
Neonatal Bloodstream Infection with Ceftazidime-Avibactam-Resistant blaKPC-2-Producing Klebsiella pneumoniae Carrying blaVEB-25

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
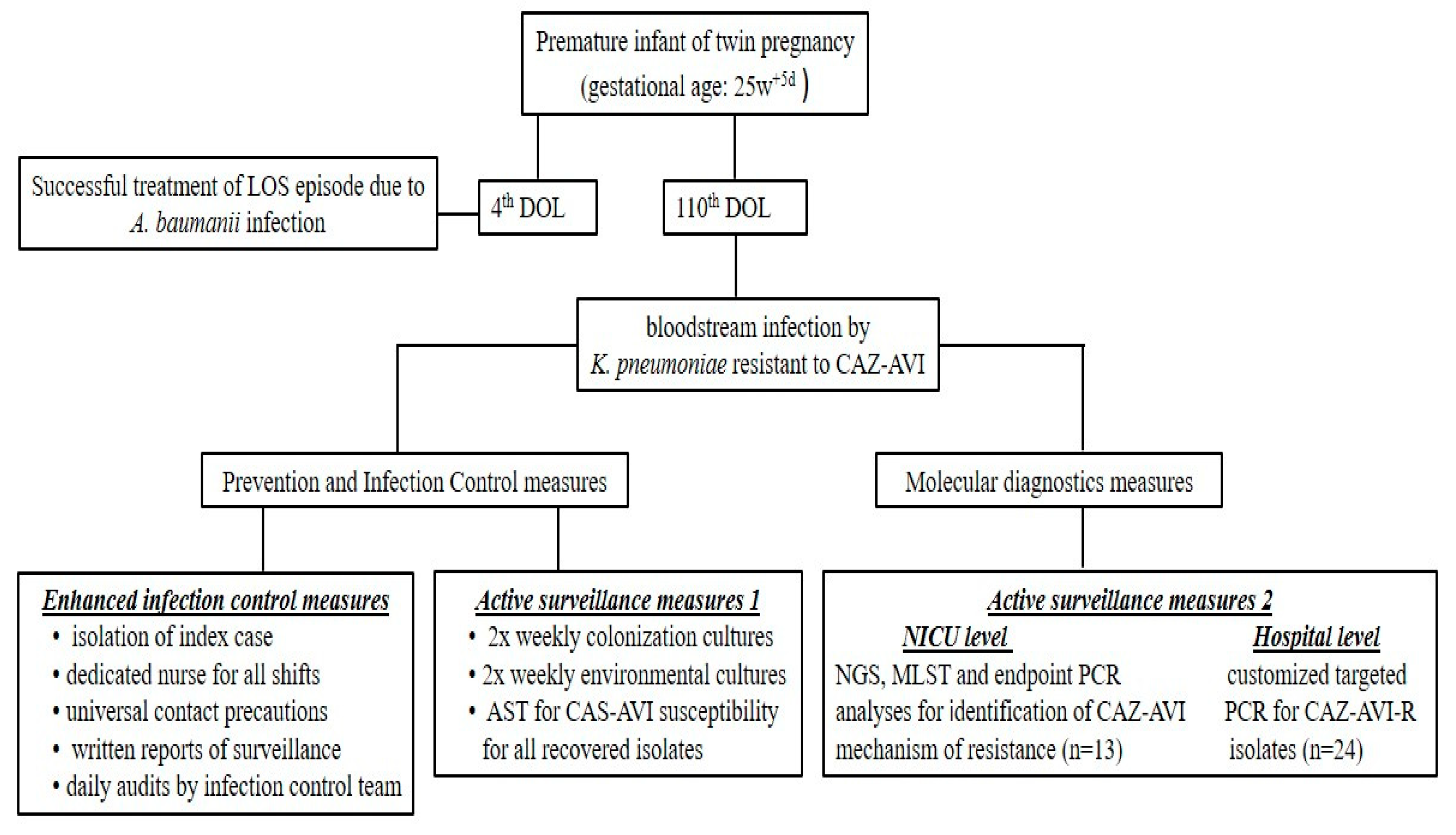
2.1. Index Case
NGS Report
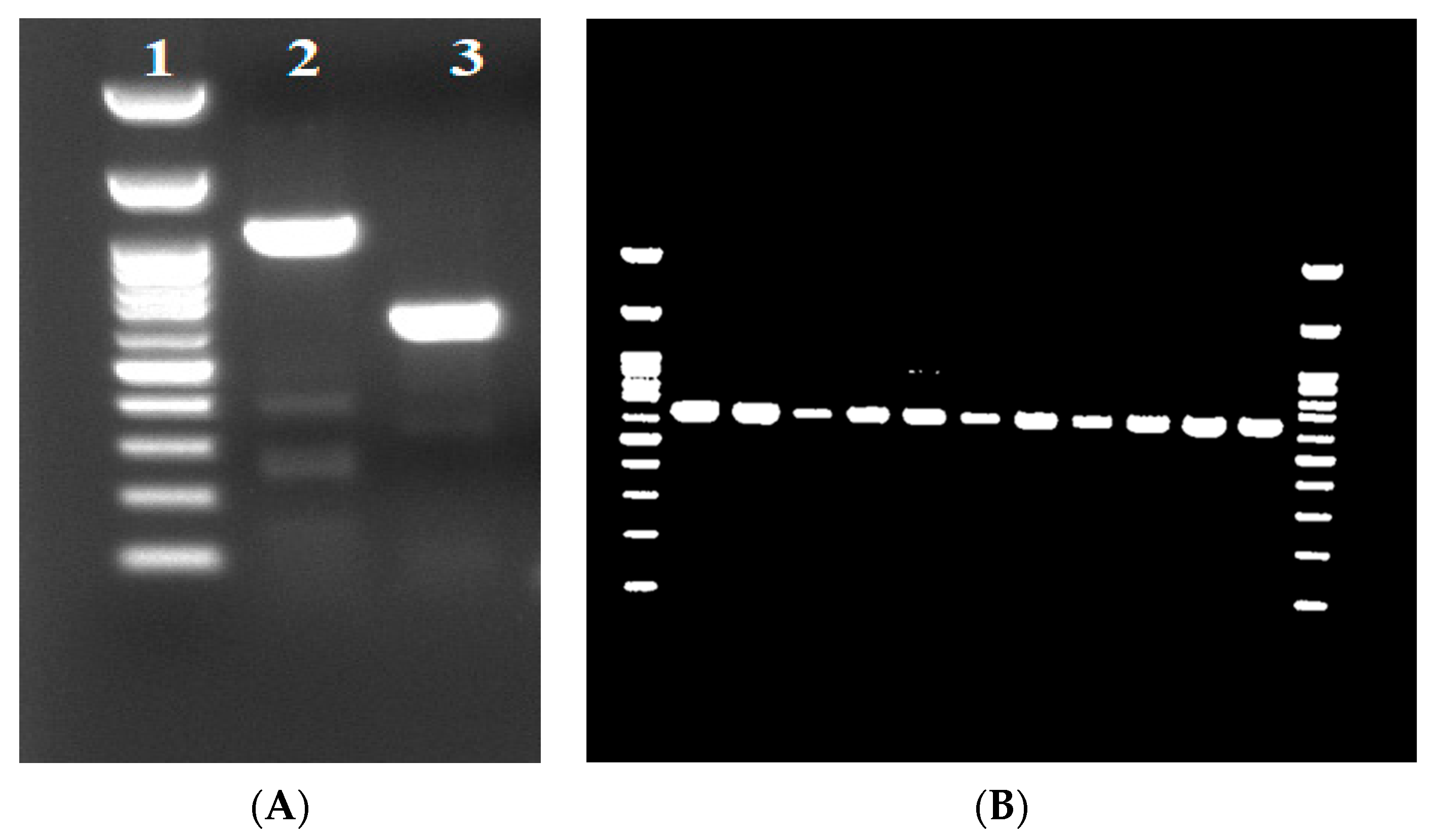
2.2. Molecular and Phenotypic Surveillance within the NICU and the Hospital
2.3. Overall Assessment
3. Discussion
4. Materials and Methods
4.1. Risk Assessment and Bundle of Actions Taken after Index Case
4.1.1. Infection Control Measures
4.1.2. Active Surveillance
4.2. Microbiological Methods, Antimicrobial Susceptibility Testing, and Phenotypic Analysis
4.3. Next-Generation Sequencing (NGS)
4.4. MLST and Detection of Antimicrobial Resistance Genes and Plasmids
4.5. Targeted PCR Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Accession Numbers
References
- Aljeldah, M.M. Antimicrobial Resistance and Its Spread Is a Global Threat. Antibiotics 2022, 11, 1082. [Google Scholar] [CrossRef] [PubMed]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reygaert, W.C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018, 4, 482–501. [Google Scholar] [CrossRef] [PubMed]
- Chaw, P.S.; Hopner, J.; Mikolajczyk, R. The knowledge, attitude and practice of health practitioners towards antibiotic prescribing and resistance in developing countries-A systematic review. J. Clin. Pharm. Ther. 2018, 43, 606–613. [Google Scholar] [CrossRef] [Green Version]
- Schurch, A.C.; van Schaik, W. Challenges and opportunities for whole-genome sequencing-based surveillance of antibiotic resistance. Ann. N.Y. Acad. Sci. 2017, 1388, 108–120. [Google Scholar] [CrossRef]
- Ssekatawa, K.; Byarugaba, D.K.; Nakavuma, J.L.; Kato, C.D.; Ejobi, F.; Tweyongyere, R.; Eddie, W.M. Prevalence of pathogenic Klebsiella pneumoniae based on PCR capsular typing harbouring carbapenemases encoding genes in Uganda tertiary hospitals. Antimicrob. Resist. Infect. Control. 2021, 10, 57. [Google Scholar] [CrossRef]
- Juan, C.H.; Chuang, C.; Chen, C.H.; Li, L.; Lin, Y.T. Clinical characteristics, antimicrobial resistance and capsular types of community-acquired, healthcare-associated, and nosocomial Klebsiella pneumoniae bacteremia. Antimicrob. Resist. Infect. Control. 2019, 8, 1. [Google Scholar] [CrossRef]
- Milton, R.; Gillespie, D.; Dyer, C.; Taiyari, K.; Carvalho, M.J.; Thomson, K.; Sands, K.; Portal, E.A.R.; Hood, K.; Ferreira, A.; et al. Neonatal sepsis and mortality in low-income and middle-income countries from a facility-based birth cohort: An international multisite prospective observational study. Lancet Glob. Health 2022, 10, e661–e672. [Google Scholar] [CrossRef]
- Agyeman, A.A.; Bergen, P.J.; Rao, G.G.; Nation, R.L.; Landersdorfer, C.B. Mortality, clinical and microbiological response following antibiotic therapy among patients with carbapenem-resistant Klebsiella pneumoniae infections (a meta-analysis dataset). Data Brief 2020, 28, 104907. [Google Scholar] [CrossRef]
- Cassini, A.; Plachouras, D.; Monnet, D.L. Attributable deaths caused by infections with antibiotic-resistant bacteria in France–Authors’ reply. Lancet Infect. Dis. 2019, 19, 129–130. [Google Scholar] [CrossRef] [Green Version]
- Alexander, B.T.; Marschall, J.; Tibbetts, R.J.; Neuner, E.A.; Dunne, W.M., Jr.; Ritchie, D.J. Treatment and clinical outcomes of urinary tract infections caused by KPC-producing Enterobacteriaceae in a retrospective cohort. Clin. Ther. 2012, 34, 1314–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainoda, Y.; Aoki, K.; Ishii, Y.; Okuda, K.; Furukawa, H.; Manabe, R.; Sahara, T.; Nakamura-Uchiyama, F.; Kurosu, H.; Ando, Y.; et al. Klebsiella pneumoniae carbapenemase (KPC)-producing Klebsiella pneumoniae ST258 isolated from a Japanese patient without a history of foreign travel-a new public health concern in Japan: A case report. BMC Infect. Dis. 2019, 19, 20. [Google Scholar] [CrossRef] [Green Version]
- Mathers, A.J.; Vegesana, K.; German-Mesner, I.; Ainsworth, J.; Pannone, A.; Crook, D.W.; Sifri, C.D.; Sheppard, A.; Stoesser, N.; Peto, T.; et al. Risk factors for Klebsiella pneumoniae carbapenemase (KPC) gene acquisition and clinical outcomes across multiple bacterial species. J. Hosp. Infect. 2020, 104, 456–468. [Google Scholar] [CrossRef] [Green Version]
- Jean, S.S.; Harnod, D.; Hsueh, P.R. Global Threat of Carbapenem-Resistant Gram-Negative Bacteria. Front. Cell. Infect. Microbiol. 2022, 12, 823684. [Google Scholar] [CrossRef]
- Sherry, N.; Howden, B. Emerging Gram negative resistance to last-line antimicrobial agents fosfomycin, colistin and ceftazidime-avibactam-epidemiology, laboratory detection and treatment implications. Expert Rev. Anti-Infect. Ther. 2018, 16, 289–306. [Google Scholar] [CrossRef]
- Coskun, Y.; Atici, S. Successful Treatment of Pandrug-resistant Klebsiella pneumoniae Infection With Ceftazidime-avibactam in a Preterm Infant: A Case Report. Pediatr. Infect. Dis. J. 2020, 39, 854–856. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves New Antibacterial Drug Avycaz; FDA news release; U.S. FDA: Silver Spring, MD, USA, 2015. [Google Scholar]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum beta-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2022, 75, 187–212. [Google Scholar] [CrossRef]
- van Duin, D.; Bonomo, R.A. Ceftazidime/Avibactam and Ceftolozane/Tazobactam: Second-generation beta-Lactam/beta-Lactamase Inhibitor Combinations. Clin. Infect. Dis. 2016, 63, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Di Bella, S.; Giacobbe, D.R.; Maraolo, A.E.; Viaggi, V.; Luzzati, R.; Bassetti, M.; Luzzaro, F.; Principe, L. Resistance to ceftazidime/avibactam in infections and colonisations by KPC-producing Enterobacterales: A systematic review of observational clinical studies. J. Glob. Antimicrob. Resist. 2021, 25, 268–281. [Google Scholar] [CrossRef]
- ECDC. Emergence of Resistance to Ceftazidime-Avibactam in Carbapenem-Resistant Enterobacteriaceae-12 June 2018; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Hemarajata, P.; Humphries, R.M. Ceftazidime/avibactam resistance associated with L169P mutation in the omega loop of KPC-2. J. Antimicrob. Chemother. 2019, 74, 1241–1243. [Google Scholar] [CrossRef]
- Haidar, G.; Clancy, C.J.; Shields, R.K.; Hao, B.; Cheng, S.; Nguyen, M.H. Mutations in blaKPC-3 That Confer Ceftazidime-Avibactam Resistance Encode Novel KPC-3 Variants That Function as Extended-Spectrum beta-Lactamases. Antimicrob. Agents Chemother. 2017, 61, e02245-21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galani, I.; Karaiskos, I.; Souli, M.; Papoutsaki, V.; Galani, L.; Gkoufa, A.; Antoniadou, A.; Giamarellou, H. Outbreak of KPC-2-producing Klebsiella pneumoniae endowed with ceftazidime-avibactam resistance mediated through a VEB-1-mutant (VEB-25), Greece, September to October 2019. Euro Surveill. 2020, 25, 2000028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castanheira, M.; Simner, P.J.; Bradford, P.A. Extended-spectrum beta-lactamases: An update on their characteristics, epidemiology and detection. JAC-Antimicrob. Resist. 2021, 3, dlab092. [Google Scholar] [CrossRef] [PubMed]
- Humphries, R.M.; Hemarajata, P. Resistance to Ceftazidime-Avibactam in Klebsiella pneumoniae Due to Porin Mutations and the Increased Expression of KPC-3. Antimicrob. Agents Chemother. 2017, 61, 10–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, K.; Hemarajata, P.; Sun, D.; Rubio-Aparicio, D.; Tsivkovski, R.; Yang, S.; Sebra, R.; Kasarskis, A.; Nguyen, H.; Hanson, B.M.; et al. Resistance to Ceftazidime-Avibactam Is Due to Transposition of KPC in a Porin-Deficient Strain of Klebsiella pneumoniae with Increased Efflux Activity. Antimicrob. Agents Chemother. 2017, 61, e00989-17. [Google Scholar] [CrossRef] [Green Version]
- Protonotariou, E.; Meletis, G.; Pilalas, D.; Mantzana, P.; Tychala, A.; Kotzamanidis, C.; Papadopoulou, D.; Papadopoulos, T.; Polemis, M.; Metallidis, S.; et al. Polyclonal Endemicity of Carbapenemase-Producing Klebsiella pneumoniae in ICUs of a Greek Tertiary Care Hospital. Antibiotics 2022, 11, 149. [Google Scholar] [CrossRef]
- Lahiri, S.D.; Alm, R.A. Identification of Novel VEB beta-Lactamase Enzymes and Their Impact on Avibactam Inhibition. Antimicrob. Agents Chemother. 2016, 60, 3183–3186. [Google Scholar] [CrossRef] [Green Version]
- Carattoli, A.; Hasman, H. PlasmidFinder and In Silico pMLST: Identification and Typing of Plasmid Replicons in Whole-Genome Sequencing (WGS). Methods Mol. Biol. 2020, 2075, 285–294. [Google Scholar] [CrossRef]
- Clausen, P.; Aarestrup, F.M.; Lund, O. Rapid and precise alignment of raw reads against redundant databases with KMA. BMC Bioinform. 2018, 19, 307. [Google Scholar] [CrossRef]
- Larsen, M.V.; Cosentino, S.; Rasmussen, S.; Friis, C.; Hasman, H.; Marvig, R.L.; Jelsbak, L.; Sicheritz-Ponten, T.; Ussery, D.W.; Aarestrup, F.M.; et al. Multilocus sequence typing of total-genome-sequenced bacteria. J. Clin. Microbiol. 2012, 50, 1355–1361. [Google Scholar] [CrossRef] [Green Version]
- Bartual, S.G.; Seifert, H.; Hippler, C.; Luzon, M.A.; Wisplinghoff, H.; Rodriguez-Valera, F. Development of a multilocus sequence typing scheme for characterization of clinical isolates of Acinetobacter baumannii. J. Clin. Microbiol. 2005, 43, 4382–4390. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, D.; Fawley, W.; Kachrimanidou, M.; Bowden, R.; Crook, D.W.; Fung, R.; Golubchik, T.; Harding, R.M.; Jeffery, K.J.; Jolley, K.A.; et al. Multilocus sequence typing of Clostridium difficile. J. Clin. Microbiol. 2010, 48, 770–778. [Google Scholar] [CrossRef] [Green Version]
- Jaureguy, F.; Landraud, L.; Passet, V.; Diancourt, L.; Frapy, E.; Guigon, G.; Carbonnelle, E.; Lortholary, O.; Clermont, O.; Denamur, E.; et al. Phylogenetic and genomic diversity of human bacteremic Escherichia coli strains. BMC Genom. 2008, 9, 560. [Google Scholar] [CrossRef] [Green Version]
- Wirth, T.; Falush, D.; Lan, R.; Colles, F.; Mensa, P.; Wieler, L.H.; Karch, H.; Reeves, P.R.; Maiden, M.C.; Ochman, H.; et al. Sex and virulence in Escherichia coli: An evolutionary perspective. Mol. Microbiol. 2006, 60, 1136–1151. [Google Scholar] [CrossRef] [Green Version]
- Lemee, L.; Dhalluin, A.; Pestel-Caron, M.; Lemeland, J.F.; Pons, J.L. Multilocus sequence typing analysis of human and animal Clostridium difficile isolates of various toxigenic types. J. Clin. Microbiol. 2004, 42, 2609–2617. [Google Scholar] [CrossRef] [Green Version]
- Zusman, O.; Altunin, S.; Koppel, F.; Dishon Benattar, Y.; Gedik, H.; Paul, M. Polymyxin monotherapy or in combination against carbapenem-resistant bacteria: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2017, 72, 29–39. [Google Scholar] [CrossRef] [Green Version]
- Shi, Q.; Han, R.; Guo, Y.; Yang, Y.; Wu, S.; Ding, L.; Zhang, R.; Yin, D.; Hu, F. Multiple Novel Ceftazidime-Avibactam-Resistant Variants of bla(KPC-2)-Positive Klebsiella pneumoniae in Two Patients. Microbiol. Spectr. 2022, 10, e0171421. [Google Scholar] [CrossRef]
- Shields, R.K.; Chen, L.; Cheng, S.; Chavda, K.D.; Press, E.G.; Snyder, A.; Pandey, R.; Doi, Y.; Kreiswirth, B.N.; Nguyen, M.H.; et al. Emergence of Ceftazidime-Avibactam Resistance Due to Plasmid-Borne bla(KPC-3) Mutations during Treatment of Carbapenem-Resistant Klebsiella pneumoniae Infections. Antimicrob. Agents Chemother. 2017, 61, 10–1128. [Google Scholar] [CrossRef] [Green Version]
- Findlay, J.; Poirel, L.; Bouvier, M.; Gaia, V.; Nordmann, P. Resistance to ceftazidime-avibactam in a KPC-2-producing Klebsiella pneumoniae caused by the extended-spectrum beta-lactamase VEB-25. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 639–644. [Google Scholar] [CrossRef]
- Galani, I.; Antoniadou, A.; Karaiskos, I.; Kontopoulou, K.; Giamarellou, H.; Souli, M. Genomic characterization of a KPC-23-producing Klebsiella pneumoniae ST258 clinical isolate resistant to ceftazidime-avibactam. Clin. Microbiol. Infect. 2019, 25, 763.e5–763.e8. [Google Scholar] [CrossRef]
- Voulgari, E.; Kotsakis, S.D.; Giannopoulou, P.; Perivolioti, E.; Tzouvelekis, L.S.; Miriagou, V. Detection in two hospitals of transferable ceftazidime-avibactam resistance in Klebsiella pneumoniae due to a novel VEB beta-lactamase variant with a Lys234Arg substitution, Greece, 2019. Euro Surveill. 2020, 25, 1900766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, S.R.; Tran, T.T.T.; Hujer, A.M.; Hill, C.B.; Hujer, K.M.; Mediavilla, J.R.; Manca, C.; Domitrovic, T.N.; Perez, F.; Farmer, M.; et al. Rapid Molecular Diagnostics to Inform Empiric Use of Ceftazidime/Avibactam and Ceftolozane/Tazobactam Against Pseudomonas aeruginosa: PRIMERS IV. Clin. Infect. Dis. 2019, 68, 1823–1830. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Strain ID | A1746/22 | |
|---|---|---|
| Date of isolation | 25 February 2022 | |
| Biological sample | Blood | |
| MLST | 35 | |
| Plasmids | IncC, IncR, IncFIA(HI1), IncFIB(K), IncFIB(pKPHS1), IncFIB(pQil), IncFII(K) | |
| Antibiotic Resistance | β-lactamases | SHV-33, TEM-1B, VEB-25, DHA-1, OXA-10 |
| Carbapenemases | KPC-2 | |
| Aminoglycosides | ant(2″)-Ia, aph(3″)-Ib, aph(6)-Id, rmtB, aadA1 | |
| Quinolone | qnrB4, oqxA, oqxB | |
| Fosfomycin | fosA | |
| Sulfonamide | sul1, sul2 | |
| Phenicol | catA1, cmlA1 | |
| Tetracycline | tet(A), tet(G) | |
| Resistance to Heavy Metals | merC, merP, merT, silR | |
| Virulence | kfuA, mrkA, mrkF, mrkH, mrkl, ybtE, ybtQ, ybtT, ybtX | |
| Capsule | wzi | |
| Efflux and Regulator Systems | acrR, envR, fis, marA, marR, oqxR, rob, sdiA, soxR, soxS, ramA, ramR, rarA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarras, C.; Iosifidis, E.; Simitsopoulou, M.; Pappa, S.; Kontou, A.; Roilides, E.; Papa, A. Neonatal Bloodstream Infection with Ceftazidime-Avibactam-Resistant blaKPC-2-Producing Klebsiella pneumoniae Carrying blaVEB-25. Antibiotics 2023, 12, 1290. https://doi.org/10.3390/antibiotics12081290
Zarras C, Iosifidis E, Simitsopoulou M, Pappa S, Kontou A, Roilides E, Papa A. Neonatal Bloodstream Infection with Ceftazidime-Avibactam-Resistant blaKPC-2-Producing Klebsiella pneumoniae Carrying blaVEB-25. Antibiotics. 2023; 12(8):1290. https://doi.org/10.3390/antibiotics12081290
Chicago/Turabian StyleZarras, Charalampos, Elias Iosifidis, Maria Simitsopoulou, Styliani Pappa, Angeliki Kontou, Emmanuel Roilides, and Anna Papa. 2023. "Neonatal Bloodstream Infection with Ceftazidime-Avibactam-Resistant blaKPC-2-Producing Klebsiella pneumoniae Carrying blaVEB-25" Antibiotics 12, no. 8: 1290. https://doi.org/10.3390/antibiotics12081290
APA StyleZarras, C., Iosifidis, E., Simitsopoulou, M., Pappa, S., Kontou, A., Roilides, E., & Papa, A. (2023). Neonatal Bloodstream Infection with Ceftazidime-Avibactam-Resistant blaKPC-2-Producing Klebsiella pneumoniae Carrying blaVEB-25. Antibiotics, 12(8), 1290. https://doi.org/10.3390/antibiotics12081290