


Prevalence and Antibiotic Resistance Pattern of Streptococcus, Staphylococcus, Neisseria meningitidis and Enterobacteriaceae in Two Reference Hospitals of Yaoundé: An Overview before and during COVID-19 Pandemic Era
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Age and Sex of the Study Population
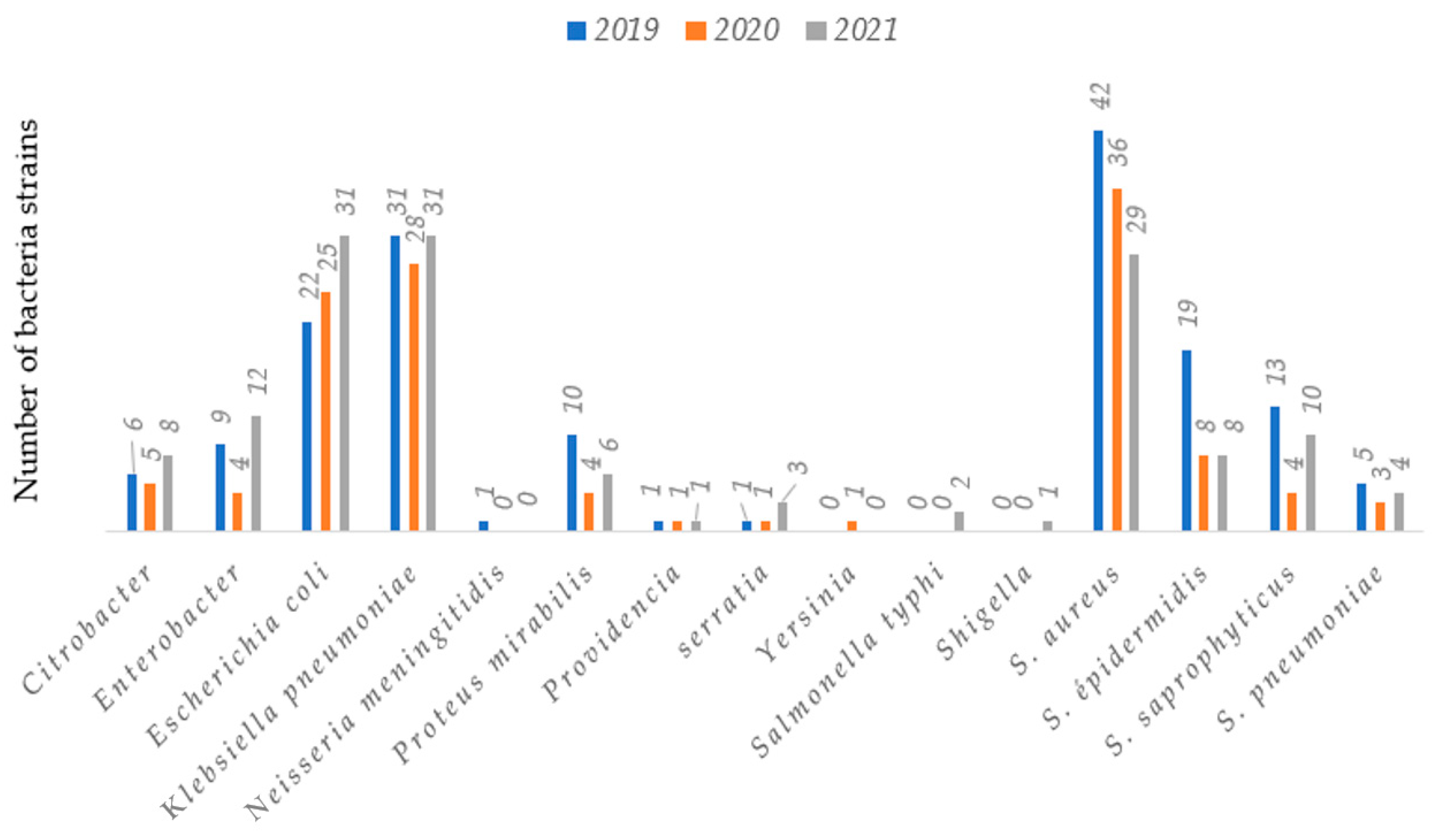
2.2. Bacteria Profile of the Study Population
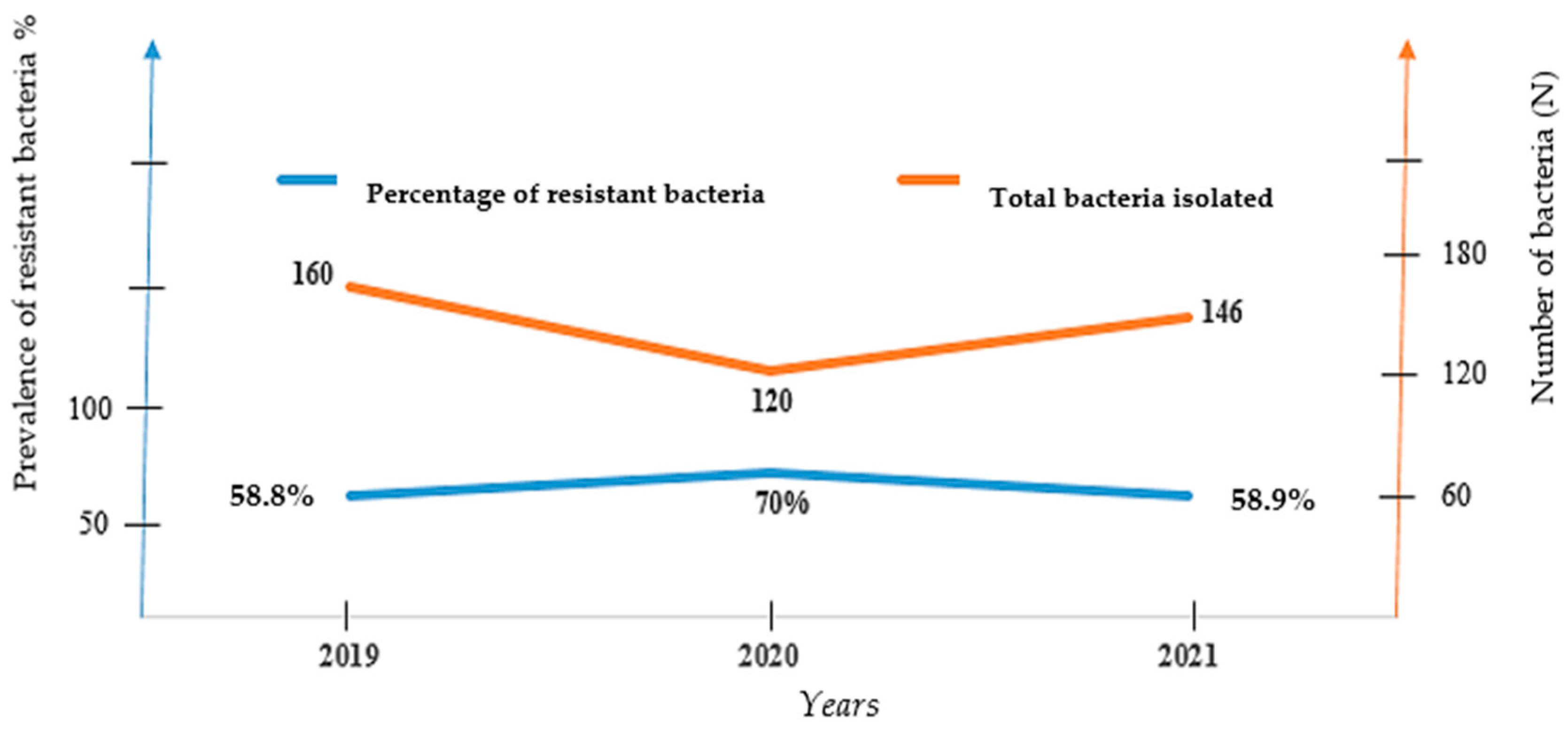
2.3. Number of Bacteria Isolate and Their Corresponding Resistance Rate over Years
2.4. Resistance Pattern of Bacterial Strains Isolated in 2019, 2020 and 2021
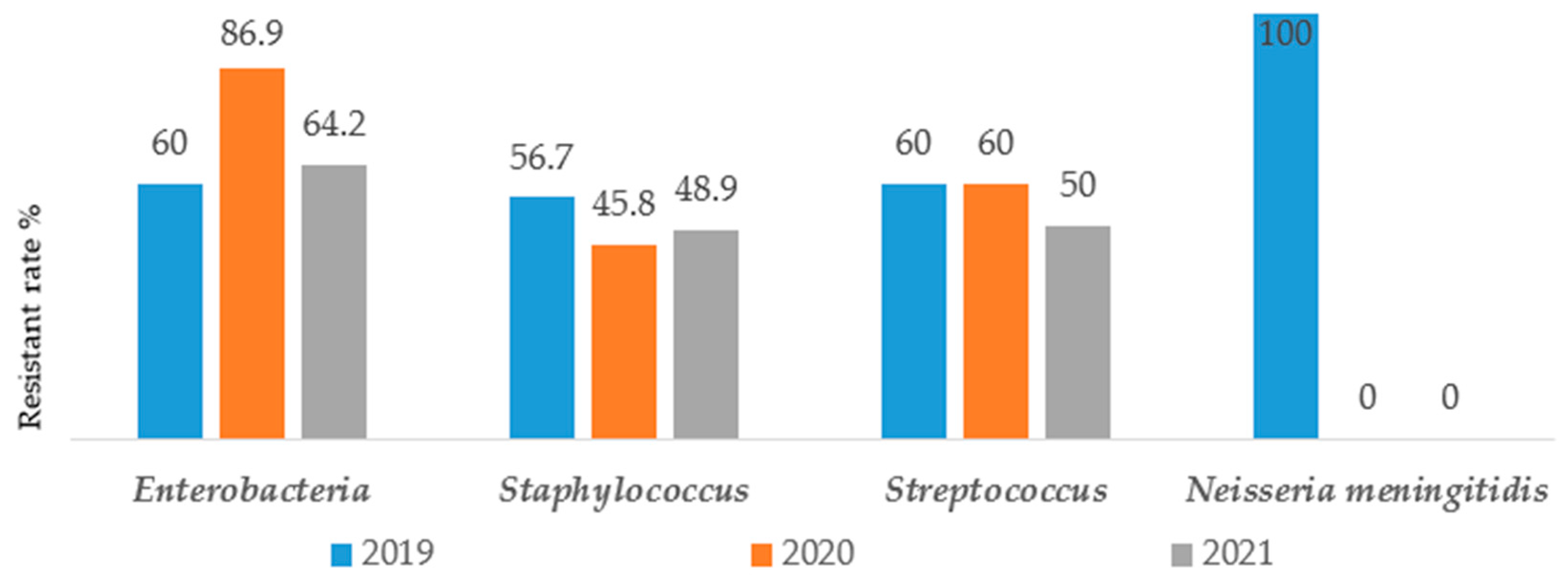
2.4.1. Resistance Rate by Group of Bacteria
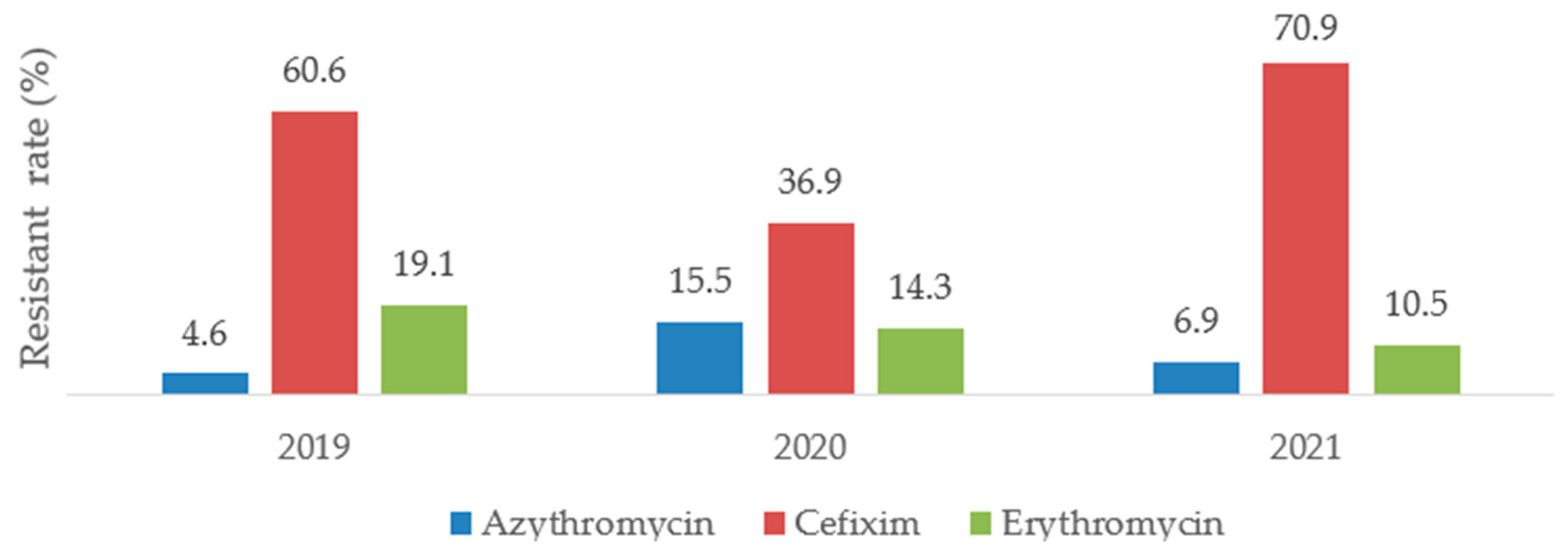
2.4.2. Global Resistance Rate of Bacteria according to the Antibiotics of Interest
2.4.3. Resistant Rate according to the COVID-19 Era and Year of Isolation
2.4.4. Bacteria Resistant Rate before and during COVID-19 Pandemic Era according to Gender
2.4.5. Age and Global Resistance Rate according to COVID-19 Pandemic Era
2.5. Repartition of Bacterial Resistant Rate to Selected Antibiotics before (2019) and during COVID-19 Pandemic (2020 and 2021)
3. Discussion
4. Materials and Methods
4.1. Study Duration and Location
4.2. Sampling Method and Sampling Population
4.3. Microbiological Methods
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Antibiotic Resistance, Key Facts. 31 July 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 24 April 2023).
- WHO. Publication of the List of Bacteria Against Which New Antibiotics Are Urgently Needed; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Gómez-Lus, L.R. Evolución de la resistencia bacteriana a los antibióticos. An. Real Acad. Nac. Med. 2003, 120, 717–726. (In Spanish) [Google Scholar]
- Davies, J.E. Origins, acquisition and dissemination of antibiotic resistance determinants. Ciba Found. Symp. 1997, 207, 15–27. [Google Scholar] [PubMed]
- Munita, J.M.; Arias, C.A. Mechanisms of Antibiotic Resistance. Microbiol. Spectr. 2016, 4, 481–511. [Google Scholar] [CrossRef] [PubMed]
- Nicole, A.L.; Andrew, D.S.C. Horizontal transfer of antibiotic resistance genes in clinical environments. Can. J. Microbiol. 2018, 65, 34–44. [Google Scholar] [CrossRef]
- Malik, S.S.; Mundra, S. Increasing Consumption of Antibiotics during the COVID-19 Pandemic: Implications for Patient Health and Emerging Anti-Microbial Resistance. Antibiotics 2022, 12, 45. [Google Scholar] [CrossRef]
- Kariyawasam, R.M.; Julien, D.A.; Jelinski, D.C.; Larose, S.L.; Rennert-May, E.; Conly, J.M.; Dingle, T.C.; Chen, J.Z.; Tyrrell, G.J.; Ronksley, P.E.; et al. Antimicrobial resistance (AMR) in COVID-19 patients: A systematic review and meta-analysis (November 2019-June 2021). Antimicrob. Resist. Infect. Control 2022, 11, 45. [Google Scholar] [CrossRef]
- Chih-Cheng, L.; Shey-Ying, C.; Wen-Chien, K.; Po-Ren, H. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agent 2021, 57, 106324. [Google Scholar] [CrossRef]
- Mahadi, A.R. Post COVID Antimicrobial Resistance Threat in Lower- and Middle-Income Countries: Bangladesh. Front. Public Health 2021, 9, 770593. [Google Scholar] [CrossRef]
- Hoffman, S.J.; Outterson, K. What will it take to address the global threat of antibiotic resistance? J. Law Med. Ethics 2015, 43, 363–368. [Google Scholar] [CrossRef]
- Wilson, L.A.; Rogers, S.; Katwyk, V.; Fafard, P.; Viens, A.M.; Hoffman, S.J. Lessons learned from COVID-19 for the post-antibiotic future. Glob. Health 2021, 16, 94. [Google Scholar] [CrossRef]
- Segala, F.V.; Bavaro, D.F.; Di Gennaro, F.; Salvati, F.; Marotta, C.; Saracino, A.; Murri, R.; Fantoni, M. Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review. Viruses 2021, 13, 2110. [Google Scholar] [CrossRef] [PubMed]
- Junot, H.; Meloni, C.; Bleibtreu, A.; Robert, A. Impact of the COVID-19 pandemic on hospital antibiotic consumption, a single-center study of a metropolitan ESR. Méd. Mal. Infect. 2020, 50, S94. [Google Scholar] [CrossRef]
- Katsoulis, M.; Gomes, M.; Lai, A.G.; Henry, A.; Denaxas, S.; Lagiou, P.; Nafilyan, V.; Humberstone, B.; Banerjee, A.; Hemingway, H.; et al. Estimating the Effect of Reduced Attendance at Emergency Departments for Suspected Cardiac Conditions on Cardiac Mortality During the COVID-19 Pandemic. Circ. Cardiovasc. Qual. Outcomes 2021, 14, e007085. [Google Scholar] [CrossRef] [PubMed]
- Fyntanidou, B.; Stavrou, G.; Apostolopoulou, A.; Gkarmiri, S.; Kotzampassi, K. Emergencies in the COVID-19 Era: Less Attendances, More Admissions. Cureus 2022, 14, e25971. [Google Scholar] [CrossRef] [PubMed]
- Reschen, M.E.; Bowen, J.; Novak, A.; Giles, M.; Sings, S.; Lasserson, D.; O’Callaghan, C.A. Impact of the COVID-19 pandemic on emergency department attendances and acute medical admissions. BMC Emerg. Med. 2021, 21, 143. [Google Scholar] [CrossRef]
- Mączyńska, B.; Frej-Mądrzak, M.; Sarowska, J.; Woronowicz, K.; Choroszy-Król, I.; Jama-Kmiecik, A. Evolution of Antibiotic Resistance in Escherichia coli and Klebsiella pneumoniae Clinical Isolates in a Multi-Profile Hospital over 5 Years (2017–2021). J. Clin. Med. 2023, 12, 2414. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic prescribing in patients with COVID-19: Rapid review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef]
- Gesu, G.P.; Marchetti, F. Increasing Resistance According to Patient’s Age and Sex in Escherichia coli Isolated from Urine in Italy. J. Chemother. 2007, 19, 1169–1205. [Google Scholar] [CrossRef]
- Djuikoue, C.I.; Djoulako, P.D.D.; Wouambo, R.K.; Tomi, C.N.; Kiyang, C.P.; Tchitchoua, M.C.; Nyatchoutou, V.M.; Messeu, B.K.; Tagne, H.K.; Nana, C.D.S.; et al. Phenotypic Characterization of Carbapenemase-Producing Enterobacteriaceae Strains in a Referral Teaching Hospital in Yaoundé, Cameroon. Open J. Med. Microbiol. 2023, 13, 52–67. [Google Scholar] [CrossRef]
- Djuikoue, C.I.; Djouela Djoulako, P.D.; Wouambo, R.K.; Lacmago, S.T.; Dayomo, A.; Kamga, H.G.; Thumamo Pokam, B.D.; Apalata, T. Prevalence of Escherichia coli Producing Extended Spectrum Beta-Lactamase (ESBL) Driven Septicaemia in Children Aged 0–2 Years in Two Districts Hospitals in Yaounde, Cameroon. Bacteria 2022, 1, 294–301. [Google Scholar] [CrossRef]
- Golkar, Z.; Bagazra, O.; Pace, D.G. Bacteriophage therapy: A potential solution for the antibiotic resistance crisis. J. Infect. Dev. Ctries 2014, 8, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Gould, I.M.; Bal, A.M. New antibiotic agents in the pipeline and how they can overcome microbial resistance. Virulence 2013, 4, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Wright, G.D. Something new: Revisiting natural products in antibiotic drug discovery. Can. J. Microbiol. 2014, 60, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Chattopadhyay, M.K.; Grossart, H.P. The multifaceted roles of antibiotics and antibiotic resistance in nature. Front. Microbiol. 2013, 4, 447. [Google Scholar] [CrossRef] [PubMed]
- WHO. Tackling Antimicrobial Resistance (AMR) Together; Working Paper 5.0: Enhancing the Focus on Gender and Equity; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/336977/WHO-WSI-AMR-2018.3-eng.pdf (accessed on 25 April 2023).
- Bertakis, K.D. The influence of gender on the doctor–patient interaction. Patient Educ. Couns. 2009, 76, 356–360. [Google Scholar] [CrossRef]
- Eggermont, D.; Smit, M.A.M.; Kwestroo, G.A.; Verheij, R.A.; Hek, K.; Kunst, A.E. The influence of gender concordance between general practitioner and patient on antibiotic prescribing for sore throat symptoms: A retrospective study. BMC Fam. Pract. 2018, 19, 175. [Google Scholar] [CrossRef]
- Schröder, W.; Sommer, H.; Gladstone, B.P.; Foschi, F.; Hellman, J.; Evengard, B.; Tacconelli, E. Gender differences in antibiotic prescribing in the community: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2016, 71, 1800–1806. [Google Scholar] [CrossRef]
- Fang, R.; Sun, Y.; Xiao, L.; Chenhao, Z. Drug Resistance Mechanism of Enterobacteriaceae with Decreased Antibiotic Sensitivity. Appl. Bionics Biomech. 2022, 2022, 8285437. [Google Scholar] [CrossRef]
- Storey, P.; Dollin, M.; Rayess, N.; Pitcher, J.; Reddy, S.; Vander, J.; Hsu, J.; Garg, S. Post-Injection Endophthalmitis Study Team. The effect of prophylactic topical antibiotics on bacterial resistance patterns in endophthalmitis following intravitreal injection. Graefes. Arch. Clin. Exp. Ophthalmol. 2016, 254, 235–242. [Google Scholar] [CrossRef]
- Lin, S.; Koh, J.J.; Aung, T.T.; Lim, F.; Li, J.; Zou, H.; Wang, L.; Lakshminarayanan, R.; Verma, C.; Wang, Y.; et al. Symmetrically Substituted Xanthone Amphiphiles Combat Gram-Positive Bacterial Resistance with Enhanced Membrane Selectivity. J. Med. Chem. 2017, 60, 1362–1378. [Google Scholar] [CrossRef]
- Farfour, E.; Lecuru, M.; Dortet, L.; Guen, M.L.; Cerf, C.; Karnycheff, F.; Lesprit, P. Carbapenemase-producing Enterobacterales outbreak: Another dark side of COVID-19. Am. J. Infect. Control 2020, 48, 1533–1536. [Google Scholar] [CrossRef] [PubMed]
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial stewardship program, COVID-19, and infection control: Spread of carbapenem-resistant Klebsiella pneumoniae colonization in ICU COVID-19 patients. What did not work? J. Clin. Med. 2020, 9, E2744. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, J.; Yang, Y.; Cai, P.; Cao, J.; Cai, X.; Zhang, Y. Etiology and antimicrobial resistance of secondary bacterial infections in patients hospitalized with COVID-19 in Wuhan, China: A retrospective analysis. Antimicrob. Resist. Infect. Control 2020, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; Ej Golzari, S. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect. Dis. 2020, 20, 646. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and fungal coinfection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459. [Google Scholar] [CrossRef]
- Comité de L’antibiogramme de la Société Française de Microbiologie. Recommandations 2022 V.1.0. Available online: https://www.sfm-microbiologie.org/wp-content/uploads/2022/05/CASFM2022_V1.0.pdf (accessed on 25 April 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | |||
|---|---|---|---|---|
| Pre-COVID19 (2019) n = 160 | Sex | Male | 93 | 38.4 |
| Female | 67 | 36.4 | ||
| Age | (0–25) | 30 | 18.7 | |
| (25–50) | 85 | 53.1 | ||
| >50 | 45 | 28.1 | ||
| During COVID-19 (2020) n = 120 | Sex | Male | 69 | 28.5 |
| Female | 51 | 27.7 | ||
| Age | (0–25) | 31 | 25.8 | |
| (25–50) | 52 | 43.3 | ||
| >50 | 37 | 30.8 | ||
| During COVID-19 (2021) n = 146 | Sex | Male | 80 | 33 |
| Female | 66 | 35.9 | ||
| Age | (0–25) | 37 | 25.3 | |
| (25–50) | 72 | 49.3 | ||
| >50 | 37 | 25.3 |
| Bacterial Resistance Rate | |||||
|---|---|---|---|---|---|
| Year | Yes n (%) | No n (%) | χ2 | p-Value | |
| Pre-COVID-19 | 2019 | 94 (58.7) | 66 (41.2) | Ref | Ref |
| During COVID-19 | 2020 | 84 (70) | 36 (30) | 3.75 | 0.05 |
| 2021 | 86 (58.9) | 60 (41.1) | 0.001 | 0.97 | |
| Bacterial Resistance Rate | |||||
|---|---|---|---|---|---|
| Yes n (%) | No n (%) | χ2 | p-Value | ||
| Pre-COVID19 (2019) (n = 160) | Male | 56 (60.2) | 37 (39.8) | Ref | Ref |
| Female | 38 (56.7) | 29 (43.3) | 0.2 | 0.66 | |
| During COVID-19(2020) n = 120 | Male | 46 (66.7) | 23 (33.3) | Ref | Ref |
| Female | 38 (74.5) | 13 (25.5) | 0.86 | 0.35 | |
| During COVID-19(2021) n = 146 | Male | 34 (42.5) | 46 (57.5) | Ref | Ref |
| Female | 52 (78.9) | 14 (21.2) | 19.67 | 0.0000 | |
| Bacterial Resistance Rate | |||||
|---|---|---|---|---|---|
| Yes n (%) | No n (%) | χ2 | p-Value | ||
| Pre-COVID-19 (2019) n = 160 | (0–25) | 22 (73.3) | 8 (26.7) | Ref | Ref |
| (25–50) | 44 (51.8) | 41 (48.2) | 4.21 | 0.04 | |
| >50 | 28 (62.2) | 17 (37.8) | 1 | 0.3 | |
| During COVID-19 (2020) n = 120 | (0–25) | 19 (61.3) | 12 (38.7) | Ref | Ref |
| (25–50) | 38 (73) | 14 (27) | 1.25 | 0.26 | |
| >50 | 27 (73) | 10 (27) | 1.05 | 0.30 | |
| During COVID-19 (2021) n = 146 | (0–25) | 18 (48.6) | 19 (51.4) | Ref | Ref |
| (25–50) | 45 (62.5) | 27 (37.5) | 1.92 | 0.16 | |
| >50 | 23 (62.4) | 14 (38) | 1.34 | 0.24 | |
| Bacterial Strains | Overall Resistance | Cefixime Resistance | Azythromycin Resistance | Arythromycin Resistance | R | p-Value |
|---|---|---|---|---|---|---|
| 2019 | ||||||
| Enterobacteriaceae | 48 (60.00%) | 34 (70.83%) | - | - | 0.5 | 0.0001 |
| Staphylococcus | 42 (56.75%) | - | 7 (16.66%) | - | 0 | 0.77 |
| Staphylococcus | 42 (56.75%) | - | - | 11 (26.19%) | 0.4 | 0.0001 |
| Streptococcus | 3 (60.00%) | - | 2 (66.66%) | - | 0.2 | 0.04 |
| Streptococcus | 3 (60.00%) | - | - | 1 (33.33%) | 0.2 | 0.01 |
| Neisseria méningitidis | 1 (100%) | - | - | 1 (100%) | 0.1 | 0.12 |
| 2020 | ||||||
| Enterobacteriaceae | 60 (86.95%) | 23 (38.33%) | - | - | 0.7 | 0.0001 |
| Staphylococcus | 22 (45.83%) | - | 3 (13.63%) | - | −0.2 | 0.85 |
| Staphylococcus | 22 (45.83%) | - | - | 5 (22.72%) | 0.8 | 0.0001 |
| Streptococcus | 2 (60.00%) | - | 1 (50.00%) | - | 0.2 | 0.13 |
| Streptococcus | 2 (60.00%) | - | - | 1 (50.00%) | 0.1 | 0.58 |
| 2021 | ||||||
| Enterobacteriaceae | 61 (64.21%) | 31 (50.81%) | - | - | 0.5 | 0.0001 |
| Staphylococcus | 23 (48.93%) | - | - | 12 (52.17%) | 0.7 | 0.0001 |
| Streptococcus | 2 (50.00%) | - | 1 (50.00%) | - | 0.2 | 0.16 |
| Streptococcus | 2 (50.00%) | - | - | 1 (50.00%) | 0.4 | 0.0005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djuikoue, C.I.; Yamdeu Djonkouh, W.; Epie Bekolo, C.; Kamga Wouambo, R.; Carrel Founou, R.; Djouela Djoulako, P.D.; Tonfak Temgoua, G.; Pokam, B.D.T.; Antoine-Moussiaux, N.; Apalata, T.R. Prevalence and Antibiotic Resistance Pattern of Streptococcus, Staphylococcus, Neisseria meningitidis and Enterobacteriaceae in Two Reference Hospitals of Yaoundé: An Overview before and during COVID-19 Pandemic Era. Antibiotics 2023, 12, 929. https://doi.org/10.3390/antibiotics12050929
Djuikoue CI, Yamdeu Djonkouh W, Epie Bekolo C, Kamga Wouambo R, Carrel Founou R, Djouela Djoulako PD, Tonfak Temgoua G, Pokam BDT, Antoine-Moussiaux N, Apalata TR. Prevalence and Antibiotic Resistance Pattern of Streptococcus, Staphylococcus, Neisseria meningitidis and Enterobacteriaceae in Two Reference Hospitals of Yaoundé: An Overview before and during COVID-19 Pandemic Era. Antibiotics. 2023; 12(5):929. https://doi.org/10.3390/antibiotics12050929
Chicago/Turabian StyleDjuikoue, Cecile Ingrid, Willy Yamdeu Djonkouh, Cavin Epie Bekolo, Rodrigue Kamga Wouambo, Raspail Carrel Founou, Paule Dana Djouela Djoulako, Gilder Tonfak Temgoua, Benjamin D. Thumamo Pokam, Nicolas Antoine-Moussiaux, and Teke R. Apalata. 2023. "Prevalence and Antibiotic Resistance Pattern of Streptococcus, Staphylococcus, Neisseria meningitidis and Enterobacteriaceae in Two Reference Hospitals of Yaoundé: An Overview before and during COVID-19 Pandemic Era" Antibiotics 12, no. 5: 929. https://doi.org/10.3390/antibiotics12050929
APA StyleDjuikoue, C. I., Yamdeu Djonkouh, W., Epie Bekolo, C., Kamga Wouambo, R., Carrel Founou, R., Djouela Djoulako, P. D., Tonfak Temgoua, G., Pokam, B. D. T., Antoine-Moussiaux, N., & Apalata, T. R. (2023). Prevalence and Antibiotic Resistance Pattern of Streptococcus, Staphylococcus, Neisseria meningitidis and Enterobacteriaceae in Two Reference Hospitals of Yaoundé: An Overview before and during COVID-19 Pandemic Era. Antibiotics, 12(5), 929. https://doi.org/10.3390/antibiotics12050929