
Fluoroquinolones Are Useful as Directed Treatment for Complicated UTI in a Setting with a High Prevalence of Quinolone-Resistant Microorganisms

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
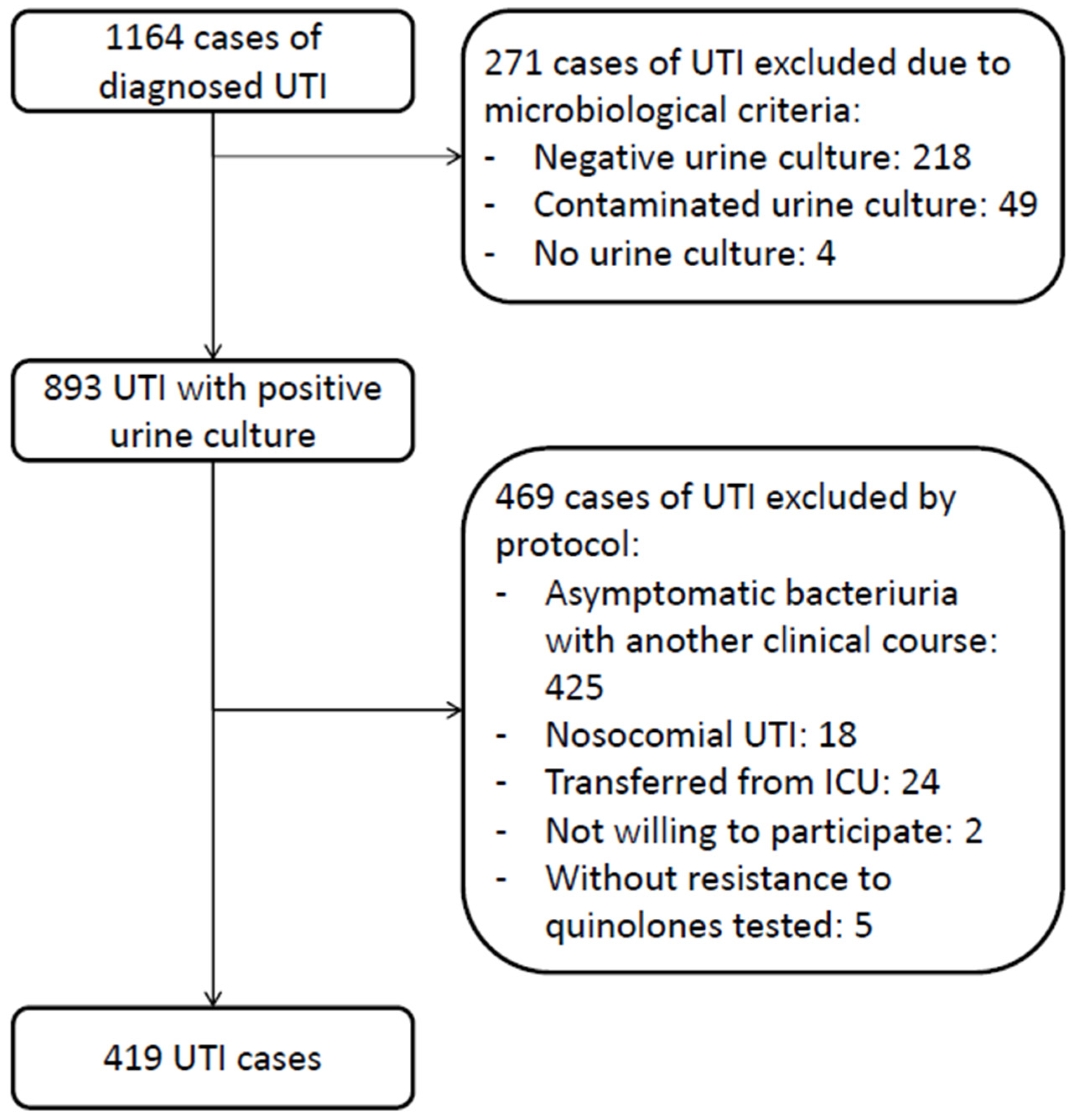
2.1. Patient Selection
2.2. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wagenlehner, F.M.E.; Bjerklund Johansen, T.E.; Cai, T.; Koves, B.; Kranz, J.; Pilatz, A.; Tandogdu, Z. Epidemiology, definition and treatment of complicated urinary tract infections. Nat. Rev. Urol. 2020, 17, 586–600. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, 103–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, D.C.; Wolfson, J.S. Fluoroquinolone Antimicrobial Agents. N. Engl. J. Med. 1991, 324, 384–394. [Google Scholar] [CrossRef]
- Sandberg, T.; Skoog, G.; Hermansson, A.B.; Kahlmeter, G.; Kuylenstierna, N.; Lannergard, A.; Otto, G.; Settergren, B.; Ekman, G.S. Ciprofloxacin for 7 days versus 14 days in women with acute pyelonephritis: A randomised, open-label and double-blind, placebo-controlled, non-inferiority trial. Lancet 2012, 380, 484–490. [Google Scholar] [CrossRef]
- van Nieuwkoop, C.; van der Starre, W.E.; Stalenhoef, J.E.; van Aartrijk, A.M.; van der Reijden, T.J.K.; Vollaard, A.M.; Delfos, N.M.; van’t Wout, J.W.; Blom, J.W.; Spelt, I.C.; et al. Treatment duration of febrile urinary tract infection: A pragmatic randomized, double-blind, placebo-controlled non-inferiority trial in men and women. BMC Med. 2017, 15, 70. [Google Scholar] [CrossRef] [Green Version]
- Malik, S.; Mathur, A.G.; Salmani, M.F. Resistance to Ciprofloxacin in Urinary Tract Infection. J. Med. Acad. 2018, 1, 50–52. [Google Scholar] [CrossRef]
- Kim, E.S.; Hooper, D.C. Clinical importance and epidemiology of quinolone resistance. Infect. Chemother. 2014, 46, 226–238. [Google Scholar] [CrossRef] [Green Version]
- Jorgensen, S.; Zurayk, M.; Yeung, S.; Terry, J.; Dunn, M.; Nieberg, P. Emergency Department Urinary Antibiograms Differ by Specific Patient Group. J. Clin. Microbiol. 2017, 55, 2629–2636. [Google Scholar] [CrossRef] [Green Version]
- Redgrave, L.S.; Sutton, S.B.; Webber, M.A.; Piddock, L.J.V. Fluoroquinolone resistance: Mechanisms, impact on bacteria, and role in evolutionary success. Trends Microbiol. 2014, 22, 438–445. [Google Scholar] [CrossRef]
- Yoshida, H.; Bogaki, M.; Nakamura, M.; Yamanaka, L.M.; Nakamura, S. Quinolone resistance-determining region in the DNA gyrase gyrB gene of Escherichia coli. Antimicrob. Agents Chemother. 1991, 35, 1647–1650. [Google Scholar] [CrossRef]
- Hooper, D.C. Emerging mechanisms of fluoroquinolone resistance. Emerg. Infect. Dis. 2001, 7, 337–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killgore, K.M.; March, K.L.; Guglielmo, B.J. Risk factors for community-acquired ciprofloxacin-resistant Escherichia coli urinary tract infection. Ann. Pharmacother. 2004, 38, 1148–1152. [Google Scholar] [CrossRef] [PubMed]
- Mulder, M.; Kiefte-de Jong, J.C.; Goessens, W.H.F.; de Visser, H.; Hofman, A.; Stricker, B.H.; Verbon, A. Risk factors for resistance to ciprofloxacin in community-acquired urinary tract infections due to Escherichia coli in an elderly population. J. Antimicrob. Chemother. 2017, 72, 281–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, K.; Zhu, M.; Jia, Y.; Wang, J.; Cai, Y. Efficacy and safety of quinolones vs. other antimicrobials for the treatment of uncomplicated urinary tract infections in adults: A systematic review and meta-analysis. Int. Urogynecol. J. 2022, 33, 1103–1123. [Google Scholar] [CrossRef]
- FDA Drug Safety Communication: FDA Advises Restricting Fluoroquinolone Antibiotic Use for Certain Uncomplicated Infections; Warns about Disabling Side Effects That Can Occur Together. Available online: http://www.fda.gov/Drugs/DrugSafety/ucm500143.htm (accessed on 6 December 2022).
- Madrazo, M. Aplicación de los criterios de sepsis-3 en la infección urinaria. Ph.D.Thesis, Universitat de València, València, Spain, 2020. [Google Scholar]
- Esparcia, A.; Artero, A.; Eiros, J.M.; Balaguer, M.; Madrazo, M.; Alberola, J.; Nogueira, J.M. Influence of inadequate antimicrobial therapy on prognosis in elderly patients with severe urinary tract infections. Eur. J. Intern. Med. 2014, 25, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.D.; Kaye, K.S.; Stout, J.E.; McGarry, S.A.; Trivette, S.L.; Briggs, J.P.; Lamm, W.; Clark, C.; MacFarquhar, J.; Walton, A.L.; et al. Health care-associated bloodstream infections in adults: A reason to change the accepted definition of community-acquired infections. Ann. Intern. Med. 2002, 137, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Pallett, A.; Hand, K. Complicated urinary tract infections: Practical solutions for the treatment of multiresistant gram-negative bacteria. J. Antimicrob. Chemother. 2010, 65, iii25–iii33. [Google Scholar] [CrossRef] [Green Version]
- Kahlmeter, G.; Åhman, J.; Matuschek, E. Antimicrobial Resistance of Escherichia coli Causing Uncomplicated Urinary Tract Infections: A European Update for 2014 and Comparison with 2000 and 2008. Infect. Dis. Ther. 2015, 4, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, A.E.; Wagenlehner, F.M.E.; Mulgirigama, A.; Twynholm, M. Escherichia coli resistance to fluoroquinolones in community-acquired uncomplicated urinary tract infection in women: A systematic review. Antimicrob. Agents Chemother. 2020, 64, e00862-20. [Google Scholar] [CrossRef]
- Silva, A.; Costa, E.; Freitas, A.; Almeida, A. Revisiting the Frequency and Antimicrobial Resistance Patterns of Bacteria Implicated in Community Urinary Tract Infections. Antibiotics 2022, 11, 768. [Google Scholar] [CrossRef]
- Bischoff, S.; Walter, T.; Gerigk, M.; Ebert, M.; Vogelmann, R. Empiric antibiotic therapy in urinary tract infection in patients with risk factors for antibiotic resistance in a German emergency department. BMC Infect. Dis. 2018, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Maddali, N.; Cantin, A.; Koshy, S.; Eiting, E.; Fedorenko, M. Antibiotic prescribing patterns for adult urinary tract infections within emergency department and urgent care settings. Am. J. Emerg. Med. 2021, 45, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Kabbani, S.; Hersh, A.L.; Shapiro, D.J.; Fleming-Dutra, K.E.; Pavia, A.T.; Hicks, L.A. Opportunities to improve fluoroquinolone prescribing in the United States for adult ambulatory care visits. Clin. Infect. Dis. 2018, 67, 134–136. [Google Scholar] [CrossRef] [Green Version]
- Zhu, D.M.; Li, Q.H.; Shen, Y.; Zhang, Q. Risk factors for quinolone-resistant Escherichia coli infection: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2020, 9, 11. [Google Scholar] [CrossRef]
- Bonkat, G.; Bartoletti, R.; Bruyère, F.; Geerling, S.; Koves, B.; Schubert, S. EAU Guidelines on Urological Infections; European Association of Urology: 2022. Available online: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Urological-Infections-2022.pdf (accessed on 6 December 2022).
- Zilberberg, M.D.; Nathanson, B.H.; Sulham, K.; Shorr, A.F. Multiple antimicrobial resistance and outcomes among hospitalized patients with complicated urinary tract infections in the US, 2013–2018: A retrospective cohort study. BMC Infect. Dis. 2021, 21, 159. [Google Scholar] [CrossRef]
- Madrazo, M.; Esparcia, A.; López-Cruz, I.; Alberola, J.; Piles, L.; Viana, A.; Eiros, J.M.; Artero, A. Clinical impact of multidrug-resistant bacteria in older hospitalized patients with community-acquired urinary tract infection. BMC Infect. Dis. 2021, 21, 1232. [Google Scholar] [CrossRef]
- Peterson, J.; Kaul, S.; Khashab, M.; Fisher, A.C.; Kahn, J.B. A double-blind, randomized comparison of levofloxacin 750 mg once-daily for five days with ciprofloxacin 400/500 mg twice-daily for 10 days for the treatment of complicated urinary tract infections and acute pyelonephritis. Urology 2008, 71, 17–22. [Google Scholar] [CrossRef]


{kind=link}
| Total n 419 | ETQ n 27 | ETOA n 388 * | p | DTQ n 135 | DTOA n 273 ** | p | |
|---|---|---|---|---|---|---|---|
| Female, n (%) | 216 (51.6) | 14 (51.9) | 198 (51) | 0.934 | 67 (49.6) | 142 (52) | 0.650 |
| Age (years), median (IQR) | 79 (70–86) | 79 (71–85) | 79 (70–87) | 0.935 | 77 (67–86) | 79 (71–87) | 0.136 |
| Age ≥ 75 years, n (%) | 269 (64.2) | 18 (66.7) | 249 (64.2) | 0.794 | 77 (57) | 183 (67) | 0.048 |
| McCabe ≥ 2, n (%) | 294 (70.2) | 20 (74.1) | 271 (69.8) | 0.643 | 76 (56.3) | 207 (75.8) | <0.001 |
| Charlson ≥ 3, n (%) | 369 (88.1) | 23 (85.2) | 343 (88.4) | 0.616 | 115 (85.2) | 243 (89) | 0.267 |
| Barthel < 40, n (%) | 137 (32.7) | 10 (37) | 127 (32.7) | 0.646 | 29 (21.5) | 99 (36.3) | 0.002 |
| Comorbidities | |||||||
| Dementia, n (%) | 112 (26.7) | 8 (29.6) | 104 (26.8) | 0.749 | 28 (20.7) | 76 (27.8) | 0.122 |
| Diabetes mellitus, n (%) | 151 (36) | 13 (48.1) | 136 (35.1) | 0.170 | 46 (34.1) | 100 (36.6) | 0.612 |
| COPD, n (%) | 51 (12.2) | 3 (11.1) | 48 (12.4) | 0.847 | 15 (11.1) | 35 (12.8) | 0.620 |
| CKD, n (%) | 136 (32.5) | 10 (37) | 125 (32.2) | 0.605 | 37 (27.4) | 95 (34.8) | 0.133 |
| Cancer, n (%) | 88 (21) | 3 (11.1) | 83 (21.4) | 0.203 | 30 (22.2) | 55 (20.1) | 0.627 |
| Indwelling urinary catheter, n (%) | 81 (19.3) | 3 (11.1) | 77 (19.8) | 0.265 | 22 (16.3) | 58 (21.2) | 0.236 |
| HCA-UTI, n (%) | 227 (54.2) | 17 (63) | 208 (53.6) | 0.345 | 56 (41.5) | 163 (59.7) | 0.001 |
| Previous hospitalization, n (%) | 127 (30.3) | 7 (25.9) | 119 (31) | 0.604 | 28 (20.7) | 93 (34.1) | 0.006 |
| Previous antimicrobial therapy, n (%) | 192 (45.8) | 16 (59.3) | 174 (44.8) | 0.146 | 53 (39.3) | 133 (48.7) | 0.044 |
| Nursing home residence, n (%) | 27 (6.4) | 0 | 27 (7) | 0.156 | 2 (1.5) | 25 (9.2) | 0.003 |
| Prior exposure to quinolones, n (%) | 47 (11.2) | 3 (11.1) | 44 (11.3) | 0.971 | 8 (5.9) | 39 (14.3) | 0.016 |
| Clinical characteristics | |||||||
| APACHE II, median (IQR) | 11 (8–16) | 10 (8–12) | 11 (8–16) | 0.167 | 10 (8–14) | 11 (8–16) | 0.146 |
| Fever, n (%) | 329 (78.5) | 22 (81.5) | 304 (78.4) | 0.702 | 113 (83.7) | 207 (75.8) | 0.069 |
| RR ≥ 22, n (%) | 79 (18.9) | 3 (11.1) | 74 (19.1) | 0.301 | 24 (17.8) | 47 (17.3) | 0.901 |
| Altered mental status, n (%) | 169 (40.3) | 8 (29.6) | 159 (41.1) | 0.241 | 38 (28.1) | 122 (44.9) | 0.001 |
| SBP < 100, n (%) | 75 (17.9) | 3 (11.1) | 72 (18.6) | 0.328 | 24 (17.8) | 46 (16.9) | 0.827 |
| qSOFA ≥ 2, n (%) | 101 (24.1) | 5 (18.5) | 95 (24.5) | 0.483 | 23 (17) | 68 (24.9) | 0.072 |
| Sepsis (SOFA ≥ 2), n (%) | 175 (41.8) | 7 (25.9) | 166 (42.8) | 0.086 | 52 (38.5) | 113 (41.4) | 0.578 |
| Septic shock-3, n (%) | 38 (9.1) | 0 | 38 (9.8) | 0.088 | 9 (6.7) | 22 (8.1) | 0.618 |
| Albumin, median (IQR) | 3.3 (3–3.6) | 3.4 (3.1–3.5) | 3.3 (3–3.6) | 0.645 | 3.4 (3.1–3.6) | 3.3 (2.9–3.6) | 0.110 |
| Leukocytosis, median (IQR) | 13,100 (9300–18,100) | 13,200 (9400–14,100) | 13,100 (9300–18,400) | 0.646 | 13,500 (9400–17,900) | 12,700 (8900–18,000) | 0.363 |
| Polymicrobial UTI, n (%) | 36 (8.6) | 1 (3.7) | 35 (9) | 0.343 | 8 (5.9) | 26 (9.5) | 0.216 |
| MDR, n (%) | 148 (35.3) | 13 (48.1) | 135 (34.8) | 0.161 | 34 (25.2) | 110 (40.3) | 0.003 |
| BLEE, n (%) | 40 (9.5) | 4 (14.8) | 36 (9.3) | 0.346 | 3 (2.2) | 37 (13.6) | <0.001 |
| Bacteremia, positive/total blood cultures, n (%) | 90/236 (38.1) | 5/13 (38.5) | 84/221 (38) | 0.529 | 28/81 (34.6) | 58/148 (39.2) | 0.533 |
| IEAT, n (%) | 92 (22) | 8 (29.6) | 82 (21.1) | 0.300 | 13 (9.6) | 76 (27.8) | <0.001 |
| Outcomes | |||||||
| In-hospital mortality, n (%) | 32 (7.6) | 3 (11.1) | 29 (7.5) | 0.493 | 3 (2.2) | 18 (6.6) | 0.044 |
| 30-day mortality, n (%) | 47 (11.2) | 5 (18.5) | 42 (10.8) | 0.223 | 6 (4.4) | 30 (11) | 0.028 |
| Length of hospital stay (days), median (IQR) | 5 (3–7) | 5 (3–6) | 5 (3–7) | 0.571 | 5 (3–7) | 5 (3–7) | 0.328 |
| Resistance to Ciprofloxacin n 156 | Non-resistance to Ciprofloxacin n 263 | p | |
|---|---|---|---|
| Female, n (%) | 71 (45.5) | 145 (55.1) | 0.057 |
| Age (years), median (IQR) | 81 (74–87] | 77 (66–85) | 0.002 |
| Age ≥ 75 years, n (%) | 115 (73.7) | 154 (58.6) | 0.002 |
| McCabe ≥ 2, n (%) | 125 (80.1) | 169 (64.3) | 0.001 |
| Charlson ≥ 3, n (%) | 146 (93.6) | 223 (84.8) | 0.007 |
| Barthel < 40, n (%) | 68 (43.6) | 69 (26.2) | <0.001 |
| Comorbidities | |||
| Dementia, n (%) | 48 (30.8) | 64 (24.3) | 0.150 |
| Diabetes mellitus, n (%) | 62 (39.7) | 89 (33.8) | 0.224 |
| COPD, n (%) | 24 (15.4) | 27 (10.3) | 0.121 |
| CKD, n (%) | 66 (42.3) | 70 (26.6) | 0.001 |
| Cancer, n (%) | 35 (22.4) | 53 (20.2) | 0.579 |
| Indwelling urinary catheter, n (%) | 46 (29.5) | 35 (13.3) | <0.001 |
| Prior exposure to quinolones, n (%) | 35 (22.4) | 12 (4.6) | <0.001 |
| HCA-UTI, n (%) Previous hospitalization, n (%) Previous antimicrobial therapy, n (%) Nursing home residence, n (%) | 119 (76.3) 68 (43.6) 102 (65.4) 21 (13.5) | 108 (41.1) 59 (22.4) 90 (34.2) 6 (2.3) | <0.001 <0.001 <0.001 <0.001 |
| Severity scores | |||
| APACHE II, median (IQR) | 12 (8–17) | 11 (8–14) | 0.016 |
| qSOFA ≥ 2, n (%) | 45 (28.8) | 56 (21.3) | 0.081 |
| Sepsis (SOFA ≥ 2), n (%) | 65 (41.7) | 110 (41.8) | 0.975 |
| Septic shock-3, n (%) | 17 (10.9) | 21 (8) | 0.316 |
| Microbiological data | |||
| Polymicrobial UTI, n (%) | 19 (12.2) | 17 (6.5) | 0.044 |
| MDR, n (%) | 102 (65.4) | 46 (17.5) | <0.001 |
| ESBL, n (%) | 36 (23.1) | 4 (1.5) | <0.001 |
| Bacteremia, positive/total blood cultures, n (%) | 35/86 (40.7) | 55/150 (36.7) | 0.891 |
| Univariate Analysis p | OR (95% CI) | Multivariate Analysis p | OR (95% CI) | |
|---|---|---|---|---|
| Charlson ≥ 3 | 0.007 | 1.9 (1.1–3.5) | 0.866 | - |
| Age ≥ 75 years old | 0.002 | 1.6 (1.2–2.1) | 0.157 | |
| Barthel < 40 | <0.001 | 1.6 (1.3–2) | 0.064 | - |
| HCA-UTI | <0.001 | 2.7 (2–3.7) | <0.001 | 22 (12.4–31.7) |
| Previous use of quinolones | <0.001 | 2.7 (1.9–3.7) | <0.001 | 28.5 (14.2–42.9) |
| Indwelling catheter | <0.001 | 1.7 (1.4–2.2) | 0.091 | - |
| APACHE II ≥ 12 | 0.781 | 1.1 (0.6–1.8) | 0.807 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Artero, A.; López-Cruz, I.; Piles, L.; Alberola, J.; Eiros, J.M.; Salavert, S.; Madrazo, M. Fluoroquinolones Are Useful as Directed Treatment for Complicated UTI in a Setting with a High Prevalence of Quinolone-Resistant Microorganisms. Antibiotics 2023, 12, 183. https://doi.org/10.3390/antibiotics12010183
Artero A, López-Cruz I, Piles L, Alberola J, Eiros JM, Salavert S, Madrazo M. Fluoroquinolones Are Useful as Directed Treatment for Complicated UTI in a Setting with a High Prevalence of Quinolone-Resistant Microorganisms. Antibiotics. 2023; 12(1):183. https://doi.org/10.3390/antibiotics12010183
Chicago/Turabian StyleArtero, Arturo, Ian López-Cruz, Laura Piles, Juan Alberola, José María Eiros, Sofia Salavert, and Manuel Madrazo. 2023. "Fluoroquinolones Are Useful as Directed Treatment for Complicated UTI in a Setting with a High Prevalence of Quinolone-Resistant Microorganisms" Antibiotics 12, no. 1: 183. https://doi.org/10.3390/antibiotics12010183
APA StyleArtero, A., López-Cruz, I., Piles, L., Alberola, J., Eiros, J. M., Salavert, S., & Madrazo, M. (2023). Fluoroquinolones Are Useful as Directed Treatment for Complicated UTI in a Setting with a High Prevalence of Quinolone-Resistant Microorganisms. Antibiotics, 12(1), 183. https://doi.org/10.3390/antibiotics12010183