
Empowering Low- and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: A Way Forward

 ,
, {kind=link}
Abstract
:1. Introduction
2. Trends of Consumption in LMICs
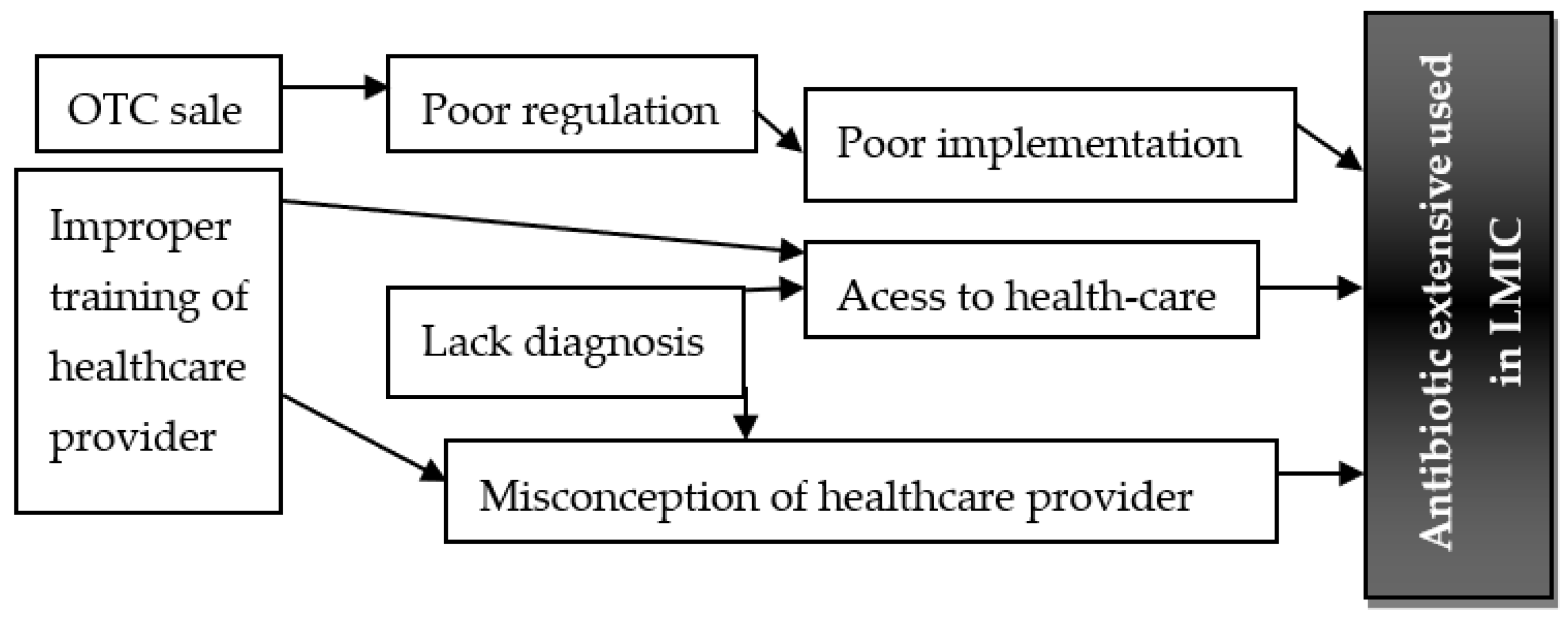
3. Factors Associated with Extensive Use
4. Issues and Mitigations
4.1. Regulatory Framework
4.2. Accessible Diagnostic Facilities
4.3. Scalable Stewardship Programs
4.4. Vaccination Drives
4.5. Healthcare Systems and Sanitation
5. Conclusions
6. Suggestions and Way Forward
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hsia, Y.; Lee, B.R.; Versporten, A. Use of the WHO Access, Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): An analysis of paediatric survey data from 56 countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [PubMed]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–15: An analysis of pharmaceutical sales data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Naing, S.; van Wijk, M.; Vila, J.; Ballesté-Delpierre, C. Understanding Antimicrobial Resistance from the Perspective of Public Policy: A Multinational Knowledge, Attitude, and Perception Survey to Determine Global Awareness. Antibiotics 2021, 10, 1486. [Google Scholar] [CrossRef]
- Dunachie, S.J.; Day, N.P.; Dolecek, C. The challenges of estimating the human global burden of disease of antimicrobial resistant bacteria. Curr. Opin. Microbiol. 2020, 57, 95–101. [Google Scholar] [CrossRef]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Hardcastle, T.C.; Haque, M.; Lugova, H.; Dhingra, S.; Sharma, P.; Islam, S.; et al. Surveillance of antimicrobial resistance in low- and middle-income countries: A scattered picture. Antimicrob Resist. Infect. Control. 2021, 10, 1–13. [Google Scholar]
- Sulis, G.; Daniels, B.; Kwan, A. Antibiotic overuse in the primary health care setting: A secondary data analysis of standardised patient studies from India, China and Kenya. BMJ Glob. Health 2020, 5, e003393. [Google Scholar] [CrossRef]
- Sulis, G.; Sayood, S.; Gandra, S. Antimicrobial resistance in low- and middle-income countries: Current status and future directions. Expert Rev. Anti. Infect. Ther. 2022, 20, 147–160. [Google Scholar] [CrossRef]
- Baraz, A.; Chowers, M.; Nevo, D.; Obolski, U. The time-varying association between previous antibiotic use and antibiotic resistance. Clin. Microbiol. Infect. 2023, 29, 390.e391–390.e394. [Google Scholar] [CrossRef]
- Sulis, G.; Sayood, S.; Katukoori, S. Exposure to World Health Organization’s AWaRe antibiotics and isolation of multidrug resistant bacteria: A systematic review and metaanalysis. Clin. Microbiol. Infect. 2022, 28, 1193–1202. [Google Scholar] [CrossRef]
- Poudel, A.N.; Zhu, S.; Cooper, N. The economic burden of antibiotic resistance: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0285170. [Google Scholar] [CrossRef] [PubMed]
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Sulis, G.; Adam, P.; Nafade, V. Antibiotic prescription practices in primary care in low and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003139. [Google Scholar] [CrossRef]
- Allwell-Brown, G.; Hussain-Alkhateeb, L.; Kitutu, F.E.; Strömdahl, S.; Mårtensson, A.; Johansson, E.W. Trends in reported antibiotic use among children under 5 years of age with fever, diarrhoea, or cough with fast or difficult breathing across low-income and middle-income countries in 2005–17: A systematic analysis of 132 national surveys from 73 countries. Lancet Glob. Health 2020, 8, e799–e807. [Google Scholar] [CrossRef] [PubMed]
- Sulis, G.; Pradhan, R.; Kotwani, A.; Gandra, S. India’s ban on antimicrobial fixed-dose combinations: Winning the battle, losing the war? J. Pharm. Policy Pract. 2022, 15, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Vliegenthart-Jongbloed, K.; Jacobs, J. Not recommended fixed-dose antibiotic combinations in low- and middle-income countries the example of Tanzania. Antimicrob. Resist. Infect. Control. 2023, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Simeonova, M. Antimicrobial resistance in patients with COVID-19: A systematic review and meta-analysis. Lancet Microbe. 2023, 4, e179–e191. [Google Scholar] [CrossRef]
- Bortone, B.; Jackson, C.; Hsia, Y.; Bielicki, J.; Magrini, N.; Sharland, M. High global consumption of potentially inappropriate fixe dose combination antibiotics: Analysis of data from 75 countries. PLoS ONE 2021, 16, e0241899. [Google Scholar] [CrossRef]
- Al-Azzam, S.; Mhaidat, N.M.; Banat, H.A. An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan. Antibiotics 2021, 10, 690. [Google Scholar] [CrossRef]
- Sulis, G.; Batomen, B.; Kotwani, A.; Pai, M.; Gandra, S. Sales of antibiotics and hydroxychloroquine in India during the COVID-19 epidemic: An interrupted time series analysis. PLoS Med. 2021, 18, e1003682. [Google Scholar] [CrossRef]
- Silva, A.R.O.; Salgado, D.R.; Lopes, L.P.N.; Castanheira, D.; Emmerick, I.C.M.; Lima, E.C. Increased Use of Antibiotics in the Intensive Care Unit During Coronavirus Disease (COVID-19) Pandemic in a Brazilian Hospital. Front. Pharmacol. 2021, 12, 778386. [Google Scholar] [CrossRef] [PubMed]
- Del Fiol, F.S.; Bergamaschi, C.C.; De Andrade, I.P., Jr.; Lopes, L.C.; Silva, M.T.; Barberato-Filho, S. Consumption Trends of Antibiotics in Brazil During the COVID-19 Pandemic. Front. Pharmacol. 2022, 13, 844818. [Google Scholar] [CrossRef] [PubMed]
- Nandi, A.; Pecetta, S.; Bloom, D.E. Global antibiotic use during the COVID-19 pandemic: Analysis of pharmaceutical sales data from 71 countries, 2020–2022. eClinicalMedicine 2023, 57, 101848. [Google Scholar] [CrossRef]
- Mah, E.M.S.; Hassan, M.Z.; Biswas, M. Use of Antimicrobials among Suspected COVID-19 Patients at Selected Hospitals, Bangladesh: Findings from the First Wave of COVID-19 Pandemic. Antibiotics 2021, 10, 738. [Google Scholar]
- Li, J.; Zhou, P.; Wang, J. Worldwide dispensing of non-prescription antibiotics in community pharmacies and associated factors: A mixed-methods systematic review. Lancet Infect. Dis. 2023, 24, S1473–S3099. [Google Scholar] [CrossRef] [PubMed]
- Oleribe, O.O.; Momoh, J.; Uzochukwu, B.S. Identifying Key Challenges Facing Healthcare Systems in Africa And Potential Solutions. Int. J. Gen. Med. 2019, 12, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.V.; Pulcini, C.; Demirjian, A.; van Hecke, O. Rapid diagnostic tests for common infection syndromes: Less haste, more speed. J. Antimicrob. Chemother. 2020, 75, 2028–2030. [Google Scholar] [CrossRef]
- Belachew, S.A.; Hall, L.; Erku, D.A.; Selvey, L.A. No prescription? No problem: Drivers of non-prescribed sale of antibiotics among community drug retail outlets in low and middle income countries: A systematic review of qualitative studies. BMC Public Health 2021, 21, 1056. [Google Scholar] [CrossRef]
- Cox, S.; Vleeming, M.; Giorgi, W.; Dinant, G.J.; Cals, J.; de Bont, E. Patients’ Experiences, Expectations, Motivations, and Perspectives around Urinary Tract Infection Care in General Practice: A Qualitative Interview Study. Antibiotics 2023, 12, 241. [Google Scholar] [CrossRef]
- Lim, J.M.; Huy, S.; Chhay, T.; Khieu, B.; Hsu, L.Y.; Tam, C.C. Understanding networks in rural Cambodian farming communities and how they influence antibiotic use: A mixed methods study. PLOS Glob. Public Health 2023, 3, e0001569. [Google Scholar] [CrossRef]
- Amábile-Cuevas, C.F. Myths and Misconceptions around Antibiotic Resistance: Time to Get Rid of Them. Infect. Chemother. 2022, 54, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Paredes, D.; Larrea-Álvarez, C.M.; Torres-Elizalde, L. Antibiotic Resistance Awareness among Undergraduate Students in Quito, Ecuador. Antibiotics 2022, 11, 197. [Google Scholar] [CrossRef] [PubMed]
- Gunasekera, Y.D.; Kinnison, T.; Kottawatta, S.A.; Silva-Fletcher, A.; Kalupahana, R.S. Misconceptions of Antibiotics as a Potential Explanation for Their Misuse. A Survey of the General Public in a Rural and Urban Community in Sri Lanka. Antibiotics 2022, 11, 454. [Google Scholar] [CrossRef] [PubMed]
- Al-Taie, A.; Hussein, A.N.; Albasry, Z. A Cross-Sectional Study of Patients’ Practices, Knowledge and Attitudes of Antibiotics among Iraqi Population. J. Infect. Dev. Ctries. 2021, 15, 1845–1853. [Google Scholar] [CrossRef]
- Shamim, M.A.; Padhi, B.K.; Satapathy, P. Parents’ expectation of antibiotic prescriptions for respiratory infections in children: A systematic review and meta-analysis. Ther. Adv. Infect. Dis. 2023, 10, 20499361231169429. [Google Scholar] [CrossRef]
- Shamsudeen, S.M.; Priya, R.S.; Sujatha, G.; Muruganandhan, J.; Manikandan, K. Selfmedication with antibiotics: A knowledge, attitude, and practice appraisal of 610 dental patients in Chennai, India, from 2016 to 2017. J. Educ. Health Promot. 2018, 7, 66. [Google Scholar]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey; World Health Organization (WHO): Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/194460 (accessed on 1 October 2023).
- Elong Ekambi, G.A.; Okalla Ebongue, C.; Penda, I.C.; Nnanga Nga, E.; Mpondo Mpondo, E.; EboumbouMoukoko, C.E. Knowledge, practices and attitudes on antibiotics use in Cameroon: Self-medication and prescription survey among children, adolescents and adults in private pharmacies. PLoS ONE 2019, 14, e0212875. [Google Scholar] [CrossRef]
- Ahmed, I.; King, R.; Akter, S.; Akter, R.; Aggarwal, V.R. Determinants of antibiotic self medication: A systematic review and mata-analysis. Res. Social Adm. Pharm. 2023, 19, 1007–1017. [Google Scholar] [CrossRef]
- Muleme, J.; Ssempebwa, J.C.; Musoke, D. Antimicrobial resistance among farming communities in Wakiso District, Central Uganda: A knowledge, awareness and practice study. PLoS ONE 2023, 18, e0284822. [Google Scholar] [CrossRef]
- Chukwu, E.E.; Oladele, D.A.; Awoderu, O.B. A national survey of public awareness of antimicrobial resistance in Nigeria. Antimicrob. Resist. Infect. Control. 2020, 9, 1–13. [Google Scholar] [CrossRef]
- Greer, S.L.; Méndez, C.A. Universal Health Coverage: A Political Struggle and Governance Challenge. Am. J. Public Health 2015, 105, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Whitehorn, A.; Fu, L.; Porritt, K. Mapping Clinical Barriers and Evidence-Based Implementation Strategies in Low-to-Middle Income Countries (LMICs). Worldviews Evid. Based Nurs. 2021, 18, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Sulis, G.; Gandra, S. Access to antibiotics: Not a problem in some LMICs. Lancet Glob. Health 2021, 9, e561–e562. [Google Scholar] [CrossRef] [PubMed]
- Porter, G.; Kotwani, A.; Bhullar, L.; Joshi, J. Over-the-counter sales of antibiotics for human use in India: The challenges and opportunities for regulation. Med. Law Int. 2021, 21, 147–173. [Google Scholar] [CrossRef]
- Wirtz, V.J.; Herrera-Patino, J.J.; Santa-Ana-Tellez, Y.; Dreser, A.; Elseviers, M.; Vander Stichele, R.H. Analysing policy interventions to prohibit over-the-counter antibiotic sales in four Latin American countries. Trop. Med. Int. Health 2013, 18, 665–673. [Google Scholar] [CrossRef]
- Rao, U.P.; Rao, N.S.S. The rural medical practitioner of India. J. Evol. Med. Dental Sci. 2017, 6, 5321–5323. [Google Scholar]
- Jacobs, T.G.; Robertson, J.; van den Ham, H.A.; Iwamoto, K.; Bak Pedersen, H.; Mantel-Teeuwisse, A.K. Assessing the impact of law enforcement to reduce over-the-counter OTC) sales of antibiotics in low- and middle-income countries; A systematic literature review. BMC Health Serv. Res. 2019, 19, 1–15. [Google Scholar] [CrossRef]
- Kumah, E. The informal healthcare providers and universal health coverage in low and middle-income countries. Glob. Health 2022, 18, 1–5. [Google Scholar] [CrossRef]
- Khare, S.; Purohit, M.; Sharma, M. Antibiotic Prescribing by Informal Healthcare Providers for Common Illnesses: A Repeated Cross-Sectional Study in Rural India. Antibiotics 2019, 8, 139. [Google Scholar] [CrossRef]
- Das, J.; Chowdhury, A.; Hussam, R.; Banerjee, A.V. The impact of training informal health care providers in India: A randomized controlled trial. Science 2016, 354, aaf7384. [Google Scholar] [CrossRef]
- Sudhinaraset, M.; Ingram, M.; Lofthouse, H.K.; Montagu, D. What is the role of informal healthcare providers in developing countries? A systematic review. PLoS ONE 2013, 8, e54978. [Google Scholar] [CrossRef]
- Poluektova, O.; Robertson, D.A.; Rafferty, A.; Cunney, R.; Lunn, P.D. A scoping review and behavioural analysis of factors underlying overuse of antimicrobials. JAC Antimicrob. Resist. 2023, 5, dlad043. [Google Scholar] [CrossRef]
- Kotwani, A.; Joshi, P.C.; Jhamb, U.; Holloway, K. Prescriber and dispenser perceptions about antibiotic use in acute uncomplicated childhood diarrhea and upper respiratory tract infection in New Delhi: Qualitative study. Indian J. Pharmacol. 2017, 49, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Ingelbeen, B.; Phanzu, D.M.; Phoba, M.F. Antibiotic use from formal and informal healthcare providers in the Democratic Republic of Congo: A population-based study in two health zones. Clin. Microbiol. Infect. 2022, 28, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for the Management of Symptomatic Sexually Transmitted Infections; World Health Organization (WHO): Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240024168 (accessed on 1 October 2023).
- Huth, P.F.B.; Addo, M.; Daniel, T. Extensive Antibiotic and Antimalarial Prescription Rate among Children with Acute Febrile Diseases in the Lake Victoria Region, Tanzania. J. Trop. Pediatr. 2021, 67, fmaa135. [Google Scholar] [CrossRef] [PubMed]
- Wangdi, K.; Kasturiaratchi, K.; Nery, S.V.; Lau, C.L.; Gray, D.J.; Clements, A.C.A. Diversity of infectious aetiologies of acute undifferentiated febrile illnesses in south and Southeast Asia: A systematic review. BMC Infect Dis. 2019, 19, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Van Hecke, O.; Raymond, M.; Lee, J.J. In-vitro diagnostic point-of-care tests in paediatric ambulatory care: A systematic review and meta-analysis. PLoS ONE 2020, 15, e02356051. [Google Scholar] [CrossRef]
- Mullis, A.S.; Peroutka-Bigus, N.; Phadke, K.S.; Bellaire, B.H.; Narasimhan, B. Nanomedicines to counter microbial barriers and anti microbial resistance. Curr. Opin. Chem. Eng. 2021, 31, 100672. [Google Scholar] [CrossRef]
- Apisarnthanarak, A.; Bin Kim, H.; Moore, L.S.P. Utility and Applicability of Rapid Diagnostic Testing in Antimicrobial Stewardship in the Asia-Pacific Region: A Delphi Consensus. Clin. Infect Dis. 2022, 74, 2067–2076. [Google Scholar] [CrossRef]
- Escadafal, C.; Incardona, S.; Fernandez-Carballo, B.L.; Dittrich, S. The good and the bad: Using C reactive protein to distinguish bacterial from non-bacterial infection among febrile patients in low-resource settings. BMJ Glob. Health 2020, 5, e002396. [Google Scholar] [CrossRef]
- Zay Ya, K.; Win, P.T.N.; Bielicki, J.; Lambiris, M.; Fink, G. Association Between Antimicrobial Stewardship Programs and Antibiotic Use Globally: A Systematic Review and Meta- Analysis. JAMA Netw. Open 2023, 6, e2253806. [Google Scholar] [CrossRef]
- O’Leary, E.N.; van Santen, K.L.; Webb, A.K.; Pollock, D.A.; Edwards, J.R.; Srinivasan, A. Uptake of Antibiotic Stewardship Programs in US Acute Care Hospitals: Findings From the 2015 National Healthcare Safety Network Annual Hospital Survey. Clin. Infect. Dis. 2017, 65, 1748–1750. [Google Scholar] [CrossRef]
- Chakraborty, N.; Jha, D.; Roy, I. Nanobiotics against antimicrobial resistance: Harnessing the power of nanoscale materials and technologies. J. Nanobiotechnol. 2022, 20, 375. [Google Scholar] [CrossRef] [PubMed]
- Simmons, B.; Ariyoshi, K.; Ohmagari, N. Progress towards antibiotic use targets in eight high-income countries. Bull. World Health Organ. 2021, 99, 550–561. [Google Scholar] [CrossRef] [PubMed]
- Nathwani, D.; Varghese, D.; Stephens, J.; Ansari, W.; Martin, S.; Charbonneau, C. Value of hospital antimicrobial stewardship programs: A systematic review. Antimicrob. Resist. Infect. Control. 2019, 35, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Durkin, M.J.; Keller, M.; Butler, A.M. An Assessment of Inappropriate Antibiotic Use and Guideline Adherence for Uncomplicated Urinary Tract Infections. Open Forum Infect. Dis. 2018, 5, ofy198. [Google Scholar] [CrossRef]
- Havers, F.P.; Hicks, L.A.; Chung, J.R. Outpatient Antibiotic Prescribing for Acute Respiratory Infections During Influenza Seasons. JAMA Netw. Open 2018, 1, e180243. [Google Scholar] [CrossRef]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef]
- Badur, İ.; Bilgin Badur, N.; Berk, B. Investigation of hidden crisis of prescription drug abuse in Turkey: Pregabalin monitoring. Acta Pharm. Sci. 2022, 60, 1–12. [Google Scholar] [CrossRef]
- Wellcome Trust. The Global Response to AMR: Momentum, Success, and Critical Gaps; Wellcome Trust: London, UK, 2020; Available online: https://wellcome.org/reports/global-response-amr-momentum-success-and-critical-gaps (accessed on 1 October 2023).
- Aksoy, M.; Isli, F.; Kadi, E. Evaluation of more than one billion outpatient prescriptions and eight-year trend showing a markable reduction in antibiotic prescription in Turkey: A success model of governmental interventions at national level. Pharmacoepidemiol. Drug Saf. 2021, 30, 1242–1249. [Google Scholar] [CrossRef]
- Aydın, M.; Koyuncuoğlu, C.Z.; Kırmızı, İ. Pattern of Antibiotic Prescriptions in Dentistry in Turkey: Population Based Data from the Prescription Information System. Infect. Dis. Clin. Microbiol. 2019, 1, 62–69. [Google Scholar] [CrossRef]
- Kerr, F.; Sefah, I.A.; Essah, D.O. Practical Pharmacist-Led Interventions to Improve Antimicrobial Stewardship in Ghana, Tanzania, Uganda and Zambia. Pharmacy 2021, 9, 124. [Google Scholar] [CrossRef] [PubMed]
- Blanchette, L.; Gauthier, T.; Heil, E. The essential role of pharmacists in antibiotic stewardship in outpatient care: An official position statement of the Society of Infectious Diseases Pharmacists. J. Am. Pharm. Assoc. 2018, 58, 481–484. [Google Scholar] [CrossRef]
- Gebretekle, G.B.; Haile Mariam, D.; Abebe Taye, W. Half of Prescribed Antibiotics Are Not Needed: A Pharmacist-Led Antimicrobial Stewardship Intervention and Clinical Outcomes in a Referral Hospital in Ethiopia. Front Public Health 2020, 8, 109. [Google Scholar] [CrossRef] [PubMed]
- van den Bergh, D.; Messina, A.P.; Goff, D.A. A pharmacist-led prospective antibiotic stewardship intervention improves compliance to community-acquired pneumonia guidelines in 39 public and private hospitals across South Africa. Int. J. Antimicrob. Agents 2020, 56, 106189. [Google Scholar] [CrossRef]
- Baubie, K.; Shaughnessy, C.; Kostiuk, L. Evaluating antibiotic stewardship in a tertiary care hospital in Kerala, India: A qualitative interview study. BMJ Open 2019, 9, e026193. [Google Scholar] [CrossRef]
- Rehman, I.U.; Asad, M.M.; Bukhsh, A. Knowledge and Practice of Pharmacists toward Antimicrobial Stewardship in Pakistan. Pharmacy 2018, 6, 116. [Google Scholar] [CrossRef]
- Koju, P.; Rousseau, S.P.; Van der Putten, M.; Shrestha, A.; Shrestha, R. Advertisement of antibiotics for upper respiratory infections and equity in access to treatment: A cross sectional study in Nepal. J. Pharm. Policy Pract. 2020, 13, 1–7. [Google Scholar] [CrossRef]
- Matin, M.A.; Khan, W.A.; Karim, M.M. What influences antibiotic sales in rural Bangladesh? A drug dispensers’ perspective. J. Pharm. Policy Pract. 2020, 13, 1–12. [Google Scholar] [CrossRef]
- Cuevas, C.; Batura, N.; Wulandari, L.P.L.; Khan, M.; Wiseman, V. Improving antibiotic use through behaviour change: A systematic review of interventions evaluated in low- and middle-income countries. Health Policy Plan. 2021, 36, 594–605. [Google Scholar]
- Zheng, K.; Xie, Y.; Dan, L. Effectiveness of Educational Interventions for Health Workers on Antibiotic Prescribing in Outpatient Settings in China: A Systematic Review and Meta-Analysis. Antibiotics 2022, 11, 791. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The WHO AWaRe (Access, Watch, Reserve) Antibiotic Book; World Health Organization (WHO): Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240062382 (accessed on 1 October 2023).
- Sharland, M.; Zanichelli, V.; Ombajo, L.A. The WHO essential medicines list AWaRe book: From a list to a quality improvement system. Clin. Microbiol. Infect. 2022, 28, 1533–1535. [Google Scholar] [CrossRef] [PubMed]
- Sharland, M.; Cappello, B.; Ombajo, L.A. The WHO AWaRe Antibiotic Book: Providing guidance on optimal use and informing policy. Lancet Infect. Dis. 2022, 22, 1528–1530. [Google Scholar] [CrossRef]
- Zanichelli, V.; Sharland, M.; Cappello, B. The WHO AWaRe (Access, Watch, Reserve) antibiotic book and prevention of antimicrobial resistance. Bull. World Health Organ. 2023, 101, 290–296. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Collaborators. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Hay, S.I.; Rao, P.C.; Dolecek, C. Measuring and mapping the global burden of antimicrobial resistance. BMC Med. 2018, 16, 1–3. [Google Scholar] [CrossRef]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef]
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef]
- Gandra, S.; Barter, D.M.; Laxminarayan, R. Economic burden of antibiotic resistance: How much do we really know? Clin. Microbiol. Infect. 2014, 20, 973–980. [Google Scholar] [CrossRef]
- Largeron, N.; Lévy, P.; Wasem, J.; Bresse, X. Role of vaccination in the sustainability of healthcare systems. J. Mark. Access Health Policy 2015, 3, 27043. [Google Scholar] [CrossRef]
- Marangu, D.; Zar, H.J. Childhood pneumonia in low-and-middle-income countries: An update. Paediatr. Respir. Rev. 2019, 32, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, S.N.; Collins, S.; Djennad, A. Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000–2017: A prospective national observational cohort study. Lancet Infect. Dis. 2018, 18, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Lo, N.C.; Arinaminpathy, N.; Frost, I.; Laxminarayan, R. Childhood vaccines and antibiotic use in low- and middle-income countries. Nature 2020, 581, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Awuor, A.O.; Ogwel, B.; Powell, H. Antibiotic-Prescribing Practices for Management of Childhood Diarrhea in 3 Sub-Saharan African Countries: Findings from the Vaccine Impact on Diarrhea in Africa (VIDA) Study, 2015–2018. Clin. Infect. Dis. 2023, 76, S32–S40. [Google Scholar] [CrossRef]
- Buckley, B.S.; Henschke, N.; Bergman, H. Impact of vaccination on antibiotic usage: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2019, 25, 1213–1225. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Fries, L.F.; Cho, I.; Chen, J.; Laxminarayan, R. Prevention of antimicrobial prescribing among infants following maternal vaccination against respiratory syncytial virus. Proc. Natl. Acad. Sci. USA 2022, 119, e2112410119. [Google Scholar] [CrossRef]
- Heymann, D.L.; Kieny, M.P.; Laxminarayan, R. Adding to the mantra: Vaccines prevent illness and death, and preserve existing antibiotics. Lancet Infect. Dis. 2022, 22, 1108–1109. [Google Scholar] [CrossRef]
- Schueller, E.; Nandi, A.; Joshi, J.; Laxminarayan, R.; Klein, E.Y. Associations between private vaccine and antimicrobial consumption across Indian states, 2009–2017. Ann. N. Y. Acad. Sci. 2021, 1494, 31–43. [Google Scholar] [CrossRef]
- Yousafzai, M.T.; Qamar, F.N.; Shakoor, S. Ceftriaxone-resistant Salmonella Typhi Outbreak in Hyderabad City of Sindh, Pakistan: High Time for the Introduction of Typhoid Conjugate Vaccine. Clin. Infect. Dis. 2019, 68, S16–S21. [Google Scholar] [CrossRef]
- Qamar, F.N.; Yousafzai, M.T.; Khalid, M. Outbreak investigation of ceftriaxone resistant Salmonella enterica serotype Typhi and its risk factors among the general population in Hyderabad, Pakistan: A matched case-control study. Lancet Infect. Dis. 2018, 18, 1368–1376. [Google Scholar] [CrossRef]
- Klemm, E.J.; Shakoor, S.; Page, A.J. Emergence of an Extensively Drug-Resistant Salmonella enterica Serovar Typhi Clone Harboring a Promiscuous Plasmid Encoding Resistance to Fluoroquinolones and Third-Generation Cephalosporins. mBio 2018, 9, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, S.; Naveed, A.B.; Yousafzai, M.T. Response of extensively drug resistant Salmonella Typhi to treatment with meropenem and azithromycin, in Pakistan. PLoS Negl. Trop. Dis. 2020, 14, e0008682. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.Z.R.; de Lima, E.M.; Martins Aires, C.A. Outbreak report of polymyxincarbapenem- resistant Klebsiella pneumoniae causing untreatable infections evidenced by synergy tests and bacterial genomes. Sci. Rep. 2023, 13, 6238. [Google Scholar] [CrossRef] [PubMed]
- Allel, K.; Day, L.; Hamilton, A. Global antimicrobial-resistance drivers: An ecological country-level study at the human-animal interface. Lancet Planet Health 2023, 7, e291–e303. [Google Scholar] [CrossRef]
- World Health Organization—Regional Office for the Eastern Mediterranean. Pakistan First Country to Introduce New Typhoid Vaccine into Routine Immunization Programme; World Health Organization (WHO) Regional Office for the Eastern Mediterranean: Karachi, Pakistan, 2019; Available online: https://www.emro.who.int/pak/pakistan-news/pakistan-first-country-to-introduce-new-typhoid-vaccine-into-routine-immunization-programme.html. (accessed on 1 October 2023).
- Nampota-Nkomba, N.; Nyirenda, O.M.; Khonde, L. Safety and immunogenicity of a typhoid conjugate vaccine among children aged 9 months to 12 years in Malawi: A nested substudy of a double-blind, randomised controlled trial. Lancet Glob. Health 2022, 10, e1326–e1335. [Google Scholar] [CrossRef]
- Yousafzai, M.T.; Karim, S.; Qureshi, S. Effectiveness of typhoid conjugate vaccine against culture-confirmed Salmonella enterica serotype Typhi in an extensively drugresistant outbreak setting of Hyderabad, Pakistan: A cohort study. Lancet Glob. Health 2021, 9, e1154–e1162. [Google Scholar] [CrossRef]
- Birger, R.; Antillón, M.; Bilcke. J. Estimating the effect of vaccination on antimicrobial-resistant typhoid fever in 73 countries supported by Gavi: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 679–691. [Google Scholar] [CrossRef]
- Frost, I.; Sati, H.; Garcia-Vello, P. The role of bacterial vaccines in the fight against antimicrobial resistance: An analysis of the preclinical and clinical development pipeline. Lancet Microbe. 2023, 4, e113–e125. [Google Scholar] [CrossRef]
- World Health Organization. WHO Priority Pathogens List for R&D of New Antibiotics; World Health Organization (WHO): Geneva, Switzerland, 2017; Available online: https://www.who.int/news/item/27–02–2017-who-publishes-list-of-bacteria-for-which-new-antibiotics-are-urgently-needed (accessed on 1 October 2023).
- Micoli, F.; Bagnoli, F.; Rappuoli, R.; Serruto, D. The role of vaccines in combatting antimicrobial resistance. Nat. Rev. Microbiol. 2021, 19, 287–302. [Google Scholar] [CrossRef]
- Riou, J.; Althaus, C.L.; Allen, H. Projecting the development of antimicrobial resistance in Neisseria gonorrhoeae from antimicrobial surveillance data: A mathematical modelling study. BMC Infect. Dis. 2023, 23, 252. [Google Scholar] [CrossRef]
- Whittles, L.K.; White, P.J.; Didelot, X. Assessment of the Potential of Vaccination to Combat Antibiotic Resistance in Gonorrhea: A Modeling Analysis to Determine Preferred Product Characteristics. Clin. Infect. Dis. 2020, 71, 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Causey, K.; Fullman, N.; Sorensen, R.J.D. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Ashok, G.; Debroy, R.; Ramaiah, S.; Livingstone, P.; Anbarasu, A. Impact of the COVID-19 pandemic on routine vaccine landscape: A global perspective. Hum. Vaccine Immunother. 2023, 18, 2199656. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Partners Announce a New Effort—“The Big Catch-Up”—To Vaccinate Millions of Children and Restore Immunization Progress Lost During the Pandemic; World Health Organization (WHO): Geneva, Switerland, 2023; Available online: https://www.unicefusa.org/press/global-partners-announce-new-effort-big-catch-vaccinate-millions-children-and-restore (accessed on 1 October 2023).
- Do, N.T.T.; Vu, H.T.L.; Nguyen, C.T.K. Community-based antibiotic access and use in six low-income and middle-income countries: A mixed-method approach. Lancet Glob. Health 2021, 9, e610–e619. [Google Scholar] [CrossRef] [PubMed]
- Kotwani, A.; Bhanot, A.; Singal, G.L.; Gandra, S. Marketing and Distribution System Foster Misuse of Antibiotics in the Community: Insights from Drugs Wholesalers in India. Antibiotics 2022, 11, 95. [Google Scholar] [CrossRef]
- Statista. Share of Urban Population Worldwide in 2022, by Continent; Statista Research Department: New York, NY, USA, 2023; Available online: https://www.statista.com/statistics/270860/urbanization-by-continent/ (accessed on 1 October 2023).
- Davis, M. Slum Ecology. In Planet of Slums; Verso: Brooklyn, NY, USA; pp. 120–150. Available online: https://orionmagazine.org/article/slum-ecology/ (accessed on 1 October 2023).
- Ritchie, H.; Roser, M. Urbanization . 2018. Available online: https://ourworldindata.org/urbanization (accessed on 1 October 2023).
- Denyer Willis, L.; Chandler, C. Quick fix for care, productivity, hygiene and inequality: Reframing the entrenched problem of antibiotic overuse. BMJ Glob. Health 2019, 4, e001590. [Google Scholar] [CrossRef]
- Collignon, P.; Beggs, J.J. Socioeconomic Enablers for Contagion: Factors Impelling the Antimicrobial Resistance Epidemic. Antibiotics 2019, 8, 86. [Google Scholar] [CrossRef]
- Ramay, B.M.; Caudell, M.A.; Cordón-Rosales, C. Antibiotic use and hygiene interact to influence the distribution of antimicrobial-resistant bacteria in low-income communities in Guatemala. Sci. Rep. 2022, 10, 13767. [Google Scholar] [CrossRef]
- Dixon, J.; MacPherson, E.E.; Nayiga, S. Antibiotic stories: A mixed-methods, multicountry analysis of household antibiotic use in Malawi, Uganda and Zimbabwe. BMJ Glob. Health 2021, 6, e006920. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanan, M.; Ramadan, M.; Haif, H.; Abdullah, B.; Mubarak, J.; Ahmad, W.; Mari, S.; Hassan, S.; Eid, R.; Hasan, M.; et al. Empowering Low- and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: A Way Forward. Antibiotics 2023, 12, 1504. https://doi.org/10.3390/antibiotics12101504
Kanan M, Ramadan M, Haif H, Abdullah B, Mubarak J, Ahmad W, Mari S, Hassan S, Eid R, Hasan M, et al. Empowering Low- and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: A Way Forward. Antibiotics. 2023; 12(10):1504. https://doi.org/10.3390/antibiotics12101504
Chicago/Turabian StyleKanan, Mohammed, Maali Ramadan, Hanan Haif, Bashayr Abdullah, Jawaher Mubarak, Waad Ahmad, Shahad Mari, Samaher Hassan, Rawan Eid, Mohammed Hasan, and et al. 2023. "Empowering Low- and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: A Way Forward" Antibiotics 12, no. 10: 1504. https://doi.org/10.3390/antibiotics12101504
APA StyleKanan, M., Ramadan, M., Haif, H., Abdullah, B., Mubarak, J., Ahmad, W., Mari, S., Hassan, S., Eid, R., Hasan, M., Qahl, M., Assiri, A., Sultan, M., Alrumaih, F., & Alenzi, A. (2023). Empowering Low- and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: A Way Forward. Antibiotics, 12(10), 1504. https://doi.org/10.3390/antibiotics12101504