


Antibiotic Use in Pregnancy: A Global Survey on Antibiotic Prescription Practices in Antenatal Care
 , and
, and 
Abstract
:1. Introduction
2. Results
2.1. Respondents’ Characteristics
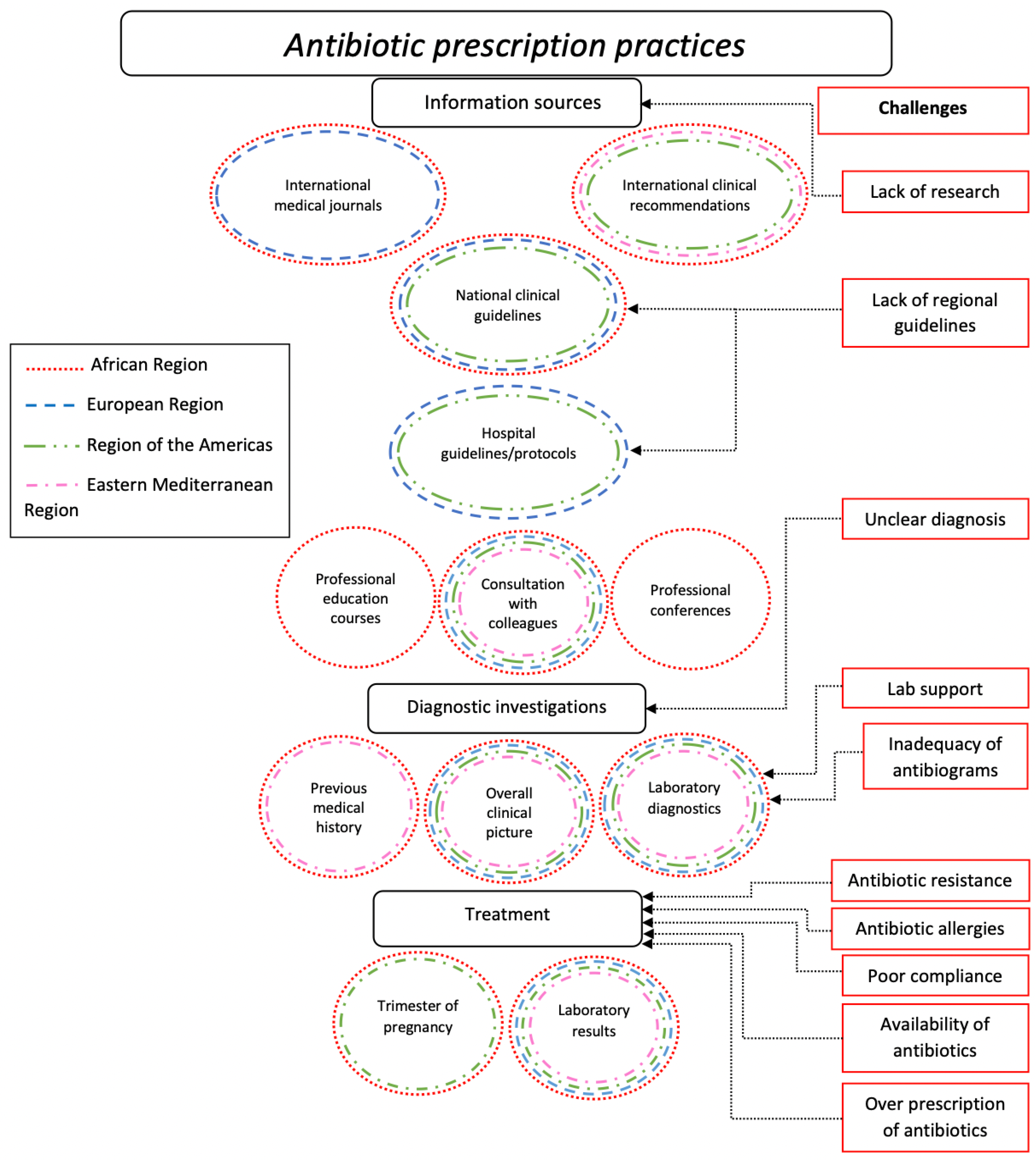
2.2. Practices of Antibiotic Prescription
2.2.1. Diagnostics
2.2.2. Treatment
2.2.3. Indicators Considered when Prescribing Antibiotics
2.2.4. Consultations
2.2.5. Reasons for Switching between Hospital and National Guidelines
“Particularly with preventive antibiotics, there is sometimes discussion in guidelines. For example, in case of preterm ruptured membranes. Previously, the advice was to treat, then not for a while, and now there is a review in which the option is considered again. This is based on the same trials. So, it is not always clear what the best policy is.”(The Netherlands; translated from Dutch.)
“Working in rural areas within LMICs (low and middle-income countries) often requires prescriptions based on available medications amongst other considerations.”(Nigeria.)
2.3. Challenges of Diagnostics/Antibiotic Treatment
“Antibiograms often investigate antibiotics that cannot be prescribed during pregnancy”(Italy; translated from Italian.)
“- Not unequivocal best policy—There is a lack of studies on proper dosing for pregnant women and on the extent of transmission to the child. During delivery, leucocytes and CRP are routinely elevated, which makes differentiation between infection and inflammation due to delivery not always possible.”(The Netherlands; translated from Dutch)
“When I have a report of a urine or vaginal culture that gives me sensitivity to antibiotics not recommended for the corresponding trimester of pregnancy.”(Dominican Republic; translated from Spanish.)
“There are multi-resistant germs that make it necessary to treat with antibiotics that are not ideal in pregnancy.”(Uruguay; translated from Spanish.)
2.4. Sources of Information
2.5. Recommendations
“Taking into account antibiotic resistance. Taking into account the unavailability in Italy of amoxicillin for prevention of Streptococcus agalactia infection in labor.”(Italy; translated from Italian.)
“Publish updated national/regional pocket guidelines based on local epidemiology. Establish a national registry on (severe) pregnancy infections treated in inpatient settings.”(Italy; translated from Italian.)
“Hospital develop antibiograms for mothers and should be adhered to. Culture and sensitivity testing should be fully utilized by the clinicians.”(Uganda.)
3. Discussion
4. Materials and Methods
4.1. Online Survey
4.2. Study Population
4.3. Data Analysis
4.4. Ethical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Survey
Appendix B. Informed Consent/Information Form
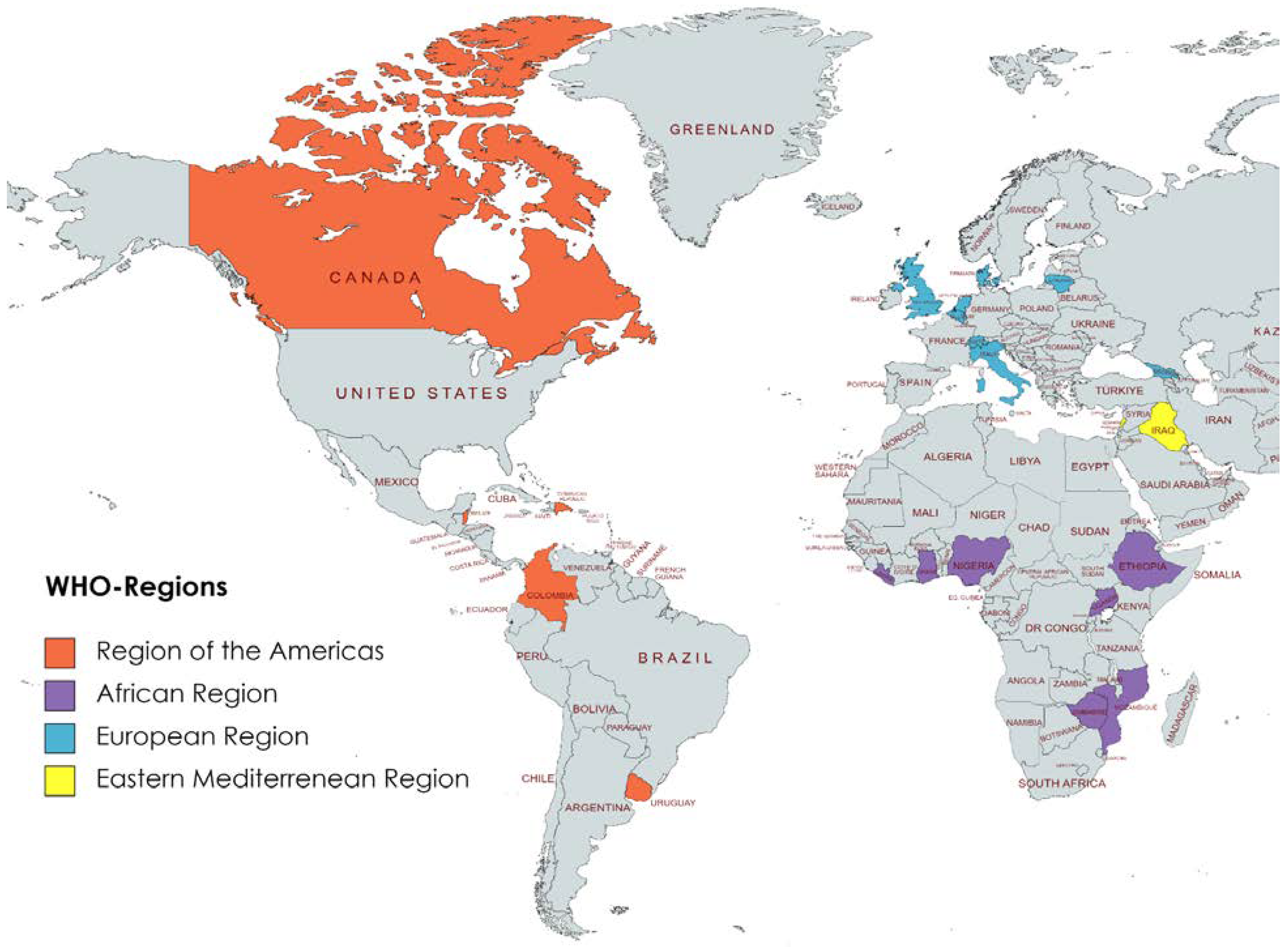
Appendix C. Geographical Distribution of Survey Responses

References
- Broe, A.; Pottegård, A.; Lamont, R.F.; Jørgensen, J.S.; Damkier, P. Increasing Use antibiotics in pregnancy during the period 2000-2010: Prevalence, timing, category, and demographics. Bjog 2014, 121, 988–996. [Google Scholar] [CrossRef] [PubMed]
- Kuperman, A.A.; Koren, O. Antibiotic use during pregnancy: How bad is it? BMC Med. 2016, 14, 91. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.A.; Tran, E.L.; Parker, C.M.; Kim, H.-J.; Yee, E.L.; Smith, P.W.; Russell, Z.; A Nelson, C.; Broussard, C.S.; Yu, Y.C.; et al. Safety of antimicrobials during pregnancy: A systematic review of antimicrobials considered for treatment and postexposure prophylaxis of plague. Clin. Infect. Dis. 2020, 70 (Suppl. S1), S37–S50. [Google Scholar] [CrossRef] [PubMed]
- Furfaro, L.L.; Chang, B.J.; Payne, M.S. Applications for bacteriophage therapy during pregnancy and the perinatal period. Front. Microbiol. 2018, 8, 2660. [Google Scholar] [CrossRef] [PubMed]
- Cantarutti, A.; Rea, F.; Franchi, M.; Beccalli, B.; Locatelli, A.; Corrao, G. Use of antibiotic treatment in pregnancy and the risk of several neonatal outcomes: A population-based study. Int. J. Environ. Res. Public. Health 2021, 18, 12621. [Google Scholar] [CrossRef]
- Harbison, A.F.; Polly, D.M.; Musselman, M.E. Antiinfective therapy for pregnant or lactating patients in the emergency department. Am. J. Health-Syst. Pharm. 2015, 72, 189–197. [Google Scholar] [CrossRef]
- Lamont, H.F.; Blogg, H.J.; Lamont, R.F. Safety of antimicrobial treatment during pregnancy: A current review of resistance, immunomodulation and teratogenicity. Expert. Opin. Drug. Saf. 2014, 13, 1569–1581. [Google Scholar] [CrossRef]
- Lee, A.C.; Mullany, L.C.; Koffi, A.K.; Rafiqullah, I.; Khanam, R.; Folger, L.V.; Rahman, M.; Mitra, D.K.; Labrique, A.; Christian, P. Urinary tract infections in pregnancy in a rural population of Bangladesh: Population-based prevalence, risk factors, etiology, and antibiotic resistance. BMC Pregnancy Childbirth 2019, 20, 1. [Google Scholar] [CrossRef]
- Heikkilä, A.M. Antibiotics in pregnanc—A prospective cohort study on the policy of antibiotic prescription. Ann. Med. 1993, 25, 467–471. [Google Scholar] [CrossRef]
- WHO. Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA; Executive Summary; World Bank Group and the United Nations Population Division: Geneva, Switzerland, 2019. [Google Scholar]
- Say, L.; Chou, D.; Getmmill, A.; Tunçalp, Ö.; Moller, A.-B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef]
- Vidal, A.C.; Murphy, S.K.; Murtha, A.P.; Schildkraut, J.M.; Soubry, A.; Huang, Z.; Neelon, S.E.B.; Fuemmeler, B.; Iversen, E.; Wang, F.; et al. Associations between antibiotic exposure during pregnancy, birth weight and aberrant methylation at imprinted genes among offspring. Int. J. Obes. 2013, 37, 907–913. [Google Scholar] [CrossRef]
- Holderness, M.; Straughan, J.L. South African Medicines Formulary; Medical Association of South Africa, Publications Division: Pretoria, South Africa, 1991. [Google Scholar]
- Amann, U.; Egen-Lappe, V.; Strunz-Lehner, C.; Hasford, J. Antibiotics in pregnancy: Analysis of potential risks and determinants in a large German statutory sickness fund population. Pharmacoepidemiol. Drug. Saf. 2006, 15, 327–337. [Google Scholar] [CrossRef]
- Ledger, W.J.; Blaser, M.J. Are we using too many antibiotics during pregnancy? Bjog 2013, 120, 1450–1452. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilizand, R.; Shah, P.S.; Seshia, M.; Yee, W.; Yoon, E.W.; Dow, K. Antibiotic exposure and development of necrotizing enterocolitis in very preterm neonates. Paediatr. Child. Health 2018, 23, e56–e61. [Google Scholar] [CrossRef] [PubMed]
- Bookstaver, P.B.; Bland, C.M.; Griffin, B.; Stover, K.R.; Eiland, L.S.; McLaughlin, M. A Review of Antibiotic Use in Pregnancy. Pharmacotherapy 2015, 35, 1052–1062. [Google Scholar] [CrossRef]
- Crider, K.S.; Cleves, M.A.; Reefhuis, J.; Berry, R.J.; Hobbs, C.A.; Hu, D.J. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch. Pediatr. Adolesc. Med. 2009, 163, 978–985. [Google Scholar] [CrossRef]
- Ayad, M.; Costantine, M.M. Epidemiology of medications use in pregnancy. Semin. Perinatol. 2015, 39, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Sheffield, J.S.; Sietgel, D.; Mirochnick, M.; Heine, R.P.; Nguyen, C.; Bergman, K.L.; Savic, R.M.; Long, J.; Dooley, K.E.; Nesin, M. Designing drug trials: Considerations for pregnant women. Clin. Infect. Dis. 2014, 59 (Suppl. S7), S437–S444. [Google Scholar] [CrossRef] [PubMed]
- Schuts, E.C.; Hulscher, M.E.J.L.; Mouton, J.W.; Verduin, C.M.; Stuart, J.W.T.C.; Overdiek, H.W.P.M.; van der Linden, P.D.; Natsch, S.; Hertogh, C.M.P.M.; Wolfs, T.F.W.; et al. Current evidence on hospital antimicrobial stewardship objectives: A systematic review and meta-analysis. Lancet Infect. Dis 2016, 16, 847–856. [Google Scholar] [CrossRef]
- Hermanides, H.S.; Hulscher, M.E.; Schouten, J.A.; Prins, J.M.; Geerlings, S.E. Development of quality indicators for the antibiotic treatment of complicated urinary tract infections: A first step to measure and improve care. Clin. Infect. Dis. 2008, 46, 703–711. [Google Scholar] [CrossRef]
- Mensah, K.B.; Opoku-Agyeman, K.; Ansah, C. Antibiotic use during pregnancy: A retrospective study of prescription patterns and birth outcomes at an antenatal clinic in rural Ghana. J. Pharm. Policy Pract. 2017, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Health Global. Essential diagnostics: Mind the gap. Lancet Glob. Health 2021, 9, e1474. [Google Scholar] [CrossRef] [PubMed]
- Fleming, K.A.; Horton, S.; Wilson, M.L.; Atun, R.; DeStigter, K.; Flanigan, J.; Sayed, S.; Adam, P.; Aguilar, B.; Andronikou, S.; et al. The Lancet Commission on diagnostics: Transforming access to diagnostics. Lancet 2021, 398, 1997–2050. [Google Scholar] [CrossRef] [PubMed]
- Menéndez, C.; Quintó, L.; Castillo, P.; Fernandes, F.; Carrilho, C.; Ismail, M.R.; Lorenzoni, C.; Hurtado, J.C.; Rakislova, N.; Munguambe, K.; et al. Quality of care and maternal mortality in a tertiary-level hospital in Mozambique: A retrospective study of clinicopathological discrepancies. Lancet Global Health 2020, 8, e965–e972. [Google Scholar] [CrossRef] [PubMed]
- Habak, P.J.; Griggs, R.P., Jr. Urinary Tract. Infection In Pregnancy, StatPearls ed.; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537047/ (accessed on 13 February 2023).
- Kollef, M.H. Broad-Spectrum Antimicrobials and the Treatment of Serious Bacterial Infections: Getting It Right Up Front. Clin. Infect. Dis. 2008, 47 (Suppl. S1), S3–S13. [Google Scholar] [CrossRef]
- Dashe, J.S.; Gilstrap, L.C. Antibiotic Use in Pregnancy. Obstet. Gynecol. Clin. North. Am. 1997, 24, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, M.; Khan, F.; Shukla, I.; Malik, A.; Shaheen. Rising prevalence of antimicrobial resistance in urinary tract infections during pregnancy: Necessity for exploring newer treatment options. J. Lab. Physicians 2011, 3, 98–103. [Google Scholar] [CrossRef]
- Lo, W.Y.; Friedman, J.M. Teratogenicity of recently introduced medications in human pregnancy. Obstet. Gynecol. 2002, 100, 465–473. [Google Scholar] [CrossRef]
- Dathe, K.; Schaefer, C. The Use of Medication in Pregnancy. Dtsch. Arztebl. Int. 2019, 116, 783–790. [Google Scholar] [CrossRef]
- Lynch, M.M.; Squiers, L.B.; Kosa, K.M.; Dolina, S.; Read, J.G.; Broussard, C.S.; Frey, M.T.; Polen, K.N.; Lind, J.N.; Gilboa, S.M.; et al. Making Decisions About Medication Use During Pregnancy: Implications for Communication Strategies. Matern. Child. Health J. 2018, 22, 92–100. [Google Scholar] [CrossRef]
- Craig, J.; Hiban, K.; Frost, I.; Kapoor, G.; Alimi, Y.; Varma, J.K. Comparison of national antimicrobial treatment guidelines, African Union. Bull. World Health Organ. 2022, 100, 50–59. [Google Scholar] [CrossRef]
- Saleh, N.; Awada, S.; Awwad, R.; Jibai, S.; Arfoul, C.; Zaiter, L.; Dib, W.; Salameh, P. Evaluation of antibiotic prescription in the Lebanese community: A pilot study. Infect. Ecol. Epidemiol. 2015, 5, 27094. [Google Scholar] [CrossRef]
- Warremana, E.; Lambregtsa, M.; Wouters, R.; Visser, L.; Staats, H.; van Dijk, E.; de Boer, M. Determinants of in-hospital antibiotic prescription behaviour: A systematic review and formation of a comprehensive framework. Clin. Microbiol. Infect. 2019, 25, 538–545. [Google Scholar] [CrossRef]
- Seyed-Nezhad, M.; Ahmadi, B.; Akbari-Sari, A. Factors affecting the successful implementation of the referral system: A scoping review. J. Fam. Med. Prim. Care 2021, 10, 4364–4375. (In English) [Google Scholar] [CrossRef]
- Van den Broek d’Obrenan, J.; Verheij, T.J.M.; Numans, M.E.; van der Velden, A.W. Antibiotic use in Dutch primary care: Relation between diagnosis, consultation and treatment. J. Antimicrob. Chemother. 2014, 69, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, M.; Haverkate, M.; Achterberg, P.; Timen, A. The public uptake of information about antibiotic resistance in the Netherlands. Public. Underst. Sci. 2019, 28, 486–503. [Google Scholar] [CrossRef] [PubMed]
- Federal Action Plan On Antimicrobial Resistance And Use In Canada. 2015. Available online: https://www.canada.ca/en/health-canada/services/publications/drugs-health-products/federal-action-plan-antimicrobial-resistance-canada.html (accessed on 21 February 2023).
- Chandler, C.I.R. Current accounts of antimicrobial resistance: Stabilisation, individualisation and antibiotics as infrastructure. Palgrave Commun. 2019, 5, 53. [Google Scholar] [CrossRef] [PubMed]
- Willis, L.D.; Chandler, C. Quick fix for care, productivity, hygiene and inequality: Reframing the entrenched problem of antibiotic overuse. BMJ Glob. Health 2019, 4, e001590. [Google Scholar] [CrossRef]
- Ajibola, O.; Omisakin, O.A.; Eze, A.A.; Omoleke, S.A. Self-Medication with Antibiotics, Attitude and Knowledge of Antibiotic Resistance among Community Residents and Undergraduate Students in Northwest Nigeria. Diseases 2018, 6, 32. Available online: https://www.mdpi.com/2079-9721/6/2/32 (accessed on 21 February 2023). [CrossRef] [PubMed]
- Obakiro, S.B.; Napyo, A.; Wilberforce, M.J.; Adongo, P.; Kiyimba, K.; Anthierens, S.; Kostyanev, T.; Waako, P.; Van Royen, P. Are antibiotic prescription practices in Eastern Uganda concordant with the national standard treatment guidelines? A cross-sectional retrospective study. J. Glob. Antimicrob. Resist. 2022, 29, 513–519. [Google Scholar] [CrossRef]
- Barchitta, M.; Sabbatucci, M.; Furiozzi, F.; Iannazzo, S.; Maugeri, A.; Maraglino, F.; Prato, R.; Agodi, A.; Pantosti, A. Knowledge, attitudes and behaviors on antibiotic use and resistance among healthcare workers in Italy, 2019: Investigation by a clustering method. Antimicrob. Resist. Infect. Control. 2021, 10, 134. [Google Scholar] [CrossRef] [PubMed]
- Menichetti, F.; Falcone, M.; Lopalco, P.; Tascini, C.; Pan, A.; Busani, L.; Viaggi, B.; Rossolini, G.M.; Arena, F.; Novelli, A.; et al. The GISA call to action for the appropriate use of antimicrobials and the control of antimicrobial resistance in Italy. Int. J. Antimicrob. Agents 2018, 52, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, K.; Hopkins, S.; Llewelyn, M.; Walker, A.; McNulty, C.; Robotham, J. Duration of antibiotic treatment for common infections in English primary care: Cross sectional analysis and comparison with guidelines. BMJ 2019, 364, 1440. [Google Scholar] [CrossRef] [PubMed]
- Graham, W.J.; Morrison, E.; Dancer, S.; Afsana, K.; Aulakh, A.; Campbell, O.M.R.; Cross, S.; Ellis, R.; Enkubahiri, S.; Fekad, B.; et al. What are the threats from antimicrobial resistance for maternity units in low- and middle- income countries? Glob. Health Action. 2016, 9, 33381. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | Total (N = 137), n (%) |
|---|---|
| Gender | |
| Male | 44 (32.1) |
| Female | 93 (67.9) |
| Non-binary | 0 (0) |
| Prefer not to say | 0 (0) |
| Age | |
| 20–29 | 12 (8.8) |
| 30–39 | 39 (28.5) |
| 40–49 | 22 (16.1) |
| 50+ | 60 (43.8) |
| Other | 4 (2.9) |
| Profession | |
| Gynecologist/obstetrician | 116 (84.7) |
| General practitioner | 5 (3.6) |
| Midwife | 2 (1.5) |
| Nurse | 1 (0.7) |
| Other | 13 (9.5) |
| Country of practice (WHO region) | |
| Region of the Americas | 16 (11.7) |
| European Region | 101 (73.8) |
| African Region | 8 (5.8) |
| Eastern Mediterranean Region | 12 (8.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gamberini, C.; Donders, S.; Al-Nasiry, S.; Kamenshchikova, A.; Ambrosino, E. Antibiotic Use in Pregnancy: A Global Survey on Antibiotic Prescription Practices in Antenatal Care. Antibiotics 2023, 12, 831. https://doi.org/10.3390/antibiotics12050831
Gamberini C, Donders S, Al-Nasiry S, Kamenshchikova A, Ambrosino E. Antibiotic Use in Pregnancy: A Global Survey on Antibiotic Prescription Practices in Antenatal Care. Antibiotics. 2023; 12(5):831. https://doi.org/10.3390/antibiotics12050831
Chicago/Turabian StyleGamberini, Carlotta, Sabine Donders, Salwan Al-Nasiry, Alena Kamenshchikova, and Elena Ambrosino. 2023. "Antibiotic Use in Pregnancy: A Global Survey on Antibiotic Prescription Practices in Antenatal Care" Antibiotics 12, no. 5: 831. https://doi.org/10.3390/antibiotics12050831
APA StyleGamberini, C., Donders, S., Al-Nasiry, S., Kamenshchikova, A., & Ambrosino, E. (2023). Antibiotic Use in Pregnancy: A Global Survey on Antibiotic Prescription Practices in Antenatal Care. Antibiotics, 12(5), 831. https://doi.org/10.3390/antibiotics12050831