
The Microbiological Profile and Antibiotic Susceptibility of Fracture Related Infections in a Low Resource Setting Differ from High Resource Settings: A Cohort Study from Cameroon
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Profile of Isolated Microorganisms
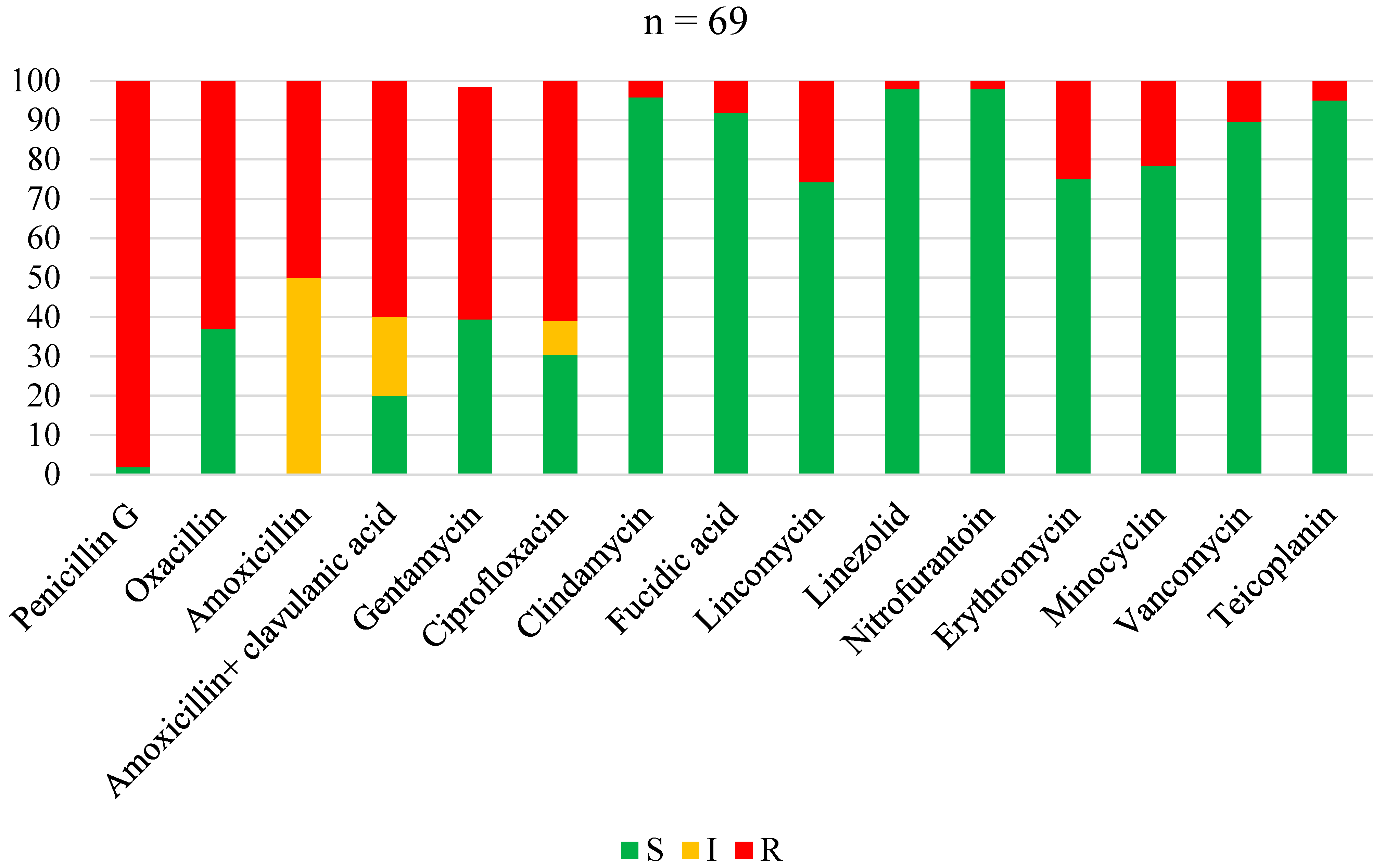
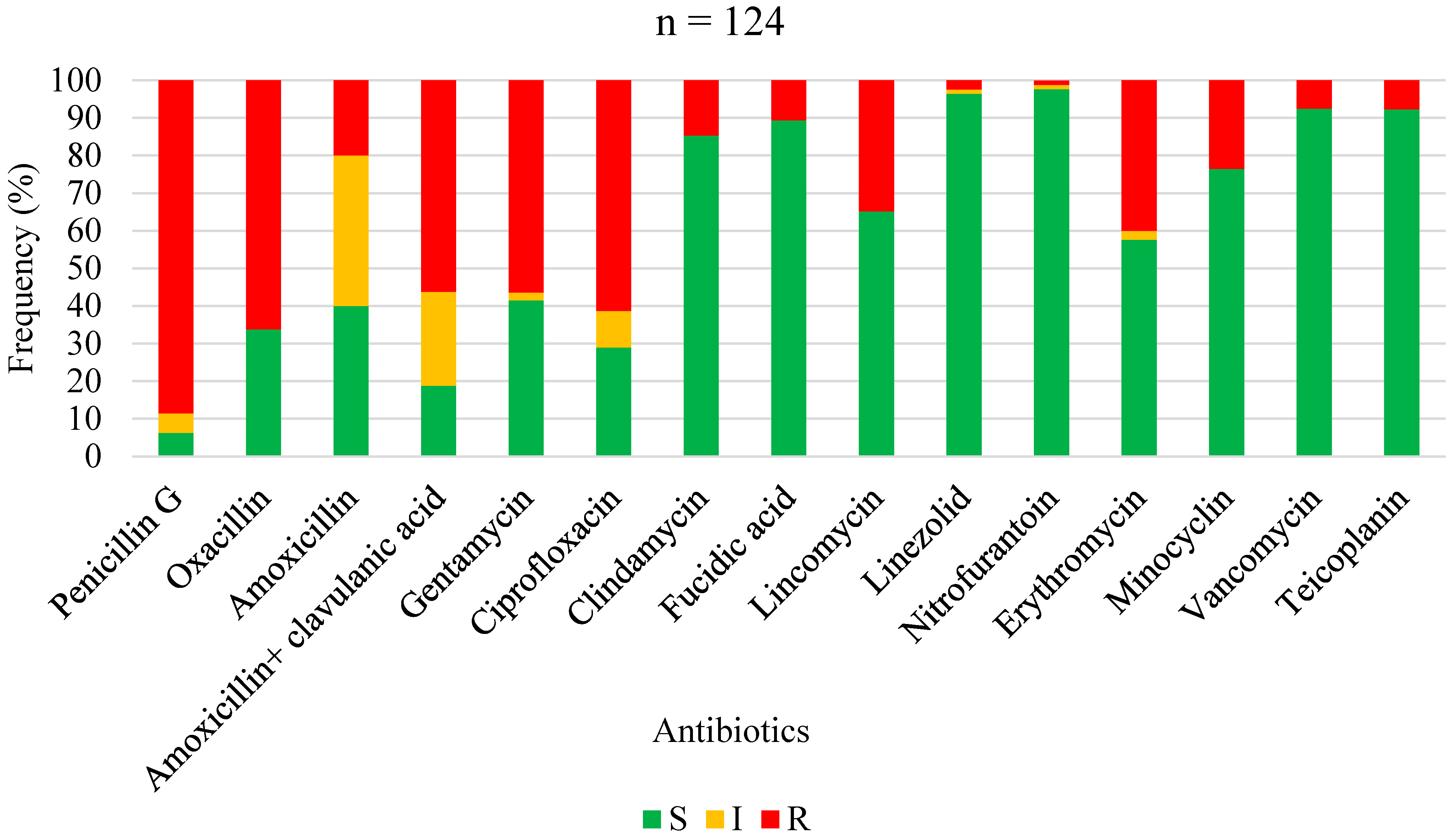
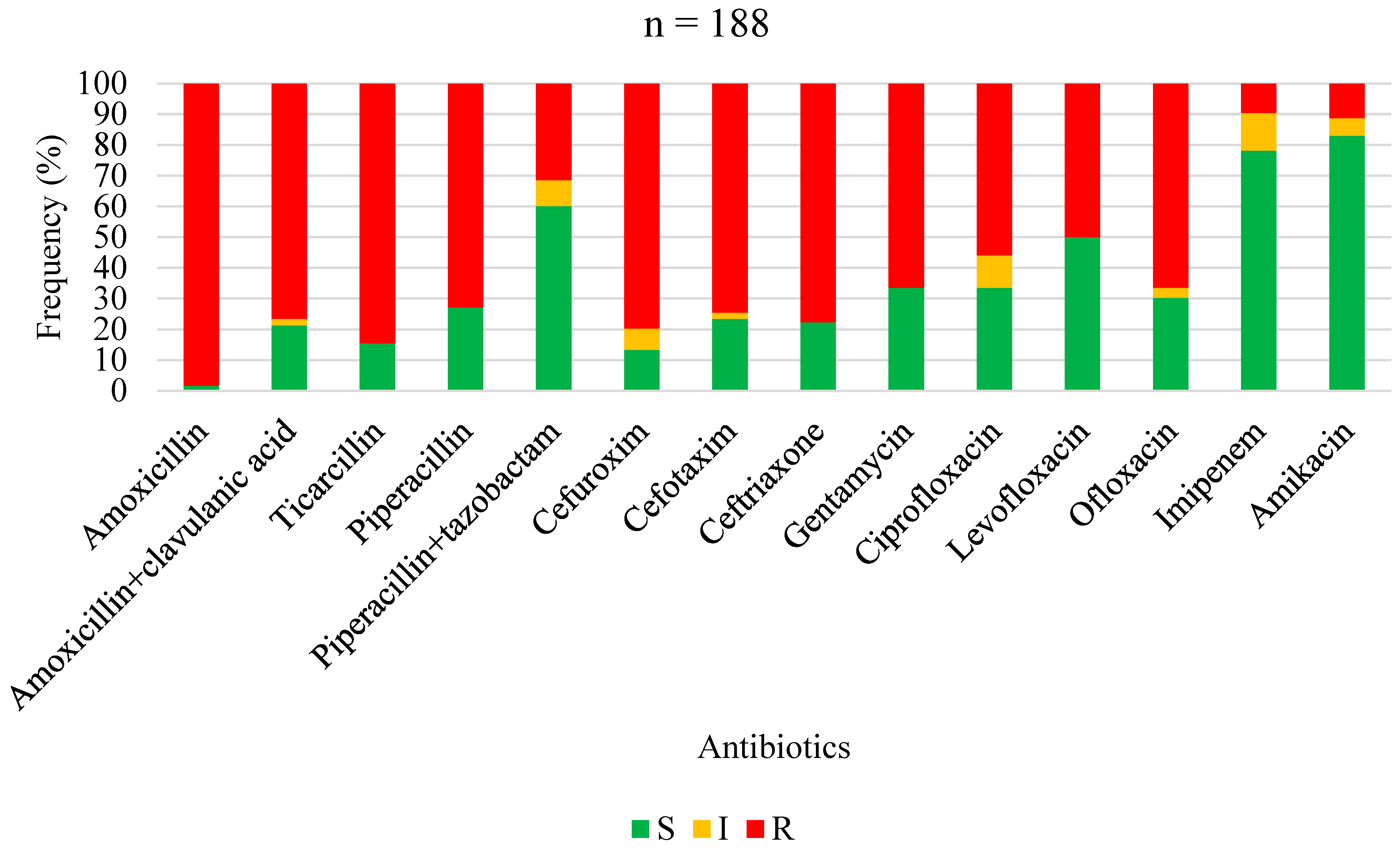
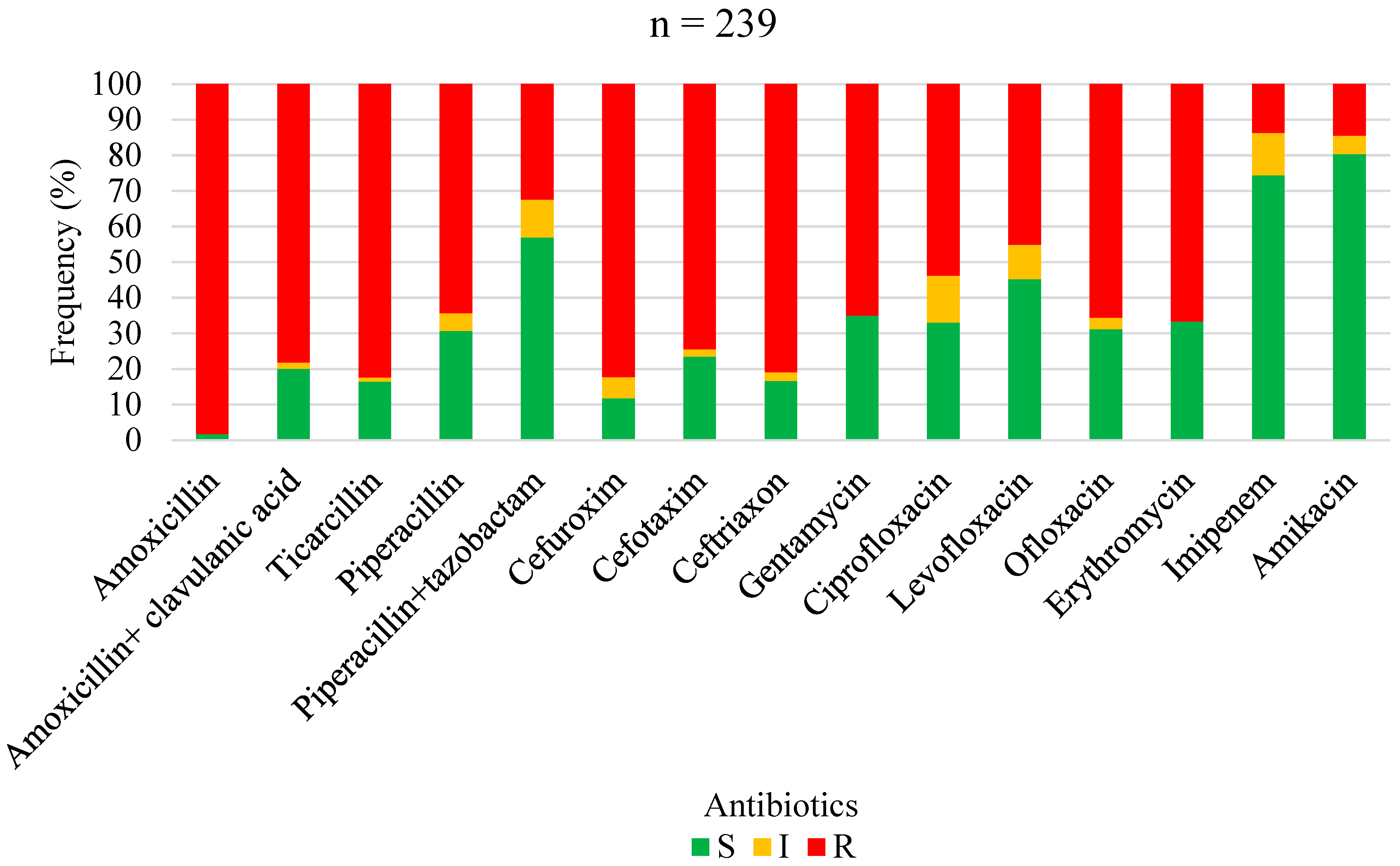
2.2. Antimicrobial Susceptibility of Isolated Pathogens
3. Discussion
NR Not Reported
4. Materials and Methods
4.1. Study Design and Patient Identification
4.2. Data Collection
4.3. Microbiological Analysis
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Metsemakers, W.J.; Moriarty, T.F.; Morgenstern, M.; Marais, L.; Onsea, J.; O’Toole, R.V.; Depypere, M.; Obremskey, W.T.; Verhofstad, M.H.J.; McNally, M.; et al. The global burden of fracture-related infection: Can we do better? Lancet Infect. Dis. 2023. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.S.H.; Lee, A.L.H.; Fang, C.; Leung, H.C.H.; Liu, A.H.Y.; So, R.C.K.; Yung, C.S.Y.; Wong, T.M.; Leung, F. Outcomes of fracture-related infections—Do organism, depth of involvement, and temporality count? J. Orthop. Surg. 2022, 30, 10225536221118519. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.H.; Gill, L.I.; Tissingh, E.K.; Galanis, A.; Hadjihannas, I.; Iliadis, A.D.; Heidari, N.; Cherian, B.; Rosmarin, C.; Vris, A. Microbiological Profile of Fracture Related Infection at a UK Major Trauma Centre. Antibiotics 2023, 12, 1358. [Google Scholar] [CrossRef] [PubMed]
- Rupp, M.; Baertl, S.; Walter, N.; Hitzenbichler, F.; Ehrenschwender, M.; Alt, V. Is There a Difference in Microbiological Epidemiology and Effective Empiric Antimicrobial Therapy Comparing Fracture-Related Infection and Periprosthetic Joint Infection? A Retrospective Comparative Study. Antibiotics 2021, 10, 921. [Google Scholar] [CrossRef] [PubMed]
- Depypere, M.; Kuehl, R.; Metsemakers, W.J.; Senneville, E.; McNally, M.A.; Obremskey, W.T.; Zimmerli, W.; Atkins, B.L.; Trampuz, A. Recommendations for Systemic Antimicrobial Therapy in Fracture-Related Infection: A Consensus From an International Expert Group. J. Orthop. Trauma 2020, 34, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.J.; Morgenstern, M.; Senneville, E.; Borens, O.; Govaert, G.A.M.; Onsea, J.; Depypere, M.; Richards, R.G.; Trampuz, A.; Verhofstad, M.H.J.; et al. General treatment principles for fracture-related infection: Recommendations from an international expert group. Arch. Orthop. Trauma Surg. 2020, 140, 1013–1027. [Google Scholar] [CrossRef]
- Dudareva, M.; Hotchen, A.J.; Ferguson, J.; Hodgson, S.; Scarborough, M.; Atkins, B.L.; McNally, M.A. The microbiology of chronic osteomyelitis: Changes over ten years. J. Infect. 2019, 79, 189–198. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Morgenstern, M.; McNally, M.A.; Moriarty, T.F.; McFadyen, I.; Scarborough, M.; Athanasou, N.A.; Ochsner, P.E.; Kuehl, R.; Raschke, M.; et al. Fracture-related infection: A consensus on definition from an international expert group. Injury 2018, 49, 505–510. [Google Scholar] [CrossRef]
- Abalo, A.; Walla, A.; Ayouba, G.; Ndjam, M.; Agounké, W.; Dossim, A. Surgical site infection (SSI) in orthopaedics’ patients in a developing country. Rev. De Chir. Orthopédique Et Traumatol. 2010, 96, 112–117. [Google Scholar] [CrossRef]
- Bercion, R.; Gaudeuille, A.; Mapouka, P.A.; Behounde, T.; Guetahoun, Y. Surgical site infection survey in the Orthopaedics surgery department of the “Hôpital communautaire de Bangui” Central African Republic. Bull. Soc. Pathol. Exot. 2007, 100, 197–200. [Google Scholar]
- Fonkoue, L.; Tissingh, E.K.; Muluem, O.K.; Kong, D.; Ngongang, O.; Tambekou, U.; Handy, D.; Cornu, O.; McNally, M. Predictive factors for fracture-related infection in open tibial fractures in a Sub-Saharan African setting. Injury 2023, 54, 110816. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Lyu, J.; Ma, J.; Huang, X.; Chen, K.; Wang, S.; Wei, Y.; Shi, J.; Xia, J.; Zhao, G.; et al. Comparative analysis of pathogen distribution in patients with fracture-related infection and periprosthetic joint infection: A retrospective study. BMC Musculoskelet. Disord. 2023, 24, 123. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, N.; Tsang, S.-T.J.; Rensburg AJv Rudolph Venter, G.Z.E. Unexpected high prevalence of Gram-negative pathogens in fracture-related infection: Is it time to consider extended Gram-negative cover antibiotic prophylaxis in open fractures? S. Afr. Orthop. J. 2023, 22, 146–150. [Google Scholar]
- Mthethwa, P.G.; Marais, L.C. The microbiology of chronic osteomyelitis in a developing world setting. SA Orthop. J. 2017, 16, 39–45. [Google Scholar] [CrossRef]
- Wang, B.; Xiao, X.; Zhang, J.; Han, W.; Hersi, S.A.; Tang, X. Epidemiology and microbiology of fracture-related infection: A multicenter study in Northeast China. J. Orthop. Surg. Res. 2021, 16, 490. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, A.B.; Yerriswamy, P.R.; Suphala, B.; Ananya, G.; Vinod Kumar, C.S. Microbiological and antibiotic profile of osteomyelitis in tertiary care hospital. Int. Surg. J. 2021, 8, 910–914. [Google Scholar]
- Willenegger, H.; Roth, B. Treatment tactics and late results in early infection following osteosynthesis. Unfallchirurgie 1986, 12, 241–246. [Google Scholar] [CrossRef]
- Depypere, M.; Sliepen, J.; Onsea, J.; Debaveye, Y.; Govaert, G.A.M.; Ijpma, F.F.A.; Zimmerli, W.; Metsemakers, W.J. The Microbiological Etiology of Fracture-Related Infection. Front. Cell. Infect. Microbiol. 2022, 12, 934485. [Google Scholar] [CrossRef]
- Baertl, S.; Walter, N.; Engelstaedter, U.; Ehrenschwender, M.; Hitzenbichler, F.; Alt, V.; Rupp, M. What Is the Most Effective Empirical Antibiotic Treatment for Early, Delayed, and Late Fracture-Related Infections? Antibiotics 2022, 11, 287. [Google Scholar] [CrossRef]
- Corrigan, R.A.; Sliepen, J.; Dudareva, M.; FFAIJ; Govaert, G.; Atkins, B.L.; Rentenaar, R.; Wouthuyzen-Bakker, M.; McNally, M. Causative Pathogens Do Not Differ between Early, Delayed or Late Fracture-Related Infections. Antibiotics 2022, 11, 943. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, P.; Wang, W.; Wang, S.; Li, B.; Li, J.; Yang, B.; Li, M.; Li, Q.; Yang, H.; et al. Epidemiology and Drug Resistance of Fracture-Related Infection of the Long Bones of the Extremities: A Retrospective Study at the Largest Trauma Center in Southwest China. Front. Microbiol. 2022, 13, 923735. [Google Scholar] [CrossRef]
- Kuehl, R.; Tschudin-Sutter, S.; Morgenstern, M.; Dangel, M.; Egli, A.; Nowakowski, A.; Suhm, N.; Theilacker, C.; Widmer, A.F. Time-dependent differences in management and microbiology of orthopaedic internal fixation-associated infections: An observational prospective study with 229 patients. Clin. Microbiol. Infect. 2019, 25, 76–81. [Google Scholar] [CrossRef]
- Collaborators, A.R. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar]
- Di Gennaro, F.; Marotta, C.; Amicone, M.; Bavaro, D.F.; Bernaudo, F.; Frisicale, E.M.; Kurotschka, P.; Mazzari, A.; Veronese, N.; Murri, R.; et al. Italian young doctors’ knowledge, attitudes and practices on antibiotic use and resistance: A national cross-sectional survey. J. Glob. Antimicrob. Resist. 2020, 23, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Bezstarosti, H.; Croughs, P.D.; Van den Hurk, M.K.B.; Kortram, K.; Oprel, P.; Metsemakers, W.J.; Van Lieshout, E.M.M.; Verhofstad, M.H.J. Antimicrobial Effect of Cerament G on Bacterial Isolates, with Various Levels of Gentamicin Resistance, Found in Fracture-Related Infection: An In Vitro Study. eCM Online Periodical. 2019. Collection 5; eCM Conference Abstracts (page P1). Available online: https://wwwecmconferencesorg/abstracts/2019/Collection5/posterspdf2022 (accessed on 24 October 2022).
- Onsea, J.; Van Lieshout, E.M.M.; Zalavras, C.; Sliepen, J.; Depypere, M.; Noppe, N.; Ferguson, J.; Verhofstad, M.H.J.; Govaert, G.A.M.; Jpma, F.F.A.; et al. Validation of the diagnostic criteria of the consensus definition of fracture-related infection. Injury 2022, 53, 1867–1879. [Google Scholar] [CrossRef] [PubMed]
- Dudareva, M.; Barrett, L.K.; Morgenstern, M.; Atkins, B.L.; Brent, A.J.; McNally, M.A. Providing an Evidence Base for Tissue Sampling and Culture Interpretation in Suspected Fracture-Related Infection. J. Bone Jt. Surg. [AM] 2021, 103, 977–983. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value (N = 217) |
|---|---|
| Age (in years) (mean ± SD, range) | 40.64 ± 15.12 (5–85) |
| Gender: number of men (%) | 150 (69.1%) |
| Body mass index (kg/m2) | 27.22 ± 4.59 |
| Alcohol, number (%) | 14 (6.5%) |
| Obesity, number (%) | 7 (4.8%) |
| Diabetes, number (%) | 6 (2.7%) |
| HIV, number (%) | 3 (1.4%) |
| Smoking, number (%) | 5 (2.3%) |
| Initial fracture | |
| Closed fracture | 110 (52.1%) |
| Open fracture | 107 (47.9%) |
| Site of the FRI | |
| Tibia | 95 (42.6%) |
| Femur | 87 (39.0%) |
| Ankle | 13 (5.8%) |
| Humerus | 8 (3.6%) |
| Radius | 7 (3.1%) |
| Ulna | 6 (2.7%) |
| Fibula | 3 (1.3%) |
| Carpus | 2 (0.9%) |
| Tarsus | 1 (0.5%) |
| Patella | 1 (0.5%) |
| Classification of FRI | |
| Early | 115 (53.0%) |
| Delayed | 37 (17.1%) |
| Late | 65 (29.9%) |
| Number of isolated microorganisms per culture | |
| 0 | 37 (15.1%) |
| 1 | 100 (40.6%) |
| 2 | 67 (27.2%) |
| 3 | 39 (15.9%) |
| 4 | 3 (1.2%) |
| Microorganism | Number | Percentage of Positive Cultures |
|---|---|---|
| Gram-positive bacteria | ||
| Staphylococcus aureus | 69 | 19 |
| Coagulase-negative Staphylococcus | 21 | 5.8 |
| Enterococcus faecalis | 16 | 4.4 |
| Enterococcus faecium | 3 | 0.8 |
| Other Enterococcus | 6 | 1.6 |
| Group A Streptococcus | 4 | 1.1 |
| Other Streptococcus | 4 | 1.1 |
| Other GPC | 1 | 0.3 |
| Gram-negative bacteria | ||
| Enterobacterales | ||
| Enterobacter cloacae | 43 | 11.8 |
| Klebsiella pneumoniae | 36 | 9.9 |
| Escherichia coli | 35 | 9.6 |
| Proteus mirabilis | 17 | 4.7 |
| Morganella morganii | 14 | 3.9 |
| Providencia stuartii | 8 | 2.2 |
| Citrobacter freundii | 5 | 1.4 |
| Other Enterobacterales | 30 | 8.3 |
| Non-fermenting Gram-negative bacilli | ||
| Pseudomonas aeruginosa | 27 | 7.4 |
| Acinetobacter baumannii | 4 | 1.1 |
| Sternotrophomonas maltophilia | 2 | 0.6 |
| Other non-fermenting Gram-negative bacilli | 11 | 3.1 |
| Other GNB | 6 | 1.6 |
| Total | 363 | 100% |
| Variable | Early FR In (%) | Delayed FR In (%) | Late FR In (%) | Whole Group n (%) | p-Value * |
|---|---|---|---|---|---|
| Number of cases | 127 (51.6) | 44 (17.9) | 75 (30.5) | 246 (100) | |
| Culture type | |||||
| Monomicrobial (%) | 45 (35.4) | 18 (41.9) | 37 (48.7) | 100 (40.6) | 0.174 |
| Polymicrobial (%) | 71 (55.9) | 18 (41.9) | 20 (27.6) | 109 (44.3) | 0.000 |
| Culture-negative (%) | 11 (8.7) | 8 (18.6) | 18 (23.7) | 37 (15.1) | 0.012 |
| Gram stain | |||||
| Gram-negative (%) | 156 (70.9) | 41 (73.2) | 42 (48.3) | 239 (65.8) | 0.000 |
| Gram-positive (%) | 64 (29.1) | 15 (26.8) | 45 (51.7) | 124 (34.2) | 0.000 |
| Species isolated | |||||
| Staphylococcus aureus | 33 (15) | 7 (12.5) | 29 (33.3) | 69 (19) | 0.000 |
| Enterobacter cloacae | 23 (10.5) | 12 (21.4) | 8 (9.2) | 43 (11.8) | 0.052 |
| Klebsiella pneumonia | 25 (11.4) | 3 (5.4) | 8 (9.2) | 36 (9.6) | 0.393 |
| Escherichia coli | 22 (10) | 8 (14.3) | 5 (5.7) | 35 (9.6) | 0.231 |
| Pseudomonas aeruginosa | 18 (8.2) | 4 (7.1) | 5 (5.7) | 27 (7.4) | 0.761 |
| CoNS | 8 (3.6) | 6 (10.7) | 7 (8) | 21 (5.9) | 0.075 |
| Proteus mirabilis | 10 (4.5) | 4 (7.1) | 3 (3.4) | 17 (4.7) | 0.587 |
| Enterococcus faecalis | 13 (5.9) | - | 3 (3.4) | 16 (4.4) | 0.139 |
| Morganella morganii | 7 (3.2) | 3 (5.4) | 4 (4.6) | 14 (3.9) | 0.691 |
| Others | 61 (27.7) | 9 (16.1) | 15 (17.2) | 85 (23.7) | 0.055 |
| Total | 220 (100) | 56 (100) | 87 (100) | 363 (100) |
| This Study | Ferriera et al. [13] | Corrigan et al. [20] | Baertl et al. [19] | Depypere et al. [18] | Patel et al. [3] | |
|---|---|---|---|---|---|---|
| Location | Cameroon | South Africa | UK and The Netherlands | Germany | Belgium | UK |
| Number | 246 | 267 | 433 | 117 | 194 | 325 |
| Time of Presentation (%) | ||||||
| Early | 52 | NR | 12 | 16 | 18 | NR |
| Delayed | 17 | NR | 19 | 51 | 38 | NR |
| Late | 31 | NR | 69 | 33 | 44 | NR |
| Type of Culture | ||||||
| Polymicrobial (%) | 44.3 | 14 | 36 | 8.6 | 25.3 | 34.2 |
| Monomicrobial (%) | 40.6 | 67 | 46 | 82 | 71.1 | 48.3 |
| Culture-negative (%) | 15.1 | 19 | 19 | 9.4 | 3.6 | 24.4 |
| Gram Negatives (%) | 65.8 | 55 | 22 | 16.4 | 21.1 | 39.7 |
| Staphylococcus Aureus (%) | 19 | 27 | 31 | 40 | 31.4 | 24.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonkoue, L.; Tissingh, E.K.; Ngouateu, M.T.; Muluem, K.O.; Ngongang, O.; Mbouyap, P.; Ngougni Pokem, P.; Fotsing, K.; Bahebeck, J.; McNally, M.; et al. The Microbiological Profile and Antibiotic Susceptibility of Fracture Related Infections in a Low Resource Setting Differ from High Resource Settings: A Cohort Study from Cameroon. Antibiotics 2024, 13, 236. https://doi.org/10.3390/antibiotics13030236
Fonkoue L, Tissingh EK, Ngouateu MT, Muluem KO, Ngongang O, Mbouyap P, Ngougni Pokem P, Fotsing K, Bahebeck J, McNally M, et al. The Microbiological Profile and Antibiotic Susceptibility of Fracture Related Infections in a Low Resource Setting Differ from High Resource Settings: A Cohort Study from Cameroon. Antibiotics. 2024; 13(3):236. https://doi.org/10.3390/antibiotics13030236
Chicago/Turabian StyleFonkoue, Loïc, Elizabeth K. Tissingh, Michelle Tognia Ngouateu, Kennedy Olivier Muluem, Olivier Ngongang, Pretty Mbouyap, Perrin Ngougni Pokem, Kuetche Fotsing, Jean Bahebeck, Martin McNally, and et al. 2024. "The Microbiological Profile and Antibiotic Susceptibility of Fracture Related Infections in a Low Resource Setting Differ from High Resource Settings: A Cohort Study from Cameroon" Antibiotics 13, no. 3: 236. https://doi.org/10.3390/antibiotics13030236
APA StyleFonkoue, L., Tissingh, E. K., Ngouateu, M. T., Muluem, K. O., Ngongang, O., Mbouyap, P., Ngougni Pokem, P., Fotsing, K., Bahebeck, J., McNally, M., & Cornu, O. (2024). The Microbiological Profile and Antibiotic Susceptibility of Fracture Related Infections in a Low Resource Setting Differ from High Resource Settings: A Cohort Study from Cameroon. Antibiotics, 13(3), 236. https://doi.org/10.3390/antibiotics13030236