

On the Potential of Relational Databases for the Detection of Clusters of Infection and Antibiotic Resistance Patterns

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
1.1. The Spread of Infections
1.2. Klebsiella Pneumoniae
1.3. Antibiotic Resistance
1.4. The Role of Prevention
2. Databases Technology and Content
2.1. Relational Databases as Decision Support Systems
2.2. The Database
3. Results
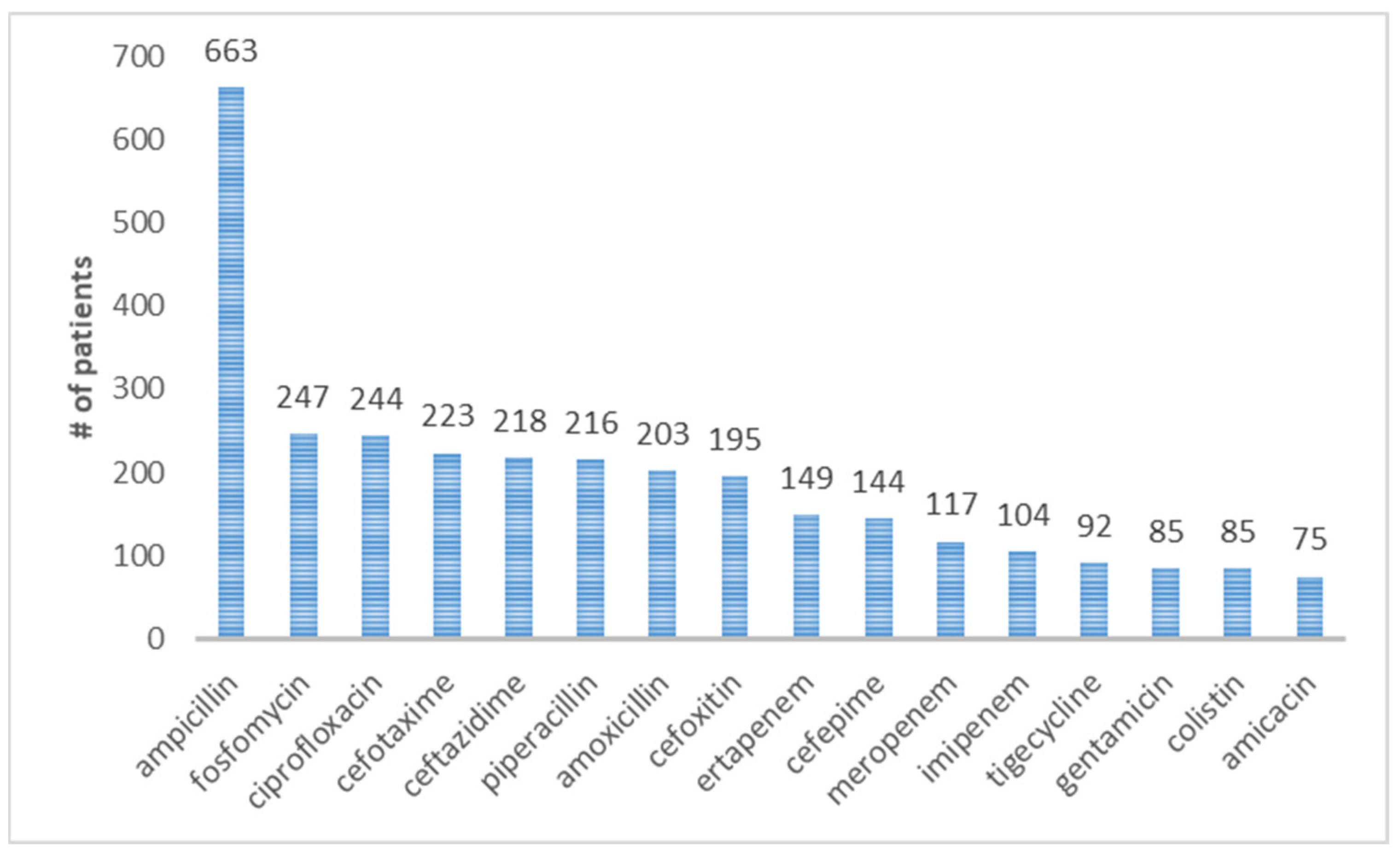
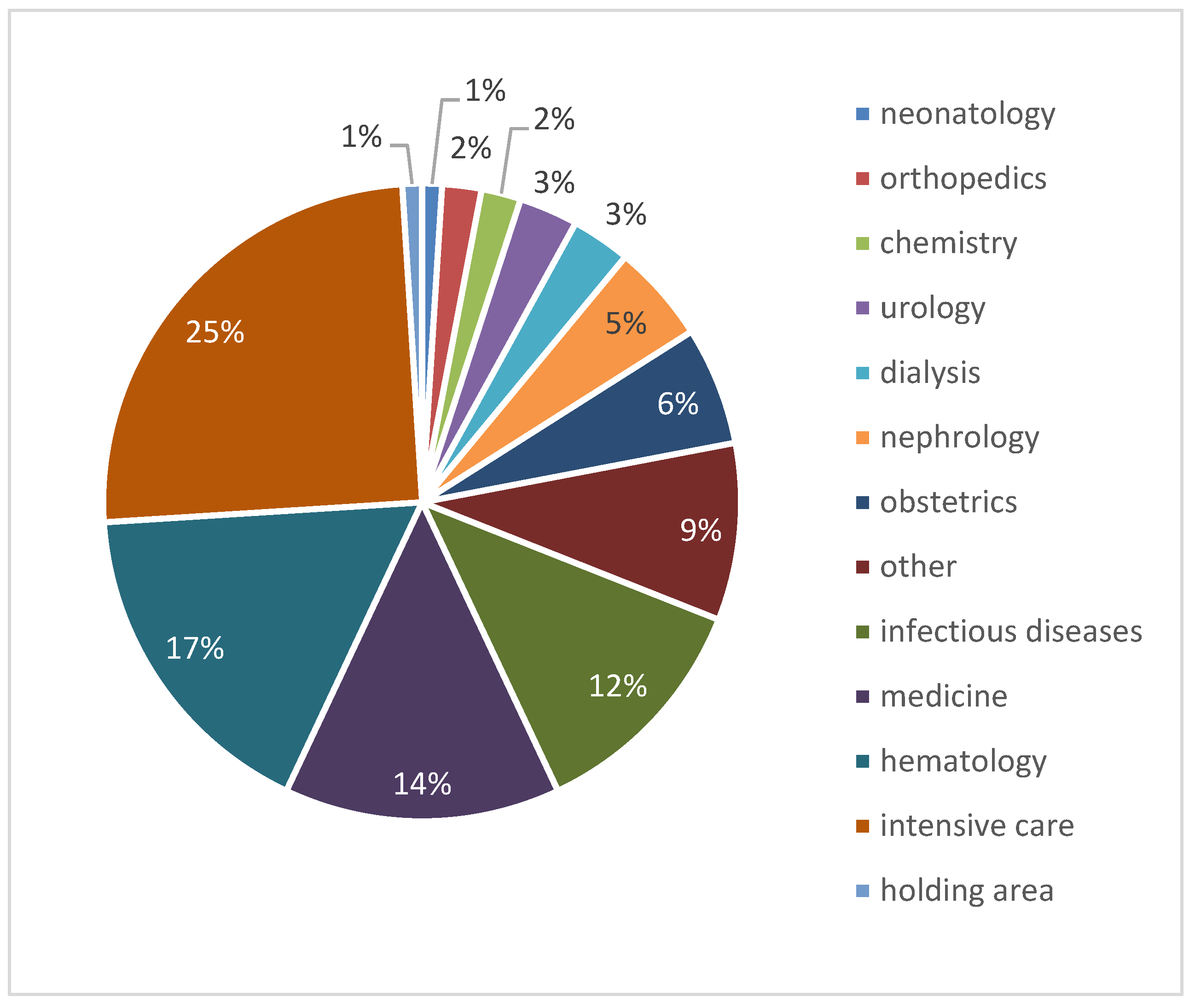
3.1. Global Statistics
3.2. Statistics of Provenance and Antibiotic Resistance for External Patients
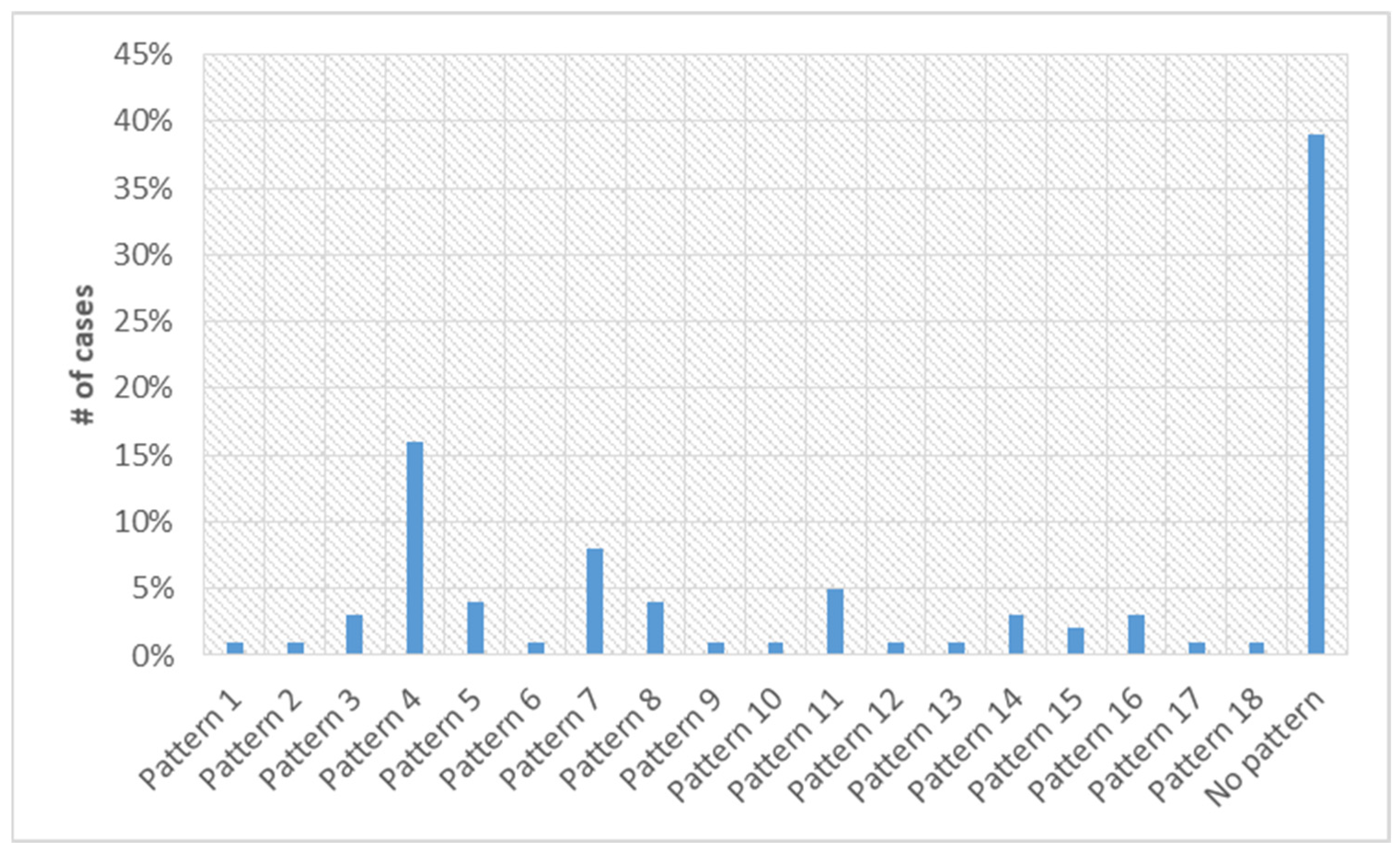
3.3. Statistics of Nosocomial Cases
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abbott, L.S. Klebsiella, Enterobacter, Citrobacter, Serratia, Plesiomonas, and Other Enterobacteriacae. In Manuel of Clinical Microbiology; Murray, P.R., Baron, J.O.E., Jorgensen, J.H., Candry, M.L., Pfaller, M.A., Eds.; Wiley: Hoboken, NJ, USA, 2007; pp. 705–711. [Google Scholar]
- Akova, M.; Daikos, G.; Tzouvelekis, L.; Carmeli, Y. Interventional strategies and current clinical experience with carbapenemase-producing Gram-negative bacteria. Clin. Microbiol. Infect. 2012, 18, 439–448. [Google Scholar] [CrossRef]
- Sanchez, G.V.; Master, R.N.; Clark, R.B.; Fyyaz, M.; Duvvuri, P.; Ekta, G.; Bordon, J. Klebsiella pneumoniae an-timicrobial drug resistance, United States, 1998–2010. Emerg. Infect. Dis. 2013, 19, 133–136. [Google Scholar] [CrossRef]
- Schmidt, H.; Hensel, M. Pathogenicity Islands in Bacterial Pathogenesis. Clin. Microbiol. Rev. 2004, 17, 14–56. [Google Scholar] [CrossRef]
- Alberts, B.; Johnson, A.; Lewis, J.; Walter, P.; Raff, M.; Roberts, K. Molecular Biology of the Cell 4th Edition: International Student Edition; Garland Science: Wolverhampton, UK, 2002. [Google Scholar]
- Mack, A.; Relman, D.A.; Choffnes, E.R. (Eds.) Antibiotic Resistance: Implications for Global Health and Novel Intervention Strategies: Workshop Summary; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Friis, R.H.; Sellers, T. Epidemiology for Public Health Practice; Jones & Bartlett Publishers: Boston, MA, USA, 2013. [Google Scholar]
- Euzéby, J.P. List of Bacterial Names with Standing in Nomenclature: A Folder Available on the Internet. Int. J. Syst. Evol. Microbiol. 1997, 47, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Fair, R.J.; Tor, Y. Antibiotics and Bacterial Resistance in the 21st Century. Perspect. Med. Chem. 2014, 6, S14459. [Google Scholar] [CrossRef] [PubMed]
- Riggs, M.M.; Sethi, A.K.; Zabarsky, T.F.; Eckstein, E.C.; Jump, R.L.; Donskey, C.J. Asymptomatic carriers are a potential source for transmission of epidemic and nonepidemic Clostridium difficile strains among long-term care facility res-idents. Clin. Infect. Dis. 2007, 45, 992–998. [Google Scholar] [CrossRef]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate Point-Prevalence Survey of Health Care–Associated Infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef]
- Tulchinsky, T.H.; Varavikova, E.A. The New Public Health; Academic Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Thomas, R.J. Particle size and pathogenicity in the respiratory tract. Virulence 2013, 4, 847–858. [Google Scholar] [CrossRef] [PubMed]
- Tzouvelekis, L.S.; Markogiannakis, A.; Psichogiou, M.; Tassios, P.T.; Daikos, G.L. Carbapenemases in Klebsiella pneumoniae and other Enterobacteriaceae: An evolving crisis of global dimensions. Clin. Microbiol. Rev. 2012, 25, 682–707. [Google Scholar] [CrossRef]
- Eisenberg, J.N.; Desai, M.A.; Levy, K.; Bates, S.J.; Liang, S.; Naumoff, K.; Scott, J.C. Environmental Determinants of Infectious Disease: A Framework for Tracking Causal Links and Guiding Public Health Research. Environ. Health Perspect. 2007, 115, 1216–1223. [Google Scholar] [CrossRef]
- Duffy, J.; Sievert, D.; Rebmann, C.; Kainer, M.; Lynfield, R.; Smith, P.; Fridkin, S. Effective State-Based Surveillance for Multidrug-Resistant Organisms Related to Health Ca re-Associated Infections. Public Health Rep. 2011, 126, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Guggenbichler, J.P.; Assadian, O.; Boeswald, M.; Kramer, A. Incidence and clinical implication of nosocomial infec-tions associated with implantable biomaterials–catheters, ventilator-associated pneumonia, urinary tract infections. GMS Krankenh. Interdiszip. 2011, 6. [Google Scholar] [CrossRef]
- Barton, A. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. AORN J. 2009, 90, 601–602. [Google Scholar] [CrossRef]
- Battersby, S. (Ed.) Clay’s Handbook of Environmental Health; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Lawlor, M.S.; Hsu, J.; Rick, P.D.; Miller, V.L. Identification of Klebsiella pneumoniae virulence determinants using an intranasal infection model. Mol. Microbiol. 2005, 58, 1054–1073. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.L. Resistance in Gram-Negative Bacteria: Enterobacteriaceae. Am. J. Med. 2006, 119, S20–S28. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.L.; Bonomo, R.A. Extended-Spectrum β-Lactamases: A Clinical Update. Clin. Microbiol. Rev. 2005, 18, 657–686. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.W. Bacterial pathogenesis. In Med. Microbiol.; 1996; 592. Available online: https://pubmed.ncbi.nlm.nih.gov/21413346/ (accessed on 12 April 2023).
- Ventola, C.L. The Antibiotic Resistance Crisis: Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Podshum, R.; Ullmann, U. Klebsiella spp. as nosocomial pathogens: Epidemiology, taxonomy, typing methods, and pathogenicity factors. Clin. Microbiol. Rev. 1998, 11, 589–603. [Google Scholar] [CrossRef]
- Sydnor, E.R.M.; Perl, T.M. Hospital Epidemiology and Infection Control in Acute-Care Settings. Clin. Microbiol. Rev. 2011, 24, 141–173. [Google Scholar] [CrossRef]
- Sun, Y.; Patel, A.; SantaLucia, J.; Roberts, E.; Zhao, L.; Kaye, K.; Rao, K.; Bachman, M.A. Measurement of Klebsiella Intestinal Colonization Density To Assess Infection Risk. Msphere 2021, 6, e0050021. [Google Scholar] [CrossRef] [PubMed]
- Brisse, S.; Fevre, C.; Passet, V.; Issenhuth-Jeanjean, S.; Tournebize, R.; Diancourt, L.; Grimont, P. Virulent Clones of Klebsiella pneumoniae: Identification and Evolutionary Scenario Based on Genomic and Phenotypic Characterization. PLoS ONE 2009, 4, e4982. [Google Scholar] [CrossRef]
- Bowler, P.G.; Duerden, B.I.; Armstrong, D.G. Wound microbiology and associated approaches to wound management. Clin. Microbiol. Rev. 2001, 14, 244–269. [Google Scholar] [CrossRef]
- Bouza, E.; Cercenado, E. Klebsiella and enterobacter: Antibiotic resistance and treatment implications. In Proceedings of the Seminars in Respiratory Infections, London, UK, 1 September 2002; Volume 17, pp. 215–230. [Google Scholar]
- Snitkin, E.S.; Zelazny, A.M.; Thomas, P.J.; Stock, F.; Henderson, D.K.; Palmore, T.N.; Segre, J.A.; NISC; Comparative Sequencing Program. Tracking a hospital outbreak of carbapenem-resistant Klebsiella pneumoniae with whole-genome sequencing. Sci. Transl. Med. 2012, 4, 148ra116. [Google Scholar] [CrossRef] [PubMed]
- Struve, C.; Roe, C.C.; Stegger, M.; Stahlhut, S.G.; Hansen, D.S.; Engelthaler, D.M.; Andersen, P.S.; Driebe, E.M.; Keim, P.; Krogfelt, K.A. Mapping the Evolution of Hypervirulent Klebsiella pneumoniae. mBio 2015, 6, e00630-15. [Google Scholar] [CrossRef]
- Doorduijn, D.J.; Rooijakkers, S.H.; van Schaik, W.; Bardoel, B.W. Complement resistance mechanisms of Klebsiella pneumoniae. Immunobiology 2016, 221, 1102–1109. [Google Scholar] [CrossRef]
- Conway, M.J.; Colpitts, T.M.; Fikrig, E. Role of the Vector in Arbovirus Transmission. Annu. Rev. Virol. 2014, 1, 71–88. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Davies, D. Origins and Evolution of Antibiotic Resistance. Microbiol. Mol. Biol. Rev. 2010, 74, 417–433. [Google Scholar] [CrossRef]
- Shaikh, S.; Fatima, J.; Shakil, S.; Rizvi, S.M.D.; Kamal, M.A. Antibiotic resistance and extended spectrum beta-lactamases: Types, epidemiology and treatment. Saudi J. Biol. Sci. 2015, 22, 90–101. [Google Scholar] [CrossRef]
- Arnold, R.S.; Thom, K.A.; Sharma, S.; Phillips, M.; Johnson, J.K.; Morgan, D.J. Emergence of Klebsiella pneu-moniae carbapenemase (KPC)-producing bacteria. South. Med. J. 2011, 104, 40. [Google Scholar] [CrossRef]
- Petrosillo, N.; Capone, A.; Di Bella, S.; Taglietti, F. Management of antibiotic resistance in the intensive care unit setting. Expert Rev. Anti-Infect. Ther. 2010, 8, 289–302. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Carbapenem-Resistant Enterobacteriaceae in Healthcare Settings; CDC: Atlanta, GA, USA, 2016. [Google Scholar]
- Garbati, M.A.; Al Godhair, A.I. The Growing Resistance of Klebsiella pneumonia; the Need to Expand Our Anti-biogram: Case Report and Review of the Literature. Afr. J. Infect. Dis. 2013, 7, 8–10. [Google Scholar]
- Lin, W.P.; Wang, J.T.; Chang, S.C.; Chang, F.Y.; Fung, C.P.; Chuang, Y.C.; Chen, Y.-S.; Shiau, Y.-R.; Tan, M.-C.; Lai, J.F.; et al. The antimicrobial susceptibility of klebsiella pneumoniae from community settings in Taiwan, a trend analysis. Sci. Rep. 2016, 6, 36280. [Google Scholar] [CrossRef] [PubMed]
- Onori, R.; Gaiarsa, S.; Comandatore, F.; Pongolini, S.; Brisse, S.; Colombo, A.; Cassani, G.; Marone, P.; Grossi, P.; Bandi, C. Tracking nosocomial Klebsiella pneumoniae infections and outbreaks by whole-genome analysis: Small-scale Italian scenario within a single hospital. J. Clin. Microbiol. 2015, 53, 2861–2868. [Google Scholar] [CrossRef]
- Quale, J. Global Spread of Carbapenemase-Producing Klebsiella pneumoniae-These pathogens arose in the mid-1990s and continue to spread, leaving few options for treating infected patients. Microbe 2008, 3, 516. [Google Scholar]
- Ripabelli, G.; Sammarco, M.; Salzo, A.; Scutellà, M.; Felice, V.; Tamburro, M. New Delhi metallo-β-lactamase (NDM-1)-producingKlebsiella pneumoniaeof sequence type ST11: First identification in a hospital of central Italy. Lett. Appl. Microbiol. 2020, 71, 652–659. [Google Scholar] [CrossRef]
- Rahal, J.J. Antimicrobial Resistance among and Therapeutic Options against Gram-Negative Pathogens. Clin. Infect. Dis. 2009, 49, S4–S10. [Google Scholar] [CrossRef] [PubMed]
- Girometti, N.; Lewis, R.E.; Giannella, M.; Ambretti, S.; Bartoletti, M.; Tedeschi, S.; Tumietto, F.; Cristini, F.; Trapani, F.; Viale, P.; et al. Klebsiella pneumoniae bloodstream infection: Epidemiology and impact of inappropriate empirical therapy. Medicine 2014, 93, 298–309. [Google Scholar] [CrossRef]
- Aliabadi, A.A.; Rogak, S.N.; Bartlett, K.H.; Green, S.I. Preventing airborne disease transmission: Review of methods for ventilation design in health care facilities. Adv. Prev. Med. 2011, 2011, 124064. [Google Scholar] [CrossRef]
- Simonsen, K.A.; Anderson-Berry, A.L.; Delair, S.F.; Davies, H.D. Early-onset neonatal sepsis. Clin. Microbiol. Rev. 2014, 27, 21–47. [Google Scholar] [CrossRef]
- Lledo, W.; Hernandez, M.; Lopez, E.; Molinari, O.L.; Soto, R.Q.; Hernandez, E.; Santiago, N.; Flores, M.; Vazquez, G.J.; Robledo, I.E.; et al. Guidance for Control of Infections With Carbapenem-Resistant or Carbapenemase-Producing Enterobacteriaceae in Acute Care Facilities. Jama-J. Am. Med. Assoc. 2009, 301, 1980–1982, reprinted in MMWR 2009, 58, 256–260. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Facility Guidance for Control of Carbapenem-Resistant Enterobacteriaceae (CRE). Update CRE Toolkit; CDC: Atlanta, GA, USA, 2015. [Google Scholar]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L. Management of multidrug-resistant organisms in health care settings, 2006. Am. J. Infect. Control. 2007, 35, S165–S193. [Google Scholar] [CrossRef]
- Zaidi, A.K.; Huskins, W.C.; Thaver, D.; Bhutta, Z.A.; Abbas, Z.; Goldmann, D.A. Hospital-acquired neonatal infections in developing countries. Lancet 2005, 365, 1175–1188. [Google Scholar] [CrossRef]
- Singh, A.; Goering, R.V.; Simjee, S.; Foley, S.L.; Zervos, M.J. Application of Molecular Techniques to the Study of Hospital Infection. Clin. Microbiol. Rev. 2006, 19, 512–530. [Google Scholar] [CrossRef] [PubMed]
- Cano, V.; March, C.; Insua, J.L.; Aguiló, N.; Llobet, E.; Moranta, D.; Regueiro, V.; Brennan, G.P.; Millán-Lou, M.I.; Garmendia, J.; et al. Klebsiella pneumoniae survives within macrophages by avoiding delivery to lysosomes. Cell. Microbiol. 2015, 17, 1537–1560. [Google Scholar] [CrossRef]
- Codd, E.F. A relational model of data for large shared data banks. Commun. ACM 1970, 13, 377–387. [Google Scholar] [CrossRef]
- Connolly, T.M.; Begg, C.E. Database Systems—A Practical Approach to Design Implementation and Management, 6th ed.; Pearson Education: Hudson, NY, USA, 2014; p. 64. ISBN 978-1292061184. Available online: http://www.cherrycreekeducation.com/bbk/b/Pearson_Database_Systems_A_Practical_Approach_to_Design_Implementation_and_Management_6th_Global_Edition_1292061189.pdf (accessed on 12 April 2023).
- Capone, A.; Giannella, M.; Fortini, D.; Giordano, A.; Meledandri, M.; Ballardini, M.; Venditti, M.; Bordi, E.; Capozzi, D.; Tarasi, A.; et al. High rate of col-istin resistance among patients with carbapenem-resistant Klebsiella pneumoniae infection accounts for an excess of mortality. Clin. Microbiol. Infect. 2013, 19, E23–E30. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO manual for surveillance of human transmissible spongiform encephalopathies, including variant Creutzfeldt-Jakob disease. Proc. Natl. Acad. Sci. USA 2003, 101, 3065–3070. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Penicillins | Cephalosporins | Carbapenems | Aminoglycosides | Fluoroquinolones | Glycylcycline | Fosfomycin | Polymyxins | Diaminopyridines | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| penicillins | 45 | 40% | 19 | 17% | 20 | 31% | 35 | 31% | 10 | 9% | 40 | 35% | 16 | 14% | 28 | 25% | ||
| cephalosporins | 45 | 40% | 18 | 17% | 17 | 15% | 30 | 27% | 8 | 7% | 24 | 21% | 11 | 10% | 18 | 16% | ||
| carbapenems | 19 | 17% | 17 | 15% | 7 | 6% | 13 | 12% | 4 | 4% | 12 | 11% | 9 | 8% | 11 | 10% | ||
| aminoglycosides | 20 | 18% | 17 | 15% | 7 | 6% | 17 | 15% | 4 | 4% | 13 | 16% | 5 | 4% | 10 | 9% | ||
| fluoroquinolones | 35 | 31% | 30 | 27% | 13 | 12% | 17 | 15% | 6 | 5% | 18 | 16% | 7 | 6% | 20 | 18% | ||
| glycylcycline | 10 | 9% | 8 | 27% | 4 | 4% | 4 | 4% | 6 | 55% | 8 | 7% | 4 | 4% | 2 | 2% | ||
| fosfomycin | 40 | 35% | 24 | 21% | 12 | 11% | 13 | 12% | 18 | 16% | 8 | 7% | 9 | 8% | 18 | 16% | ||
| polymyxins | 16 | 14% | 11 | 10% | 9 | 8% | 5 | 4% | 7 | 6% | 4 | 4% | 9 | 8% | 6 | 5% | ||
| diaminopyridines | 28 | 25% | 18 | 16% | 11 | 10% | 10 | 9% | 20 | 18% | 2 | 2% | 18 | 16% | 18 | 16% | ||
| Cobined Refreshments | Antibiotics | Frosinone (p = 66) | Veroli (p = 6) | Boville (p = 3) | Ceprano (p = 21) | Ferentino (p = 3) | Ceccano (p = 14) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | penicillins | 41 | 62% | 3 | 50% | 1 | 33% | 17 | 81% | 2 | 67% | 13 | 93% |
| cephalosporins | 42 | 64% | 3 | 50% | 1 | 33% | 17 | 81% | 2 | 67% | 13 | 93% | |
| carbapenems | 50 | 76% | 6 | 100% | 3 | 100% | 20 | 95% | 2 | 67% | 13 | 93% | |
| 1 | aminoglycosides | 53 | 80% | 3 | 50% | 2 | 67% | 19 | 90% | 3 | 100% | 13 | 93% |
| fluoroquinolones | 46 | 70% | 3 | 50% | 1 | 33% | 18 | 86% | 3 | 100% | 13 | 93% | |
| glycylcycline | 61 | 92% | 6 | 100% | 3 | 100% | 20 | 95% | 2 | 67% | 13 | 93% | |
| 2 | fosfomycin | 50 | 76% | 5 | 83% | 1 | 33% | 18 | 86% | 3 | 100% | 13 | 93% |
| polymyxins | 59 | 89% | 6 | 100% | 3 | 100% | 19 | 90% | 2 | 67% | 13 | 93% | |
| diaminopyridines | 49 | 74% | 5 | 83% | 1 | 33% | 19 | 90% | 3 | 100% | 14 | 100% | |
| 3 | penicillins | 20 | 30% | 3 | 50% | 2 | 67% | 3 | 14% | 1 | 33% | 0 | 0% |
| cephalosporins | 18 | 27% | 3 | 50% | 2 | 67% | 2 | 10% | 1 | 33% | 0 | 0% | |
| carbapenems | 11 | 17% | 0 | 0% | 0 | 67% | 0 | 0% | 1 | 33% | 0 | 0% | |
| 6 | aminoglycosides | 9 | 14% | 3 | 50% | 1 | 0% | 1 | 5% | 0 | 0% | 0 | 0% |
| fluoroquinolones | 15 | 23% | 3 | 50% | 2 | 33% | 1 | 5% | 0 | 0% | 0 | 0% | |
| glycylcycline | 3 | 5% | 0 | 0% | 0 | 67% | 0 | 0% | 1 | 33% | 0 | 0% | |
| 5 | fosfomycin | 10 | 15% | 1 | 17% | 2 | 0% | 2 | 10% | 0 | 0% | 0 | 0% |
| polymyxins | 6 | 9% | 3 | 0% | 0 | 67% | 1 | 5% | 1 | 33% | 0 | 0% | |
| diaminopyridines | 11 | 17% | 1 | 17% | 2 | 0% | 2 | 10% | 0 | 0% | 0 | 0% | |
| 6 | penicillins | 5 | 8% | 0 | 0% | 0 | 0% | 1 | 5% | 0 | 0% | 1 | 7% |
| cephalosporins | 6 | 9% | 0 | 0% | 0 | 0% | 2 | 10% | 0 | 0% | 1 | 7% | |
| carbapenems | 5 | 8% | 0 | 0% | 0 | 0% | 1 | 5% | 0 | 0% | 1 | 7% | |
| 7 | aminoglycosides | 4 | 6% | 0 | 0% | 0 | 0% | 1 | 5% | 0 | 0% | 1 | 7% |
| fluoroquinolones | 5 | 8% | 0 | 0% | 0 | 0% | 2 | 10% | 0 | 0% | 1 | 7% | |
| glycylcycline | 2 | 3% | 0 | 0% | 0 | 0% | 1 | 5% | 0 | 0% | 1 | 7% | |
| 8 | fosfomycin | 6 | 9% | 0 | 0% | 0 | 0% | 1 | 5% | 0 | 0% | 1 | 7% |
| polymyxins | 1 | 2% | 0 | 0% | 0 | 0% | 1 | 5% | 0 | 0% | 1 | 7% | |
| diaminopyridines | 6 | 9% | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% | 0 | 0% | |
| Antibiotics/Pattern | Pattern 4 | Pattern 7 | Pattern 11 | Pattern 5 | Pattern 8 | Pattern 3 | Pattern 16 |
|---|---|---|---|---|---|---|---|
| Ampicillin | |||||||
| Amoxicillin | |||||||
| Piperacillin | |||||||
| Cefoxitin | |||||||
| Cefotaxime | |||||||
| Ceftazidime | |||||||
| Cefepime | |||||||
| Ertapenem | |||||||
| Imipenem | |||||||
| Meropenem | |||||||
| Amicacina | |||||||
| Gentamicin | |||||||
| Ciprofloxacin | |||||||
| Tigecycline | |||||||
| Fosfomycin | |||||||
| Colistin |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gelfusa, M.; Murari, A.; Ludovici, G.M.; Franchi, C.; Gelfusa, C.; Malizia, A.; Gaudio, P.; Farinelli, G.; Panella, G.; Gargiulo, C.; et al. On the Potential of Relational Databases for the Detection of Clusters of Infection and Antibiotic Resistance Patterns. Antibiotics 2023, 12, 784. https://doi.org/10.3390/antibiotics12040784
Gelfusa M, Murari A, Ludovici GM, Franchi C, Gelfusa C, Malizia A, Gaudio P, Farinelli G, Panella G, Gargiulo C, et al. On the Potential of Relational Databases for the Detection of Clusters of Infection and Antibiotic Resistance Patterns. Antibiotics. 2023; 12(4):784. https://doi.org/10.3390/antibiotics12040784
Chicago/Turabian StyleGelfusa, Michela, Andrea Murari, Gian Marco Ludovici, Cristiano Franchi, Claudio Gelfusa, Andrea Malizia, Pasqualino Gaudio, Giovanni Farinelli, Giacinto Panella, Carla Gargiulo, and et al. 2023. "On the Potential of Relational Databases for the Detection of Clusters of Infection and Antibiotic Resistance Patterns" Antibiotics 12, no. 4: 784. https://doi.org/10.3390/antibiotics12040784
APA StyleGelfusa, M., Murari, A., Ludovici, G. M., Franchi, C., Gelfusa, C., Malizia, A., Gaudio, P., Farinelli, G., Panella, G., Gargiulo, C., & Casinelli, K. (2023). On the Potential of Relational Databases for the Detection of Clusters of Infection and Antibiotic Resistance Patterns. Antibiotics, 12(4), 784. https://doi.org/10.3390/antibiotics12040784