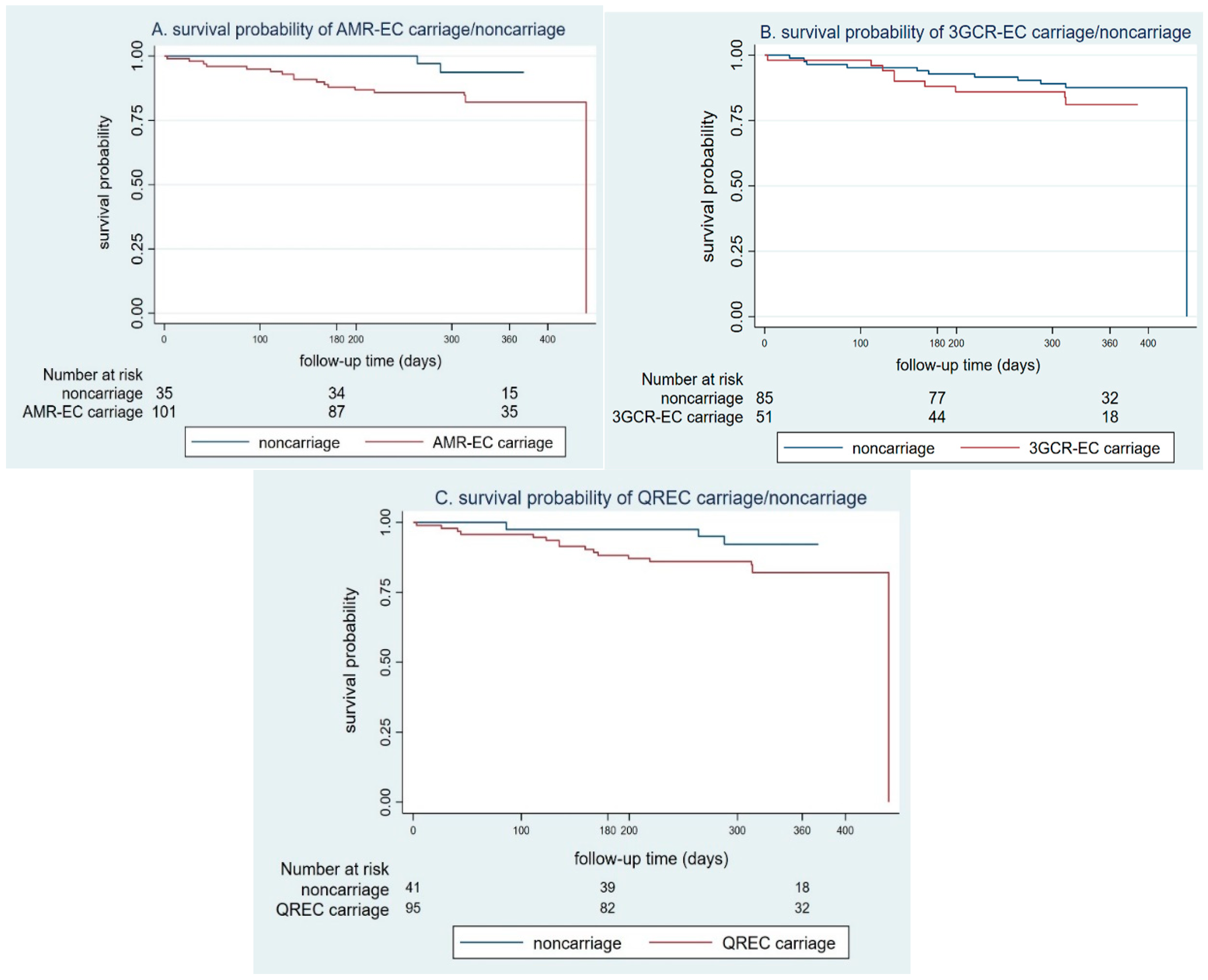
2.2. Mortality Rate of EC Carriage
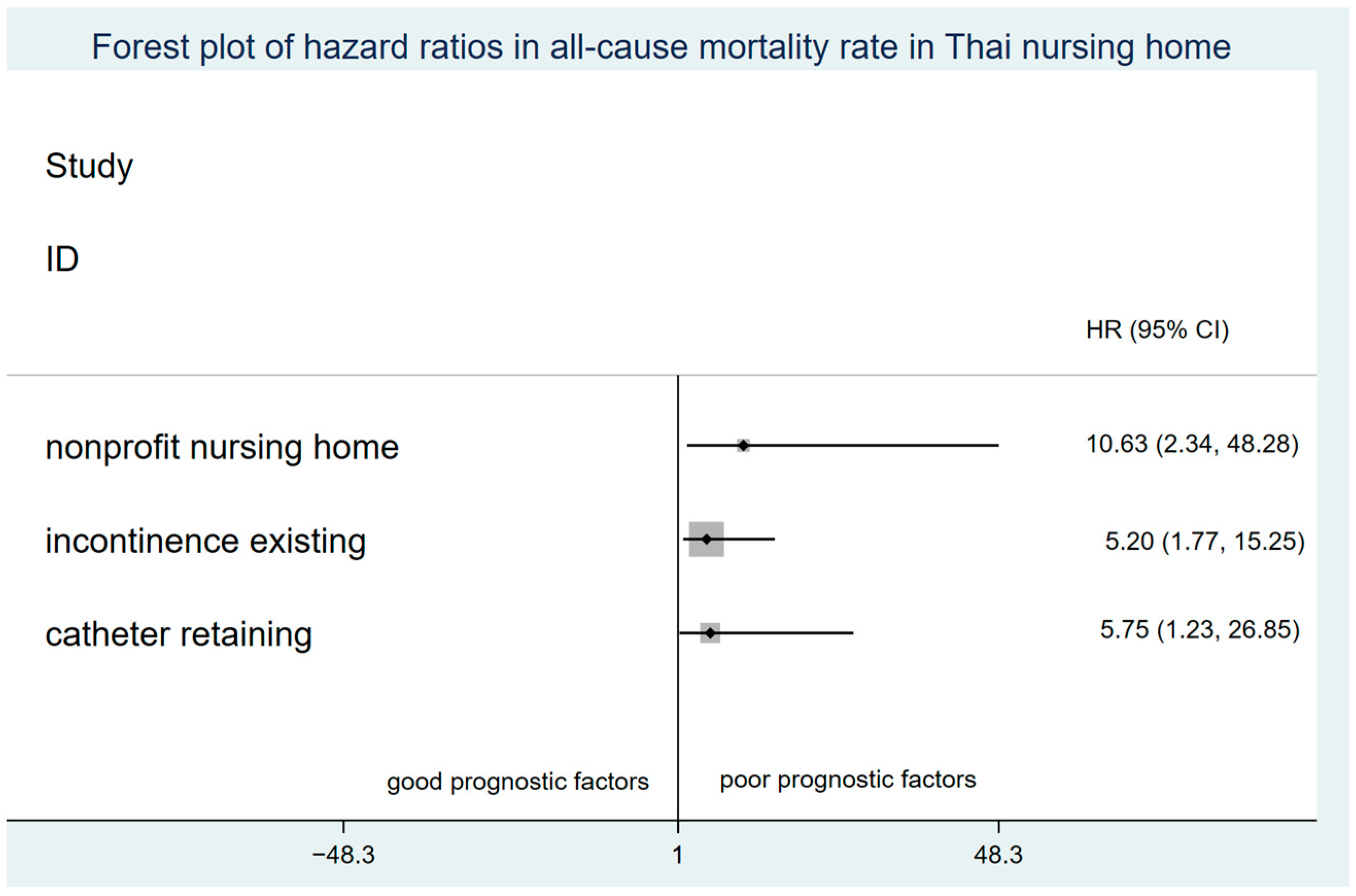
2.3. Associated Factors and Incidence Mortality Rate among Residents
3. Discussion
4. Materials and Methods
4.1. Study Design and Setting
4.2. Study Populations
4.3. Study Procedure and Data Collection
4.3.1. Rectal Sampling and Microbiological Outcome Measurement
4.3.2. Study Endpoints
4.3.3. Study Variables Definition
4.4. Statistical Method
4.4.1. Sample Size Calculation
4.4.2. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aschbacher, R.; Pagani, E.; Confalonieri, M.; Farina, C.; Fazii, P.; Luzzaro, F.; Montanera, P.G.; Piazza, A.; Pagani, L. Review on colonization of residents and staff in Italian long-term care facilities by multidrug-resistant bacteria compared with other European countries. Antimicrob. Resist. Infect. Control 2016, 5, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Dool, C.; Haenen, A.; Leenstra, T.; Wallinga, J. The Role of Nursing Homes in the Spread of Antimicrobial Resistance over the Healthcare Network. Infect. Control Hosp. Epidemiol. 2016, 37, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruscher, C.; Pfeifer, Y.; Layer, F.; Schaumann, R.; Levin, K.; Mielke, M. Inguinal skin colonization with multidrug-resistant bacteria among residents of elderly care facilities: Frequency, persistence, molecular analysis and clinical impact. Int. J. Med Microbiol. 2014, 304, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- March, A.; Aschbacher, R.; Dhanji, H.; Livermore, D.M.; Böttcher, A.; Sleghel, F.; Maggi, S.; Noale, M.; Larcher, C.; Woodford, N. Colonization of residents and staff of a long-term-care facility and adjacent acute-care hospital geriatric unit by multiresistant bacteria. Clin. Microbiol. Infect. 2010, 16, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Rooney, P.J.; O’Leary, M.C.; Loughrey, A.C.; McCalmont, M.; Smyth, B.; Donaghy, P.; Badri, M.; Woodford, N.; Karisik, E.; Livermore, D.M. Nursing homes as a reservoir of extended-spectrumβ-lactamase (ESBL)-producing ciprofloxacin-resistant Escherichia coli. J. Antimicrob. Chemother. 2009, 64, 635–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochard, H.; Aubier, B.; Quentin, R.; van der Mee-Marquet, N.; du Centre, R.D.H. Extended-Spectrumβ-Lactamase–Producing Enterobacteriaceae in French Nursing Homes: An Association between High Carriage Rate among Residents, Environmental Contamination, Poor Conformity with Good Hygiene Practice, and Putative Resident-to-Resident Transmission. Infect. Control Hosp. Epidemiol. 2014, 35, 384–389. [Google Scholar] [CrossRef]
- Reddy, P.; Malczynski, M.; Obias, A.; Reiner, S.; Jin, N.; Huang, J.; Noskin, G.A.; Zembower, T. Screening for Extended-Spectrum -Lactamase-Producing Enterobacteriaceae among High-Risk Patients and Rates of Subsequent Bacteremia. Clin. Infect. Dis. 2007, 45, 846–852. [Google Scholar] [CrossRef]
- Leitner, E.; Zechner, E.; Ullrich, E.; Zarfel, G.; Luxner, J.; Pux, C.; Pichler, G.; Schippinger, W.; Krause, R.; Zollner-Schwetz, I. Low prevalence of colonization with multidrug-resistant gram-negative bacteria in long-term care facilities in Graz, Austria. Am. J. Infect. Control 2018, 46, 76–80. [Google Scholar] [CrossRef]
- Nicolle, L.E. Infection Control in Long-Term Care Facilities. Clin. Infect. Dis. 2000, 31, 752–756. [Google Scholar] [CrossRef]
- Baker, N.R.; Dunn, D.; Greenberg, S.A.; Shaughnessy, M. Infection Control in Long-Term Care: An Old Problem and New Priority. J. Am. Med. Dir. Assoc. 2021, 23, 321–322. [Google Scholar] [CrossRef]
- Peae, P. Situation of the Thai Elderly 2019; Mahidol University and Foundation of Thai Gerontology Research and Development Institute (TGRI), Institute for Population and Social Research: Nakhon Pathom, Thailand, 2020. [Google Scholar]
- Lloyd-Sherlock, P.G.; Sasat, S.; Sanee, A.; Miyoshi, Y.; Lee, S. The rapid expansion of residential long-term care services in Bangkok: A challenge for regulation. J. Public Health Dev. 2021, 19, 89–101. Available online: https://he01.tci-thaijo.org/index.php/AIHD-MU/article/view/246485 (accessed on 20 March 2022).
- Sasat, S.; Choowattanapakorn, T.; Pukdeeprom, T.; Lertrat, P.; Aroonsang, P. Long-Term Care Institutions in Thailand. J. Health Res. 2017, 27, 413–418. Available online: https://he01.tci-thaijo.org/index.php/jhealthres/article/view/88736 (accessed on 20 March 2022).
- Niumsup, P.R.; Tansawai, U.; Na-Udom, A.; Jantapalaboon, D.; Assawatheptawee, K.; Kiddee, A.; Romgaew, T.; Lamlertthon, S.; Walsh, T.R. Prevalence and risk factors for intestinal carriage of CTX-M-type ESBLs in Enterobacteriaceae from a Thai community. Eur. J. Clin. Microbiol. 2017, 37, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Hirai, I.; Niki, M.; Nakamura, T.; Komalamisra, C.; Maipanich, W.; Kusolsuk, T.; Sa-Nguankiat, S.; Pubampen, S.; Yamamoto, Y. High prevalence of CTX-M -lactamase-producing Enterobacteriaceae in stool specimens obtained from healthy individuals in Thailand. J. Antimicrob. Chemother. 2010, 65, 666–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thamlikitkul, V.; Tangkoskul, T.; Seenama, C. Fecal Carriage Rate of Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae as a Proxy Composite Indicator of Antimicrobial Resistance in a Community in Thailand. Open Forum Infect. Dis. 2019, 6, ofz425. [Google Scholar] [CrossRef]
- Hjaltadóttir, I.; Hallberg, I.R.; Ekwall, A.K.; Nyberg, P. Predicting mortality of residents at admission to nursing home: A longitudinal cohort study. BMC Health Serv. Res. 2011, 11, 86. [Google Scholar] [CrossRef] [Green Version]
- Saka, B.; Ozkaya, H.; Karisik, E.; Akin, S.; Akpinar, T.; Tufan, F.; Bahat, G.; Dogan, H.; Horasan, Z.; Cesur, K.; et al. Malnutrition and sarcopenia are associated with increased mortality rate in nursing home residents: A prospective study. Eur. Geriatr. Med. 2016, 7, 232–238. [Google Scholar] [CrossRef]
- Vossius, C.; Selbæk, G.; Benth, J.; Bergh, S. Mortality in nursing home residents: A longitudinal study over three years. PLoS ONE 2018, 13, e0203480. [Google Scholar] [CrossRef] [Green Version]
- Schoevaerdts, D.; Agelas, J.-P.; Ingels, M.-G.; Jamart, J.; Frennet, M.; Huang, T.-D.; Swine, C.; Glupczynski, Y. Health outcomes of older patients colonized by multi-drug resistant bacteria (MDRB): A one-year follow-up study. Arch. Gerontol. Geriatr. 2013, 56, 231–236. [Google Scholar] [CrossRef]
- Igbinosa, O.; Dogho, P.; Osadiaye, N. Carbapenem-resistant Enterobacteriaceae: A retrospective review of treatment and outcomes in a long-term acute care hospital. Am. J. Infect. Control 2019, 48, 7–12. [Google Scholar] [CrossRef]
- Aliyu, S.; McGowan, K.; Hussain, D.; Kanawati, L.; Ruiz, M.; Yohannes, S. Prevalence and Outcomes of Multi-Drug Resistant Blood Stream Infections among Nursing Home Residents Admitted to an Acute Care Hospital. J. Intensiv. Care Med. 2021, 37, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, D.C.; Mor, V. Nursing Home Care in Crisis in the Wake of COVID-19. JAMA 2020, 324, 23. [Google Scholar] [CrossRef]
- Choi, J.-P.; Cho, E.H.; Lee, S.J.; Koo, M.S.; Song, Y.G. Influx of multidrug resistant, Gram-negative bacteria (MDRGNB) in a public hospital among elderly patients from long-term care facilities: A single-center pilot study. Arch. Gerontol. Geriatr. 2012, 54, e19–e22. [Google Scholar] [CrossRef] [PubMed]
- Ramphal, R.; Ambrose, P.G. Extended-Spectrum β-Lactamases and Clinical Outcomes: Current Data. Clin. Infect. Dis. 2006, 42, S164–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Östholmbalkhed, Å.; Tärnberg, M.; Nilsson, M.; Nilsson, L.E.; Hanberger, H.; Hällgren, A.; for the Southeast Sweden Travel Study Group. Duration of travel-associated faecal colonisation with ESBL-producing Enterobacteriaceae—A one year follow-up study. PLoS ONE 2018, 13, e0205504. [Google Scholar] [CrossRef]
- Latour, K.; Huang, T.-D.; Jans, B.; Berhin, C.; Bogaerts, P.; Noel, A.; Nonhoff, C.; Dodémont, M.; Denis, O.; Ieven, M.; et al. Prevalence of multidrug-resistant organisms in nursing homes in Belgium in 2015. PLoS ONE 2019, 14, e0214327. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-M.; Lai, C.-C.; Chiang, H.-T.; Lu, M.-C.; Wang, L.-F.; Tsai, T.-L.; Kang, M.-Y.; Jan, Y.-N.; Lo, Y.-T.; Ko, W.-C.; et al. Presence of multidrug-resistant organisms in the residents and environments of long-term care facilities in Taiwan. J. Microbiol. Immunol. Infect. 2017, 50, 133–144. [Google Scholar] [CrossRef]
- Hollander, J.E.; Carr, B.G. Virtually Perfect? Telemedicine for COVID-19. N. Engl. J. Med. 2020, 382, 1679–1681. [Google Scholar] [CrossRef]
- Williams, C.S.; Zheng, Q.; White, A.J.; Bengtsson, A.I.; Shulman, E.T.; Herzer, K.R.; Fleisher, L.A. The association of nursing home quality ratings and spread of COVID-19. J. Am. Geriatr. Soc. 2021, 69, 2070–2078. [Google Scholar] [CrossRef]
- Li, Y.; Temkin-Greener, H.; Shan, G.; Cai, X. COVID-19 Infections and Deaths among Connecticut Nursing Home Residents: Facility Correlates. J. Am. Geriatr. Soc. 2020, 68, 1899–1906. [Google Scholar] [CrossRef]
- He, M.; Li, Y.; Fang, F. Is There a Link between Nursing Home Reported Quality and COVID-19 Cases? Evidence from California Skilled Nursing Facilities. J. Am. Med. Dir. Assoc. 2020, 21, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Ming, D.; Ahmad, R.; Moore, L.S.P.; Holmes, A.H. Antimicrobial use, drug-resistant infections and COVID-19. Nat. Rev. Microbiol. 2020, 18, 409–410. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.; Romano, J.; Chmelnitsky, I.; Navon-Venezia, S.; Edgar, R.; Carmeli, Y. Rectal Swabs Are Suitable for Quantifying the Carriage Load of KPC-Producing Carbapenem-Resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2013, 57, 1474–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suñer, C.; Ouchi, D.; Mas, M.; Alarcon, R.L.; Mesquida, M.M.; Prat, N.; Bonet-Simó, J.M.; Izquierdo, M.E.; Sánchez, I.G.; Noguerola, S.R.; et al. A retrospective cohort study of risk factors for mortality among nursing homes exposed to COVID-19 in Spain. Nat. Aging 2021, 1, 579–584. [Google Scholar] [CrossRef]
- Panagiotou, O.A.; Kosar, C.M.; White, E.M.; Bantis, L.E.; Yang, X.; Santostefano, C.M.; Feifer, R.A.; Blackman, C.; Rudolph, J.L.; Gravenstein, S.; et al. Risk Factors Associated with All-Cause 30-Day Mortality in Nursing Home Residents with COVID-19. JAMA Intern. Med. 2021, 181, 439. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Residents N = 142, N. (%) | Enterobacterales Carriage * (N = 136) | ||
|---|---|---|---|---|
| Antimicrobial-Resistant Carriage (N = 101; 74.3%), No. (%) | No Antimicrobial-Resistant Carriage (N = 35; 25.8%) No. (%) | p Value | ||
| Sex Male Female | 57 (40.1) 85 (59.9) | 37 (36.6) 64 (63.4) | 19 (54.3) 16 (45.7) | 0.067 |
| Age, year <80 ≥80 | 67 (47.2) 75 (52.8) | 49 (48.5) 52 (51.5) | 14 (40.0) 21 (60.0) | 0.384 |
| Comorbidities None Single Multiple | 5 (3.5) 33 (23.2) 104 (73.2) | 1 (1) 26 (25.7) 74 (73.3) | 4 (11.4) 6 (17.1) 25 (71.4) | 0.014 + |
| Duration of living, year <1 ≥1 | 46 (32.4) 96 (67.6) | 33 (32.7) 68 (67.3) | 11 (31.4) 24 (68.6) | 0.892 |
| Types of nursing home Nonprofit Profit | 73 (51.4) 69 (48.6) | 56 (55.5) 45 (44.6) | 15 (42.9) 20 (57.1) | 0.199 |
| Activities of Daily Living (ADLs) Dependence Partial dependence Independence | 53 (37.6) 76 (53.9) 12 (8.5) | 39 (39.0) 56 (56.0) 5 (5.0) | 12 (34.3) 17 (48.6) 6 (17.1) | 0.078 |
| Incontinence or pressure ulcer existing Yes No | 62 (43.7) 80 (56.3) | 51 (50.5) 50 (49.5) | 8 (22.9) 27 (77.1) | 0.016 + |
| Catheter or foreign material retaining Yes No | 59 (41.6) 83 (58.5) | 48 (47.6) 53 (52.5) | 7 (20.0) 28 (80.0) | 0.016+ |
| Recent antimicrobial agents use Yes No | 50 (38.2) 81 (61.8) | 39 (41.1) 56 (59.0) | 8 (26.7) 22 (73.3) | 0.156 |
| Need regular follow-up Yes No | 60 (72.2) 23 (27.7) | 41 (68.3) 18 (30.0) | 14 (70.0) 4 (20.0) | 0.189 |
| Recent in hospital admission Yes No | 41 (49.3) 42 (50.6) | 28 (46.7) 31 (51.7) | 9 (45.0) 11 (55.0) | 0.829 |
| Recent ICU admission Yes No | 8 (22.2) 28 (77.8) | 6 (25.0) 18 (75.0) | 1 (11.1) 8 (88.9) | 0.385 |
| Characteristics | Quinolone-Resistant EC * Carriage | Third-Generation Cephalosporin-Resistant EC ** Carriage | Antimicrobial Resistant EC *** Carriage | |||
|---|---|---|---|---|---|---|
| Crude OR (95% CI) | Adjusted OR (95%CI) | Crude OR (95% CI) | Adjusted (OR 95% CI) | Crude OR (95% CI) | Adjusted OR (95%CI) | |
| Comorbidities None Single Multiple | - 1 12 (1.16,123.68) | - 1 17.33 (1.63,184.36) | ||||
| Duration of living, year <1 ≥1 | 1 0.46 (0.22,0.96) | |||||
| Activities of Daily Living (ADLs) Dependence Partial dependence Independence | 4.63 (1.17,18.27) 4.64 (1.22, 17.57) 1 | 0.96 (0.19,4.91) 3.52 (0.92,13.45) 1 | ||||
| Incontinence or pressure ulcer existing Yes No | 3.95 (1.70, 9.17) 1 | 3.44 (1.43, 8.30) 1 | 2.15 (0.75, 6.18) 1 | |||
| Catheter or foreign material retaining Yes No | 4.96 (2.00, 12.29) 1 | 9.52 (2.74,33.11) 1 | 3.62 (1.45, 9.05) 1 | 2.30 (0.77, 6.90) 1 | ||
| Recent antimicrobial agents use Yes No | 2.437 (1.00, 5.96) 1 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngamprasertchai, T.; Vanaporn, M.; Muangnoicharoen, S.; Pan-ngum, W.; Ruenroengbun, N.; Piroonamornpun, P.; Ponam, T.; Duangdee, C.; Chankete, P.; Jitmuang, A.; et al. Mortality in Thai Nursing Homes Based on Antimicrobial-Resistant Enterobacterales Carriage and COVID-19 Lockdown Timing: A Prospective Cohort Study. Antibiotics 2022, 11, 762. https://doi.org/10.3390/antibiotics11060762
Ngamprasertchai T, Vanaporn M, Muangnoicharoen S, Pan-ngum W, Ruenroengbun N, Piroonamornpun P, Ponam T, Duangdee C, Chankete P, Jitmuang A, et al. Mortality in Thai Nursing Homes Based on Antimicrobial-Resistant Enterobacterales Carriage and COVID-19 Lockdown Timing: A Prospective Cohort Study. Antibiotics. 2022; 11(6):762. https://doi.org/10.3390/antibiotics11060762
Chicago/Turabian StyleNgamprasertchai, Thundon, Muthita Vanaporn, Sant Muangnoicharoen, Wirichada Pan-ngum, Narisa Ruenroengbun, Pittaya Piroonamornpun, Thitiya Ponam, Chatnapa Duangdee, Phanita Chankete, Anupop Jitmuang, and et al. 2022. "Mortality in Thai Nursing Homes Based on Antimicrobial-Resistant Enterobacterales Carriage and COVID-19 Lockdown Timing: A Prospective Cohort Study" Antibiotics 11, no. 6: 762. https://doi.org/10.3390/antibiotics11060762
APA StyleNgamprasertchai, T., Vanaporn, M., Muangnoicharoen, S., Pan-ngum, W., Ruenroengbun, N., Piroonamornpun, P., Ponam, T., Duangdee, C., Chankete, P., Jitmuang, A., & Thamlikitkul, V. (2022). Mortality in Thai Nursing Homes Based on Antimicrobial-Resistant Enterobacterales Carriage and COVID-19 Lockdown Timing: A Prospective Cohort Study. Antibiotics, 11(6), 762. https://doi.org/10.3390/antibiotics11060762