
Antimicrobial Stewardship Strategies Including Point-of-Care Testing (POCT) for Pediatric Patients with Upper-Respiratory-Tract Infections in Primary Care: A Systematic Review of Economic Evaluations

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Registration
2.2. Search Strategy
2.3. Eligibility Criteria
- Only studies in English published after the year 2000 were included. No geographical restrictions were applied.
- Abstracts/unpublished articles were included if relevant; journal articles, commentaries, editorials, letters, (systematic) reviews, and conference abstracts were included if they reported extractable data; conference abstracts/unpublished articles or articles for which full texts were not available were excluded.
- Studies were included if a POCT was employed for diagnostic purposes, excluding the use for screenings and monitoring. Studies conducted only on adult populations were excluded. Studies without any type of economic evaluation did not meet the “cost-effectiveness and costing” eligibility criteria and were excluded from the analysis.
2.4. Study Selection
2.5. Methodological Assessment
2.6. Data Extraction and Management
3. Results
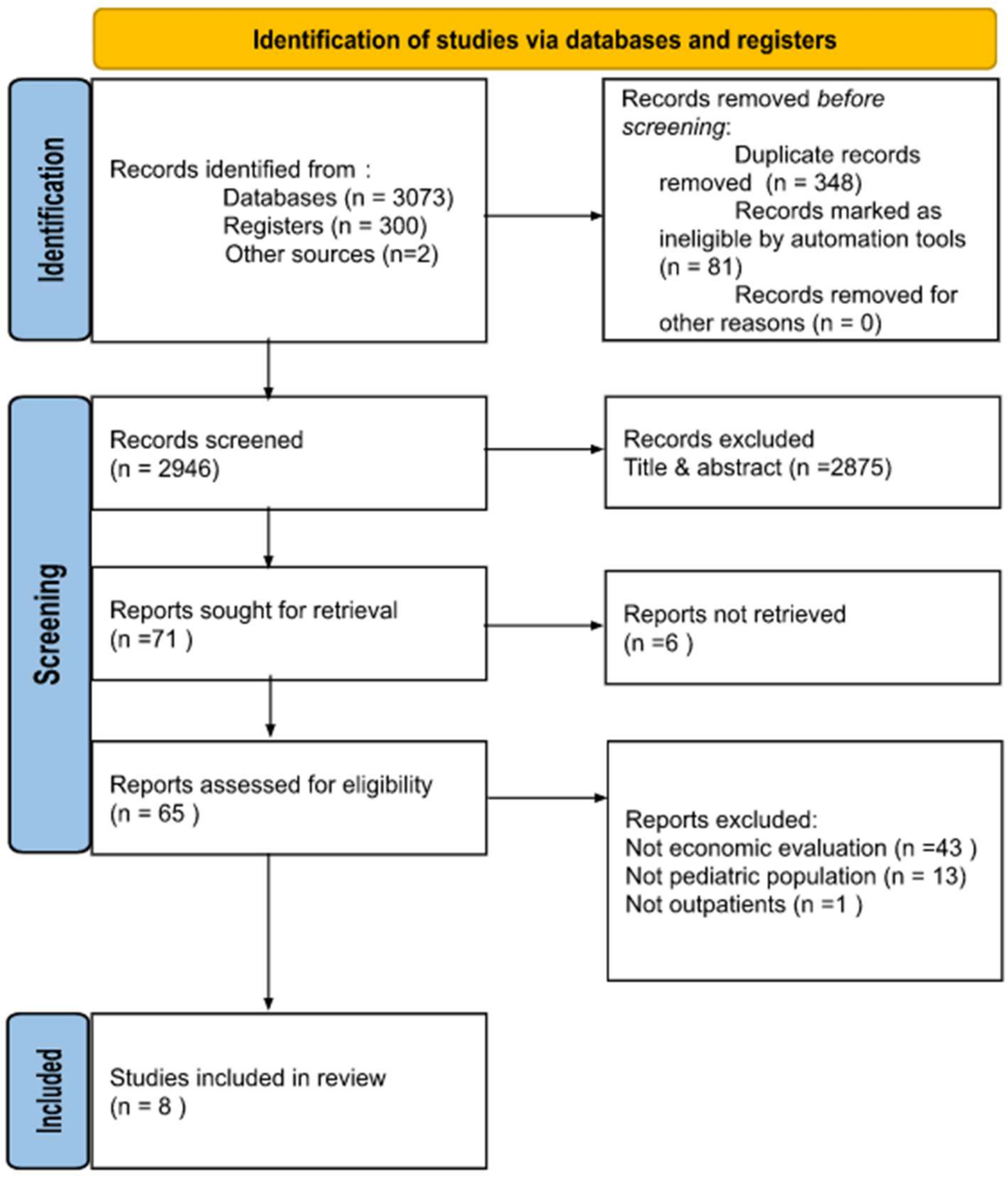
3.1. Database Research
3.2. Quality of Included Studies
3.3. Study Characteristics
3.4. Methodological Characteristics of Economic Evaluations
3.5. Economic-Evaluations Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hersh, A.L.; Shapiro, D.J.; Pavia, A.T.; Shah, S.S. Antibiotic Prescribing in Ambulatory Pediatrics in the United States. Pediatrics 2011, 128, 1053–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dooling, K.L.; Shapiro, D.J.; van Beneden, C.; Hersh, A.L.; Hicks, L.A. Overprescribing and Inappropriate Antibiotic Selection for Children with Pharyngitis in the United States, 1997–2010. JAMA Pediatr. 2014, 168, 1073–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, N.; Leonard, E.; Martin, J.M. Prevalence of Streptococcal Pharyngitis and Streptococcal Carriage in Children: A Meta-Analysis. Pediatrics 2010, 126, e557–e564. [Google Scholar] [CrossRef]
- Kronman, M.P.; Gerber, J.S.; Grundmeier, R.W.; Zhou, C.; Robinson, J.D.; Heritage, J.; Stout, J.; Burges, D.; Hedrick, B.; Warren, L.; et al. Reducing Antibiotic Prescribing in Primary Care for Respiratory Illness. Pediatrics 2020, 146, e20200038. [Google Scholar] [CrossRef] [PubMed]
- Miao, R.; Wan, C.; Wang, Z.; Zhu, Y.; Zhao, Y.; Zhang, L.; Liu, J.; Qin, J.; Xia, J.; Yan, H. Inappropriate Antibiotic Prescriptions among Pediatric Inpatients in Different Type Hospitals. Medicine 2020, 99, e18714. [Google Scholar] [CrossRef] [Green Version]
- Mattila, S.; Paalanne, N.; Honkila, M.; Pokka, T.; Tapiainen, T. Effect of Point-of-Care Testing for Respiratory Pathogens on Antibiotic Use in Children: A Randomized Clinical Trial. JAMA Netw. Open 2022, 5, e2216162. [Google Scholar] [CrossRef]
- Donà, D.; Barbieri, E.; Daverio, M.; Lundin, R.; Giaquinto, C.; Zaoutis, T.; Sharland, M. Implementation and Impact of Pediatric Antimicrobial Stewardship Programs: A Systematic Scoping Review. Antimicrob. Resist. Infect. Control. 2020, 9, 3. [Google Scholar] [CrossRef]
- Thompson, T.Z.; McMullen, A.R. Group A Streptococcus Testing in Pediatrics: The Move to Point-of-Care Molecular Testing. J. Clin. Microbiol. 2020, 58, e01494-19. [Google Scholar] [CrossRef]
- Impact of Point-of-Care C Reactive Protein in Ambulatory Care: A Systematic Review and Meta-Analysis | BMJ Open. Available online: https://bmjopen.bmj.com/content/9/1/e025036 (accessed on 26 July 2022).
- Lingervelder, D.; Koffijberg, H.; Kusters, R.; IJzerman, M.J. Health Economic Evidence of Point-of-Care Testing: A Systematic Review. PharmacoEconomics Open 2021, 5, 157–173. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.H.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 Explanation and Elaboration: A Report of the ISPOR CHEERS II Good Practices Task Force. Value Health 2022, 25, 10–31. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.E.; Boehme, C.; Borisch, B.; Dittrich, S. Application of a Simple Point-of-Care Test to Reduce UK Healthcare Costs and Adverse Events in Outpatient Acute Respiratory Infections. J. Med. Econ. 2020, 23, 673–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Howe, R.S.; Kusnier, L.P., II. Diagnosis and Management of Pharyngitis in a Pediatric Population Based on Cost-Effectiveness and Projected Health Outcomes. Pediatrics 2006, 117, 609–619. [Google Scholar] [CrossRef]
- Giraldez-Garcia, C.; Rubio, B.; Gallegos-Braun, J.F.; Imaz, I.; Gonzalez-Enriquez, J.; Sarria-Santamera, A. Diagnosis and Management of Acute Pharyngitis in a Paediatric Population: A Cost-Effectiveness Analysis. Eur. J. Pediatr. 2011, 170, 1059–1067. [Google Scholar] [CrossRef]
- Małecki, M.; Mazur, A.; Sobolewski, M.; Binkowska-Bury, M.; Marć, M.; Januszewicz, P. Rapid strip tests as a decision-making tool about antibiotic treatment in children—A prospective study. Pediatria Polska. 2017, 92, 149–155. [Google Scholar] [CrossRef]
- Lubell, Y.; Do, N.T.T.; Nguyen, K.V.; Ta, N.T.D.; Tran, N.T.H.; Than, H.M.; Hoang, L.B.; Shrestha, P.; van Doorn, R.H.; Nadjm, B.; et al. C-Reactive Protein Point of Care Testing in the Management of Acute Respiratory Infections in the Vietnamese Primary Healthcare Setting—A Cost Benefit Analysis. Antimicrob. Resist. Infect. Control. 2018, 7, 119. [Google Scholar] [CrossRef] [Green Version]
- Behnamfar, Z.; Shahkarami, V.; Sohrabi, S.; Aghdam, A.S.; Afzali, H. Cost and Effectiveness Analysis of the Diagnostic and Therapeutic Approaches of Group A Streptococcus Pharyngitis Management in Iran. J. Family Med. Prim. Care 2019, 8, 2942–2949. [Google Scholar] [CrossRef]
- Fraser, H.; Gallacher, D.; Achana, F.; Court, R.; Taylor-Phillips, S.; Nduka, C.; Stinton, C.; Willans, R.; Gill, P.; Mistry, H. Rapid antigen detection and molecular tests for group A streptococcal infections for acute sore throat: Systematic reviews and economic evaluation. Health Technol Assess. 2020, 24, 1–232. [Google Scholar] [CrossRef]
- Bilir, S.P.; Kruger, E.; Faller, M.; Munakata, J.; Karichu, J.K.; Sickler, J.; Cheng, M.M. US Cost-Effectiveness and Budget Impact of Point-of-Care NAAT for Streptococcus. Am. J. Manag. Care 2021, 27, e157–e163. [Google Scholar] [CrossRef]
- Zetts, R.M.; Stoesz, A.; Smith, B.A.; Hyun, D.Y. Outpatient Antibiotic Use and the Need for Increased Antibiotic Stewardship Efforts. Pediatrics 2018, 141, e20174124. [Google Scholar] [CrossRef] [Green Version]
- Ang, L.; Laskar, R.; Gray, J.W. A Point Prevalence Study of Infection and Antimicrobial Use at a UK Children’s Hospital. J. Hosp. Infect. 2008, 68, 372–374. [Google Scholar] [CrossRef]
- Vicentini, C.; Quattrocolo, F.; D’Ambrosio, A.; Corcione, S.; Ricchizzi, E.; Moro, M.L.; Rosa, F.G.D.; Zotti, C.M. Point Prevalence Data on Antimicrobial Usage in Italian Acute-Care Hospitals: Evaluation and Comparison of Results from Two National Surveys (2011–2016). Infect. Control. Hosp. Epidemiol. 2020, 41, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, S.E. The Relationship between Antimicrobial Resistance and Patient Outcomes: Mortality, Length of Hospital Stay, and Health Care Costs. Clin. Infect. Dis 2006, 42, S82–S89. [Google Scholar] [CrossRef] [Green Version]
- Messacar, K.; Parker, S.K.; Todd, J.K.; Dominguez, S.R. Implementation of Rapid Molecular Infectious Disease Diagnostics: The Role of Diagnostic and Antimicrobial Stewardship. J. Clin. Microbiol. 2017, 55, 715–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Randel, A. IDSA Updates Guideline for Managing Group A Streptococcal Pharyngitis. Am. Fam. Physician 2013, 88, 338–340. [Google Scholar]
- Martínez-González, N.A.; Keizer, E.; Plate, A.; Coenen, S.; Valeri, F.; Verbakel, J.Y.J.; Rosemann, T.; Neuner-Jehle, S.; Senn, O. Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing for Respiratory Tract Infections in Primary Care: Systematic Review and Meta-Analysis of Randomised Controlled Trials. Antibiotics 2020, 9, 610. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.J.; Hoffman, J.R.; Bartlett, J.G.; Besser, R.E.; Gonzales, R.; Hickner, J.M.; Sande, M.A.; American Academy of Family Physicians; American College of Physicians-American Society of Internal Medicine. Centers for Disease Control Principles of Appropriate Antibiotic Use for Acute Pharyngitis in Adults: Background. Ann. Intern. Med. 2001, 134, 509–517. [Google Scholar] [CrossRef]
- Cals, J.W.L.; Ament, A.J.H.A.; Hood, K.; Butler, C.C.; Hopstaken, R.M.; Wassink, G.F.; Dinant, G.-J. C-Reactive Protein Point of Care Testing and Physician Communication Skills Training for Lower Respiratory Tract Infections in General Practice: Economic Evaluation of a Cluster Randomized Trial. J. Eval. Clin. Pract. 2011, 17, 1059–1069. [Google Scholar] [CrossRef]
- Little, P.; Stuart, B.; Francis, N.; Douglas, E.; Tonkin-Crine, S.; Anthierens, S.; Cals, J.W.L.; Melbye, H.; Santer, M.; Moore, M.; et al. Effects of Internet-Based Training on Antibiotic Prescribing Rates for Acute Respiratory-Tract Infections: A Multinational, Cluster, Randomised, Factorial, Controlled Trial. Lancet 2013, 382, 1175–1182. [Google Scholar] [CrossRef] [Green Version]
- Aabenhus, R.; Jensen, J.-U.S. Biomarker-Guided Antibiotic Use in Primary Care in Resource-Constrained Environments. Lancet Glob. Health 2016, 4, e586–e587. [Google Scholar] [CrossRef] [Green Version]
- Rao, A.; Berg, B.; Quezada, T.; Fader, R.; Walker, K.; Tang, S.; Cowen, U.; Duncan, D.; Sickler, J. Diagnosis and Antibiotic Treatment of Group a Streptococcal Pharyngitis in Children in a Primary Care Setting: Impact of Point-of-Care Polymerase Chain Reaction. BMC Pediatr. 2019, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- Monsees, E.A.; Burns, A.N.; Lee, B.R.; Wirtz, A.; El Feghaly, R.E. Considerations for implementation: Pediatric outpatient antimicrobial stewardship program. Am. J. Infect. Control. 2021, 49, 1543–1546. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author, Year of Publication | Country | Population | Setting | Condition | POCT | Implementation Strategy for POCT | Non-POCT Comparator | Study Quality (CHEERS Score) |
|---|---|---|---|---|---|---|---|---|
| Van Howe, 2006 [15] | USA | Children (age not specified) | Primary care | URTI | RADT | (1) Standalone RADT, (2) RADT with culture confirmation of negative results, (3) clinical scoring tool + RADT | (1) No treatment, (2) treat all suspected cases, (3) perform culture | 21 |
| Giraldez-Garcia, 2011 [16] | Spain | Children (aged 2–14 years) | Primary care | URTI | RADT | (1) Standalone RADT, (2) RADT with culture confirmation of negative results, (3) clinical scoring tool + RADT | (1) Treat all suspected cases, (2) perform culture, (3) clinical scoring tool | 22 |
| Malecki, 2017 [17] | Poland | Children (aged 2–15 years) | Primary healthcare centers | URTI | RADT | Standalone RADT | Routine clinical practice | 11 |
| Lubell, 2018 [18] | Vietnam | Both children and adults (aged 1–65 years) | Primary healthcare centers | RTI | CRP | Standalone POC CRP | Routine clinical practice | 21 |
| Behnamfar, 2019 [19] | Iran | Children (aged 4–12.5 years) | Outpatient (GPs, pediatricians) | URTI | RADT | (1) Standalone RADT, (2) RADT plus culture, (3) RADT with culture confirmation of negative results | (1) Treat all suspected cases, (2) no treatment, (3) perform culture | 21 |
| Fraser, 2020 [20] | UK | Both children (aged 5–14 years) and adults (aged 15–75, modeled separately) | Primary and secondary care (modeled separately) | URTI | 17 different RADTs and four molecular tests | POCT + clinical scoring tool | Clinical assessment incorporating clinical scoring tools | 27 |
| Schneider, 2020 [14] | UK | Both children and adults (age not specified) | Outpatient | URTI and otitis media | CRP, dual-biomarker (CRP and MxA), hypothetical test | Standalone POCT | Routine clinical practice | 22 |
| Bilir, 2021 [21] | USA | Both children (<18 years) and adults (≥18 years) | Ambulatory care | URTI | NAAT vs. RADT | (1) Standalone POCT NAAT, (2) RADT with culture confirmation of negative results | (Only in budget impact analysis) All diagnostic techniques available in the USA (including culture and clinical scoring tools) | 24 |
| First Author, Year of Publication | Study Characteristics | Results | ||||||
|---|---|---|---|---|---|---|---|---|
| Study Design | Model-Based vs. Trial-Based | Time Horizon | Perspective | Outcomes | Sensitivity Analysis | Base-Case Results | Sensitivity-Analysis Results | |
| Van Howe, 2006 [15] | CUA | Model-based (decision tree) | NR | Societal, payer | Cost–effectiveness | DSA | RADT had the best cost–utility result from the payer perspective. | Considerable overlap among all of the options except (1) treating all patients and (2) observing all patients. |
| Giraldez-Garcia, 2011 [16] | CEA | Model-based (decision tree) | NR | Healthcare system | Cost–effectiveness, ICER, total annual cost | DSA | RADT combined with clinical score was the most cost-effective strategy. | Standalone RADT was the most cost-effective strategy when the sensitivity and specificity of clinical score decreased. |
| Malecki, 2017 [17] | CIA | Trial-based | NR | Healthcare system | Cost per patient | Not performed | Threshold cost per test set at PLN 12 | Not performed |
| Lubell, 2018 [18] | CBA | Trial-based | 14 days | Societal | Cost per patient | DSA | CRP testing was not cost-beneficial compared to usual care. | If adherence to test result increased, POCT would be cost-beneficial. |
| Behnamfar, 2019 [19] | CUA | Model-based (decision tree) | NR | Societal, payer | Cost–effectiveness, ICER | DSA | RADT was the most cost-effective strategy. | (1) RADT + culture and (2) culture were the most cost-effective strategies in some scenarios (varying the probability of peritonsillar abscess). |
| Fraser, 2020 [20] | CUA | Model-based (decision tree) | 1 year | Healthcare system and Personal Social Services perspective | Cost–effectiveness, ICER | PSA | Children’s primary care model: usual care was dominant compared to 4 tests; the other 17 tests were cost-effective compared to usual care but over WTP. | In line with deterministic results. |
| Schneider, 2020 [14] | BIA | Model-based | 1 year | Healthcare system | Cost per patient, total annual cost | DSA | All POCTs were cost-saving compared to status quo: hypothetical test −54%, CRP + MxA −27%, and CRP −11%. | Confirmed usual care to be the highest-cost prescription strategy, followed by CRP. |
| Bilir, 2021 [21] | CUA, BIA | Model-based (decision tree) | CUA: 1 year, BIA: 5 years | Payer, third-party payer | Cost per patient, cost–effectiveness, ICER, total costs over 5 years | DSA and PSA | POC NAAT was dominant compared to RADT + culture. | POC NAAT remained cost-saving across all simulations. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicentini, C.; Vola, L.; Previti, C.; Brescia, V.; Dal Mas, F.; Zotti, C.M.; Bert, F. Antimicrobial Stewardship Strategies Including Point-of-Care Testing (POCT) for Pediatric Patients with Upper-Respiratory-Tract Infections in Primary Care: A Systematic Review of Economic Evaluations. Antibiotics 2022, 11, 1139. https://doi.org/10.3390/antibiotics11081139
Vicentini C, Vola L, Previti C, Brescia V, Dal Mas F, Zotti CM, Bert F. Antimicrobial Stewardship Strategies Including Point-of-Care Testing (POCT) for Pediatric Patients with Upper-Respiratory-Tract Infections in Primary Care: A Systematic Review of Economic Evaluations. Antibiotics. 2022; 11(8):1139. https://doi.org/10.3390/antibiotics11081139
Chicago/Turabian StyleVicentini, Costanza, Lorenzo Vola, Christian Previti, Valerio Brescia, Francesca Dal Mas, Carla Maria Zotti, and Fabrizio Bert. 2022. "Antimicrobial Stewardship Strategies Including Point-of-Care Testing (POCT) for Pediatric Patients with Upper-Respiratory-Tract Infections in Primary Care: A Systematic Review of Economic Evaluations" Antibiotics 11, no. 8: 1139. https://doi.org/10.3390/antibiotics11081139
APA StyleVicentini, C., Vola, L., Previti, C., Brescia, V., Dal Mas, F., Zotti, C. M., & Bert, F. (2022). Antimicrobial Stewardship Strategies Including Point-of-Care Testing (POCT) for Pediatric Patients with Upper-Respiratory-Tract Infections in Primary Care: A Systematic Review of Economic Evaluations. Antibiotics, 11(8), 1139. https://doi.org/10.3390/antibiotics11081139