1. Introduction
Antimicrobial resistance (AMR) is a major public health concern that affects individuals of all ages [
1]. AMR is associated with high rates of mortality and increased medical costs, especially in low- and middle-income countries, due to the high burden of infectious diseases [
2]. Pediatric patients are particularly vulnerable to antibiotic-resistant infections, as children are often exposed to antibiotics and have immature immune systems. Furthermore, bacteriemia is a leading cause of mortality among pediatric patients, and its treatment is threatened by the alarming increase in the prevalence of AMR [
3]. Therefore, it is crucial to understand the prevalence and patterns of antibiotic resistance in pediatric hospital settings.
Global antibiotic consumption experienced a 65% increase worldwide between 2000 and 2015, showing an inverse correlation with the decline in deaths caused by infectious diseases. However, the extensive use of antibiotics has led to the emergence of antibiotic-resistant bacterial strains, complicating infection management and limiting the effectiveness of available antibiotics. Researchers predict millions of deaths due to bacterial AMR, highlighting the urgent need for action. To address this issue, implementing AMR surveillance systems is crucial to collect antimicrobial resistance data. This data can be used to develop empirical therapy and establish local and national antibiotic treatment guidelines. The World Health Organization (WHO) has introduced the ‘One Health’ concept, emphasizing the surveillance of AMR in humans, animals, and the environment through collaborative efforts between various research teams from different sectors [
4].
The overuse and misuse of antibiotics, along with breaches in Infection Prevention and Control (IPC) and lack of policies and education, have led to the emergence of bacteria resistant to many commonly used antibiotics. AMR has several primary mechanisms, including the formation of biofilms, reduction of antibiotic permeability, and the use of active efflux pumps [
5]. Additionally, novel AMR mechanisms are emerging despite efforts to control them. Multidrug-resistant pathogens (MDR) are of particular concern since they can cause infections that are challenging or impossible to treat with conventional antibiotic regimens. This, in turn, results in longer hospital stays, increased healthcare expenses, and higher mortality rates [
6]. Some of the most frequent MDR bacteria includes extended-spectrum beta-lactamase producers (ESBL)
Escherichia coli and
Klebsiella pneumonie, carbapenem-resistant
Pseudomonas aeruginosa (CRPA), carbapenem-resistant
Acinetobacter baumanii (CRAB), carbapenem-resistant
Enterobacteriaceae (CRE), methicillin-resistant
Staphylococcus aureus (MRSA), vancomycin-resistant
Staphylococcus aureus (VRSA) and vancomycin-resistant
enterococci (VRE) [
7].
There are various international surveillance networks, such as GLASS (Global Antimicrobial Resistance and Use Surveillance System), EARS-Net (European Antimicrobial Resistance Surveillance Network), CARSS (China Antimicrobial Resistance Surveillance System), and CHINET (China Antimicrobial Surveillance Network) [
8,
9]. However, these networks primarily focus on monitoring AMR in adults rather than addressing the issue in children. Furthermore, the prevalence distributions and AMR patterns of bacteria isolated from children differ significantly from those found in adults, as children cannot be considered mere “miniature adults” in the context of AMR [
10,
11]. Taking
Streptococcus pneumoniae as an example, the rate of
S. pneumoniae carriage is considerably higher in children (53%) compared to adults (4%), and the serotype distribution and antibiotic resistance patterns of
S. pneumoniae also exhibit notable variations between the two age groups. For this reason, in 2015, China implemented the Infectious Diseases Surveillance of Pediatrics, including 11 tertiary care hospitals, but more international homogenous programs are needed [
6].
The endorsed global action plan on AMR by the World Health Organization emphasizes the significance of promoting awareness of AMR through continuous monitoring and research initiatives across various regions worldwide. Monitoring AMR is crucial and offers several benefits, such as providing insights into bacterial resistance rates, facilitating the selection of suitable antibiotics, thereby reducing AMR rates, reducing hospitalization and treatment expenses, and lowering mortality rates [
12,
13,
14].
In the present study, we aim to increase awareness of AMR among children by providing a description of the epidemiology and AMR rates of the main isolated bacterial pathogens in hospitalized patients between January 2022 and December 2022 at the tertiary center Marie Curie Emergency Children’s Hospital, Bucharest, Romania. The Marie Curie Emergency Children’s Hospital is a tertiary emergency hospital with 473 beds, catering to children from all over the country. The hospital houses several departments, including pediatrics, nephrology, cardiology, pediatric surgery and orthopedics, otolaryngology, cardiovascular surgery, neurosurgery, intensive care unit, and neonatal intensive care unit.
3. Discussion
The incidence of multidrug-resistant organisms is on the rise, causing substantial morbidity and mortality among patients. Infections caused by MDR bacteria pose greater treatment challenges, leading to more severe and protracted illnesses, which in turn result in longer hospital stays. These infections have been shown to increase hospitalization times by up to 20% and to be associated with poorer outcomes, including a mortality rate that may be as high as 40% in cases of hospital-acquired MDR infections [
15].
Given the rapidly evolving context, failure to take urgent action may lead us into a post-antibiotic era where common infections become fatal once again. This is particularly valid for children who are more susceptible to common infections.
Our study aimed to examine the distribution of the main pathogens and the prevalence of AMR at Marie Curie Emergency Children’s Hospital during the last year. Due to the potential serious infections occurring in hospitalized patients caused by antibiotic-resistant GN and GP bacteria, physicians are concerned with identifying the presence and spread of these agents [
16,
17]. Choosing and prescribing effective antibiotics for the treatment of pediatric infections presents a significant challenge. This is further complicated by the fact that certain categories of antibiotic regimens cannot be used in neonates and children and that the patterns of AMR may vary across different regions [
18]. Therefore, knowing the AMR distribution could help healthcare providers to prescribe the most effective drugs [
19]. Additionally, the absence of adequate surveillance for AMR could lead to the inappropriate use of antibacterial agents by healthcare providers and patients, leading to significant healthcare issues, particularly in developing countries such as Romania [
20].
In our study, from 1445 isolated microorganisms, the majority were GN (64.49%), and 34.8% were GP. These results are similar to the China Antimicrobial Surveillance Network (CHINET) [
8]. Among Gram-negative bacteria,
Escherichia coli was the most frequently isolated, and among Gram-positive,
Staphylococcus aureus was the most frequently isolated. The most frequent ten isolated bacterial species in our study are mentioned in
Table 1. Except for
Escherichia coli, which was at the top of the list, the distribution was largely different in the international reports of CHINET and China Antimicrobial Resistance Surveillance System (CARSS) in 2016 [
8,
21]. The reported top ten bacterial pathogens in children by the Infectious Disease Surveillance of Pediatrics (ISPED) were
Escherichia coli,
Streptococcus pneumoniae,
Staphylococcus aureus,
Haemophillus influenzae,
Klebsiella pneumoniae,
Moraxella catarrhalis,
Streptococcus pyogenes,
Staphylococcus epidermidis,
Pseudomonas aeruginosa, and
Acinetobacter baumannii [
6].
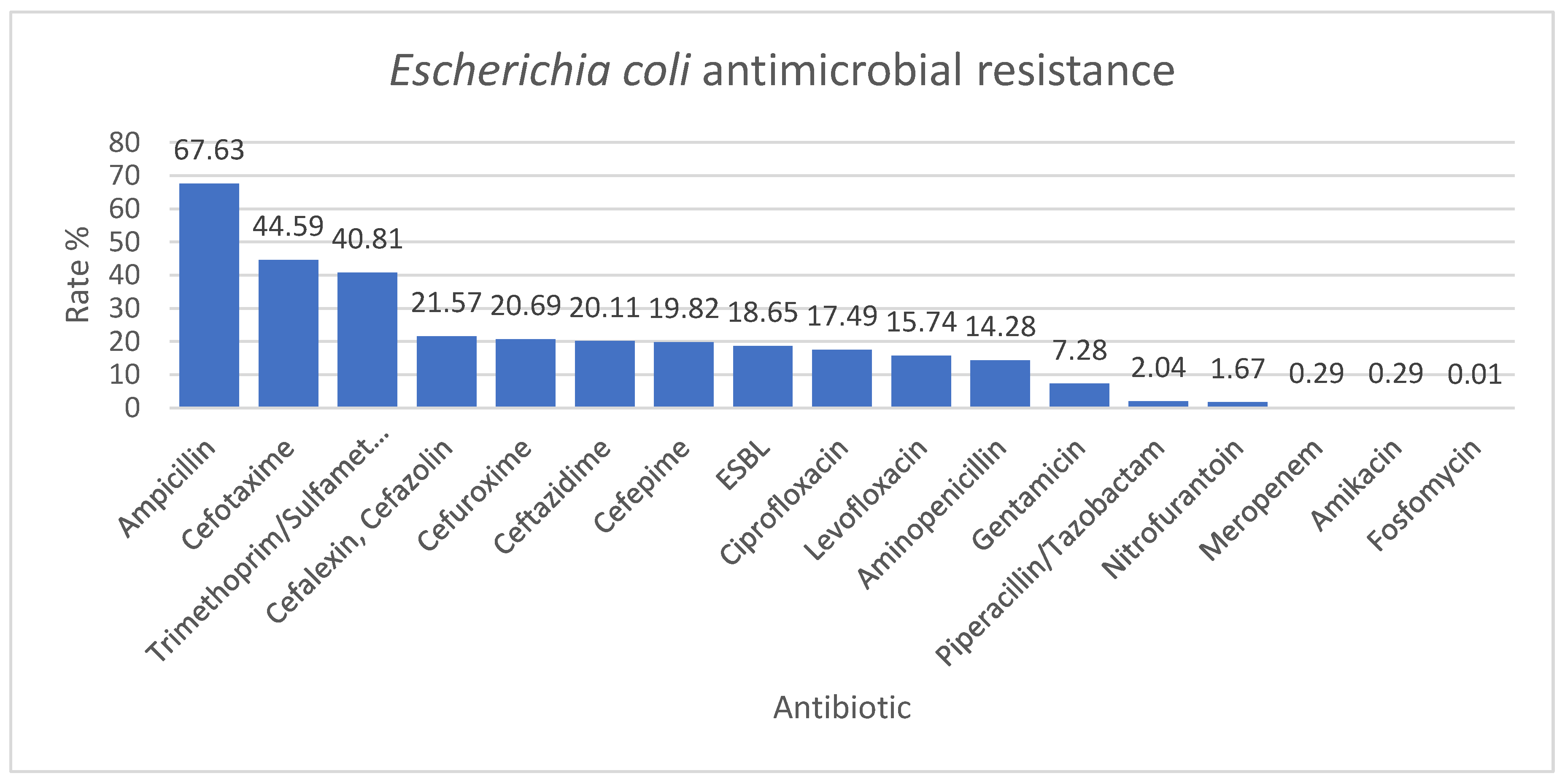
Escherichia coli had the lowest resistance rates to amikacin, meropenem, and fosfomycin (0.29%, 0.29%, and 0.01%); the values were comparable with the results of a three-year study conducted in Bologna, Italy. In this study,
Escherichia coli resistance rate to amikacin and fosfomycin was 0.6%. They also obtained a high resistance rate to amoxicillin-clavulanate and cotrimoxazole, comparable to our results. On the other hand, in this Italian study, the resistance rate to cefotaxime was 5.8%, much lower than in our study (44.59%) [
22]. The ESBL-producing
Escherichia coli resistance rate was 18.65% in our study. This is almost similar to a John Hopkins study where the ESBL-producing
Escherichia coli resistance rate was 13.2% [
23]. The risk factors associated with high ESBL levels were long hospital stays, previous use of antibiotics, and previous Intensive Care Unit (ICU) admission [
24,
25,
26]. In our hospital, many patients with serious diseases require a wide spectrum of antimicrobial regimens and ICU passages, which could explain the higher rate of ESBL. In the John Hopkins study, the ESBL were sensitive to amikacin and carbapenems (ertapenem, meropenem), which could indicate the use of these antibiotics in patients at risk until the result of the culture is obtained [
23].
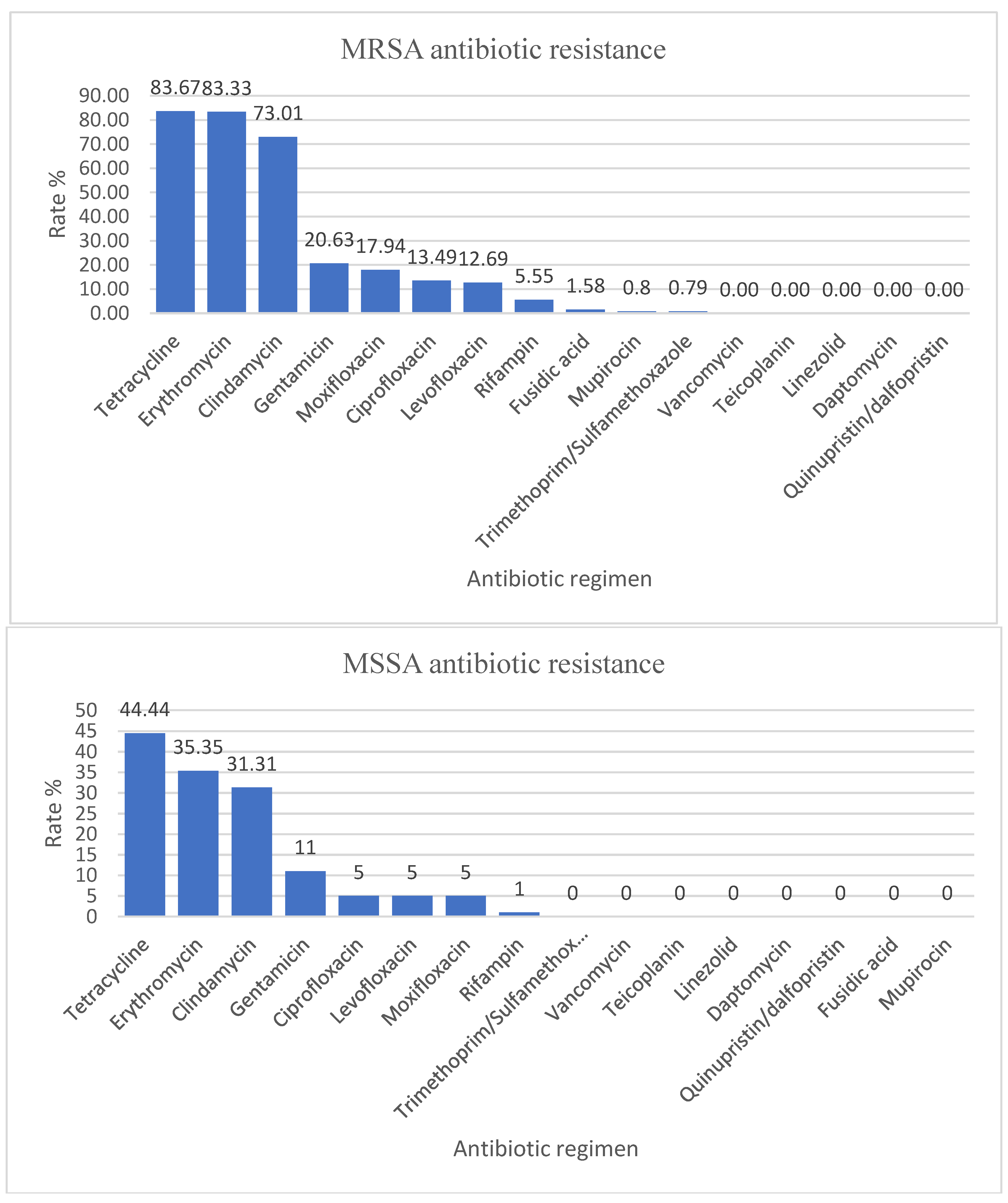
Staphylococcus aureus strains were divided into MSSA, which represented 100/226 (44.25%), and MRSA, which represented 126/226 (55.75%). The data in our analysis are consistent with those reported by our country to the European Antibiotic Resistance Surveillance Network (EARS-Net), which shows an increased rate of MRSA isolated from invasive infections and places Romania in the undesirable leading position in this regard (47.3% of all
Staphylococcus aureus strains reported in 2020, which is 2.84 times higher than the estimated weighted average for participating countries). In 2021, it decreased to 41%, a decrease without statistical significance [
27,
28]. The rate of MRSA antibiotic resistance in our hospital is higher than the rate reported in the literature. In a study conducted by La Vecchia et al. in Milan during 2017–2021, the rate of MSSA antibiotic resistance was 70%, and the rate of MRSA antibiotic resistance was only 30% [
29]. Additionally, in a study from Utah, USA, by Crandall et al., the AMR for MSSA was 79%, and for MRSA, only 21% [
30]. MRSA strains typically affect people who are vulnerable due to factors such as recent hospitalization or use of healthcare services, living in long-term care facilities, undergoing hemodialysis, or having percutaneous medical devices and catheters [
31,
32]. In our hospital, there are many hospitalized patients having these risks, but further studies are needed to be done to investigate the high prevalence of MRSA strains. According to several studies, linezolid and vancomycin were effective against
Staphylococcus aureus strains, so no AMR for vancomycin-resistant
Staphylococcus aureus (VRSA) strains was declared [
19,
29,
33].
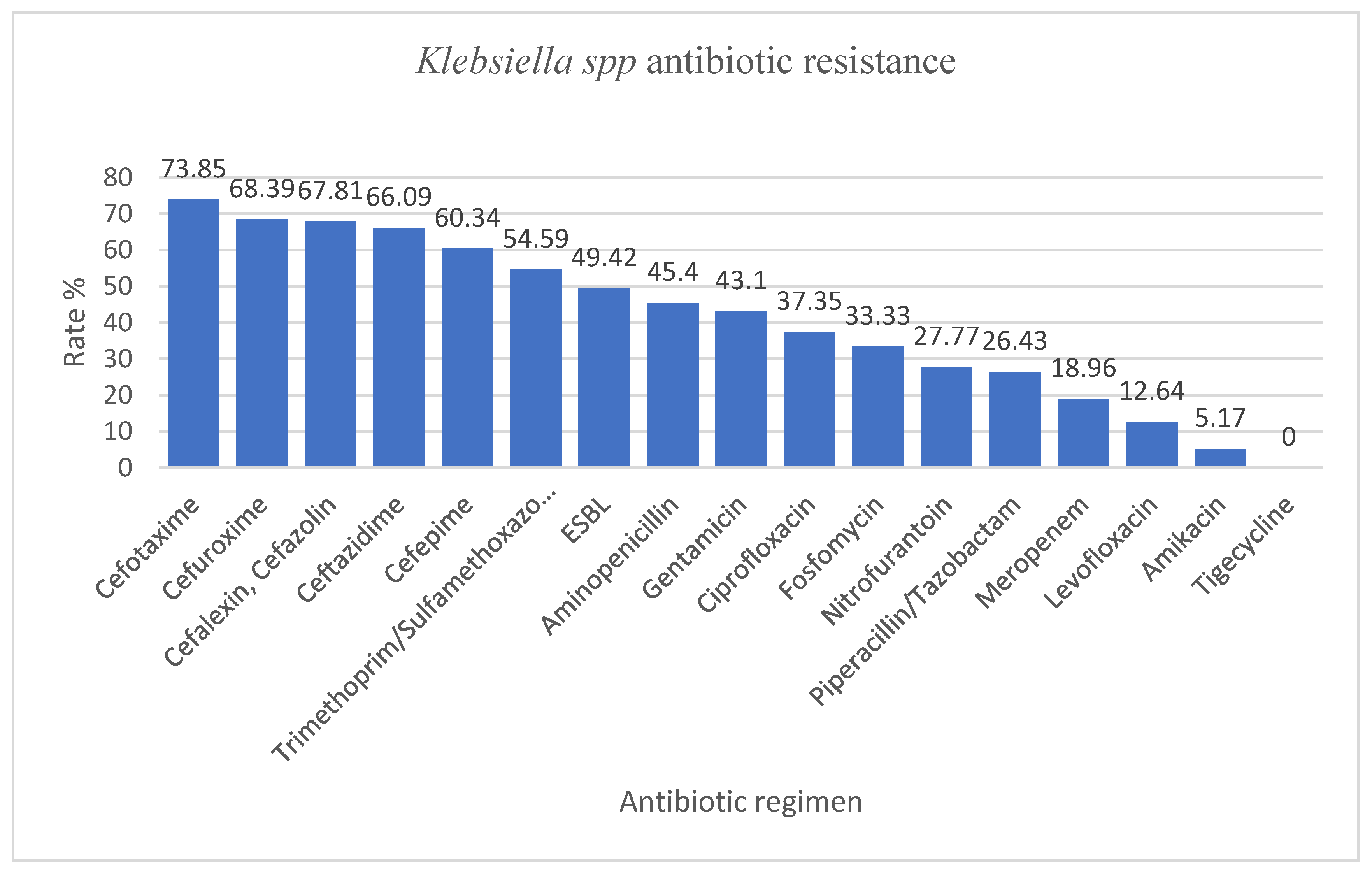
Klebsiella spp. isolated in our hospital presented with an increased AMR of more than 50% resistance rate to cefotaxime, cefuroxime, cefalexin, cefazolin, ceftazidime, cefepime, trimethoprim/sulfamethoxazole, values much higher than the ones reported by Ballén et al. where the highest resistance rate was to ciprofloxacin (41%). The resistance rates to third-generation cephalosporins were similar to those reported by our country to EARS-Net (around 70% in our study vs. 70.8%), as well as the resistance to aminoglycosides (43.1% in our study vs. 51.6%). However, unlike the data from EARS-Net, we found lower resistance rates to meropenem (18.69% in our study vs. 54.5%) and fluoroquinolones (more than two times less in our study, probably due to the fact that this class of antibiotics is less used in children) [
27]. In that study by Ballén et al., 40.16% of the strains were considered MDR, and 1.57% were considered XDR. The rate of MDR and XDR in our study were 43.67% and 19.54%, respectively [
34]. The AMR for ESBL-producing
Klebsiella spp. was 49.42%. In our study, the highest susceptibility was for amikacin and tigecycline.
Klebsiella spp. are identified as members of a group that includes six highly virulent and antibiotic-resistant bacterial pathogens:
Enterococcus faecium,
Staphylococcus aureus,
Klebsiella pneumoniae,
Acinetobacter baumannii,
Pseudomonas aeruginosa, and
Enterobacter spp. (ESKAPE group). This group is known for its characteristic ability to resist or avoid the action of antimicrobial agents [
35]. In addition, the World Health Organization has designated
Klebsiella pneumoniae as a high-priority species and advocates for the development of new antibiotics due to the growing global issue of antimicrobial resistance [
36].
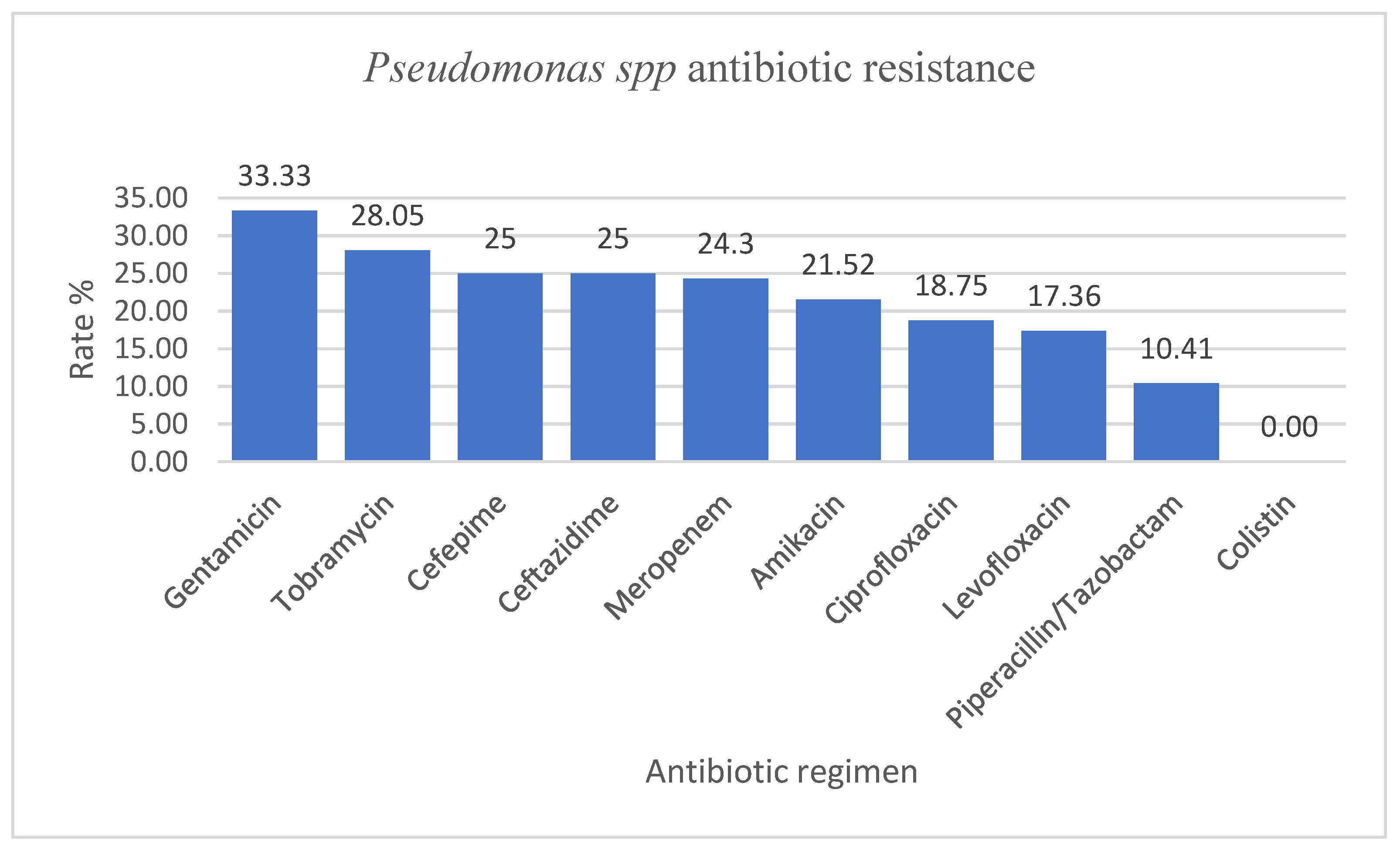
Pseudomonas spp. had resistance rate values to ceftazidime, meropenem, amikacin, ciprofloxacin, and piperacillin/tazobactam ranging from 10 to 35%, while the Infectious Disease Surveillance of Pediatrics (ISPED) program reported values of 2.3–10.1% [
6]. However, compared to the data reported to EARS-Net by our country, in our study, we identified lower rates of resistance to piperacillin-tazobactam (10.41% vs. 47.2%), ceftazidime (25% vs. 46%), meropenem (24.3% vs. 45.9%), ciprofloxacin/levofloxacin (18.75% and 17.36% vs. 45.7%), and gentamycin (33.33% vs. 41.7%) [
27].
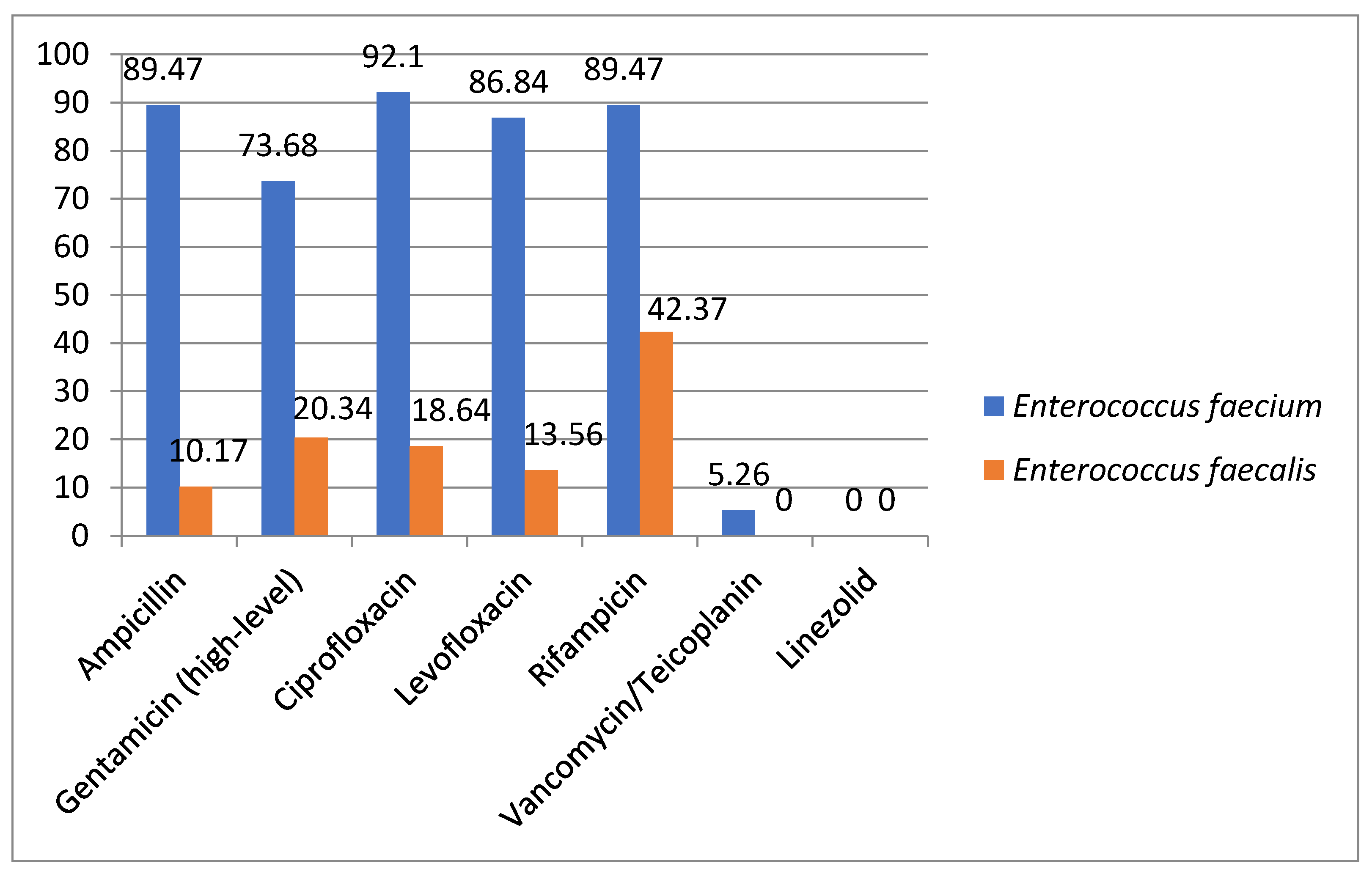
Enterococcus spp. had the highest antimicrobial resistance rates, as expected, among
Enterococcus faecium strains compared to
Enterococcus faecalis. Similar levels of resistance were seen in the results reported by ISPED [
6]. We also found two isolates of
Enterococcus facecium resistant to vancomycin and teicoplanin. This resistance profile is of concern for our country, as between 2012 and 2020, glycopeptide resistance increased significantly, from 2.9% to 41.7%; the level of resistance is now the fourth highest among EU/EEA countries [
28].
Overall, our results reveal a higher antimicrobial resistance to the main pathogens when compared to the literature findings [
37]. However, we need to mention that our hospital is classified as a tertiary care center, providing advanced and specialized medical care to patients from all over the country who suffer from complex medical conditions or illnesses. With a broad range of medical specialties, including surgical, medical, and intensive care, our center offers specialized services and complex procedures that are not commonly found in general hospitals or clinics. The high prevalence of intricate diseases among our patient population, necessitating prolonged hospital stays and the administration of multiple antibiotic regimens has been identified as a significant contributing factor to the rise in AMR rates. This concerning trend poses serious challenges in terms of available antibiotic treatment options, greatly limiting their effectiveness and often necessitating the use of reserve or watchlist antibiotics. Furthermore, the hospital environment provides an ideal breeding ground for the transmission and spread of antibiotic-resistant germs, leading to the emergence of difficult-to-control outbreaks of healthcare-associated infections. Last but not least, AMR has an economic impact by increasing treatment costs and prolonging hospitalization.
In June 2018, European Center for Disease Control (ECDC) evaluated the AMR levels in Romania. It was considered that our country presents with a high AMR compared to other states of Europe. There are several factors likely to contribute to this situation, such as excessive use of antibiotics in the general population, excessive use of last-line broad-spectrum antibiotics in hospitals, inadequate local AMR surveillance, which could contribute to proper use of antimicrobial agents, and scarce antimicrobial stewardship antimicrobial programs [
38]. Recently, awareness campaigns have been organized to limit the use of antibiotics and the sale of over-the-counter antimicrobial agents, but there are still many efforts to be made.
Study Limitations
This study has several limitations that need to be addressed. Firstly, the analysis period was relatively short, and it is crucial to continuously monitor and analyze the emerging trends of antibiotic resistance. This requires the implementation of effective antimicrobial stewardship programs, as the misuse and overuse of antibiotics contribute significantly to the increasing antimicrobial resistance. Additionally, this study was conducted in a single pediatric hospital in Bucharest, which may limit the generalizability of the findings. Conducting a multicenter study, including territorial hospitals, over a more extended period and including demographic data could provide more accurate data on the antimicrobial resistance issue in Romania. Furthermore, it is important to note that our study was conducted within a specific timeframe, namely during the COVID-19 pandemic. This unique and challenging period may have influenced our results in various ways. Additionally, during the study, we identified a significant problem with the outsourced microbiology laboratory in our hospital and the lack of a clinical microbiology specialist. This situation hinders good communication between physicians and the laboratory when unusual resistance profiles are observed. In such situations, we had to send samples to a national reference institute for confirmation, which is a time-consuming and costly process. The lack of effective communication may lead to the overlooking of critical situations that need to be clarified, ultimately impacting both the analysis of resistance data and the clinical management of the patient. Therefore, it is crucial to have a clinical microbiology specialist in our hospital to facilitate effective communication and proper management of patients with antimicrobial resistance issues.
4. Materials and Methods
We conducted a retrospective analysis of clinical specimens obtained from patients admitted to the Marie Curie Emergency Children’s Hospital between 1 January 2022 and 31 December 2022. The study included a total of 1445 clinical isolates, consecutive and non-duplicated, collected from hospitalized patients from various departments (ICU, NICU, cardiovascular ICU, cardiology, oncology, orthopedics, ENT, pediatrics, nephrology, hemodialysis, and neurosurgery).
The samples were collected for etiological identification in patients with suggestive symptomatology of acute infection. In our hospital exists portage identification protocols, notably in patients who will undergo surgery (orthopedics, cardiology, pediatric surgery) and in high-risk patients (ICU, NICU, oncology) for whom samples were taken.
Microbiological samples were processed in the outsourced microbiology laboratory, as the hospital did not have its own laboratory at the time of analysis. Each specimen was inoculated on a different medium according to the manufacturer and incubated at 37 °C for 24 h. The urine cultures were inoculated on CHROMagar medium, the nasal and pharyngeal samples on Columbia and Chocolat medium (Biomérieux), and stool cultures on Selenit enrichment broth (Sanimed) and Hektoen agar (Biomérieux). The other specimens (blood, cerebrospinal fluid—CSF, sputum, pus, auricular, ocular, vagina, urethral) were inoculated on several mediums, namely Columbia, Chocolat, MacConkey, and Brain heart infusion broth (
Table 10). Various kits were used for the identification of certain bacteria—Staphytect Plus (Oxoid) for coagulase-positive
Staphylococci, Streptococcal grouping kit (Oxoid) for hemolytic
Streptococci and API NH kit (Biomérieux) for the identification of
Neisseria, Haemophilus, and
Moraxella catharralis (
Table 11). Identification and antimicrobial resistance were performed by the MicroScan Automated System (Beckman Coulter). For identification and AMR testing, we used 3 types of standardized panel kits: one for Gram-negative bacteria, one panel for Gram-positive bacteria, and MICroSTREP plus 1 for streptococci. Each kit tested for certain antibiotics (
Table 12), and the results were reported depending on the specimen type. The AMR was interpreted in accordance with the Clinical and Laboratory Standards Institute (CLSI) guidelines. Extended-spectrum beta-lactamase-producing (ESBL)-producing bacteria were also identified automatically by MicroScan System.
We excluded bacterial duplicates, defined as the same germ with the same resistance profile isolated from the same patient within less than four weeks. We also excluded from the analysis antibiotics for which too few strains were tested to be relevant (below 30).
An isolated microorganism was classified as MDR if it demonstrated in vitro non-susceptibility to one or more agents within three or more antimicrobial categories. If a bacterium was resistant to at least one agent in almost all antimicrobial categories, except two or less, it was classified as extensively drug-resistant (XDR). Finally, the isolate was classified as pan-drug-resistant (PDR) if it was non-susceptible to all the listed antimicrobial agents [
34].



 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}