


Prevalence of Carbapenemases in Carbapenem-Resistant Acinetobacter baumannii Isolates from the Kingdom of Bahrain
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
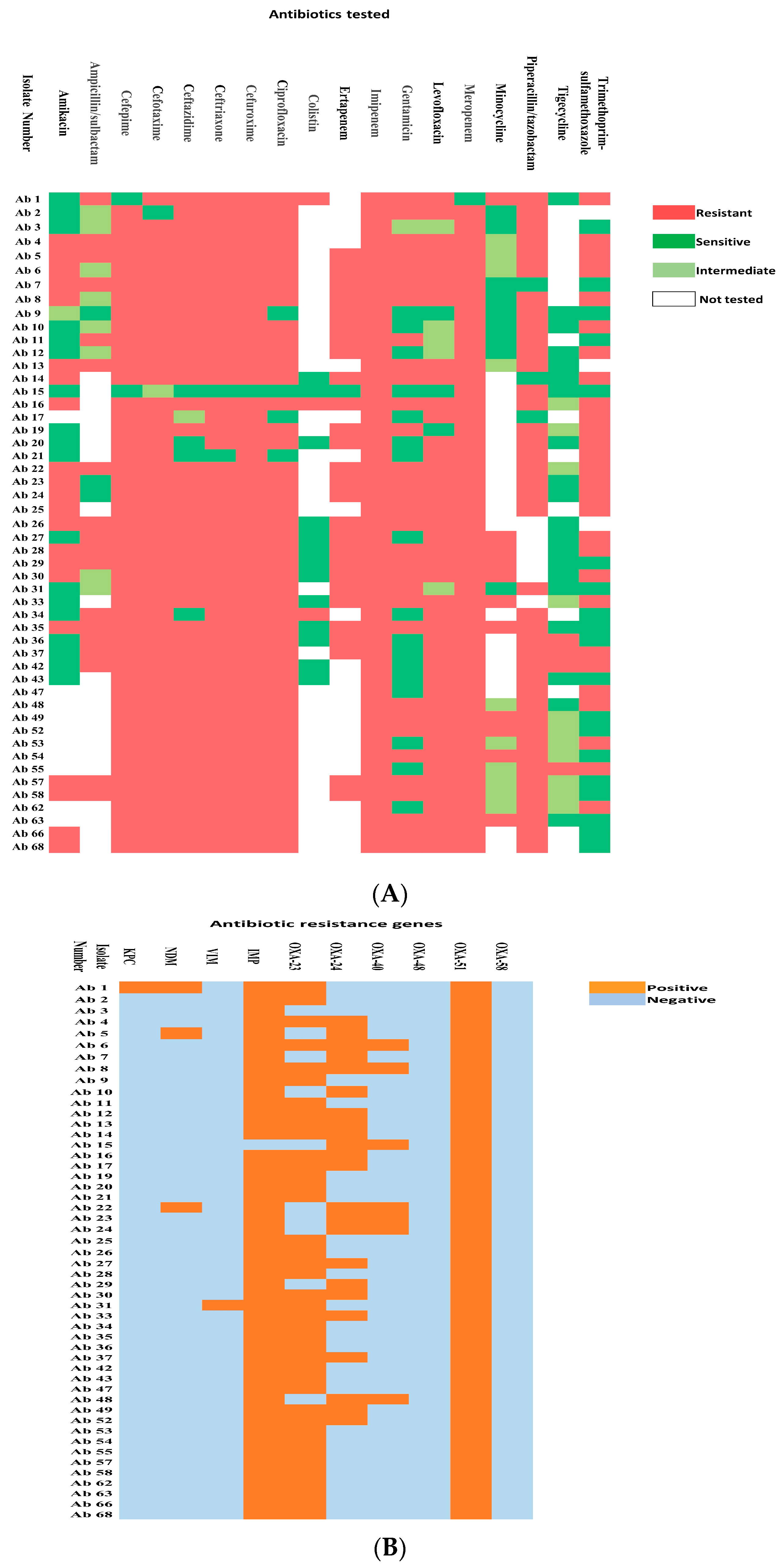
2.1. Distribution and Antibiotic Resistance Pattern of the Isolates
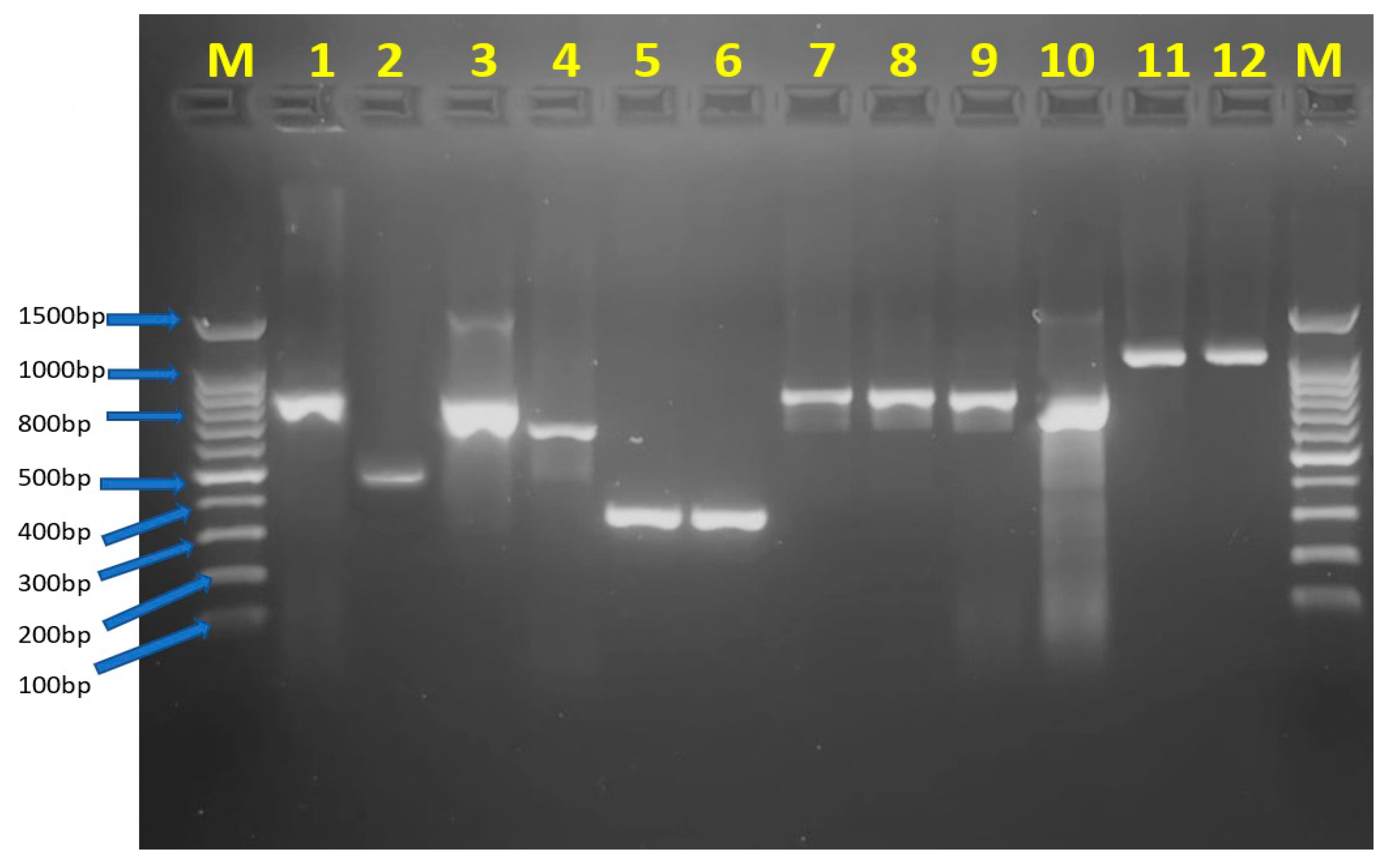
2.2. Carbapenemase-Encoding Genes’ Detection
3. Discussion
4. Materials and Methods
4.1. Bacterial Isolates and Hospital Setting
4.2. Bacterial Identification and Antibiotic Susceptibility Testing
4.3. Amplification of Carbapenemases Genes via Polymerase Chain Reaction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howard, A.; O’Donoghue, M.; Feeney, A.; Sleator, R.D. Acinetobacter baumannii: An emerging opportunistic pathogen. Virulence 2012, 3, 243–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vijayakumar, S.; Biswas, I.; Veeraraghavan, B. Accurate identification of clinically important Acinetobacter spp.: An update. Future Sci. OA 2019, 5, FSO395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Ding, F.; Luo, Y.; Fan, B.; Tao, Z.; Li, Y.; Gu, D. Distribution pattern of carbapenemases and solitary contribution to resistance in clinical strains of Acinetobacter baumannii. Ann. Palliat. Med. 2021, 10, 9184–9191. [Google Scholar] [CrossRef]
- Ejaz, H.; Ahmad, M.; Younas, S.; Junaid, K.; Abosalif, K.O.A.; Abdalla, A.E.; Alameen, A.A.M.; Elamir, M.Y.M.; Bukhari, S.N.A.; Ahmad, N.; et al. Molecular Epidemiology of Extensively-Drug Resistant Acinetobacter baumannii Sequence Type 2 Co-Harboring bla (NDM) and bla (OXA) From Clinical Origin. Infect. Drug Resist. 2021, 14, 1931–1939. [Google Scholar] [CrossRef]
- Fournier, P.E.; Richet, H. The epidemiology and control of Acinetobacter baumannii in health care facilities. Clin. Infect. Dis. 2006, 42, 692–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almasaudi, S.B. Acinetobacter spp. as nosocomial pathogens: Epidemiology and resistance features. Saudi J. Biol. Sci. 2018, 25, 586–596. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; McClean, S. Mapping Global Prevalence of Acinetobacter baumannii and Recent Vaccine Development to Tackle It. Vaccines 2021, 9, 570. [Google Scholar] [CrossRef]
- Gales, A.C.; Seifert, H.; Gur, D.; Castanheira, M.; Jones, R.N.; Sader, H.S. Antimicrobial Susceptibility of Acinetobacter calcoaceticus-Acinetobacter baumannii Complex and Stenotrophomonas maltophilia Clinical Isolates: Results From the SENTRY Antimicrobial Surveillance Program (1997-2016). Open Forum Infect. Dis. 2019, 6 (Suppl. 1), S34–S46. [Google Scholar] [CrossRef] [Green Version]
- Spellberg, B.; Rex, J.H. The value of single-pathogen antibacterial agents. Nat. Rev. Drug Discov. 2013, 12, 963. [Google Scholar] [CrossRef] [Green Version]
- Wong, D.; Nielsen, T.B.; Bonomo, R.A.; Pantapalangkoor, P.; Luna, B.; Spellberg, B. Clinical and Pathophysiological Overview of Acinetobacter Infections: A Century of Challenges. Clin. Microbiol. Rev. 2017, 30, 409–447. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Ding, Y.; Wei, Y.; Jian, C.; Liu, J.; Zeng, Z. Carbapenem-resistant Acinetobacter baumannii: A challenge in the intensive care unit. Front. Microbiol. 2022, 13. [Google Scholar] [CrossRef]
- Al-Sultan, A.A. Prevalence of High-Risk Antibiotic Resistant Acinetobacter baumannii in the Holy Cities of Makkah and Al-Madinah. Open Microbiol. J. 2021, 15, 145–151. [Google Scholar] [CrossRef]
- Al-Agamy, M.H.; Jeannot, K.; El-Mahdy, T.S.; Shibl, A.M.; Kattan, W.; Plésiat, P.; Courvalin, P. First detection of GES-5 carbapenemase-producing Acinetobacter baumannii isolate. Microb. Drug Resist. 2017, 23, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, X.; Wang, Y.; Tao, Y.; Shao, X.; Li, Y.; Li, W. Insight into carbapenem resistance and virulence of Acinetobacter baumannii from a children’s medical centre in eastern China. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 47. [Google Scholar] [CrossRef]
- Hafiz, T.A.; Alghamdi, S.S.; Mubaraki, M.A.; Alghamdi, S.S.M.; Alothaybi, A.; Aldawood, E.; Alotaibi, F. A two-year retrospective study of multidrug-resistant Acinetobacter baumannii respiratory infections in critically Ill patients: Clinical and microbiological findings. J. Infect. Public Health 2023, 16, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Al-Obeid, S.; Jabri, L.; Al-Agamy, M.; Al-Omari, A.; Shibl, A. Epidemiology of extensive drug resistant Acinetobacter baumannii (XDRAB) at Security Forces Hospital (SFH) in Kingdom of Saudi Arabia (KSA). J. Chemother. 2015, 27, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Zowawi, H.M.; Sartor, A.L.; Sidjabat, H.E.; Balkhy, H.H.; Walsh, T.R.; Al Johani, S.M.; AlJindan, R.Y.; Alfaresi, M.; Ibrahim, E.; Al-Jardani, A.; et al. Molecular epidemiology of carbapenem-resistant Acinetobacter baumannii isolates in the Gulf Cooperation Council States: Dominance of OXA-23-type producers. J. Clin. Microbiol. 2015, 53, 896–903. [Google Scholar] [CrossRef] [Green Version]
- Mugnier, P.D.; Bindayna, K.M.; Poirel, L.; Nordmann, P. Diversity of plasmid-mediated carbapenem-hydrolysing oxacillinases among carbapenem-resistant Acinetobacter baumannii isolates from Kingdom of Bahrain. J. Antimicrob. Chemother. 2009, 63, 1071–1073. [Google Scholar] [CrossRef] [Green Version]
- Azizi, O.; Shakibaie, M.R.; Modarresi, F.; Shahcheraghi, F. Molecular Detection of Class-D OXA Carbapenemase Genes in Biofilm and Non-Biofilm Forming Clinical Isolates of Acinetobacter baumannii. Jundishapur. J. Microbiol. 2015, 8, e21042. [Google Scholar] [CrossRef] [Green Version]
- Soudeiha, M.A.H.; Dahdouh, E.A.; Azar, E.; Sarkis, D.K.; Daoud, Z. In vitro Evaluation of the Colistin-Carbapenem Combination in Clinical Isolates of A. baumannii Using the Checkerboard, Etest, and Time-Kill Curve Techniques. Front. Cell. Infect. Microbiol. 2017, 7, 209. [Google Scholar] [CrossRef]
- Ibrahimagic, A.; Kamberovic, F.; Uzunovic, S.; Bedenic, B.; Idrizovic, E. Molecular characteristics and antibiotic resistance of Acinetobacter baumanniibeta-lactamase-producing isolates, a predominance of intrinsic blaOXA-51, and detection of TEM and CTX-M genes. Turk. J. Med. Sci. 2017, 47, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Amudhan, S.M.; Sekar, U.; Arunagiri, K.; Sekar, B. OXA beta-lactamase-mediated carbapenem resistance in Acinetobacter baumannii. Indian J. Med. Microbiol. 2011, 29, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Grisold, A.J.; Luxner, J.; Bedenic, B.; Diab-Elschahawi, M.; Berktold, M.; Wechsler-Fordos, A.; Zarfel, G.E. Diversity of Oxacillinases and Sequence Types in Carbapenem-Resistant Acinetobacter baumannii from Austria. Int. J. Environ. Res. Public Health 2021, 18, 2171. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.H.; Leu, Y.S.; Wang, N.Y.; Liu, C.P.; Yan, T.R. Prevalence of different carbapenemase genes among carbapenem-resistant Acinetobacter baumannii blood isolates in Taiwan. Antimicrob. Resist. Infect. Control 2018, 7, 123. [Google Scholar] [CrossRef] [Green Version]
- Lowings, M.; Ehlers, M.M.; Dreyer, A.W.; Kock, M.M. High prevalence of oxacillinases in clinical multidrug-resistant Acinetobacter baumannii isolates from the Tshwane region, South Africa—An update. BMC Infect. Dis. 2015, 15, 521. [Google Scholar] [CrossRef] [Green Version]
- Al-Agamy, M.H.; Khalaf, N.G.; Tawfick, M.M.; Shibl, A.M.; El Kholy, A. Molecular characterization of carbapenem-insensitive Acinetobacter baumannii in Egypt. Int. J. Infect. Dis. 2014, 22, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Xiao, S.Z.; Chu, H.Q.; Han, L.Z.; Zhang, Z.M.; Li, B.; Zhao, L.; Xu, L. Resistant mechanisms and molecular epidemiology of imipenem-resistant Acinetobacter baumannii. Mol. Med. Rep. 2016, 14, 2483–2488. [Google Scholar] [CrossRef] [Green Version]
- Cody, W.L.; Wilson, J.W.; Hendrixson, D.R.; McIver, K.S.; Hagman, K.E.; Ott, C.M.; Nickerson, C.A.; Schurr, M.J. Skim milk enhances the preservation of thawed -80 degrees C bacterial stocks. J. Microbiol. Methods 2008, 75, 135–138. [Google Scholar] [CrossRef] [Green Version]
- Shahid, M.; Sobia, F.; Singh, A.; Khan, H.M. Concurrent occurrence of blaampC families and blaCTX-M genogroups and association with mobile genetic elements ISEcp1, IS26, ISCR1, and sul1-type class 1 integrons in Escherichia coli and Klebsiella pneumoniae isolates originating from India. J. Clin. Microbiol. 2012, 50, 1779–1782. [Google Scholar] [CrossRef] [Green Version]
- Charfi-Kessis, K.; Mansour, W.; Ben Haj Khalifa, A.; Mastouri, M.; Nordmann, P.; Aouni, M.; Poirel, L. Multidrug-resistant Acinetobacter baumannii strains carrying the bla(OxA-23) and the bla(GES-11) genes in a neonatology center in Tunisia. Microb. Pathog. 2014, 74, 20–24. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Antibiotics | Total No. of Isolates Tested | Resistant Isolates (%) | Intermediate Isolates (%) |
|---|---|---|---|
| Amikacin | 40 | 21 (52.5%) | 1 (2.5%) |
| Ampicillin/sulbactam | 33 | 22 (66.6%) | 8 (24.2%) |
| Cefepime | 50 | 48 (96%) | |
| Cefotaxin | 50 | 48 (96%) | 1 (2%) |
| Ceftazidime | 50 | 45 (90%) | 1 (2%) |
| Ceftriaxone | 50 | 48 (96%) | |
| Cefuroxime | 50 | 49 (98%) | |
| Ciprofloxacin | 50 | 46 (92%) | |
| Colistin | 18 | 5 (27.7%) | |
| Ertapenem | 28 | 27 (96.4%) | |
| Imipenem | 50 | 50 (100%) | |
| Gentamicin | 50 | 32 (64%) | 1 (2%) |
| Levofloxacin | 48 | 42 (87.5%) | 3 (6.25%) |
| Meropenem | 50 | 49 (98%) | |
| Minocycline | 30 | 11 (36.6%) | 10 (33.3%) |
| Piperacillin/tazobactam | 44 | 43 (97.7%) | |
| Tigecycline | 35 | 3 (5.5%) | 12 (34.2%) |
| Trimetoprim-sulfamethoxazole | 47 | 28 (59.5%) |
| Combination of Carbapenem-Resistance Genes | Number of Isolates (n = 50) |
|---|---|
| blaOXA-51, blaOXA-23, blaOXA-24, blaOXA-40, blaIMP | 2 |
| blaOXA-51, blaOXA-23, blaOXA-24, blaIMP | 12 |
| blaOXA-51, blaOXA-23, blaIMP | 22 |
| blaOXA-51, blaOXA-23, blaOXA-40, blaIMP | 3 |
| blaOXA-51, blaOXA-23, | 2 |
| blaOXA-51, blaOXA-24, blaIMP | 3 |
| blaOXA-51, blaOXA-23, blaIMP, blaVIM | 1 |
| blaOXA-51, blaOXA-23, blaOXA-24, blaKPC, blaIMP, blaNDM | 1 |
| blaOXA-51, blaOXA-24, blaOXA-40, blaIMP, blaNDM | 1 |
| blaOXA-51, blaOXA-24, blaIMP, blaNDM | 1 |
| blaOXA-51, blaOXA-24, blaOXA-40 | 1 |
| blaOXA-51, blaIMP | 1 |
| Genes Targeted | Primer Sequence (5′→3′) | Amplicon Size (bp) | Reference |
|---|---|---|---|
| KPC | F-ATGTCACTGTATCGCCGTCT R-TTACTGCCCGTTGACGCCCA | 881 | [20] |
| VIM | F-ATTCCGGTCGG(A=G) GAGGTCCG R-TGTGCTKGAGCAAKTCYAGACCG | 601 | [20] |
| NDM | F-GGCCGTATGAGTGATTGC R-GAAGCTGAGCACCGCATTAG | 825 | [20] |
| IMP | F-CGGCC(G=T) CAGGAG(A=C) G(G-T) CTTT R-AACCAGTTTTGC(C=T) TTAC(C=T) AT | 484 | [20] |
| OXA-23 | F-ATGAATAAATATTTTACTTG RTTAAATAATATTCAGCTGTT | 821 | [20] |
| OXA-24 | F-ATACTTCCTATATTCAGCAT R-GATTCCAAGATTTCTAGCG | 809 | [20] |
| OXA-40 | F-GTACTAATCAAAGTTGTGAA R-TTCCCCTAACATGAATTTGT | 1024 | [30] |
| OXA-48 | F-GCTTGATCGCCCTCGATT R-GATTTGCTCCGTGGCCGAAA | 281 | [20] |
| OXA-51 | F-TAATGCTTTGATCGGCCTTG R-TGGATTGCACTTCATCTTGG | 353 | [20] |
| OXA-58 | F-ATGAAATTATTAAAAATATTGAGT R-ATAAATAATGAAAAACACCCAA | 840 | [20] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Rashed, N.; Bindayna, K.M.; Shahid, M.; Saeed, N.K.; Darwish, A.; Joji, R.M.; Al-Mahmeed, A. Prevalence of Carbapenemases in Carbapenem-Resistant Acinetobacter baumannii Isolates from the Kingdom of Bahrain. Antibiotics 2023, 12, 1198. https://doi.org/10.3390/antibiotics12071198
Al-Rashed N, Bindayna KM, Shahid M, Saeed NK, Darwish A, Joji RM, Al-Mahmeed A. Prevalence of Carbapenemases in Carbapenem-Resistant Acinetobacter baumannii Isolates from the Kingdom of Bahrain. Antibiotics. 2023; 12(7):1198. https://doi.org/10.3390/antibiotics12071198
Chicago/Turabian StyleAl-Rashed, Nouf, Khalid M. Bindayna, Mohammad Shahid, Nermin Kamal Saeed, Abdullah Darwish, Ronni Mol Joji, and Ali Al-Mahmeed. 2023. "Prevalence of Carbapenemases in Carbapenem-Resistant Acinetobacter baumannii Isolates from the Kingdom of Bahrain" Antibiotics 12, no. 7: 1198. https://doi.org/10.3390/antibiotics12071198
APA StyleAl-Rashed, N., Bindayna, K. M., Shahid, M., Saeed, N. K., Darwish, A., Joji, R. M., & Al-Mahmeed, A. (2023). Prevalence of Carbapenemases in Carbapenem-Resistant Acinetobacter baumannii Isolates from the Kingdom of Bahrain. Antibiotics, 12(7), 1198. https://doi.org/10.3390/antibiotics12071198