

Redo DAIR: The Game Is Seldom Worth the Candle

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Definitions & Criteria
- -
- Demographic & comorbidity risk factors: age, gender, American Society of anesthesiologists (ASA) classification, BMI (body mass index), Charlson’s comorbidity score, diabetes, immunodepression, renal or hepatic disease, anticoagulant or antiaggregant treatment and alcohol or tobacco abuse.
- -
- Surgical predictors: indication for the IS (osteoarthritis [OA]/other), involved joint (hip/knee), type of prosthesis (primary/revision), and use of cement for implant fixation. In regard to the debridement, the time elapsed from the IS (EAPJI), from the onset of symptoms (LAPJI) and between the first and second DAIR procedure was measured. A record was also made of whether any mobile prosthetic components were revised.
- -
- Clinical & laboratory findings: fever > 38°, drainage from the wound, culture-proven wound infection, presence of hematoma and/or fistulae. Laboratory parameters included C-reactive protein (CRP) levels, expressed in mg/dL, and white blood count (WBC) expressed in ×109/L. The measurements analyzed were those taken closest in time to the DAIR procedure.
- -
- Microbiology: tissue cultures, sonication and blood cultures. Microorganisms present were identified during the DAIR procedure, analyzing the number of positive cultures and any changes in the microbiological pattern between the first and second debridements. Cases where more than two different microorganisms were involved were classified as polymicrobial. S. lugdunensis was not considered part of the coagulase-negative staphylococcus (CoNS) group given its differential pathogenic behavior.
2.2. Diagnostic & Treatment
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
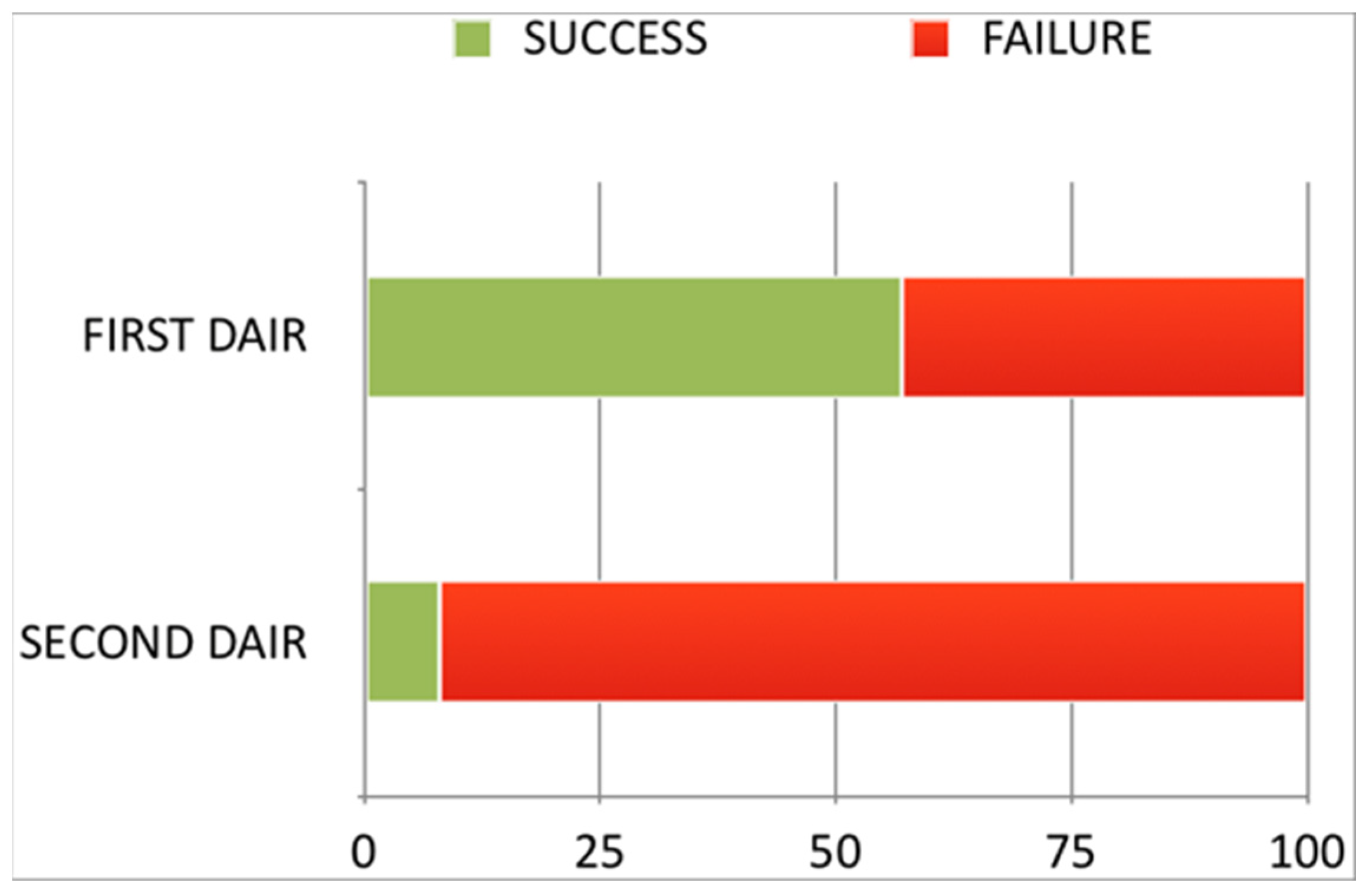
3.2. Success Rate of the Second DAIR Procedure
3.3. Differences between the Single-DAIR and the Second-DAIR Groups
3.4. Final Status Following Single vs. Repeat-DAIR
4. Discussion
5. Conclusions
- -
- Following an initial failed DAIR, a second DAIR has a low likelihood of success.
- -
- After a second failed DAIR, the patients’ final prognosis is likely to be unfavorable.
- -
- If an initial DAIR fails, it is advisable to switch to a prosthetic revision strategy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Argenson, J.N.; Arndt, M.; Babis, G.; Battenberg, A.; Budhiparama, N.; Catani, F.; Chen, F.; de Beaubien, B.; Ebied, A.; Esposito, S.; et al. Hip and Knee Section, Treatment, Debridement and Retention of Implant: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2018, 34, S399–S419. [Google Scholar] [CrossRef] [PubMed]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R.; Infectious Diseases Society of America. Infectious Diseases Society of America. Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cobo, J.; Miguel, L.G.S.; Euba, G.; Rodríguez, D.; García-Lechuz, J.; Riera, M.; Falgueras, L.; Palomino, J.; Benito, N.; del Toro, M.; et al. Early prosthetic joint infection: Outcomes with debridement and implant retention followed by antibiotic therapy. Clin. Microbiol. Infect. 2011, 17, 1632–1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duque, A.F.; Post, Z.D.; Lutz, R.W.; Orozco, F.R.; Pulido, S.H.; Ong, A.C. Is There Still a Role for Irrigation and Debridement With Liner Exchange in Acute Periprosthetic Total Knee Infection? J. Arthroplast. 2017, 32, 1280–1284. [Google Scholar] [CrossRef] [PubMed]
- Fehring, T.K.; Odum, S.M.; Berend, K.R.; Jiranek, W.A.; Parvizi, J.; Bozic, K.J.; Della Valle, C.J.; Gioe, T.J. Failure of Irrigation and Débridement for Early Postoperative Periprosthetic Infection. Clin. Orthop. Relat. Res. 2013, 471, 250–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tornero, E.; Morata, L.; Martínez-Pastor, J.; Bori, G.; Climent, C.; García-Velez, D.; García-Ramiro, S.; Bosch, J.; Mensa, J.; Soriano, A. KLIC-score for predicting early failure in prosthetic joint infections treated with debridement, implant retention and antibiotics. Clin. Microbiol. Infect. 2015, 21, 786.e9–786.e17. [Google Scholar] [CrossRef] [Green Version]
- Urish, K.L.; Bullock, A.G.; Kreger, A.M.; Shah, N.B.; Jeong, K.; Rothenberger, S.D.; The Infected Implant Consortium. A Multicenter Study of Irrigation and Debridement in Total Knee Arthroplasty Periprosthetic Joint Infection: Treatment Failure Is High. J. Arthroplast. 2018, 33, 1154–1159. [Google Scholar] [CrossRef]
- Logoluso, N.; Drago, L.; Peccati, A.; Romanò, D.; Romanò, C. Role for Irrigation and Debridement in Periprosthetic Infections. J. Knee Surg. 2014, 27, 267–272. [Google Scholar] [CrossRef]
- Löwik, C.A.; Jutte, P.C.; Tornero, E.; Ploegmakers, J.J.; Knobben, B.A.; de Vries, A.J.; Zijlstra, W.P.; Dijkstra, B.; Soriano, A.; Wouthuyzen-Bakker, M. Predicting Failure in Early Acute Prosthetic Joint Infection Treated With Debridement, Antibiotics, and Implant Retention: External Validation of the KLIC Score. J. Arthroplast. 2018, 33, 2582–2587. [Google Scholar] [CrossRef]
- Löwik, C.A.M.; Parvizi, J.; Jutte, P.C.; Zijlstra, W.P.; Knobben, B.A.S.; Xu, C.; Goswami, K.; Belden, K.A.; Sousa, R.; Carvalho, A.; et al. Debridement, Antibiotics, and Implant Retention Is a Viable Treatment Option for Early Periprosthetic Joint Infection Presenting More Than 4 Weeks After Index Arthroplasty. Clin. Infect. Dis. 2019, 71, 630–636. [Google Scholar] [CrossRef]
- Wouthuyzen-Bakker, M.; Sebillotte, M.; Lomas, J.; Taylor, A.; Palomares, E.B.; Murillo, O.; Parvizi, J.; Shohat, N.; Reinoso, J.C.; Sánchez, R.E.; et al. Clinical outcome and risk factors for failure in late acute prosthetic joint infections treated with debridement and implant retention. J. Infect. 2018, 78, 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shohat, N.; Goswami, K.; Tan, T.L.; Yayac, M.; Soriano, A.; Sousa, R.; Wouthuyzen-Bakker, M.; Parvizi, J.; On behalf of the ESCMID Study Group of Implant Associated Infections (ESGIAI) and the Northern Infection Network of Joint Arthroplasty (NINJA). 2020 Frank Stinchfield Award: Identifying who will fail following irrigation and debridement for prosthetic joint infection. Bone Jt. J. 2020, 102, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Durbhakula, S.M.; Czajka, J.; Fuchs, M.D.; Uhl, R.L. Antibiotic-loaded articulating cement spacer in the 2-stage exchange of infected total knee arthroplasty. J. Arthroplast. 2004, 19, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Haleem, A.A.; Berry, D.J.; Hanssen, A.D. The Chitranjan Ranawat Award: Mid-Term to Long-Term Followup of Two-stage Reimplantation for Infected Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2004, 428, 35–39. [Google Scholar] [CrossRef]
- Sabry, F.Y.; Buller, L.; Ahmed, S.; Klika, A.K.; Barsoum, W.K. Preoperative Prediction of Failure Following Two-Stage Revision for Knee Prosthetic Joint Infections. J. Arthroplast. 2014, 29, 115–121. [Google Scholar] [CrossRef]
- Wouthuyzen-Bakker, M.; Löwik, C.A.; Ploegmakers, J.J.; Knobben, B.A.; Dijkstra, B.; de Vries, A.J.; Mithoe, G.; Kampinga, G.; Zijlstra, W.P.; Jutte, P.C. A Second Surgical Debridement for Acute Periprosthetic Joint Infections Should Not Be Discarded. J. Arthroplast. 2020, 35, 2204–2209. [Google Scholar] [CrossRef]
- Vilchez, F.; Martínez-Pastor, J.; García-Ramiro, S.; Bori, G.; Maculé, F.; Sierra, J.; Font, L.; Mensa, J.; Soriano, A. Outcome and predictors of treatment failure in early post-surgical prosthetic joint infections due to Staphylococcus aureus treated with debridement. Clin. Microbiol. Infect. 2011, 17, 439–444. [Google Scholar] [CrossRef] [Green Version]
- Lizaur-Utrilla, A.; Gonzalez-Parreño, S.; Gil-Guillen, V.; Lopez-Prats, F. Debridement with prosthesis retention and antibiotherapy vs. two-stage revision for periprosthetic knee infection within 3 months after arthroplasty: A case–control study. Clin. Microbiol. Infect. 2015, 21, 851.e11–851.e17. [Google Scholar] [CrossRef] [Green Version]
- Triantafyllopoulos, G.; Poultsides, L.A.; Zhang, W.; Sculco, P.K.; Ma, Y.; Sculco, T.P. Multiple Irrigation and Debridements for Periprosthetic Joint Infections: Facing a Necessity or Just Prolonging the Inevitable? J. Arthroplast. 2015, 31, 219–224. [Google Scholar] [CrossRef]
- Sherrell, C.J.; Fehring, T.K.; Odum, S.; Hansen, E.; Zmistowski, B.; Dennos, A.; Kalore, N. The Chitranjan Ranawat Award: Fate of Two-stage Reimplantation After Failed Irrigation and Débridement for Periprosthetic Knee Infection. Clin. Orthop. Relat. Res. 2011, 469, 18–25. [Google Scholar] [CrossRef]
- Gardner, J.; Gioe, T.J.; Tatman, P. Can This Prosthesis Be Saved?: Implant Salvage Attempts in Infected Primary TKA. Clin. Orthop. Relat. Res. 2011, 469, 970–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lizaur-Utrilla, A.; Asensio-Pascual, A.; Gonzalez-Parreño, S.; Miralles-Muñoz, F.A.; Lopez-Prats, F.A. Negative impact of prior debridement on functional outcome of subsequent two-stage revision for early knee periprosthetic infection. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2309–2315. [Google Scholar] [CrossRef] [PubMed]
- Brimmo, O.; Ramanathan, D.; Schiltz, N.K.; Pillai, A.L.P.C.; Klika, A.K.; Barsoum, W.K. Irrigation and Debridement Before a 2-Stage Revision Total Knee Arthroplasty Does Not Increase Risk of Failure. J. Arthroplast. 2015, 31, 461–464. [Google Scholar] [CrossRef] [Green Version]
- Nodzo, S.R.; Boyle, K.K.; Nocon, A.A.; Henry, M.W.; Mayman, D.J.; Westrich, G.H. The Influence of a Failed Irrigation and Debridement on the Outcomes of a Subsequent 2-Stage Revision Knee Arthroplasty. J. Arthroplast. 2017, 32, 2508–2512. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, Ö.; Özdemir, M.; Turgut, M.C.; Altay, M. The Fate of Failed Debridement, Antibiotics, and Implant Retention in Infected Knee Arthroplasties: Nothing to Lose. Cureus 2021, 13, e18946. [Google Scholar] [CrossRef]
- Kim, K.; Zhu, M.; Cavadino, A.; Munro, J.T.; Young, S.W. Failed Debridement and Implant Retention Does Not Compromise the Success of Subsequent Staged Revision in Infected Total Knee Arthroplasty. J. Arthroplast. 2019, 34, 1214–1220.e1. [Google Scholar] [CrossRef]
- Backstein, D.; Mont, M.; Krueger, C.; Browne, J.; Krebs, V.; Mason, J.B.; Taunton, M.; Callaghan, J. Balancing Simplicity With Doing No Harm: The Case for Repeat DAIR Procedures. J. Arthroplast. 2020, 35, 1962–1963. [Google Scholar] [CrossRef]
- McNally, M.; Sousa, R.; Wouthuyzen-Bakker, M.; Chen, A.F.; Soriano, A.; Vogely, H.C.; Clauss, M.; Higuera, C.A.; Trebše, R. The EBJIS definition of periprosthetic joint infection. Bone Jt. J. 2021, 103, 18–25. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 1 April 2022).
- McQuivey, K.S.; Bingham, J.; Chung, A.; Clarke, H.; Schwartz, A.; Pollock, J.R.; Beauchamp, C.; Spangehl, M.J. The Double DAIR: A 2-Stage Debridement with Prosthesis-Retention Protocol for Acute Periprosthetic Joint Infections. JBJS Essent. Surg. Tech. 2021, 11, e19.00071. [Google Scholar] [CrossRef]
- Estes, C.S.; Beauchamp, C.P.; Clarke, H.D.; Spangehl, M.J. A Two-stage Retention Débridement Protocol for Acute Periprosthetic Joint Infections. Clin. Orthop. Relat. Res. 2010, 468, 2029–2038. [Google Scholar] [CrossRef]
- Chung, A.S.; Niesen, M.C.; Graber, T.J.; Schwartz, A.J.; Beauchamp, C.P.; Clarke, H.D.; Spangehl, M.J. Two-Stage Debridement With Prosthesis Retention for Acute Periprosthetic Joint Infections. J. Arthroplast. 2019, 34, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Antonios, J.K.; Bozic, K.J.; Clarke, H.D.; Spangehl, M.J.; Bingham, J.S.; Schwartz, A.J. Cost-effectiveness of Single vs Double Debridement and Implant Retention for Acute Periprosthetic Joint Infections in Total Knee Arthroplasty: A Markov Model. Arthroplast. Today 2021, 11, 187–195. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Data | Joint | N | Success (%) |
|---|---|---|---|---|
| Vilchez et al. [17] | 2010 | Hip & Knee | 8 | 25 |
| Lizaur et al. [18] | 2015 | Knee | 24 | 0 |
| Triantafyllopoulos et al. [19] | 2015 | Hip & Knee | 15 | 53.3 |
| Wouthuyzen-Bakker et al. [16] | 2020 | Hip & Knee | 144 | 74.3 |
| Demographics & Comorbidities | ||
|---|---|---|
| Age | Mean (SD) | 67.6 (11.8) |
| min ≤ med ≤ max | 16 ≤ 69 ≤ 85 | |
| IQR(CV) | 17 (0.2) | |
| Gender | Male n (%) | 56 (66.7%) |
| BMI (Kg/m2) | Mean (SD) | 30.7 (5.8) |
| min ≤ med ≤ max | 19 ≤ 30 ≤ 51 | |
| IQR (CV) | 7 (0.2) | |
| ASA score | I, n (%) | 9 (10.7) |
| II, n (%) | 43 (51.2) | |
| III, n (%) | 30 (35.7) | |
| IV, n (%) | 2 (2.4) | |
| Charlson score | 0–3 n (%) | 32 (38.1) |
| 4 or more, n (%) | 52 (61.9) | |
| Surgical-related factors | ||
| Type of surgery n (%) | THA | 32 (38.1) |
| TKA | 35 (41.7) | |
| RTHA | 15 (17.9) | |
| RTKA | 2 (2.4) | |
| Cemented prosthesis | Yes n (%) | 41 (48.8) |
| PJI & DAIR variables | ||
| Type of PJI | EAPJI n (%) | 72 (85.7) |
| LAPJI n (%) | 12 (14.3) | |
| Mobile components exchange | Yes n (%) | 44 (52.4) |
| Time from index surgery to DAIR (days) for EAPJI | Mean (SD) | 37 (22) |
| min ≤ med ≤ max | 8 ≤ 29.5 ≤ 88 | |
| IQR (CV) | 25.8 (0.6) | |
| Time from onset of symptoms to DAIR (days) for LAPJI | Mean (SD) | 8.77 (5.9) |
| min ≤ med ≤ max | 2 ≤ 8 ≤ 20 | |
| IQR (CV) | 5.2 (0.7) | |
| Time from first to second DAIR | Mean (SD) | 31.8 (29.4) |
| min ≤ med ≤ max | 6 ≤ 19 ≤ 90 | |
| IQR (CV) | 31.8 (0.9) | |
| Follow-up (months) | Mean (SD) | 67.4 (33.6) |
| Microbiology | ||
| Isolates n (%) | MSSA | 24 (28.6) |
| CoNS | 23 (27.4) | |
| Polymicrobial | 9 (10.7) | |
| Culture negative | 7 (8.3) | |
| S. dysgalactiae | 4 (4.8) | |
| C. acnes | 3 (3.6) | |
| S. lugdunensis | 3 (3.6) | |
| Corynebacterium spp. | 2 (2.4) | |
| P. aeruginosa | 2 (2.4) | |
| MRSA | 2 (2.4) | |
| Others | 5 (6) |
| Single DAIR, n = 72 | Second DAIR, n = 12 | p Value | |
|---|---|---|---|
| Demographics & comorbidities | |||
| Age (Median (IQR)) | 69 (60.75–77.00) | 62 (57.50–72.00) | 0.263 NonN |
| Gender = Male, n (%) | 24 (33.3) | 4 (33.3) | 1.000 |
| Charlson score; 4 or more, n (%) | 44 (61.1) | 8 (66.7) | 0.963 |
| ASA score (%) | 0.313 | ||
| I | 7 (9.7) | 2 (16.7) | |
| II | 39 (54.2) | 4 (33.3) | |
| III | 25 (34.7) | 5 (41.7) | |
| IV | 1 (1.4) | 1 (8.3) | |
| BMI (Kg/m2) (median (IQR)) | 31 (27.00–34.25) | 28.50 (26.00–31.25) | 0.161 NonN |
| Diabetes, n (%) | 17 (23.6) | 2 (16.7) | 0.873 |
| Inmunodepression, n (%) | 6 (8.3) | 0 (0.0) | 0.665 |
| Chronic renal failure, n (%) | 7 (9.7) | 2 (16.7) | 0.829 |
| Liver disease, n (%) | 0 (0.0) | 3 (25.0) | 0.001 |
| Antiplatelet drugs, n (%) | 13 (18.1) | 4 (33.3) | 0.406 |
| Anticoagulants drugs, n (%) | 7 (9.7) | 2 (16.7) | 0.829 |
| Smoking, n (%) | 35 (48.6) | 5 (41.7) | 0.894 |
| Alcohol, n (%) | 15 (20.8) | 2 (16.7) | 1.000 |
| Surgical related factors | |||
| IS Indication other than OA, n (%) | 20 (27.8) | 8 (66.7) | 0.021 |
| Implant debrided, n (%) | 0.042 | ||
| THA | 26 (36.1) | 6 (50.0) | 0.551 |
| TKA | 34 (47.2) | 1 (8.3) | 0.027 |
| RTHA | 11 (15.3) | 4 (33.3) | 0.269 |
| RTKA | 1 (1.4) | 1 (8.3) | 0.661 |
| PJI & DAIR variables | |||
| Cemented prosthesis, n (%) | 48 (52.8) | 3 (25.0) | 0.141 |
| Type of PJI: LAPJI, n (%) | 9 (12.5) | 3 (25.0) | 0.484 |
| Time from IS to 1st DAIR (days) (median (IQR)) for EAPJI | 29 (21.50–42.50) | 44 (34–72) | 0.053 NonN |
| Time from clinical onset to 1st DAIR (days) (median (IQR)) for LAPJI | 8 (4–8) | 9 (8.50–14.50) | 0.157 NonN |
| Mobile parts exchange, n (%) | 40 (55.6) | 4 (33.3) | 0.265 |
| Clinical & Laboratory findings | |||
| Wound drainage, n (%) | 39 (54.2) | 9 (75.0) | 0.301 |
| Skin infection, n (%) | 28 (38.9) | 4 (33.3) | 0.963 |
| Hematoma, n (%) | 24 (33.3) | 5 (41.7) | 0.815 |
| Draining sinus tract | 27(37.5) | 5 (41.7) | 1.000 |
| Fever > 38°, n (%) | 20 (27.8) | 8 (66.7) | 0.021 |
| Serum CRP mg/dL (median (IQR)) | 6.75 (3–14.53) | 13.50 (3.25–26.17) | 0.424 NonN |
| WBC × 109/L (median (IQR)) | 8.05 (6.57–10.53) | 9.10 (5.50–13.22) | 0.818 NonN |
| Microbiology | |||
| Positive blood cultures n (%) | 5 (6.9) | 0 (0.0) | 0.778 |
| Isolated pathogens, n (%) | 0.221 | ||
| CoNS | 22 (30.6) | 1 (8.3) | |
| Corynebacterium spp. | 2 (2.8) | 0 (0.0) | |
| Culture negative | 6 (8.3) | 1 (8.3) | |
| E. faecalis | 0 (0.0) | 1 (8.3) | |
| E. coli | 1 (1.4) | 0 (0.0) | |
| L. monocytogenes | 1 (1.4) | 0 (0.0) | |
| C. acnes | 3 (4.2) | 0 (0.0) | |
| P. aeruginosa | 2 (2.8) | 0 (0.0) | |
| Polymicrobial | 7 (9.7) | 2 (16.7) | |
| S. pneumoniae | 1 (1.4) | 0 (0.0) | |
| S. dysgalactiae | 3 (4.2) | 1 (8.3) | |
| S. lugdunensis | 2 (2.8) | 1 (8.3) | |
| MRSA | 2 (2.8) | 0 (0.0) | |
| MSSA | 20 (27.8) | 4 (33.3) | |
| S. marcesens | 0 (0.0) | 1 (8.3) | |
| % of positive cultures (median (IQR)) | 60 (33–100) | 100 (66.25–100) | 0.129 NonN |
| Cultures positive 100%, n (%) | 24 (33.3) | 7 (58.3) | 0.181 |
| Single DAIR Failures (n = 24) | Second DAIR Failures (n = 11) | |
|---|---|---|
| Free n (%) (95%CI) | 10 (41.2%) (22–63) | 0 (0–28) |
| SAT n (%) (95%CI) | 6 (25%) (10–47) | 6 (55%) (23–83) |
| Resection or Fusion surgery n (%) (95%CI) | 3 (12%) (3–32) | 0 (0–28) |
| Recurrent infection n (%) (95%CI) | 5 (21%) (7–42) | 5 (45%) (17–77) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sancho, I.; Otermin-Maya, I.; Gutiérrez-Dubois, J.; Aláez, I.; Librero, J.; Portillo, M.E.; Hidalgo-Ovejero, Á. Redo DAIR: The Game Is Seldom Worth the Candle. Antibiotics 2023, 12, 18. https://doi.org/10.3390/antibiotics12010018
Sancho I, Otermin-Maya I, Gutiérrez-Dubois J, Aláez I, Librero J, Portillo ME, Hidalgo-Ovejero Á. Redo DAIR: The Game Is Seldom Worth the Candle. Antibiotics. 2023; 12(1):18. https://doi.org/10.3390/antibiotics12010018
Chicago/Turabian StyleSancho, Ignacio, Iñaki Otermin-Maya, Jorge Gutiérrez-Dubois, Ignacio Aláez, Julián Librero, Maria Eugenia Portillo, and Ángel Hidalgo-Ovejero. 2023. "Redo DAIR: The Game Is Seldom Worth the Candle" Antibiotics 12, no. 1: 18. https://doi.org/10.3390/antibiotics12010018
APA StyleSancho, I., Otermin-Maya, I., Gutiérrez-Dubois, J., Aláez, I., Librero, J., Portillo, M. E., & Hidalgo-Ovejero, Á. (2023). Redo DAIR: The Game Is Seldom Worth the Candle. Antibiotics, 12(1), 18. https://doi.org/10.3390/antibiotics12010018