
First and Second-Line Anti-Tuberculosis Drug-Resistance Patterns in Pulmonary Tuberculosis Patients in Zambia

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Social-Demographic Characteristics of Study Participants
2.2. Drug-Resistance Pattern to First-Line Anti-TB Drugs among TB Patients
2.3. Drug Resistance to Second-Line Anti-TB Drugs among First-Line Drug-Resistant Patients
2.4. Drug-Resistant Tuberculosis among New and Previously Treated Cases
2.5. Factors Associated with Drug-Resistant TB
3. Discussion
4. Materials and Methods
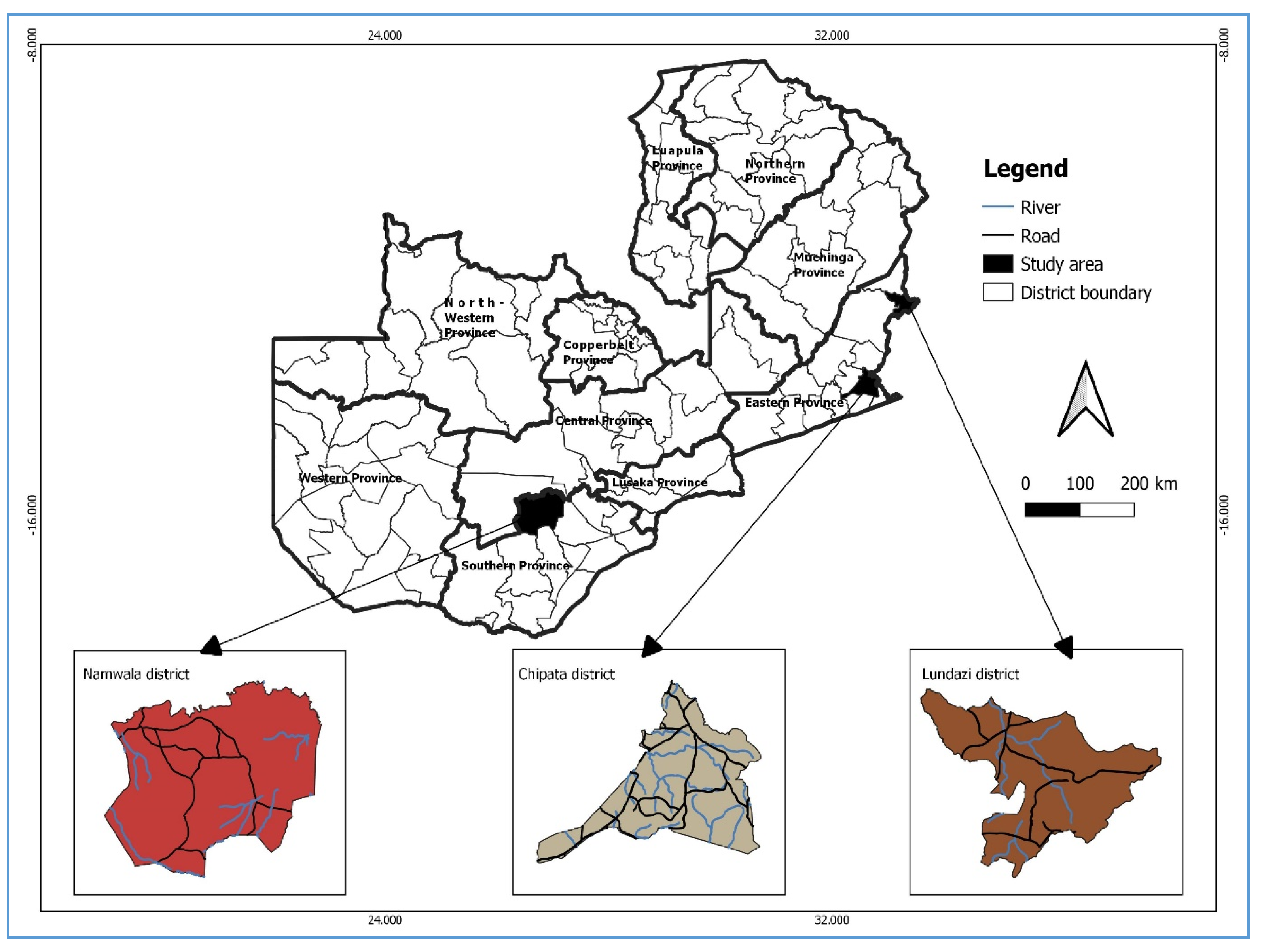
4.1. Study Design
4.2. Study Population
4.3. Data Collection
4.4. Specimen Collection
4.5. Laboratory Analyses
4.6. Quality Control
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, A.; Prasad, R.; Balasubramanian, V.; Gupta, N. Drug-resistant tuberculosis and hiv infection: Current perspectives. HIV/AIDS-Res. Palliat. Care 2020, 12, 9–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Technical Manual for Drug Susceptibility Testing of Medicines Used in the Treatment of Tuberculosis; Report No.: 9789241514842; World Health Organization: Geneva, Switzerland, 2018; p. 39. Available online: https://apps.who.int/iris/handle/10665/275469 (accessed on 21 November 2022).
- Zhang, M.W.; Zhou, L.; Zhang, Y.; Chen, B.; Peng, Y.; Wang, F.; Liu, Z.W.; Wang, X.M.; Chen, S.H. Treatment outcomes of patients with multidrug and extensively drug-resistant tuberculosis in Zhejiang, China. Eur. J. Med. Res. 2021, 26, 31. [Google Scholar] [CrossRef] [PubMed]
- Bhering, M.; Duarte, R.; Kritski, A. Predictive factors for unfavourable treatment in MDR-TB and XDR-TB patients in Rio de Janeiro State, Brazil, 2000–2016. PLoS ONE 2019, 14, e0218299. [Google Scholar] [CrossRef] [Green Version]
- Alene, K.A.; Yi, H.; Viney, K.; McBryde, E.S.; Yang, K.; Bai, L.; Gray, D.J.; Clements, A.C.A.; Xu, Z. Treatment outcomes of patients with multidrug-resistant and extensively drug resistant tuberculosis in Hunan Province, China. BMC Infect. Dis. 2017, 17, 573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, M.R.; Padayatchi, N.; Kvasnovsky, C.; Werner, L.; Master, I.; Horsburgh, C.R. Treatment Outcomes for Extensively Drug-Resistant Tuberculosis and HIV Co-infection. Emerg. Infect Dis. 2013, 19, 416–424. [Google Scholar] [CrossRef]
- Katale, B.Z.; Mbelele, P.M.; Lema, N.A.; Campino, S.; Mshana, S.E.; Rweyemamu, M.M.; Phelan, J.E.; Keyyu, J.D.; Majigo, M.; Mbugi, E.V.; et al. Whole genome sequencing of Mycobacterium tuberculosis isolates and clinical outcomes of patients treated for multidrug-resistant tuberculosis in Tanzania. BMC Genom. 2020, 21, 174. [Google Scholar] [CrossRef] [Green Version]
- Nuwagira, E.; Stadelman, A.; Baluku, J.B.; Rhein, J.; Byakika-Kibwika, P.; Mayanja, H.; Kunisaki, K.M. Obstructive lung disease and quality of life after cure of multi-drug-resistant tuberculosis in Uganda: A cross-sectional study. Trop. Med. Health 2020, 48, 34. [Google Scholar] [CrossRef]
- Singla, R.; Mallick, M.; Mrigpuri, P.; Singla, N.; Gupta, A. Sequelae of pulmonary multidrug-resistant tuberculosis at the completion of treatment. Lung India 2018, 35, 4–8. [Google Scholar] [CrossRef]
- Allwood, B.W.; Byrne, A.; Meghji, J.; Rachow, A.; van der Zalm, M.M.; Schoch, O.D. Post-Tuberculosis Lung Disease: Clinical Review of an Under-Recognised Global Challenge. Respiration 2021, 100, 751–763. [Google Scholar] [CrossRef]
- Silva, D.R.; Freitas, A.A.; Guimarães, A.R.; D’Ambrosio, L.; Centis, R.; Muñoz-Torrico, M.; Visca, D.; Migliori, G.B. Post-tuberculosis lung disease: A comparison of Brazilian, Italian, and Mexican cohorts. J Bras. Pneumol. 2022, 48, e20210515. [Google Scholar]
- Migliori, G.B.; Marx, F.M.; Ambrosino, N.; Zampogna, E.; Schaaf, H.S.; van der Zalm, M.M.; Allwood, B.; Byrne, A.L.; Mortimer, K.; Wallis, R.S.; et al. Clinical standards for the assessment, management and rehabilitation of post-TB lung disease. Int. J. Tuberc. Lung Dis. 2021, 25, 797–813. [Google Scholar] [CrossRef] [PubMed]
- Menzies, N.A.; Quaife, M.; Allwood, B.W.; Byrne, A.L.; Coussens, A.K.; Harries, A.D.; Marx, F.M.; Meghji, J.; Pedrazzoli, D.; Salomon, J.A.; et al. Lifetime burden of disease due to incident tuberculosis: A global reappraisal including post-tuberculosis sequelae. Lancet Glob. Health 2021, 9, e1679–e1687. [Google Scholar] [CrossRef]
- Akkerman, O.W.; ter Beek, L.; Centis, R.; Maeurer, M.; Visca, D.; Muñoz-Torrico, M.; Tiberi, S.; Migliori, G.B. Rehabilitation, optimized nutritional care, and boosting host internal milieu to improve long-term treatment outcomes in tuberculosis patients. Int. J. Infect. Dis. 2020, 92, S10–S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Tuberculosis Report 2021. Available online: https://www.who.int/publications-detail-redirect/9789240037021 (accessed on 3 June 2022).
- Migliori, G.B.; Dheda, K.; Centis, R.; Mwaba, P.; Bates, M.; O’Grady, J.; Hoelscher, M.; Zumla, A. Review of multidrug-resistant and extensively drug-resistant TB: Global perspectives with a focus on sub-Saharan Africa. Trop. Med. Int. Health 2010, 15, 1052–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saravanan, M.; Niguse, S.; Abdulkader, M.; Tsegay, E.; Hailekiros, H.; Gebrekidan, A.; Araya, T.; Pugazhendhi, A. Review on emergence of drug-resistant tuberculosis (MDR & XDR-TB) and its molecular diagnosis in Ethiopia. Microb. Pathog. 2018, 117, 237–242. [Google Scholar]
- Chesov, E.; Chesov, D.; Maurer, F.P.; Andres, S.; Utpatel, C.; Barilar, I.; Donica, A.; Reimann, M.; Niemann, S.; Lange, C.; et al. Emergence of bedaquiline resistance in a high tuberculosis burden country. Eur. Respir. J. 2022, 59, 2100621. [Google Scholar] [CrossRef]
- Ghodousi, A.; Rizvi, A.H.; Khanzada, F.M.; Akhtar, N.; Ghafoor, A.; Trovato, A.; Cirillo, D.M.; Tahseen, S. In vivo microevolution of Mycobacterium tuberculosis and transient emergence of atpE_Ala63Pro mutation during treatment in a pre-XDR TB patient. Eur. Respir. J. 2022, 59, 2102102. [Google Scholar] [CrossRef]
- Nair, P.; Hasan, T.; Zaw, K.K.; Allamuratova, S.; Ismailov, A.; Mendonca, P.; Bekbaev, Z.; Parpieva, N.; Singh, J.; Sitali, N.; et al. Acquired bedaquiline resistance in Karakalpakstan, Uzbekistan. Int. J. Tuberc. Lung Dis. 2022, 26, 658–663. [Google Scholar] [CrossRef]
- Nimmo, C.; Millard, J.; van Dorp, L.; Brien, K.; Moodley, S.; Wolf, A.; Grant, A.D.; Padayatchi, N.; Pym, A.S.; Balloux, F.; et al. Population-level emergence of bedaquiline and clofazimine resistance-associated variants among patients with drug-resistant tuberculosis in southern Africa: A phenotypic and phylogenetic analysis. Lancet Microbe 2020, 1, e165–e174. [Google Scholar] [CrossRef]
- Kaniga, K.; Hasan, R.; Jou, R.; Vasiliauskienė, E.; Chuchottaworn, C.; Ismail, N.; Metchock, B.; Miliauskas, S.; Nhung, N.V.; Rodrigues, C.; et al. Bedaquiline Drug Resistance Emergence Assessment in Multidrug-Resistant Tuberculosis (MDR-TB): A 5-Year Prospective In Vitro Surveillance Study of Bedaquiline and Other Second-Line Drug Susceptibility Testing in MDR-TB Isolates. J. Clin. Microbiol. 2022, 60, e0291920. [Google Scholar] [CrossRef]
- Lv, X.T.; Lu, X.W.; Shi, X.Y.; Zhou, L. Prevalence and risk factors of multi-drug resistant tuberculosis in Dalian, China. J. Int. Med. Res. 2017, 45, 1779–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yonge, S.A.; Otieno, M.F.; Sharma, R.R.; Nteka, S.S. Drug Susceptibility Patterns of Mycobacterium tuberculosis Isolates from Tuberculosis Patients in Coastal Kenya. J. Tuberc. Res. 2017, 5, 201–219. [Google Scholar] [CrossRef]
- Seyoum, B.; Demissie, M.; Worku, A.; Bekele, S.; Aseffa, A. Prevalence and Drug Resistance Patterns of Mycobacterium tuberculosis among New Smear Positive Pulmonary Tuberculosis Patients in Eastern Ethiopia. Tuberc. Res. Treat. 2014, 2014, e753492. [Google Scholar]
- Dagne, B.; Desta, K.; Fekade, R.; Amare, M.; Tadesse, M.; Diriba, G.; Zerihun, B.; Getu, M.; Sinshaw, W.; Seid, G.; et al. The Epidemiology of first and second-line drug-resistance Mycobacterium tuberculosis complex common species: Evidence from selected TB treatment initiating centers in Ethiopia. PLoS ONE 2021, 16, e0245687. [Google Scholar] [CrossRef]
- Diriba, G.; Kebede, A.; Tola, H.H.; Alemu, A.; Tadesse, M.; Tesfaye, E.; Mehamed, Z.; Meaza, A.; Yenew, B.; Molalign, H.; et al. Surveillance of drug resistance tuberculosis based on reference laboratory data in Ethiopia. Infect. Dis. Poverty 2019, 8, 54. [Google Scholar] [CrossRef]
- Uzoewulu, N.G.; Ibeh, I.N.; Lawson, L.; Goyal, M.; Umenyonu, N.; Ofiaeli, R.O.; Okonkwo, R. Drug Resistant Mycobacterium tuberculosis in Tertiary Hospital South East, Nigeria. J. Med. Microb. Diagn. 2014, 3, 1. [Google Scholar]
- Saifullah, A.; Mallhi, T.H.; Khan, Y.H.; Iqbal, M.S.; Alotaibi, N.H.; Alzarea, A.I.; Rasheed, M. Evaluation of risk factors associated with the development of MDR- and XDR-TB in a tertiary care hospital: A retrospective cohort study. PeerJ 2021, 9, e10826. [Google Scholar] [CrossRef]
- Sinshaw, W.; Kebede, A.; Bitew, A.; Tesfaye, E.; Tadesse, M.; Mehamed, Z.; Yenew, B.; Amare, M.; Dagne, B.; Diriba, G.; et al. Prevalence of tuberculosis, multidrug resistant tuberculosis and associated risk factors among smear negative presumptive pulmonary tuberculosis patients in Addis Ababa, Ethiopia. BMC Infect. Dis. 2019, 19, 641. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.B.; Nguyen, N.V.; Tran, H.T.G.; Nguyen, H.V.; Bui, Q.T.T. Prevalence of resistance to second-line tuberculosis drug among multidrug-resistant tuberculosis patients in Viet Nam, 2011. West. Pac. Surveill. Response J. WPSAR 2016, 7, 35. [Google Scholar] [CrossRef] [Green Version]
- Lecai, J.; Mijiti, P.; Chuangyue, H.; Mingzhen, L.; Qian, G.; Weiguo, T.; Jihong, C. Predictors and Trends of MDR/RR-TB in Shenzhen China: A Retrospective 2012–2020 Period Analysis. Infect. Drug Resist. 2021, 14, 4481–4491. [Google Scholar] [CrossRef]
- Welekidan, L.N.; Skjerve, E.; Dejene, T.A.; Gebremichael, M.W.; Brynildsrud, O.; Agdestein, A.; Tessema, G.T.; Tønjum, T.; Yimer, S.A. Characteristics of pulmonary multidrug-resistant tuberculosis patients in Tigray Region, Ethiopia: A cross-sectional study. PLoS ONE 2020, 15, e0236362. [Google Scholar] [CrossRef] [PubMed]
- Monde, N.; Zulu, M.; Tembo, M.; Handema, R.; Munyeme, M.; Malama, S. Drug Resistant Tuberculosis in the Northern Region of Zambia: A Retrospective Study. Front. Trop. Dis. 2021, 2, 735028. [Google Scholar] [CrossRef]
- Mehari, K.; Asmelash, T.; Hailekiros, H.; Wubayehu, T.; Godefay, H.; Araya, T.; Saravanan, M. Prevalence and Factors Associated with Multidrug-Resistant Tuberculosis (MDR-TB) among Presumptive MDR-TB Patients in Tigray Region, Northern Ethiopia. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, e2923549. [Google Scholar] [CrossRef] [PubMed]
- Sabeel, S.M.A.; Salih, M.A.; Ali, M.; EL-Zaki, S.E.; Abuzeid, N.; Elgadi, Z.A.M.; Altayb, H.N.; Elegail, A.M.A.; Ibrahim, N.Y.; Elamin, B.K. Phenotypic and Genotypic Analysis of Multidrug-Resistant Mycobacterium tuberculosis Isolates from Sudanese Patients. Tuberc. Res. Treat. 2017, 2017, 8340746. [Google Scholar] [PubMed]
- Maharjan, S.; Singh, A.; Khadka, D.K.; Aryal, M. Drug Resistance Pattern in Pulmonary Tuberculosis Patients and Risk Factors Associated with Multi-Drug Resistant Tuberculosis. J. Tuberc. Res. 2017, 5, 106–117. [Google Scholar] [CrossRef] [Green Version]
- Mvelase, N.R.; Balakrishna, Y.; Lutchminarain, K.; Mlisana, K. Evolving rifampicin and isoniazid mono-resistance in a high multidrug-resistant and extensively drug-resistant tuberculosis region: A retrospective data analysis. BMJ Open 2019, 9, e031663. [Google Scholar] [CrossRef] [Green Version]
- Sulis, G.; Pai, M. Isoniazid-resistant tuberculosis: A problem we can no longer ignore. PLoS Med. 2020, 17, e1003023. [Google Scholar] [CrossRef]
- Báez-Saldaña, R.; Delgado-Sánchez, G.; García-García, L.; Cruz-Hervert, L.P.; Montesinos-Castillo, M.; Ferreyra-Reyes, L.; Bobadilla-del-Valle, M.; Canizales-Quintero, S.; Ferreira-Guerrero, E.; Téllez-Vázquez, N.; et al. Isoniazid Mono-Resistant Tuberculosis: Impact on Treatment Outcome and Survival of Pulmonary Tuberculosis Patients in Southern Mexico 1995–2010. PLoS ONE 2016, 11, e0168955. [Google Scholar] [CrossRef] [Green Version]
- Villegas, L.; Otero, L.; Sterling, T.R.; Huaman, M.A.; der Stuyft, P.V.; Gotuzzo, E.; Seas, C. Prevalence, Risk Factors, and Treatment Outcomes of Isoniazid- and Rifampicin- Mono-Resistant Pulmonary Tuberculosis in Lima, Peru. PLoS ONE 2016, 11, e0152933. [Google Scholar] [CrossRef] [Green Version]
- Dean, A.S.; Zignol, M.; Cabibbe, A.M.; Falzon, D.; Glaziou, P.; Cirillo, D.M.; Koser, C.U.; Gonzalez-Angulo, L.Y.; Tosas-Auget, T.; Ismail, N.; et al. Prevalence and genetic profiles of isoniazid resistance in tuberculosis patients: A multicountry analysis of cross-sectional data. PLOS Med. 2020, 17, e1003008. [Google Scholar] [CrossRef] [Green Version]
- Bachir, M.; Guglielmetti, L.; Tunesi, S.; Billard-Pomares, T.; Chiesi, S.; Jaffré, J.; Langris, H.; Pourcher, V.; Schramm, F.; Lemaître, N.; et al. Isoniazid-monoresistant tuberculosis in France: Risk factors, treatment outcomes and adverse events. Int. J. Infect. Dis. 2021, 107, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S. Primary Isoniazid Mono-Resistant Pulmonary Tuberculosis in a COVID-19-Positive Male: World’s First Case of Its Kind in the Present Pandemic. Cureus 2022, 14, e27163. [Google Scholar] [CrossRef] [PubMed]
- Karo, B.; Kohlenberg, A.; Hollo, V.; Duarte, R.; Fiebig, L.; Jackson, S.; Kearns, C.; Ködmön, C.; Korzeniewska-Kosela, M.; Papaventsis, D.; et al. Isoniazid (INH) mono-resistance and tuberculosis (TB) treatment success: Analysis of European surveillance data, 2002 to 2014. Eurosurveillance 2019, 24, 1800392. [Google Scholar] [CrossRef] [PubMed]
- Stagg, H.R.; Bothamley, G.H.; Davidson, J.A.; Kunst, H.; Lalor, M.K.; Lipman, M.C.; Loutet, M.G.; Lozewicz, S.; Mohiyuddin, T.; Abbara, A.; et al. Fluoroquinolones and isoniazid-resistant tuberculosis: Implications for the 2018 WHO guidance. Eur. Respir. J. 2019, 54, 1900982. [Google Scholar] [CrossRef]
- Romanowski, K.; Campbell, J.R.; Oxlade, O.; Fregonese, F.; Menzies, D.; Johnston, J.C. The impact of improved detection and treatment of isoniazid resistant tuberculosis on prevalence of multi-drug resistant tuberculosis: A modelling study. PLoS ONE 2019, 14, e0211355. [Google Scholar] [CrossRef]
- Gegia, M.; Winters, N.; Benedetti, A.; van Soolingen, D.; Menzies, D. Treatment of isoniazid-resistant tuberculosis with first-line drugs: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 223–234. [Google Scholar] [CrossRef]
- Sonnenkalb, L.; Carter, J.; Spitaleri, A.; Iqbal, Z.; Hunt, M.; Malone, K.; Utpatel, C.; Cirillo, D.M.; Rodrigues, C.; Nilgiriwala, K.S.; et al. Deciphering Bedaquiline and Clofazimine Resistance in Tuberculosis: An Evolutionary Medicine Approach. bioRxiv 2021. [Google Scholar] [CrossRef]
- Pang, Y.; Zong, Z.; Huo, F.; Jing, W.; Ma, Y.; Dong, L.; Li, Y.; Zhao, L.; Fu, Y.; Huang, H. In Vitro Drug Susceptibility of Bedaquiline, Delamanid, Linezolid, Clofazimine, Moxifloxacin, and Gatifloxacin against Extensively Drug-Resistant Tuberculosis in Beijing, China. Antimicrob. Agents Chemother. 2017, 61, e00900-17. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.; Jiang, G.; Jing, W.; Zong, Z.; Yu, X.; Chen, S.; Li, W.; Huang, H. Prevalence and molecular characterizations of seven additional drug resistance among multidrug-resistant tuberculosis in China: A subsequent study of a national survey. J. Infect. 2021, 82, 371–377. [Google Scholar] [CrossRef]
- Kadura, S.; King, N.; Nakhoul, M.; Zhu, H.; Theron, G.; Köser, C.U.; Farhat, M. Systematic review of mutations associated with resistance to the new and repurposed Mycobacterium tuberculosis drugs bedaquiline, clofazimine, linezolid, delamanid and pretomanid. J. Antimicrob. Chemother. 2020, 75, 2031–2043. [Google Scholar] [CrossRef]
- Xu, J.; Wang, B.; Hu, M.; Huo, F.; Guo, S.; Jing, W.; Nuermberger, E.; Lua, Y. Primary Clofazimine and Bedaquiline Resistance among Isolates from Patients with Multidrug-Resistant Tuberculosis. Antimicrob. Agents Chemother. 2017, 61, e00239-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckert, P.; Sanchez-Padilla, E.; Merker, M.; Dreyer, V.; Kohl, T.A.; Utpatel, C.; Köser, C.U.; Barilar, I.; Ismail, N.; Omar, S.V.; et al. MDR M. tuberculosis outbreak clone in Eswatini missed by Xpert has elevated bedaquiline resistance dated to the pre-treatment era. Genome Med. 2020, 12, 104. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.; Cravo, P.; Viveiros, M. Efflux pump inhibitors as a promising adjunct therapy against drug resistant tuberculosis: A new strategy to revisit mycobacterial targets and repurpose old drugs. Expert Rev. Anti-Infect. Ther. 2020, 18, 741–757. [Google Scholar] [CrossRef]
- Hartkoorn, R.C.; Uplekar, S.; Cole, S.T. Cross-Resistance between Clofazimine and Bedaquiline through Upregulation of MmpL5 in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 2014, 58, 2979–2981. [Google Scholar] [CrossRef] [PubMed]
- Yao, C.; Guo, H.; Li, Q.; Zhang, X.; Shang, Y.; Li, T.; Wang, Y.; Xue, Z.; Wang, L.; Li, L.; et al. Prevalence of extensively drug-resistant tuberculosis in a Chinese multidrug-resistant TB cohort after redefinition. Antimicrob. Resist. Infect Control. 2021, 10, 126. [Google Scholar] [CrossRef] [PubMed]
- Elmi, O.S.; Hasan, H.; Abdullah, S.; Jeab, M.Z.M.; Alwi, Z.B.; Naing, N.N. Multidrug-resistant tuberculosis and risk factors associated with its development: A retrospective study. J. Infect. Dev. Ctries. 2015, 9, 1076–1085. [Google Scholar] [CrossRef] [Green Version]
- Daniel, O.; Osman, E. Prevalence and risk factors associated with drug resistant TB in South West, Nigeria. Asian Pac. J. Trop. Med. 2011, 4, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Kamolwat, P.; Nateniyom, S.; Chaiprasert, A.; Disratthakit, A.; Mahasirimongkol, S.; Yamada, N.; Smithtikarn, S. Prevalence and associated risk factors of drug-resistant tuberculosis in Thailand: Results from the fifth national anti-tuberculosis drug resistance survey. Trop. Med. Int. Health 2021, 26, 45–53. [Google Scholar] [CrossRef]
- Ladha, N.; Bhardwaj, P.; Chauhan, N.K.; Naveen, K.H.S.; Nag, V.L.; Giribabu, D. Determinants, risk factors and spatial analysis of multi-drug resistant pulmonary tuberculosis in Jodhpur, India. Monaldi. Arch. Chest Dis. 2022, 92, 2026. [Google Scholar] [CrossRef]
- Ambaye, G.Y.; Tsegaye, G.W. Factors Associated with Multi-Drug Resistant Tuberculosis among TB Patients in Selected Treatment Centers of Amhara Region: A Case-Control Study. Ethiop. J. Health Sci. 2021, 31, 25–34. [Google Scholar]
- Batte, C.; Namusobya, M.S.; Kirabo, R.; Mukisa, J.; Adakun, S.; Katamba, A. Prevalence and factors associated with non-adherence to multi-drug resistant tuberculosis (MDR-TB) treatment at Mulago National Referral Hospital, Kampala, Uganda. Afr. Health Sci. 2021, 21, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Kapata, N.; Mbulo, G.; Cobelens, F.; de Haas, P.; Schaap, A.; Mwamba, P.; Mwanza, W.; Muvwimi, M.; Muyoyeta, M.; Moyo, M.; et al. The Second Zambian National Tuberculosis Drug Resistance survey–A comparison of conventional and molecular methods. Trop. Med. Int. Health 2015, 20, 1492–1500. [Google Scholar] [CrossRef] [PubMed]
- Mulenga, C.; Chonde, A.; Bwalya, I.C.; Kapata, N.; Kakungu-Simpungwe, M.; Docx, S.; Fissette, K.; Shamputa, I.C.; Portaels, F.; Rigouts, L. Low Occurrence of Tuberculosis Drug Resistance among Pulmonary Tuberculosis Patients from an Urban Setting, with a Long-Running DOTS Program in Zambia. Tuberc. Res. Treat. 2010, 2010, 938178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapata, N.; Chanda-Kapata, P.; Bates, M.; Mwaba, P.; Cobelens, F.; Grobusch, M.P.; Zumla, A. Multidrug-resistant TB in Zambia: Review of national data from 2000 to 2011. Trop. Med. Int. Health 2013, 18, 1386–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masenga, S.K.; Mubila, H.; Hamooya, B.M. Rifampicin resistance in mycobacterium tuberculosis patients using GeneXpert at Livingstone Central Hospital for the year 2015: A cross sectional explorative study. BMC Infect. Dis. 2017, 17, 640. [Google Scholar] [CrossRef] [PubMed]
- Habeenzu, C.; Mitarai, S.; Lubasi, D.; Mudenda, V.; Kantenga, T.; Mwansa, J.; Maslow, J.N. Tuberculosis and multidrug resistance in Zambian prisons, 2000–2001. Int. J. Tuberc. Lung Dis. 2007, 11, 1216–1220. [Google Scholar]
- Lungu, P.; Kasapo, C.; Mihova, R.; Chimzizi, R.; Sikazwe, L.; Banda, I.; Mucheleng’anga, L.A.; Chanda-Kapata, P.; Kapata, N.; Zumla, A.; et al. A 10-year Review of TB Notifications and Mortality Trends Using a Joint Point Analysis in Zambia-a High TB burden country. Int. J. Infect. Dis. 2022, 124, S30–S40. [Google Scholar] [CrossRef]
- Pradipta, I.S.; Forsman, L.D.; Bruchfeld, J.; Hak, E.; Alffenaar, J.W. Risk factors of multidrug-resistant tuberculosis: A global systematic review and meta-analysis. J. Infect. 2018, 77, 469–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faustini, A.; Hall, A.J.; Perucci, C.A. Risk factors for multidrug resistant tuberculosis in Europe: A systematic review. Thorax 2006, 61, 158–163. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Lalwani, J.; Pandey, P.; Thakur, A. Factors Associated with the Development of Secondary Multidrug-resistant Tuberculosis. Int. J. Prev. Med. 2019, 10, 67. [Google Scholar]
- Suchindran, S.; Brouwer, E.S.; Van Rie, A. Is HIV infection a risk factor for multi-drug resistant tuberculosis? A systematic review. PLoS ONE 2009, 4, e5561. [Google Scholar] [CrossRef] [PubMed]
- Mesfin, Y.M.; Hailemariam, D.; Biadglign, S.; Kibret, K.T. Association between HIV/AIDS and Multi-Drug Resistance Tuberculosis: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e82235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultana, Z.Z.; Hoque, F.U.; Beyene, J.; Akhlak-Ul-Islam Md Khan, M.H.R.; Ahmed, S.; Hawlader, D.H.; Hossain, A. HIV infection and multidrug resistant tuberculosis: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 51. [Google Scholar]
- Pooranagangadevi, N.; Padmapriyadarsini, C. Treatment of Tuberculosis and the Drug Interactions Associated With HIV-TB Co-Infection Treatment. Front. Trop. Dis. 2022, 3, 834013. [Google Scholar] [CrossRef]
- Butov, D.O. Malabsorption syndromes in patients with tuberculosis as a cause of ineffective treatment: How to diagnose and overcome? Infus. Chemother. 2020, 3, 24–25. [Google Scholar] [CrossRef]
- Kent, P.T.; Kubica, G.P. Public Health Mycobacteriology: A Guide for the Level III Laboratory; Report No.: PB86216546; Centers for Disease Control: Atlanta, GA, USA, 1985. Available online: https://ntrl.ntis.gov/NTRL/dashboard/searchResults/titleDetail/PB86216546.xhtml (accessed on 29 November 2022).
- Mokaddas, E.; Ahmad, S.; Samir, I. Secular trends in susceptibility patterns of Mycobacterium tuberculosis isolates in Kuwait, 1996–2005. Int. J. Tuberc. Lung Dis. 2008, 12, 319–325. [Google Scholar] [PubMed]
- Worku, G.; Gumi, B.; Musse, G.; Mohammedbirhan, B.; Diriba, G.; Seid, G.; Getu, M.; Amare, M.; Sinshaw, W.; Ashagre, W.; et al. Drug sensitivity of clinical isolates of Mycobacterium tuberculosis and its association with bacterial genotype in the Somali region, Eastern Ethiopia. Front. Public Health 2022, 10, 942618. [Google Scholar] [CrossRef]
- Ahmad, S.; Mokaddas, E.; Al-Mutairi, N.; Eldeen, H.S.; Mohammadi, S. Discordance across Phenotypic and Molecular Methods for Drug Susceptibility Testing of Drug-Resistant Mycobacterium tuberculosis Isolates in a Low TB Incidence Country. PLoS ONE 2016, 11, e0153563. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Category | Frequency (N = 132) | Proportion (%) | 95% CI |
|---|---|---|---|---|
| Gender | Male | 94 | 71.2 | 62.7–78.8 |
| Female | 38 | 28.8 | 21.2–37.3 | |
| Age | 0–24 years | 14 | 10.6 | 5.9–17.2 |
| 25–44 years | 87 | 65.9 | 57.2–73.9 | |
| 45+ years | 31 | 23.5 | 16.5–31.6 | |
| HIV Status | Reactive | 59 | 44.7 | 36.0–53.6 |
| Non-reactive | 73 | 55.3 | 46.4–64.0 | |
| Address | Urban | 85 | 64.4 | 55.6–72.7 |
| Rural | 47 | 35.6 | 27.5–44.4 | |
| Province | Southern | 54 | 40.9 | 32.4–49.8 |
| Eastern | 78 | 59.1 | 50.2–67.6 | |
| Reasons for Examination | Diagnosis | 87 | 65.9 | 57.2–73.9 |
| Follow up | 45 | 34.1 | 26.1–42.8 | |
| TB Status | Drug Resistant | 31 | 23.5 | 16.5–31.6 |
| Drug Susceptible | 101 | 76.5 | 68.4–83.5 |
| First-Line DST | Number (N = 132) | Proportion (%) | 95% CI |
|---|---|---|---|
| Multidrug resistant | 13 | 9.8 | 5.3–16.2 |
| Rifampicin mono- resistant | 4 | 3.0 | 0.8–7.6 |
| Isoniazid mono- resistant | 13 | 9.8 | 5.3–16.2 |
| Streptomycin mono- resistant | 1 | 0.8 | 0.001–4.1 |
| Susceptible (RIF, INH, STR, ETH) | 101 | 76.5 | 68.4–83.5 |
| Second-Line DST | Number Resistant (N = 31) | Proportion (%) | 95% CI |
|---|---|---|---|
| BDQ + CFZ | 04 | 12.9 | 3.6–29.8 |
| CFZ | 04 | 12.9 | 3.6–29.8 |
| BDQ + CFZ + LEVO + MOX # | 02 | 6.5 | 0.8–21.4 |
| MOX * | 01 | 3.2 | 0.08–16.7 |
| LZD | 0 | 0 | - |
| Susceptible (BDQ, CFZ, LEXO, MOX, LZD) | 20 | 64.5 | 45.4–80.8 |
| DR Pattern | Total (n = 132), (%) | New Cases (n = 85), (%) | Previously Treated Cases (n = 47), (%) |
|---|---|---|---|
| Susceptible | 101 (76.5) | 82 (96.5) | 19 (40.2) |
| MDR | 13 (9.8) | 01 (1.2) | 12 (25.5) |
| RR | 04 (3.0) | 01 (1.2) | 03 (6.4) |
| INH | 13 (9.8) | 0 (0) | 13 (27.7) |
| STR | 01 (0.8) | 01 (1.2) | 0 (0) |
| DR Pattern | Total (n = 31) | New Cases (n = 3) | Previously Treated Cases (n = 28) |
|---|---|---|---|
| Susceptible | 20 (64.5) | 03 (100) | 17 (60.7) |
| BDQ + CFZ | 04 (12.9) | 0 (0) | 04 (14.3) |
| CFZ | 04 (12.9) | 0 (0) | 04 (14.3) |
| BDQ + CFZ + LEVO + MOX | 02 (6.5) | 0 (0) | 02 (7.1) |
| MOX | 01 (3.2) | 0 (0) | 01 (3.6) |
| LZD | 0 (0) | 0 (0) | 0 (0) |
| Variable | Level (n = 132) | Frequency | DR_TB (%) | OR | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Gender | Male | 94 | 23 (24.5) | 1.22 | 0.49–3.02 | 0.675 |
| Female | 38 | 8 (21) | 1 | |||
| Age | 0–24 years | 14 | 2 (14.3) | 2.43 | 0.46– 13.25 | 0.302 |
| 25–44 years | 87 | 20 (23.0) | 1.37 | 0.55–3.45 | 0.503 | |
| 45+ years | 31 | 9 (29.0) | 1 | |||
| HIV Status | Reactive | 59 | 13 (22.0) | 1.16 | 0.51– 2.61 | 0.724 |
| Non-reactive | 73 | 18 (24.7) | 1 | |||
| Address | Urban | 85 | 16 (18.8) | 2.02 | 0.89– 4.59 | 0.092 |
| Rural | 47 | 15 (31.9) | 1 | |||
| Province | Southern | 54 | 13 (24.1) | 0.95 | 0.42–2.14 | 0.894 |
| Eastern | 78 | 18 (23.1) | 1 | |||
| Treatment History | Previously treated New | 47 | 28 (59.6) | 40.3 | 11.1–146.0 | 0.001 |
| 85 | 3 (3.5) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monde, N.; Munyeme, M.; Chongwe, G.; Wensman, J.J.; Zulu, M.; Siziya, S.; Tembo, R.; Siame, K.K.; Shambaba, O.; Malama, S. First and Second-Line Anti-Tuberculosis Drug-Resistance Patterns in Pulmonary Tuberculosis Patients in Zambia. Antibiotics 2023, 12, 166. https://doi.org/10.3390/antibiotics12010166
Monde N, Munyeme M, Chongwe G, Wensman JJ, Zulu M, Siziya S, Tembo R, Siame KK, Shambaba O, Malama S. First and Second-Line Anti-Tuberculosis Drug-Resistance Patterns in Pulmonary Tuberculosis Patients in Zambia. Antibiotics. 2023; 12(1):166. https://doi.org/10.3390/antibiotics12010166
Chicago/Turabian StyleMonde, Ngula, Musso Munyeme, Gershom Chongwe, Jonas Johansson Wensman, Mildred Zulu, Seter Siziya, Rabecca Tembo, Kabengele K. Siame, Obi Shambaba, and Sydney Malama. 2023. "First and Second-Line Anti-Tuberculosis Drug-Resistance Patterns in Pulmonary Tuberculosis Patients in Zambia" Antibiotics 12, no. 1: 166. https://doi.org/10.3390/antibiotics12010166
APA StyleMonde, N., Munyeme, M., Chongwe, G., Wensman, J. J., Zulu, M., Siziya, S., Tembo, R., Siame, K. K., Shambaba, O., & Malama, S. (2023). First and Second-Line Anti-Tuberculosis Drug-Resistance Patterns in Pulmonary Tuberculosis Patients in Zambia. Antibiotics, 12(1), 166. https://doi.org/10.3390/antibiotics12010166