
Impact of Antibiotic Prophylaxis on Surgical Site Infections in Cardiac Surgery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions
2.3. Selection of Antibiotic Prophylaxis and Protocol of Administration
2.4. Objectives
2.5. Data Collection and Ethics
2.6. Patient Management
2.7. Statistical Analysis
3. Results
3.1. Homogeneity of the Cohort
3.2. Patient Characteristics Based on the Type of Antibiotic Prophylaxis
3.3. Relationship between Antibiotic Prophylaxis and SSI in the General Population
3.4. Microbiological Characteristics of Patients According to the Type of SSI
3.5. Relationship between Antibiotic Prophylaxis and SSI in Propensisty Score Analsysis
3.6. Relationships between Antibiotic Prophylaxis and SSI in a Sensitivity Analysis Excluding Active Infective Endocarditis
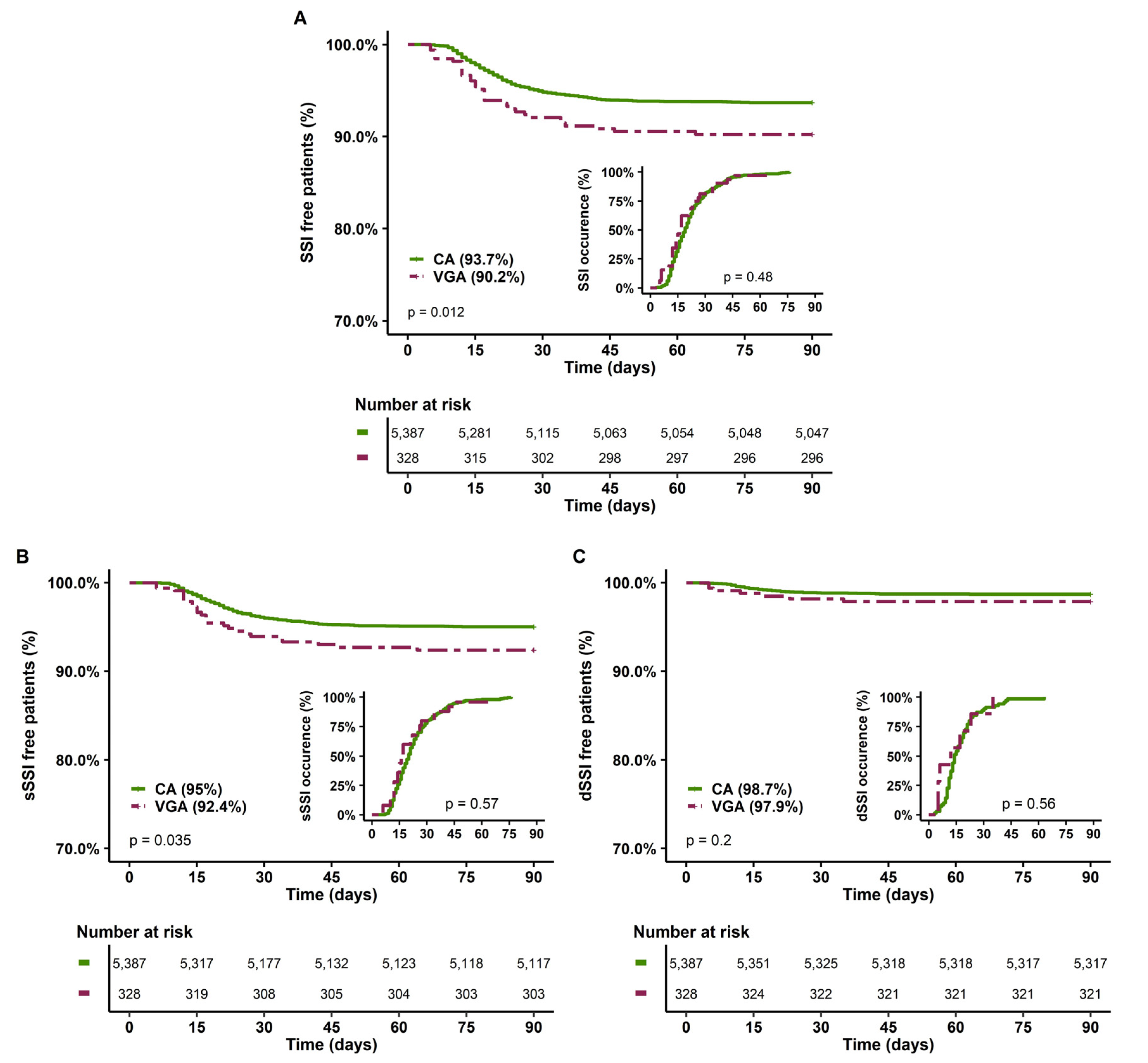
3.7. Relationships between Antibiotic Prophylaxis and SSI in a Sensitivity Analysis Restricted to CABG
4. Discussion
4.1. Summary of the Main Results
4.2. Comparison with Other Studies and Physiopathological Hypotheses
4.2.1. SSI Occurrence According to the Type of Antibiotic Prophylaxis
4.2.2. Prevention of Gram-Negative SSI by Gentamicin
4.2.3. Timing of Antibiotic Prophylaxis and Role of Gentamicin
4.3. Limits and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Item No | Recommendation | Page | |
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | 1 |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | 2 | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 2 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 2, 3 |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | 2 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | 2 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up | 2 |
| (b) For matched studies, give matching criteria and number of exposed and unexposed | - | ||
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | 2, 3 |
| Data sources/ measurement | 8 | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | 3, 4 |
| Bias | 9 | Describe any efforts to address potential sources of bias | 3, 4 |
| Study size | 10 | Explain how the study size was arrived at | 3, 4 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | 3, 4 |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | 3, 4 |
| (b) Describe any methods used to examine subgroups and interactions | 3, 4 | ||
| (c) Explain how missing data were addressed | 3, 4 | ||
| (d) If applicable, explain how loss to follow-up was addressed | - | ||
| (e) Describe any sensitivity analyses | 3, 4 | ||
| Results | |||
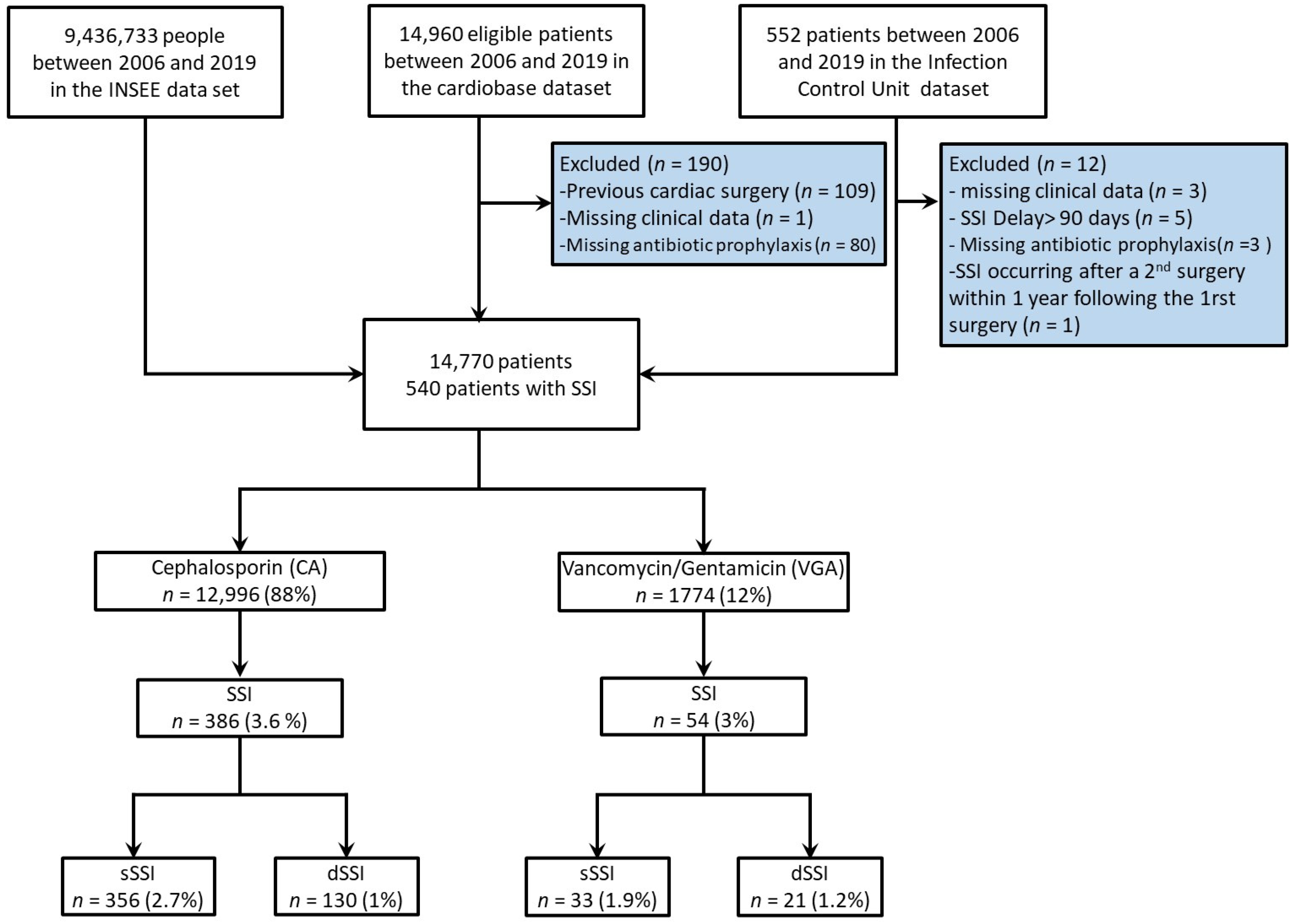
| Participants | 13 | (a) Report numbers of individuals at each stage of study—e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | 4 and Figure 1 |
| (b) Give reasons for non-participation at each stage | Figure 1 | ||
| (c) Consider use of a flow diagram | Figure 1 | ||
| Descriptive data | 14 | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders | Table 1 |
| (b) Indicate number of participants with missing data for each variable of interest | Table 1 | ||
| (c) Summarise follow-up time (e.g., average and total amount) | Supplementary Figure S1 | ||
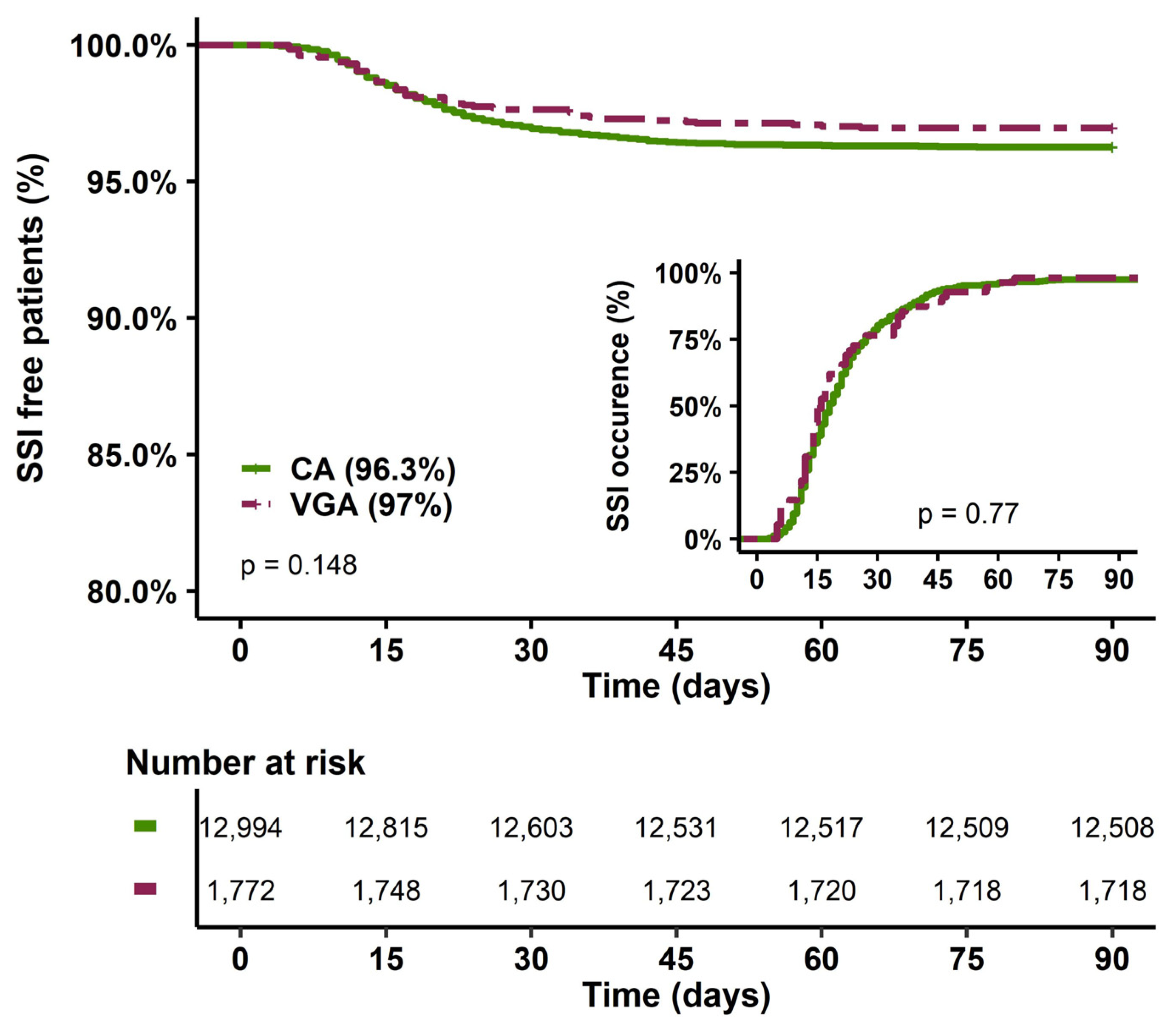
| Outcome data | 15 | Report numbers of outcome events or summary measures over time | Figure 2 |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included | Table 2 |
| (b) Report category boundaries when continuous variables were categorized | yes | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | No | ||
| Other analyses | 17 | Report other analyses done—e.g., analyses of subgroups and interactions, and sensitivity analyses | Table 4 and Table S2 |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | 12 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 13 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 12, 13 |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | 14 |
| Other information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 14 |
References
- Aminov, R.I. A Brief History of the Antibiotic Era: Lessons Learned and Challenges for the Future. Front. Microbio. 2010, 1, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firor, W.M.; Jonas, A.F. The Use of Sulfanilylguanidine in Surgical Patients. Ann. Surg. 1941, 114, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Altemeier, W.A.; Culbertson, W.R.; Veto, M. Prophylactic Antibiotic Therapy. AMA Arch. Surg. 1955, 71, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Uva, M.; Head, S.J.; Milojevic, M.; Collet, J.-P.; Landoni, G.; Castella, M.; Dunning, J.; Gudbjartsson, T.; Linker, N.J.; Sandoval, E.; et al. 2017 EACTS Guidelines on Perioperative Medication in Adult Cardiac Surgery. Eur. J. Cardio-Thorac. Surg. 2018, 53, 5–33. [Google Scholar] [CrossRef] [Green Version]
- Ackah, J.K.; Neal, L.; Marshall, N.R.; Panahi, P.; Lloyd, C.; Rogers, L.J. Antimicrobial Prophylaxis in Adult Cardiac Surgery in the United Kingdom and Republic of Ireland. J. Infect. Prev. 2021, 22, 83–90. [Google Scholar] [CrossRef]
- Antibioprophylaxie en chirurgie et médecine interventionnelle (patients adultes)—La SFAR. Société Française d’Anesthésie et de Réanimation . 2018. Available online: https://sfar.org/mise-a-jour-de-la-rfe-antibioprophylaxie-2017/ (accessed on 8 December 2022).
- Finkelstein, R.; Rabino, G.; Mashiah, T.; Bar-El, Y.; Adler, Z.; Kertzman, V.; Cohen, O.; Milo, S. Surgical Site Infection Rates Following Cardiac Surgery: The Impact of a 6-Year Infection Control Program. Am. J. Infect. Control. 2005, 33, 450–454. [Google Scholar] [CrossRef]
- Bolon, M.K.; Morlote, M.; Weber, S.G.; Koplan, B.; Carmeli, Y.; Wright, S.B. Glycopeptides Are No More Effective than B-Lactam Agents for Prevention of Surgical Site Infection after Cardiac Surgery: A Meta-Analysis. Clin. Infect. Dis. 2004, 38, 1357–1363. [Google Scholar] [CrossRef]
- Kaye, K.S.; Devine, S.T.; Ford, K.D.; Anderson, D.J. Surgical Site Infection Prophylaxis Strategies for Cardiothoracic Surgery: A Decision-Analytic Model. Scand. J. Infect. Dis. 2012, 44, 948–955. [Google Scholar] [CrossRef] [Green Version]
- Bull, A.L.; Worth, L.J.; Richards, M.J. Impact of Vancomycin Surgical Antibiotic Prophylaxis on the Development of Methicillin-Sensitive Staphylococcus Aureus Surgical Site Infections: Report From Australian Surveillance Data (VICNISS). Ann. Surg. 2012, 256, 1089–1092. [Google Scholar] [CrossRef]
- Apellaniz, G.; Valdés, M.; Perez, R.; Martin, F.; Soria, F.; Garcia, A.; Gòmez, J.; Vicente, T. Comparison of the Effectiveness of Various Antibiotics in the Treatment of Methicillin-Susceptible Staphylococcus Aureus Experimental Infective Endocarditis. J. Chemother. 1991, 3, 91–97. [Google Scholar] [CrossRef]
- LaPlante, K.L.; Rybak, M.J. Impact of High-Inoculum Staphylococcus Aureus on the Activities of Nafcillin, Vancomycin, Linezolid, and Daptomycin, Alone and in Combination with Gentamicin, in an In Vitro Pharmacodynamic Model. Antimicrob. Agents Chemother. 2004, 48, 4665–4672. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.; Alaya, M.; Mallet, M.N.; Viviand, X.; Ennabli, K.; Said, R.; De Micco, P. Penetration of Vancomycin into Mediastinal and Cardiac Tissues in Humans. Antimicrob. Agents Chemother. 1994, 38, 396–399. [Google Scholar] [CrossRef] [Green Version]
- Lador, A.; Nasir, H.; Mansur, N.; Sharoni, E.; Biderman, P.; Leibovici, L.; Paul, M. Antibiotic Prophylaxis in Cardiac Surgery: Systematic Review and Meta-Analysis. J. Antimicrob. Chemother. 2012, 67, 541–550. [Google Scholar] [CrossRef] [Green Version]
- Garey, K.W. Timing of Vancomycin Prophylaxis for Cardiac Surgery Patients and the Risk of Surgical Site Infections. J. Antimicrob. Chemother. 2006, 58, 645–650. [Google Scholar] [CrossRef] [Green Version]
- Cotogni, P.; Barbero, C.; Passera, R.; Fossati, L.; Olivero, G.; Rinaldi, M. Violation of Prophylactic Vancomycin Administration Timing Is a Potential Risk Factor for Rate of Surgical Site Infections in Cardiac Surgery Patients: A Prospective Cohort Study. BMC Cardiovasc. Disord. 2017, 17, 73. [Google Scholar] [CrossRef] [Green Version]
- Saginur, R.; Croteau, D.; Bergeron, M.G. Comparative Efficacy of Teicoplanin and Cefazolin for Cardiac Operation Prophylaxis in 3027 Patients. J. Thorac. Cardiovasc. Surg. 2000, 120, 1120–1130. [Google Scholar] [CrossRef] [Green Version]
- Lemaignen, A.; Birgand, G.; Ghodhbane, W.; Alkhoder, S.; Lolom, I.; Belorgey, S.; Lescure, F.-X.; Armand-Lefevre, L.; Raffoul, R.; Dilly, M.-P.; et al. Sternal Wound Infection after Cardiac Surgery: Incidence and Risk Factors According to Clinical Presentation. Clin. Microbiol. Infect. 2015, 21, 674.e11–674.e18. [Google Scholar] [CrossRef] [Green Version]
- Centers for disease control and Prevention CDC/NHSN Surveillance Definitions for Specific Types of Infections. Natl. Healthc. Saf. Netw. 2022, 30.
- Lemaignen, A.; Armand-Lefevre, L.; Birgand, G.; Mabileau, G.; Lolom, I.; Ghodbane, W.; Dilly, M.-P.; Nataf, P.; Lucet, J.-C. Thirteen-Year Experience with Universal Staphylococcus Aureus Nasal Decolonization Prior to Cardiac Surgery: A Quasi-Experimental Study. J. Hosp. Infect. 2018, 100, 322–328. [Google Scholar] [CrossRef]
- Couffignal, C.; Amour, J.; Ait-Hamou, N.; Cholley, B.; Fellahi, J.-L.; Duval, X.; Costa De Beauregard, Y.; Nataf, P.; Dilly, M.-P.; Provenchère, S.; et al. Timing of β-Blocker Reintroduction and the Occurrence of Postoperative Atrial Fibrillation after Cardiac Surgery. Anesthesiology 2020, 132, 267–279. [Google Scholar] [CrossRef]
- Stuart, E.A.; Cole, S.R.; Bradshaw, C.P.; Leaf, P.J. The Use of Propensity Scores to Assess the Generalizability of Results from Randomized Trials: Use of Propensity Scores to Assess Generalizability. J. R. Stat. Soc. Ser. A 2011, 174, 369–386. [Google Scholar] [CrossRef] [PubMed]
- Sekhon, J.S. Multivariate and Propensity Score Matching Software with Automated Balance Optimization: The Matching Package for R. J. Stat. Soft. 2011, 42, 49. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.B.; Klopfer, S.O. Optimal Full Matching and Related Designs via Network Flows. J. Comput. Graph. Stat. 2006, 15, 609–627. [Google Scholar] [CrossRef] [Green Version]
- Greifer, N.; Stuart, E.A. Matching Methods for Confounder Adjustment: An Addition to the Epidemiologist’s Toolbox. Epidemiol Rev. 2022, 43, 118–129. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [Green Version]
- Branch-Elliman, W.; O’Brien, W.; Strymish, J.; Itani, K.; Wyatt, C.; Gupta, K. Association of Duration and Type of Surgical Prophylaxis With Antimicrobial-Associated Adverse Events. JAMA Surg. 2019, 154, 590. [Google Scholar] [CrossRef]
- Solomon, S.; Akeju, O.; Odumade, O.A.; Ambachew, R.; Gebreyohannes, Z.; Van Wickle, K.; Abayneh, M.; Metaferia, G.; Carvalho, M.J.; Thomson, K.; et al. Prevalence and Risk Factors for Antimicrobial Resistance among Newborns with Gram-Negative Sepsis. PLoS ONE 2021, 16, e0255410. [Google Scholar] [CrossRef]
- Fleischmann, W.A.; Greenwood-Quaintance, K.E.; Patel, R. In Vitro Activity of Plazomicin Compared to Amikacin, Gentamicin, and Tobramycin against Multidrug-Resistant Aerobic Gram-Negative Bacilli. Antimicrob. Agents Chemother. 2020, 64, e01711-19. [Google Scholar] [CrossRef]
- Kristich, C.J.; Rice, L.B.; Arias, C.A. Enterococcal Infection—Treatment and Antibiotic Resistance. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Gilmore, M.S., Clewell, D.B., Ike, Y., Shankar, N., Eds.; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014. [Google Scholar]
- Bourque, M.; Quintiliani, R.; Tilton, R.C. Synergism of Cefazolin-Gentamicin Against Enterococci. Antimicrob. Agents Chemother. 1976, 10, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Peel, T.; Astbury, S.; Cheng, A.C.; Paterson, D.; Buising, K.; Spelman, T.; Tran-Duy, A.; de Steiger, R.S. Multicentre Randomised Double-Blind Placebo Controlled Trial of Combination Vancomycin and Cefazolin Surgical Antibiotic Prophylaxis: The Australian Surgical Antibiotic Prophylaxis (ASAP) Trial. BMJ Open 2019, 9, e033718. [Google Scholar] [CrossRef] [Green Version]
- Steed, M.E.; Rybak, M.J. Ceftaroline: A New Cephalosporin with Activity Against Resistant Gram-Positive Pathogens. Pharmacotherapy 2010, 30, 375–389. [Google Scholar] [CrossRef]
- Ceftaroline: A New Cephalosporin with Activity Against Methicillin-Resistant Staphylococcus Aureus (MRSA). Clin. Med. Rev. Ther. 2011, 3, 1–17. [CrossRef] [Green Version]
- The Use of Ceftaroline as Surgical Prophylaxis in Surgery With Risk of MRSA Infection (PREVTAROLINE). 2014. Available online: https://clinicaltrials.gov/ct2/show/NCT02307006 (accessed on 28 December 2022).
- McGrath, B.J.; Kang, S.L.; Kaatz, G.W.; Rybak, M.J. Bactericidal Activities of Teicoplanin, Vancomycin, and Gentamicin Alone and in Combination against Staphylococcus Aureus in an in Vitro Pharmacodynamic Model of Endocarditis. Antimicrob. Agents Chemother. 1994, 38, 2034–2040. [Google Scholar] [CrossRef] [Green Version]
- Cottagnoud, P.; Cottagnoud, M.; Täuber, M.G. Vancomycin Acts Synergistically with Gentamicin against Penicillin-Resistant Pneumococci by Increasing the Intracellular Penetration of Gentamicin. Antimicrob. Agents Chemother. 2003, 47, 144–147. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Berriel-Cass, D.; Baran, J. Sternal Surgical-Site Infection Following Coronary Artery Bypass Graft Prevalence, Microbiology, and Complications During a 42-Month Period. Infect. Control Hosp. Epidemiol. 2004, 25, 468–471. [Google Scholar] [CrossRef]
- Heilmann, C.; Stahl, R.; Schneider, C.; Sukhodolya, T.; Siepe, M.; Olschewski, M.; Beyersdorf, F. Wound Complications after Median Sternotomy: A Single-Centre Study. Interact. CardioVascular Thorac. Surg. 2013, 16, 643–648. [Google Scholar] [CrossRef] [Green Version]
- Raja, S.G.; Rochon, M.; Jarman, J.W.E. Brompton Harefield Infection Score (BHIS): Development and Validation of a Stratification Tool for Predicting Risk of Surgical Site Infection after Coronary Artery Bypass Grafting. Int. J. Surg. 2015, 16, 69–73. [Google Scholar] [CrossRef]
- Brunet, A.; N’Guyen, Y.; Lefebvre, A.; Poncet, A.; Robbins, A.; Bajolet, O.; Saade, Y.; Ruggieri, V.G.; Rubin, S. Obesity and Preoperative Anaemia as Independent Risk Factors for Sternal Wound Infection After Coronary Artery Bypass Graft Surgery with Pedicled (Non-Skeletonized) Internal Mammary Arteries: The Role of Thoracic Wall Ischemia? VHRM 2020, 16, 553–559. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall n = 14,770 (100%) | Missing Value | CA n = 12,996 (88%) | VGA n = 1774 (12%) | p Value | |
|---|---|---|---|---|---|
| Demography | |||||
| Male | 10,225 (69) | 0 | 9153 (70) | 1072 (60) | <0.001 |
| Age (years) | 66(56–74) | 0 | 66 (56–74) | 64 (53–74) | <0.001 |
| 1st quartile < 56 years | 3692 (25) | 0 | 3163 (24) | 529 (30) | <0.001 |
| 2nd quartile (56, 65) years | 3693 (25) | 0 | 3262 (25) | 431 (24) | <0.001 |
| 3rd quartile (66–74) years | 3691 (25) | 0 | 3290 (25) | 401 (23) | |
| 4th quartile > 74 years | 3694 (25) | 0 | 3281 (25) | 413 (23) | |
| BMI (kg/m2) | 26.2 (23.6–29.4) | 101 | 26.2 (23.7,29.4) | 25.6 (22.8–29.1) | <0.001 |
| Obesity | 3275 (22) | 101 | 2906 (23) | 369 (21) | 0.127 |
| Medical history | |||||
| Smoking | 5299 (36) | 0 | 4651 (36) | 648 (37) | 0.542 |
| Arterial hypertension | 8675 (59) | 0 | 7733 (60) | 942 (53) | <0.01 |
| Diabetes mellitus | 4036 (27) | 0 | 3602 (28) | 434 (24) | 0.004 |
| Insulin-dependent diabetes | 1245 (8.4) | 0 | 1086 (8.4) | 159 (9.0) | 0.389 |
| Noninsulin-dependent diabetes | 2787 (19) | 0 | 2513 (19) | 274 (15) | <0.001 |
| Dyslipidaemia | 7432 (50) | 0 | 6717 (52) | 715 (40) | <0.001 |
| Chronic peripheral arterial insufficiency | 1801 (12) | 0 | 1600 (12) | 201 (11) | 0.236 |
| Stroke | 1333 (9.0) | 0 | 1055 (8.1) | 278 (16) | <0.001 |
| Cardiac insufficiency | 670 (4.5) | 0 | 555 (4.3) | 115 (6.5) | <0.001 |
| Ischaemic heart disease | 7388 (50) | 0 | 6819 (52) | 569 (32) | <0.001 |
| ESRD | 191 (1.3) | 0 | 130 (1.0) | 61 (3.4) | <0.001 |
| COPD | 1211 (8.2) | 0 | 1007 (7.7) | 204 (11) | <0.001 |
| Cirrhosis | 148 (1.0) | 0 | 108 (0.8) | 40 (2.3) | <0.001 |
| Preoperative data | |||||
| B-blocker | 8620 (58) | 0 | 7853 (60) | 767 (43) | <0.001 |
| ACE inhibitor | 7184 (49) | 0 | 6459 (50) | 725 (41) | <0.001 |
| Statins | 8474 (57) | 0 | 7711 (59) | 763 (43) | <0.001 |
| Antiplatelet agent | 8430 (57) | 0 | 7691 (59) | 739 (42) | <0.001 |
| Aortic regurgitation | 1472 (10.0) | 0 | 1096 (8.4) | 376 (21) | <0.001 |
| Mitral regurgitation | 1794 (12) | 0 | 1415 (11) | 379 (21) | <0.001 |
| Aortic Stenosis | 3664 (25) | 0 | 3266 (25) | 398 (22) | 0.014 |
| Mitral stenosis | 1038 (7.0) | 0 | 902 (6.9) | 136 (7.7) | 0.262 |
| Surgical emergency | 1100 (7.4) | 0 | 868 (6.7) | 232 (13) | <0.001 |
| Acute infective endocarditis | 759 (5.1) | 0 | 285 (2.2) | 474 (27) | <0.001 |
| Prior cardiac surgery | 1345 (9.1) | 0 | 1001 (7.7) | 344 (19) | <0.001 |
| Preoperative critical state | 542 (3.7) | 0 | 357 (2.7) | 185 (10) | <0.001 |
| MV | 259 (1.8) | 0 | 141 (1.1) | 118 (6.7) | <0.001 |
| Catecholamine | 312 (2.1) | 0 | 200 (1.5) | 112 (6.3) | <0.001 |
| AKI | 222 (1.5) | 0 | 118 (0.9) | 104 (5.9) | <0.001 |
| Haemoglobin (g/dL) | 13.4 (12.0–14.5) | 317 | 13.5 (12.3–14.6) | 12.2 (10.5–13.6) | <0.001 |
| Platelet count (G/L) | 220 (182–266) | 525 | 219 (182–264) | 226 (181–284) | <0.001 |
| Prothrombin ratio (%) | 93 (82,100) | 770 | 94 (83–100) | 88 (75–100) | <0.001 |
| Creatinin (µg/L) | 88 (75,107) | 250 | 88 (75–106) | 91 (75–120) | <0.001 |
| EuroSCORE II | 2 (1–5) | 0 | 2 (1–4) | 4 (2–9) | <0.001 |
| Intraoperative data | |||||
| ACC time | 47 (36–66) | 386 | 46 (36, 64) | 55 (39, 78) | <0.001 |
| CBP time | 59 (46, 85) | 340 | 58 (45, 83) | 71 (51, 104) | <0.001 |
| Isolated CABG | 5715 (39) | 5387 (41) | 5387 (41) | 328 (18) | <0.001 |
| Bimammary artery bypass | 5754 (39) | 0 | 5391 (41) | 363 (20) | <0.001 |
| CABG and valve surgery | 1380 (9.3) | 0 | 1192 (9.2) | 188 (11) | 0.053 |
| Isolated valvular surgery | 5794 (39) | 0 | 4801 (37) | 993 (56) | <0.001 |
| Thoracic aortic surgery | 1508 (10) | 0 | 1334 (10) | 174 (9.8) | 0.552 |
| Cardiac transplantation | 214 (1.4) | 0 | 157 (1.2) | 57 (3.2) | <0.001 |
| Post-bypass catecholamine | 5539 (38) | 0 | 4690 (36) | 849 (48) | <0.001 |
| Post-bypass norepinephrine | 1849 (13) | 0 | 1693 (13) | 156 (8.8) | <0.001 |
| Post-bypass norepinephrine and dobutamine | 1229 (8.3) | 0 | 1000 (7.7) | 229 (13) | <0.001 |
| Postoperative data | |||||
| MV duration (h) | 6 (5, 10) | 893 | 6 (5, 9) | 8 (6, 21) | <0.001 |
| Catecholamine duration (h) | 26 (10, 57) | 7673 | 24 (10, 53) | 39 (19, 75) | <0.001 |
| Blood loss at 24 h (mL) | 540 (380, 750) | 3794 | 545 (390, 750) | 480 (320, 700) | <0.001 |
| Total blood loss (mL) | 680 (480, 950) | 3434 | 680 (490, 950) | 620 (410, 892) | <0.001 |
| Reintervention | 903 (6.1) | 0 | 801 (6.2) | 102 (5.7) | 0.495 |
| Surgical site infection | 540 (3.7) | 0 | 486 (3.7) | 54 (3.0) | 0.143 |
| Superficial SSI | 389 (2.6) | 0 | 356 (2.7) | 33 (1.9) | 0.030 |
| Deep SSI | 151 (1.0) | 0 | 130 (1.0) | 21 (1.2) | 0.471 |
| ICU LOS (days) | 3 (2, 5) | 734 | 3 (2, 5) | 4 (2, 7) | <0.001 |
| Total LOS (days) | 11 (8, 16) | 281 | 11 (8, 16) | 14 (9, 23) | <0.001 |
| D28 mortality | 589 (4.0) | 0 | 461 (3.5) | 128 (7.2) | <0.001 |
| D90 mortality | 802 (5.4) | 0 | 624 (4.8) | 178 (10) | <0.001 |
| Estimates | CI | p | |
|---|---|---|---|
| Male | 0.50 | 0.41–0.61 | <0.001 |
| Age (years) | |||
| 1st quartile <56 y | ref | ref | - |
| 2nd quartile (56, 65) y | 0.80 | 0.60–1.07 | 0.133 |
| 3rd quartile (66–74) y | 1.02 | 0.77–1.34 | 0.901 |
| 4th quartile >74 y | 1.27 | 0.96–1.69 | 0.095 |
| Obesity | 2.22 | 1.84–2.69 | <0.001 |
| Insulin-dependentdiabetes | 3.43 | 2.69–4.35 | <0.001 |
| Noninsulin-dependentdiabetes | 1.90 | 1.52–2.38 | <0.001 |
| Dyslipidaemia | 0.83 | 0.68–1.02 | 0.070 |
| Chronic peripheral arterial insufficiency | 1.66 | 1.33–2.06 | <0.001 |
| Cardiac insufficiency | 1.15 | 0.75–1.71 | 0.490 |
| ESRD | 1.97 | 1.10–3.35 | 0.016 |
| COPD | 1.55 | 1.17–2.03 | 0.002 |
| Acute infective endocarditis | 0.59 | 0.24–1.22 | 0.192 |
| Prior cardiac surgery | 1.51 | 0.97–2.30 | 0.059 |
| CPB time (/10 min) | 1.00 | 0.97–1.03 | 0.929 |
| CABG | 2.68 | 1.83–3.88 | <0.001 |
| Bimammary artery bypass | 1.97 | 1.44–2.76 | <0.001 |
| Cardiac transplantation | 3.49 | 1.59–7.15 | 0.001 |
| Post-bypass norepinephrine and dobutamine | 1.71 | 1.22–2.35 | 0.001 |
| VGA | 0.94 | 0.68–1.28 | 0.714 |
| Overall, n = 540 | CA, n = 486 (90%) | VGA n = 54 (10%) | p Value | |
|---|---|---|---|---|
| Gram-negative bacteria | 197 (36) | 169 (35) | 28 (52) | 0.013 |
| Enterobacterales | 175 (32) | 151 (31) | 24 (44) | 0.046 |
| Escherichia coli | 57 (11) | 51 (10) | 6 (11) | 0.889 |
| Serratia spp. | 16 (3.0) | 15 (3.1) | 1 (1.9) | >0.999 |
| Enterobacter spp. | 43 (8.0) | 39 (8.0) | 4 (7.4) | >0.999 |
| Morganella spp. | 14 (2.6) | 13 (2.7) | 1 (1.9) | >0.999 |
| Citrobacter spp. | 13 (2.4) | 11 (2.3) | 2 (3.7) | 0.380 |
| Proteus spp. | 21 (3.9) | 18 (3.7) | 3 (5.6) | 0.456 |
| Klebsiella spp. | 32 (5.9) | 24 (4.9) | 8 (15) | 0.009 |
| Other (Gram negative) bacteria | 7 (1.3) | 4 (0.8) | 3 (5.6) | 0.025 |
| Gram-positive bacteria | 361 (67) | 334 (69) | 27 (50) | 0.006 |
| Staphylococcus spp. | 298 (55) | 272 (56) | 26 (48) | 0.273 |
| Staphylococcus aureus | 98 (18) | 91 (19) | 7 (13) | 0.297 |
| MSSA | 89 (16) | 83 (17) | 6 (11) | 0.262 |
| MRSA | 9 (1.7) | 8 (1.6) | 1 (1.9) | >0.999 |
| CoNS | 205 (38) | 185 (38) | 20 (37) | 0.883 |
| Streptococcus spp. | 8 (1.5) | 8 (1.6) | 0 (0) | >0.999 |
| Enterococcus spp. | 62 (11) | 61 (13) | 1 (1.9) | 0.019 |
| Other (Gram positive) bacteria | 13 (2.4) | 13 (2.7) | 0 (0) | 0.630 |
| Anaerobic bacteria | 18 (3.3) | 17 (3.5) | 1 (1.9) | >0.999 |
| Fungi | 7 (1.3) | 4 (0.8) | 3 (5.6) | 0.025 |
| Associated bacteraemia | 129 (24) | 117 (24) | 12 (22) | 0.762 |
| Estimates | CI | p | |
|---|---|---|---|
| Male | 0.69 | 0.55–0.85 | 0.001 |
| Age (years) | |||
| 1st quartile < 56 y | Ref | ref | - |
| 2nd quartile [56, 65] y | 0.67 | 0.51–0.88 | 0.004 |
| 3rd quartile [66–74] y | 0.86 | 0.66–1.13 | 0.269 |
| 4th quartile > 74 y | 0.77 | 0.56–1.04 | 0.086 |
| Obesity | 3.47 | 2.84–4.23 | <0.001 |
| Insulin-dependentdiabetes | 2.79 | 2.12–3.69 | <0.001 |
| Noninsulin-dependentdiabetes | 1.62 | 1.26–2.07 | <0.001 |
| Dyslipidaemia | 0.43 | 0.35–0.54 | <0.001 |
| Chronic peripheral arterial insufficiency | 1.33 | 1.01–1.75 | 0.044 |
| Cardiac insufficiency | 1.41 | 0.92–2.15 | 0.116 |
| ESRD | 4.51 | 3.21–6.35 | <0.001 |
| COPB | 1.49 | 1.14–1.96 | 0.004 |
| Acute infective endocarditis | 1.80 | 1.36–2.37 | <0.001 |
| Prior cardiac surgery | 1.54 | 1.13–2.11 | 0.006 |
| CB time (/10 min) | 0.96 | 0.94–0.98 | 0.001 |
| CABG | 2.70 | 1.83–3.97 | <0.001 |
| Bimammary artery bypass | 1.87 | 1.28–2.73 | 0.001 |
| Cardiac transplantation | 1.43 | 0.80–2.58 | 0.228 |
| Post-bypass norepinephrine and dobutamine | 1.62 | 1.26–2.09 | <0.001 |
| VGA | 0.89 | 0.65–1.21 | 0.457 |
| Estimates | CI | p | |
|---|---|---|---|
| Male | 0.52 | 0.42–0.64 | <0.001 |
| Age (years) | |||
| 1st quartile < 56 y | ref | ref | - |
| 2nd quartile [56, 65] y | 0.81 | 0.60–1.08 | 0.155 |
| 3rd quartile [66–74] y | 1.02 | 0.77–1.35 | 0.868 |
| 4th quartile > 74 y | 1.30 | 0.98–1.73 | 0.069 |
| Obesity | 2.17 | 1.79–2.63 | <0.001 |
| Insulin-dependentdiabetes | 3.52 | 2.76–4.48 | <0.001 |
| Non insulin-dependentdiabetes | 1.90 | 1.52–2.38 | <0.001 |
| Dyslipidaemia | 0.84 | 0.68–1.03 | 0.102 |
| Chronic peripheral arterial insufficiency | 1.68 | 1.35–2.09 | <0.001 |
| Cardiac insufficiency | 1.12 | 0.74–1.69 | 0.606 |
| ESRD | 1.75 | 0.97–3.15 | 0.061 |
| COPB | 1.57 | 1.19–2.07 | 0.001 |
| Prior cardiac surgery | 1.52 | 0.98–2.36 | 0.063 |
| CB time (/10 min) | 1.00 | 0.97–1.04 | 0.766 |
| CABG | 2.65 | 1.81–3.88 | <0.001 |
| Bimammary artery bypass | 1.99 | 1.44–2.77 | <0.001 |
| Cardiac transplantation | 3.52 | 1.66–7.45 | 0.001 |
| Post-bypass norepinephrine and dobutamine | 1.66 | 1.19–2.32 | 0.003 |
| VGA | 1.03 | 0.76–1.41 | 0.838 |
| Estimates | CI | p | |
|---|---|---|---|
| Male | 0.36 | 0.28–0.47 | <0.001 |
| Age (years) | |||
| 1st quartile < 56 y | ref | ref | - |
| 2nd quartile [56, 65] y | 0.80 | 0.56–1.14 | 0.218 |
| 3rd quartile [66–74] y | 0.98 | 0.69–1.38 | 0.898 |
| 4th quartile > 74 y | 1.36 | 0.95–1.94 | 0.089 |
| Obesity | 2.19 | 1.73–2.77 | <0.001 |
| Insulin-dependentdiabetes | 3.59 | 2.68–4.79 | <0.001 |
| Non-insulin-dependentdiabetes | 2.21 | 1.68–2.90 | <0.001 |
| Dyslipidaemia | 0.94 | 0.72–1.23 | 0.655 |
| Chronic peripheral arterial insufficiency | 2.02 | 1.58–2.59 | <0.001 |
| Cardiac insufficiency | 1.22 | 0.76–1.95 | 0.404 |
| ESRD | 1.98 | 1.00–3.92 | 0.051 |
| COPB | 1.42 | 1.00–2.02 | 0.052 |
| Prior cardiac surgery | 0.25 | 0.03–1.89 | 0.177 |
| CB time (/10 min) | 0.99 | 0.93–1.05 | 0.806 |
| Post-bypass norepinephrine and dobutamine | 2.39 | 1.56–3.65 | <0.001 |
| VGA | 1.27 | 0.84–1.92 | 0.254 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Tymowski, C.; Sahnoun, T.; Provenchere, S.; Para, M.; Derre, N.; Mutuon, P.; Duval, X.; Grall, N.; Iung, B.; Kernéis, S.; et al. Impact of Antibiotic Prophylaxis on Surgical Site Infections in Cardiac Surgery. Antibiotics 2023, 12, 85. https://doi.org/10.3390/antibiotics12010085
de Tymowski C, Sahnoun T, Provenchere S, Para M, Derre N, Mutuon P, Duval X, Grall N, Iung B, Kernéis S, et al. Impact of Antibiotic Prophylaxis on Surgical Site Infections in Cardiac Surgery. Antibiotics. 2023; 12(1):85. https://doi.org/10.3390/antibiotics12010085
Chicago/Turabian Stylede Tymowski, Christian, Tarek Sahnoun, Sophie Provenchere, Marylou Para, Nicolas Derre, Pierre Mutuon, Xavier Duval, Nathalie Grall, Bernard Iung, Solen Kernéis, and et al. 2023. "Impact of Antibiotic Prophylaxis on Surgical Site Infections in Cardiac Surgery" Antibiotics 12, no. 1: 85. https://doi.org/10.3390/antibiotics12010085
APA Stylede Tymowski, C., Sahnoun, T., Provenchere, S., Para, M., Derre, N., Mutuon, P., Duval, X., Grall, N., Iung, B., Kernéis, S., Lucet, J. -C., & Montravers, P. (2023). Impact of Antibiotic Prophylaxis on Surgical Site Infections in Cardiac Surgery. Antibiotics, 12(1), 85. https://doi.org/10.3390/antibiotics12010085