
Antimicrobial Treatment of Serratia marcescens Invasive Infections: Systematic Review

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Site of S. marcescens Isolation
2.2. Method for S. marcescens Identification
2.3. Clinical Manifestation of S. marcescens Infection
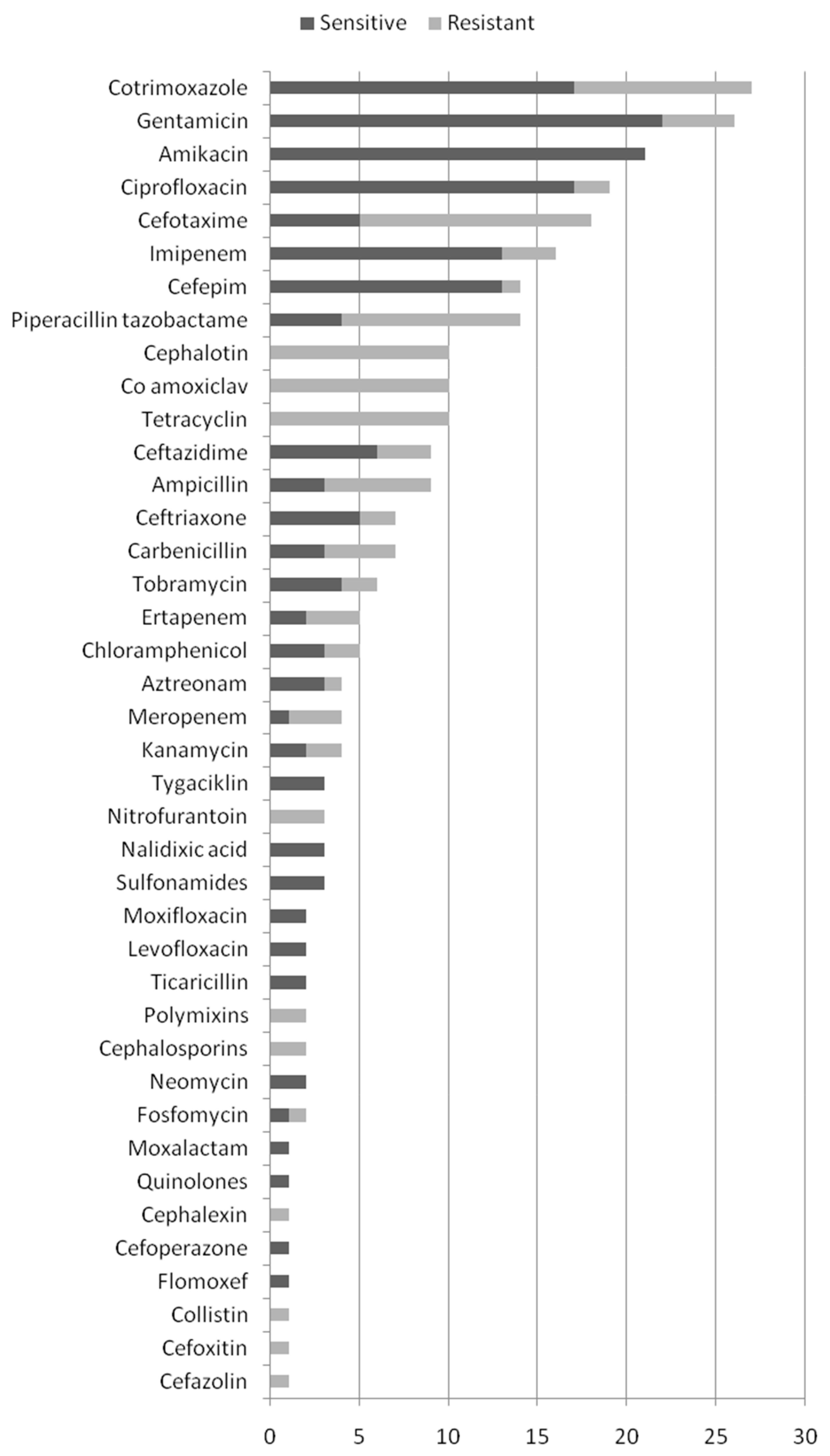
2.4. Sensitivity of S. marcescens to Antibiotics
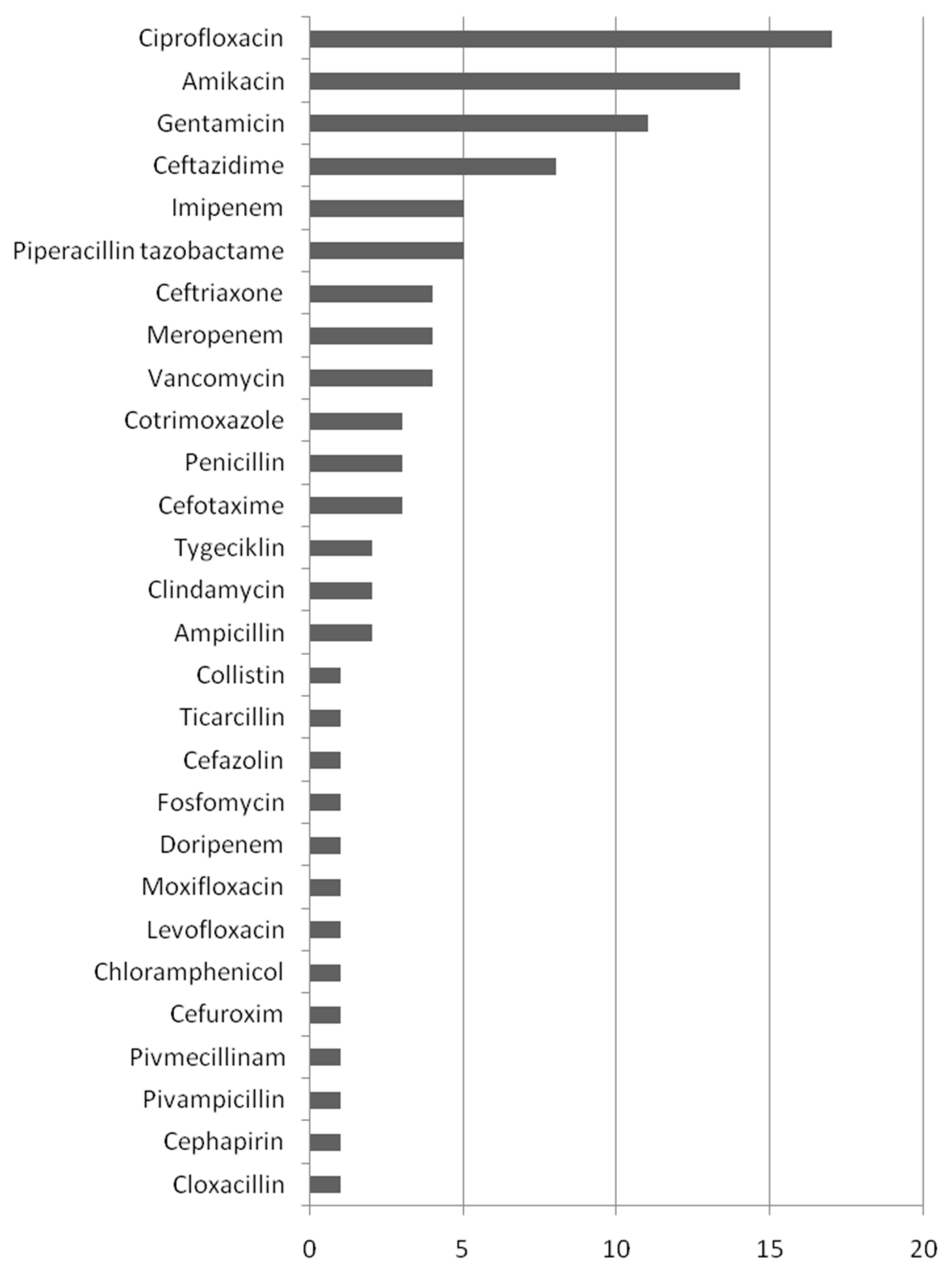
2.5. Antibiotics Used in the Treatment of Serratia marcescens Infection
2.6. Treatment Outcomes
3. Discussion
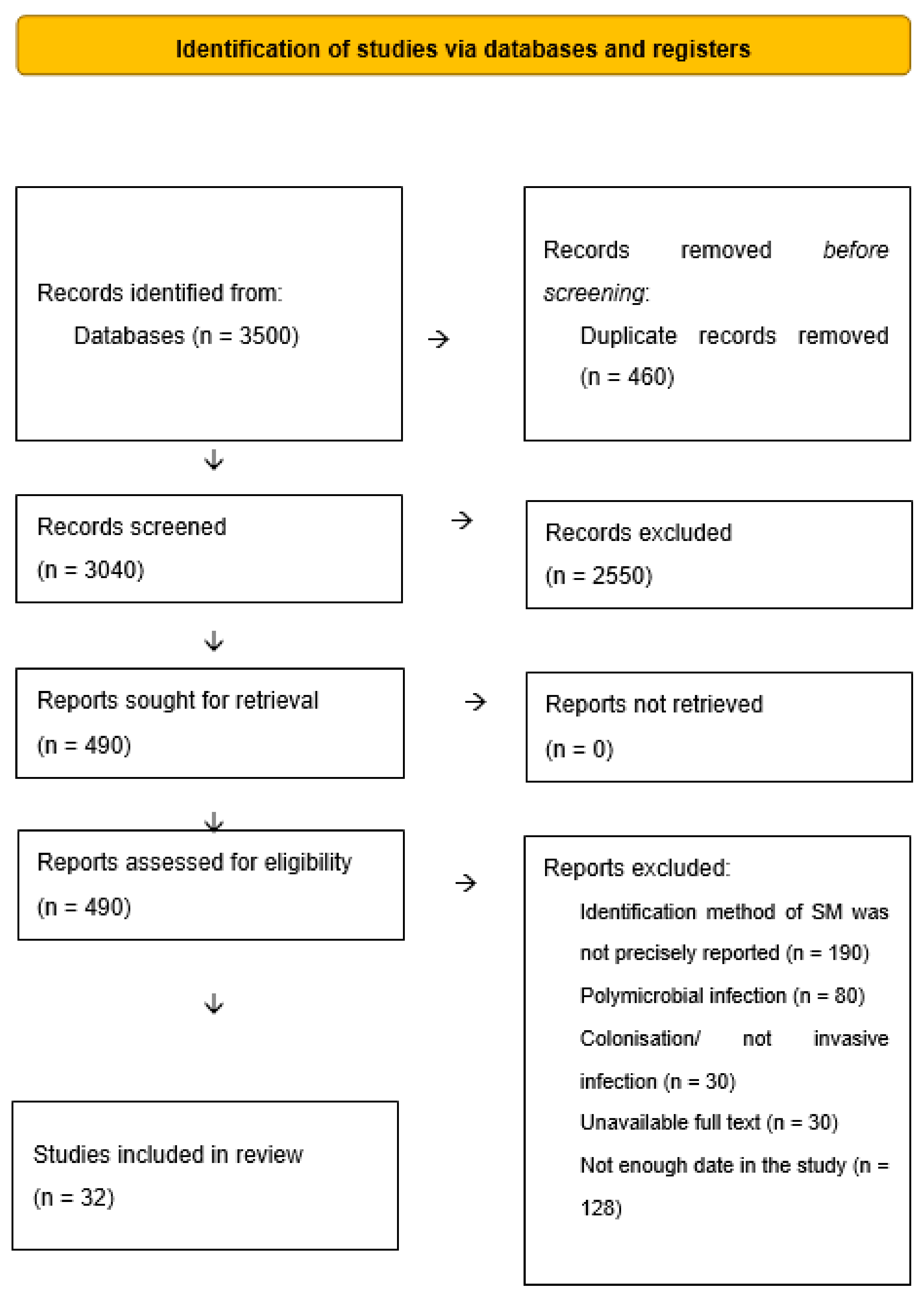
4. Materials and Methods
4.1. Data Sources
4.2. Participants and Study Eligibility Criteria
4.3. Interventions
4.4. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khanna, A.; Khanna, M.; Aggarwal, A. Serratia marcescens—A rare opportunistic nosocomial pathogen and measures to limit its spread in hospitalized patients. J. Clin. Diagn. Res. 2013, 7, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Adeolu, M.; Alnajar, S.; Naushad, S.; Gupta, R.S. Genome-based phylogeny and taxonomy of the ‘Enterobacteriales’: Proposal for Enterobacterales ord. nov. divided into the families Enterobacteriaceae, Erwiniaceae fam. nov., Pectobacteriaceae fam. nov., Yersiniaceae fam. nov., Hafniaceae fam. nov., Morganellaceae fam. nov., and Budviciaceae fam. nov. Int. J. Syst. Evol. Microbiol. 2016, 66, 5575–5599. [Google Scholar] [CrossRef] [PubMed]
- Nazzaro, G. Serratia marcescens: An Italian story. Int. J. Dermatol. 2017, 56, 795–796. [Google Scholar] [CrossRef] [PubMed]
- Herra, C.; Falkiner, F. Serratia marcescens. Available online: http://www.antimicrobe.org/b26.asp (accessed on 1 September 2022).
- Hertle, R. The family of Serratia type pores forming toxins. Curr. Protein Pept. Sci. 2005, 6, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Ray, C.; Shenoy, A.T.; Orihuela, C.J.; Gonzales Juarbe, N. Killing of Serratia marcescens biofilms with chloramphenicol. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 19. [Google Scholar] [CrossRef]
- Jones, R.N. Microbial etiologies of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia. Clin. Infect. Dis. 2010, 51 (Suppl. S1), S81–S87. [Google Scholar] [CrossRef]
- Mills, J.; Drew, D. Serratia marcescens endocarditis: A regional illness associated with intravenous drug abuse. Ann. Intern. Med. 1976, 84, 29–35. [Google Scholar] [CrossRef]
- Merkier, A.K.; Rodríguez, M.C.; Togneri, A.; Brengi, S.; Osuna, C.; Pichel, M.; Cassini, M.H.; Centrón, D. Serratia marcescens Argentinean Collaborative Group Outbreak of a Cluster with Epidemic Behavior Due to Serratia marcescens after Colistin Administration in a Hospital Setting. J. Clin. Microbiol. 2013, 51, 2295–2302. [Google Scholar] [CrossRef]
- Arslan, U.; Erayman, I.; Kirdar, S.; Yuksekkaya, S.; Cimen, O.; Tuncer, I.; Bozdogan, B. Serratia marcescens sepsis outbreak in a neonatal intensive care unit. Pediatr. Int. 2010, 52, 208–212. [Google Scholar] [CrossRef]
- Harris, P.N.; Ferguson, J.K. Antibiotic therapy for inducible AmpC β-lactamase-producing Gram-negative bacilli: What are the alternatives to carbapenems, quinolones and aminoglycosides? Int. J. Antimicrob. Agents 2012, 40, 297–305. [Google Scholar] [CrossRef]
- Altwegg, M.; Lüthy-Hottenstein, J.; Grehn, M.; von Graevenitz, A. Automated analysis of 35-S-methionine labeled proteins by SDS-PAGE as a typing method in a suspected cluster of Serratia marcescens. Zentralbl. Bakteriol. 1989, 271, 372–380. [Google Scholar] [CrossRef]
- Blajchman, M.A.; Thornley, J.H.; Richardson, H.; Elder, D.; Spiak, C.; Racher, J. Platelet transfusion-induced Serratia marcescens sepsis due to vacuum tube contamination. Transfusion 1979, 19, 39–44. [Google Scholar] [CrossRef]
- Campbell, J.R.; Diacovo, T.; Baker, C.J. Serratia marcescens meningitis in neonates. Pediatr. Infect. Dis. J. 1992, 11, 881–886. [Google Scholar] [CrossRef]
- Castro-Moraga, M.E.; Coria, P.; Conca, N.; Berho, J.; King, A. Osteomielitis multifocal por Serratia marcescens en un niño con enfermedadgranulomatosacrónica [Serratia marcescens multifocal osteomyelitis in a child with chronic granulomatous disease]. Rev. Chil. De Infectología 2021, 38, 574–579. [Google Scholar] [CrossRef]
- Cayô, R.; Leme, R.C.P.; Streling, A.P.; Matos, A.P.; Nodari, C.S.; Chaves, J.R.E.; Brandão, J.L.F.; de Almeida, M.F.; Carrareto, V.; Pereira, M.A.D.C.; et al. Serratia marcescens harboring SME-4 in Brazil: A silent threat. Diagn. Microbiol. Infect. Dis. 2017, 87, 357–358. [Google Scholar] [CrossRef]
- Connacher, A.A.; Old, D.C.; Phillips, G.; Stewart, W.K.; Grimont, F.; Grimont, P.A. Recurrent peritonitis caused by Serratia marcescens in a diabetic patient receiving continuous ambulatory peritoneal dialysis. J. Hosp. Infect. 1988, 11, 155–160. [Google Scholar] [CrossRef]
- Cope, T.E.; Cope, W.; Beaumont, D.M. A case of necrotising fasciitis caused by Serratia marsescens: Extreme age as functional immunosuppression? Age Ageing 2013, 42, 266–268. [Google Scholar] [CrossRef]
- Da Silva, K.E.; Rossato, L.; Jorge, S.; de Oliveira, N.R.; Kremer, F.S.; Campos, V.F.; Pinto, L.D.S.; Dellagostin, O.A.; Simionatto, S. Three challenging cases of infections by multidrug-resistant Serratia marcescens in patients admitted to intensive care units. Braz. J. Microbiol. 2021, 52, 1341–1345. [Google Scholar] [CrossRef]
- Esel, D.; Doganay, M.; Bozdemir, N.; Yildiz, O.; Tezcaner, T.; Sumerkan, B.; Aygen, B.; Selcuklu, A. Polymicrobial ventriculitis and evaluation of an outbreak in a surgical intensive care unit due to inadequate sterilization. J. Hosp. Infect. 2002, 50, 170–174. [Google Scholar] [CrossRef]
- Esmaeilzadeh, M.; Islamian, A.; Lang, J.; Hornef, M.; Suerbaum, S.; Krauss, J. An unusual cause of ventriculoperitoneal shunt infection. JAAPA 2015, 28, 39–42. [Google Scholar] [CrossRef]
- Gammon, J.A.; Schwab, I.; Joseph, P. Gentamicin-resistant Serratia marcescens endophthalmitis. Arch Ophthalmol. 1980, 98, 1221–1223. [Google Scholar] [CrossRef] [PubMed]
- Gona, F.; Caio, C.; Iannolo, G.; Monaco, F.; Di Mento, G.; Cuscino, N.; Fontana, I.; Panarello, G.; Maugeri, G.; Mezzatesta, M.L.; et al. Detection of the IncX3 plasmid carrying bla KPC-3 in a Serratia marcescens strain isolated from a kidney–liver transplanted patient. J. Med. Microbiol. 2017, 66, 1454–1456. [Google Scholar] [CrossRef] [PubMed]
- Heltberg, O.; Skov, F.; Gerner-Smidt, P.; Kolmos, H.; Dybkjaer, E.; Gutschik, E.; Jerne, D.; Jepsen, O.; Weischer, M.; Frederiksen, W. Nosocomial epidemic of Serratia marcescens septicemia ascribed to contaminated blood transfusion bags. Transfusion 1993, 33, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.T.; Cheng, J.F.; Liu, Y.T.; Mao, Y.C.; Wu, M.S.; Liu, P.Y. Genome-based analysis of virulence determinants of a Serratia marcescens strain from soft tissues following a snake bite. Future Microbiol. 2018, 13, 331–343. [Google Scholar] [CrossRef]
- Johnson, J.S.; Croall, J.; Power, J.S.; Armstrong, G.R. Fatal Serratia marcescens meningitis and myocarditis in a patient with an indwelling urinary catheter. J Clin. Pathol. 1998, 51, 789–790. [Google Scholar] [CrossRef]
- Kufel, W.D.; Scrimenti, A.; Steele, J.M. A Case of Septic Shock Due to Serratia marcescens Pyelonephritis and Bacteremia in a Patient Receiving Empagliflozin. J. Pharm. Pract. 2017, 30, 672–675. [Google Scholar] [CrossRef]
- Lee, S.H.; Woo, S.J.; Park, K.H.; Kim, J.H.; Song, J.H.; Heo, J.W.; Yu, H.G.; Yu, Y.S.; Chung, H.; Park, K.U. Serratia marcescens endophthalmitis associated with intravitreal injections of bevacizumab. Eye 2009, 24, 226–232. [Google Scholar] [CrossRef]
- Lewis, A.M.; Stephenson, J.R.; Garner, J.; Afshar, F.; Tabaqchali, S. A hospital outbreak of Serratia marcescens in neurosurgical patients. Epidemiol. Infect. 1989, 102, 69–74. [Google Scholar] [CrossRef]
- Liangpunsakul, S.; Pursell, K. Community-acquired necrotizing fasciitis caused by Serratia marcescens: Case report and review. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 509–510. [Google Scholar] [CrossRef]
- Memon, M.; Raman, V. Serratia marcescens endogenous endophthalmitis in an immunocompetent host. BMJ Case Rep. 2016, 20, bcr2015209887. [Google Scholar] [CrossRef] [Green Version]
- Neonakis, I.; Messaritakis, H.; Stafylaki, D.; Maraki, S. First detection of a metallo-β-lactamase producing Serratia marcescens in a European university hospital. Indian J. Med. Microbiol. 2014, 32, 352–353. [Google Scholar] [CrossRef]
- Paquin, A.; Lepelletier, D.; Leprince, C.; Chamoux, C.; Treilhaud, M.; Despins, P.; Reynaud, A.; Corvec, S. Relapse of Serratia marcescens Sternal Osteitis 15 Years after the First Episode. J. Clin. Microbiol. 2012, 50, 184–186. [Google Scholar] [CrossRef]
- Rehman, T.; Moore, T.A.; Seoane, L. Serratia marcescens necrotizing fasciitis presenting as bilateral breast necrosis. J. Clin. Microbiol. 2012, 50, 3406–3408. [Google Scholar] [CrossRef]
- Reichling, J.J.; Rose, D.N.; Mendelson, M.H.; Hirschman, S.Z. Acute suppurative thyroiditis caused by Serratia marcescens. J. Infect. Dis. 1984, 149, 281. [Google Scholar] [CrossRef]
- Rieber, H.; Frontzek, A.; Pfeifer, Y. Emergence of metallo-β-lactamase GIM-1 in a clinical isolate of Serratia marcescens. Antimicrob. Agents Chemother. 2012, 56, 4945–4947. [Google Scholar] [CrossRef]
- Rodríguez, C.; Brengi, S.; Cáceres, M.A.; Mochi, S.; Viñas, M.R.; Rizza, C.A.; Merletti, G.; Bru, E.; Assa, J.D.; Raya, R.R.; et al. Successful management with fosfomycin + ceftazidime of an infection caused by multiple highly-related subtypes of multidrug-resistant and extensively drug-resistant KPC-producing Serratia marcescens. Int. J. Antimicrob. Agents 2018, 52, 737–739. [Google Scholar] [CrossRef]
- Rowsey, J.J.; Newsom, D.L.; Sexton, D.J.; Harms, W.K. Endophthalmitis: Current approaches. Ophthalmology 1982, 89, 1055–1066. [Google Scholar] [CrossRef]
- Rubens, C.E.; McGee, Z.A.; Farrar, W.E., Jr. Loss of an aminoglycoside resistance plasmid by Serratia marcescens during treatment of meningitis with amikacin. J. Infect. Dis. 1980, 141, 346–350. [Google Scholar] [CrossRef]
- Sevencan, N.O.; Cakmakliogullari, E.K.; Ozkan, A.E.; Kayhan, B. An unusual location of squamous cell carcinoma and a rare cutaneous infection caused by Serratia marcescens on the tumoral tissue: A case report. Medicine 2018, 97, e12596. [Google Scholar] [CrossRef]
- Shimizu, S.; Kojima, H.; Yoshida, C.; Suzukawa, K.; Mukai, H.Y.; Hasegawa, Y.; Hitomi, S.; Nagasawa, T. Chorioamnionitis caused by Serratia marcescens in a non-immunocompromised host. J. Clin. Pathol. 2003, 56, 871–872. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.J.; Brookfield, D.S.; Shaw, D.A.; Gray, J. An outbreak of Serratia marcescens infections in a neonatal unit. Lancet 1984, 1, 151–153. [Google Scholar] [CrossRef] [PubMed]
- Tsakris, A.; Voulgari, E.; Poulou, A.; Kimouli, M.; Pournaras, S.; Ranellou, K.; Kosmopoulou, O.; Petropoulou, D. In Vivo Acquisition of a Plasmid-Mediated bla KPC-2 Gene among Clonal Isolates of Serratia marcescens. J. Clin. Microbiol. 2010, 48, 2546–2549. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.-J.; Yang, H.-F.; Liu, Y.-Y.; Mei, Q.; Ye, Y.; Li, H.-R.; Cheng, J.; Li, J.-B. The Emergence of the 16S rRNA Methyltransferase RmtB in a Multidrug-Resistant Serratia marcescens Isolate in China. Ann. Lab. Med. 2015, 35, 172–174. [Google Scholar] [CrossRef] [PubMed]
- Piccirilli, A.; Cherubini, S.; Brisdelli, F.; Fazii, P.; Stanziale, A.; Di Valerio, S.; Chiavaroli, V.; Principe, L.; Perilli, M. Molecular Characterization by Whole-Genome Sequencing of Clinical and Environmental Serratia marcescens Strains Isolated during an Outbreak in a Neonatal Intensive Care Unit (NICU). Diagnostics 2022, 12, 2180. [Google Scholar] [CrossRef]
- Cristina, M.L.; Sartini, M.; Spagnolo, A.M. Serratia marcescens Infections in Neonatal Intensive Care Units (NICUs). Int. J. Environ. Res. Public Health 2019, 16, 610. [Google Scholar] [CrossRef]
- Casolari, C.; Pecorari, M.; Fabio, G.; Cattani, S.; Venturelli, C.; Piccinini, L.; Tamassia, M.; Gennari, W.; Sabbatini, A.; Leporati, G.; et al. A simultaneous outbreak of Serratia marcescens and Klebsiella pneumoniae in a neonatal intensive care unit. J. Hosp. Infect. 2005, 61, 312–320. [Google Scholar] [CrossRef]
- Stock, I.; Grueger, T.; Wiedemann, B. Natural antibiotic susceptibility of strains of Serratia marcescens and the S. liquefaciens complex: S. liquefacienssensustricto, S. proteamaculans and S. grimesii. Int. J. Antimicrob. Agents 2003, 22, 35–47. [Google Scholar] [CrossRef]
- Qureshi, Z.A.; Paterson, D.; Pakstis, D.L.; Adams-Haduch, J.M.; Sandkovsky, G.; Sordillo, E.; Polsky, B.; Peleg, A.; Bhussar, M.K.; Doi, Y. Risk factors and outcome of extended-spectrum β-lactamase-producing Enterobacter cloacae bloodstream infections. Int. J. Antimicrob. Agents 2011, 37, 26–32. [Google Scholar] [CrossRef]
- Douglas, S.; Catessa, H.; Garret, C.C. An Antimicrobial Treatment Assessment of Serratia marcescens Bacteremia and Endocarditis. Front. Antibiot. 2022, 1, 942721. [Google Scholar] [CrossRef]
- Sarvikivi, E.; Lyytikäinen, O.; Salmenlinna, S.; Vuopio-Varkila, J.; Luukkainen, P.; Tarkka, E.; Saxén, H. Clustering of Serratia marcescens Infections in a Neonatal Intensive Care Unit. Infect. Control. Hosp. Epidemiol. 2004, 25, 723–729. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Zaric, R.Z.; Jankovic, S.; Zaric, M.; Milosavljevic, M.; Stojadinovic, M.; Pejcic, A. Antimicrobial treatment of Morganella morganii invasive infections: Systematic review. Indian J. Med. Microbiol. 2021, 39, 404–412. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Publication ID | Study Design | Attrition/Reporting Bias | Age | Gender | Site of Isolation of SM | Morphological Diagnosis of Infection | AB Used for Therapy | Outcomes of AB Treatment |
|---|---|---|---|---|---|---|---|---|
| Altweg et al., 1989 [12] | Case series | Low/High | NR | NR | Blood | NR | NR | CR |
| Altweg et al., 1989 [12] | Case series | Low/High | NR | NR | Bronchoalveolar lavage sample | P | NR | CR |
| Blajchman et al., 1979 [13] | Case series | Low/High | NR | M | Blood | NR | NR | CR |
| Blajchman et al., 1979 [13] | Case series | Low/High | NR | F | Blood | NR | NR | Death |
| Cambell et al., 1992 [14] | Case series | Low/Low | Newborn | F | Blood and cerebrospinal fluid | M | IV ampicillin plus gentamycin; IV cefotaxime plus amikacin | CR |
| Cambell et al., 1992 [14] | Case series | Low/Low | Newborn | M | Blood and cerebrospinal fluid | M | IV vancomycin plus amikacin; IV ampicillin plus gentamycin; amikacin plus cefotaxime; ceftazidime plus intraventricular amikacin | CR |
| Castro-Moraga et al., 2021 [15] | Case report | Low/Low | 3 | M | Pus from bone | O | IV penicillin plus clindamycin plus amikacin; IV ciprofloxacin plus cloxacillin | CR |
| Cayo et al., 2017 [16] | Case report | Low/Low | 59 | F | Blood | NR | IV meropenem; IV piperacillin–tazobactam plus ciprofloxacin | CR |
| Conacher et al., 1988 [17] | Case report | Low/Low | 49 | M | Peritoneal fluid | Pe | IP ceftriaxone plus gentamycin; IP gentamycin plus piperacillin plus cotrimoxazole | Death |
| Cope et al., 2013 [18] | Case report | Low/Low | 97 | F | Legg fascia tissue | F | NR | Death |
| Da Silva et al., 2021 [19] | Case series | Low/High | 57 | M | Bronchoalveolar lavage sample and urine | P | IV imipenem–cilastatin; ciprofloxacin | Death |
| Da Silva et al., 2021 [19] | Case series | Low/High | 52 | M | Urine | NR | IV piperacillin–tazobactam plus cotrimoxazole; meropenem plus vancomycin; ciprofloxacin | Death |
| Esel et al., 2002 [20] | Case series | Low/High | NR | NR | Blood and wound pus | Md | IV ciprofloxacin plus amikacin | CR |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Blood and wound pus | Md | IV imipenem plus amikacin | Death |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Blood and wound pus | Md | IV imipenem plus amikacin | CR |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Blood | Ed | IV ciprofloxacin plus amikacin | CR |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Blood | NR | IV ciprofloxacin plus amikacin | Death |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Blood | Ed | IV ciprofloxacin plus amikacin | Death |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Wound pus | WI | IV ciprofloxacin plus amikacin | CR |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Blood | NR | IV ciprofloxacin plus amikacin | CR |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Thoracic fluid | Md | IV ciprofloxacin plus amikacin | CR |
| Esel et al., 2002 | Case series | Low/High | NR | NR | Wound pus | Md | IV ciprofloxacin plus amikacin | Death |
| Esmelizadeh et al., 2015 [21] | Case series | Low/Low | 31 | F | Urine and cerebrospinal fluid | M | IV meropenem plus ceftazidime | Death |
| Esmelizadeh et al., 2015 | Case series | Low/Low | 39 | F | Wound pus and blood | WI | IV ceftriaxone plus ciprofloxacin; piperacillin–tazobactam; ciprofloxacin plus meropenem | CR |
| Gammon et al., 1980 [22] | Case report | Low/High | 60 | F | Urine and corpus vitreum | E | IV cefapirin; Tp gentamicin; amikacin | Death |
| Gona et al., 2017 [23] | Case report | High/High | NR | M | Bronchial lavage sample | P | NR | NR |
| Heltberg et al., 1993 [24] | Case series | Low/High | 71 | M | Blood | NR | IV penicillin G | CR |
| Heltberg et al., 1993 | Case series | Low/High | 52 | M | Blood | NR | IV gentamicin plus PO ciprofloxacin | Died from malignancy |
| Heltberg et al., 1993 | Case series | Low/High | 73 | M | Blood and urine | NR | PO ciprofloxacin; pivampicillin; pivmecillinam | Death |
| Huang et al., 2018 [25] | Case report | Low/High | 57 | M | Tissue culture | GL | NR | PR |
| Jonson et al., 1998 [26] | Case report | Low/Low | 83 | M | Urine, meninges, myocardium | M, My | IV cefuroxime | Death |
| Kufel et al., 2016 [27] | Case report | Low/Low | 75 | M | Urine and blood | NR | IV ceftriaxone; ciprofloxacin | CR |
| Lee et al., 2010 [28] | Case series | Low/High | 53 | M | Corpus vitreum | E | INV vancomycin and amikacin; vancomycin plus ceftazidime | PR |
| Lee et al., 2010 | Case series | Low/Low | 68 | M | Corpus vitreum | E | INV vancomycin plus ceftazidime | PR |
| Lewis et al., 1982 [29] | Case series | Low/High | 62 | F | Cerebrospinal fluid | M | IV ceftazidime; gentamycin; chloramphenicol plus flucloxacillin | Death |
| Lewis et al., 1982 | Case series | Low/High | 25 | M | Cerebrospinal fluid | M | IV ceftazidime plus gentamycin | CR |
| Liangpunsakul et al., 2001 [30] | Case report | Low/Low | 25 | M | Cerebrospinal fluid | M | IV clindamycin plus penicillin G plus ceftriaxone | Death |
| Memon et al., 2016 [31] | Case report | Low/Low | 66 | M | Corpus vitreum | E | IV levofloxacin plus Tp guttae ofloxacin plus Tp guttae ceftazidime | PR |
| Neonakis et al., 2014 [32] | Case report | High/High | 67 | NR | Peritoneal fluid and urine and bronchoalveolar sample | P | IV moxifloxacin plus tigecycline | CR |
| Paquin et al., 2021 [33] | Case report | Low/Low | 61 | M | Sternal collection | O | IV ceftriaxone plus gentamycin | Death |
| Rehman et al., 2012 [34] | Case report | Low/Low | 54 | F | Blood and part of the fascia | F | IV vancomycin plus piperacillin–tazobactam plus ciprofloxacin; doripenem | Death |
| Reichling et al., 1984 [35] | Case report | Low/Low | 58 | F | Thyroid abscess, blood, urine | T | IV moxalactam; cefotaxime | CR |
| Rieber et al., 2012 [36] | Case report | High/High | 53 | M | Blood and urine | NR | IV Imipenem | CR |
| Rodrigues et al., 2018 [37] | Case report | Low/High | NR | NR | Bone and soft tissue | O | IV fosfomycin plus ceftazidime | CR |
| Rowsey et al., 1982 [38] | Case report | Low/Low | 83 | F | Corpus vitreum | E | IC gentamicin and cephaloridine; gentamicin plus cephaloridine SB; gentamicin, cephaloridine a SB; IV gentamicin and cefazolin; IC gentamicin plus ticarcillin plus SC gentamicin, ticarcillin | CR |
| Rubens et al., 1980 [39] | Case report | Low/High | Newborn | M | Cerebrospinal fluid | M | IV gentamycin; amikacin | CR |
| Sevencan et al., 2018 [40] | Case report | Low/Low | 89 | M | Wound pus | IV ciprofloxacin | CR | |
| Shimizu et al., 2003 [41] | Case report | Low/High | 26 | F | Blood, urine, and vaginal discharge | Ch | IV cefotiam; ceftazidime plus imipenem/cilastatin | PR |
| Smith et al., 1984 [42] | Case series | Low/High | 28 weeks | NR | Blood | NR | NR | CR |
| Smith et al., 1984 | Case series | Low/High | 31 weeks | NR | Blood | NR | NR | Death |
| Smith et al., 1984 | Case series | Low/High | 28 weeks | NR | Blood | NR | NR | Death |
| Smith et al., 1984 | Case series | Low/High | 26 weeks | NR | Blood | NR | NR | Death |
| Smith et al., 1984 | Case series | Low/High | 30 weeks | NR | Sputum | P | NR | CR |
| Smith et al., 1984 | Case series | Low/High | 28 weeks | NR | Sputum | P | NR | CR |
| Smith et al., 1984 | Case series | Low/High | 28 weeks | NR | Sputum | P | NR | CR |
| Smith et al., 1984 | Case series | Low/High | 34 weeks | M | Sputum | P | NR | Death |
| Tsakris et al., 2010 [43] | Case report | Low/High | 77 | F | Bronchial lavage sample | P | IV tigecycline plus IH colistin | CR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zivkovic Zaric, R.; Zaric, M.; Sekulic, M.; Zornic, N.; Nesic, J.; Rosic, V.; Vulovic, T.; Spasic, M.; Vuleta, M.; Jovanovic, J.; et al. Antimicrobial Treatment of Serratia marcescens Invasive Infections: Systematic Review. Antibiotics 2023, 12, 367. https://doi.org/10.3390/antibiotics12020367
Zivkovic Zaric R, Zaric M, Sekulic M, Zornic N, Nesic J, Rosic V, Vulovic T, Spasic M, Vuleta M, Jovanovic J, et al. Antimicrobial Treatment of Serratia marcescens Invasive Infections: Systematic Review. Antibiotics. 2023; 12(2):367. https://doi.org/10.3390/antibiotics12020367
Chicago/Turabian StyleZivkovic Zaric, Radica, Milan Zaric, Marija Sekulic, Nenad Zornic, Jelena Nesic, Vesna Rosic, Tatjana Vulovic, Marko Spasic, Marko Vuleta, Jovan Jovanovic, and et al. 2023. "Antimicrobial Treatment of Serratia marcescens Invasive Infections: Systematic Review" Antibiotics 12, no. 2: 367. https://doi.org/10.3390/antibiotics12020367
APA StyleZivkovic Zaric, R., Zaric, M., Sekulic, M., Zornic, N., Nesic, J., Rosic, V., Vulovic, T., Spasic, M., Vuleta, M., Jovanovic, J., Jovanovic, D., Jakovljevic, S., & Canovic, P. (2023). Antimicrobial Treatment of Serratia marcescens Invasive Infections: Systematic Review. Antibiotics, 12(2), 367. https://doi.org/10.3390/antibiotics12020367