Dispensing Antibiotics without a Prescription for Acute Cough Associated with Common Cold at Community Pharmacies in Shenyang, Northeastern China: A Cross-Sectional Study

 ,
,  and
and
Abstract
:1. Introduction
2. Results
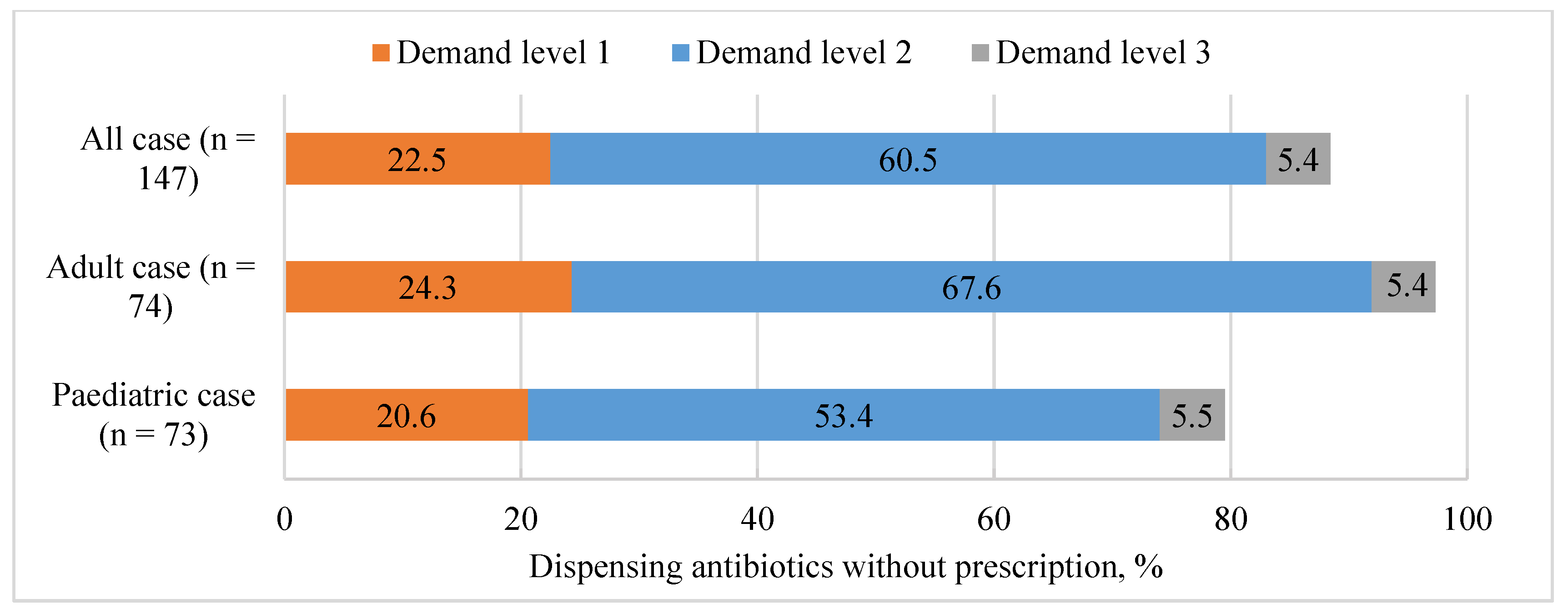
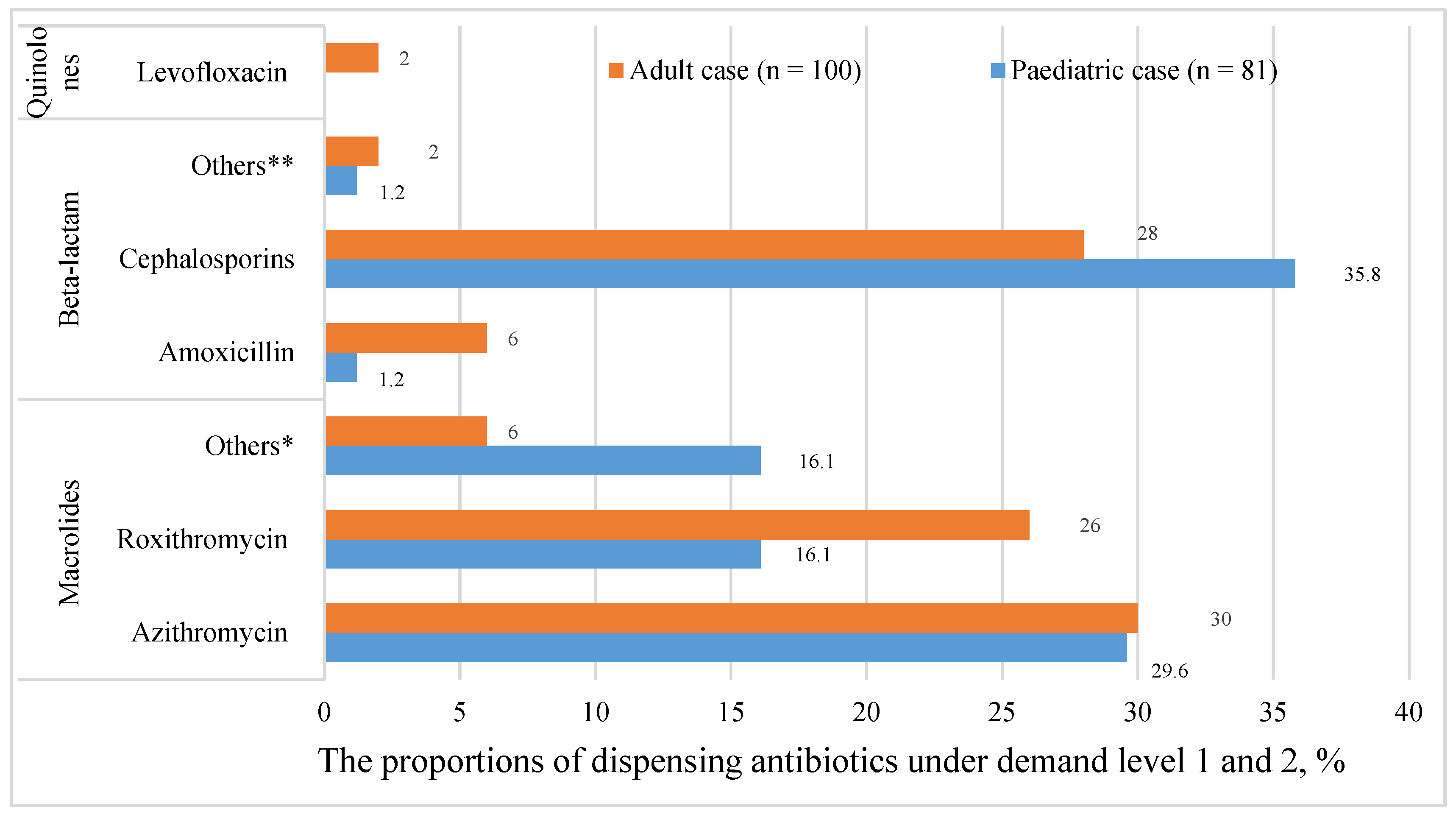
2.1. Nonprescription Antibiotic and Other Medicines Dispensing
2.1.1. Medicine Dispensing in Pediatric Acute Cough
2.1.2. Medicine Dispensing in Adult Acute Cough
2.2. Pharmacy Service Practice
2.2.1. Inquiries and Counseling
2.2.2. Other Inquired Information
3. Discussion
4. Methods
4.1. Study Setting and Pharmacy Selection
4.2. Simulated Scenarios and Standardized Client
4.3. Procedures
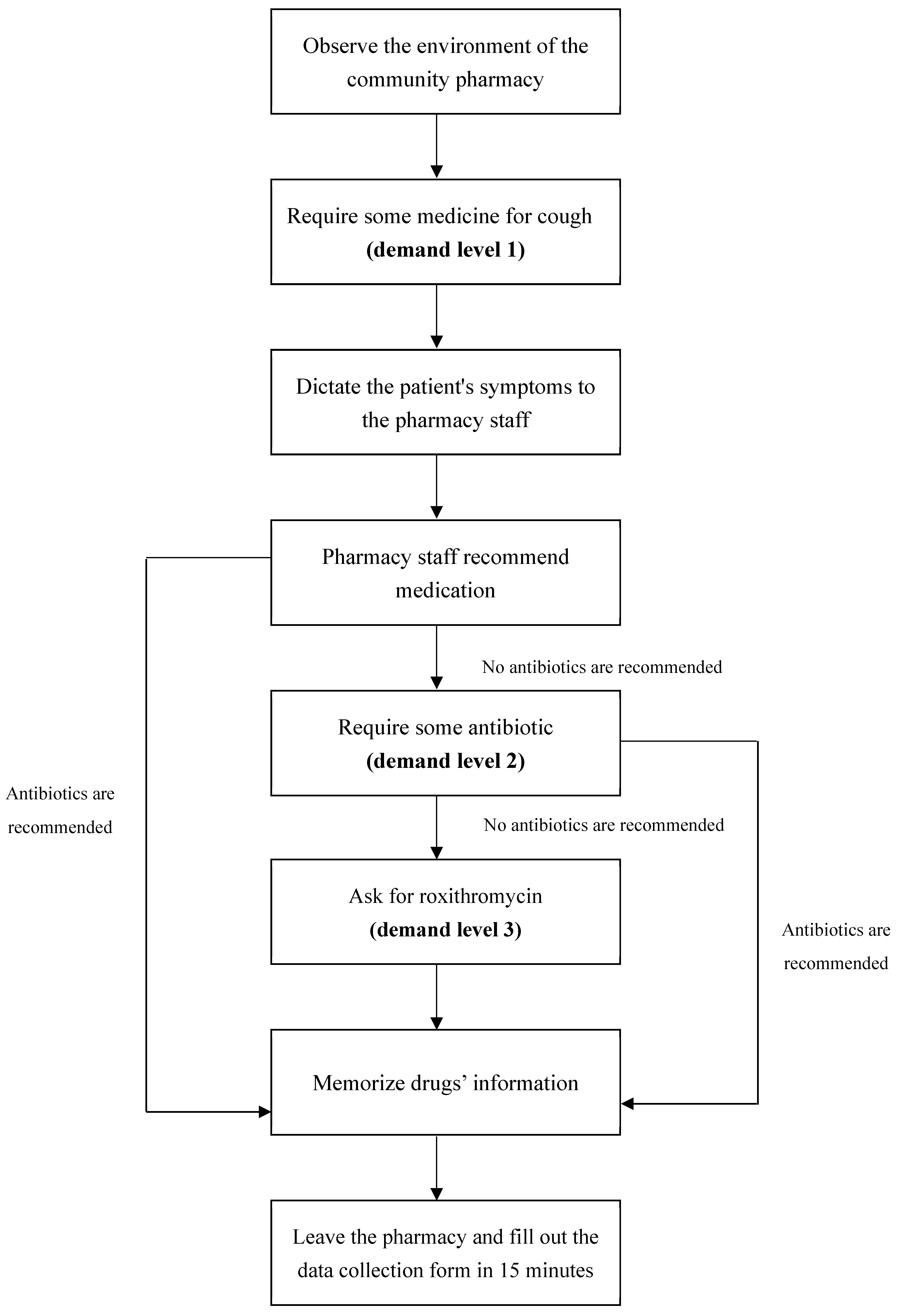
- To obtain the maximum standardization and to maintain the consistency of the simulations, the standardized visiting procedure and script of presentation Appendix A (Figure A1) were designed. Each pharmacy visit was carried out strictly according to the predefined procedure. To avoid the “Hawthorne Effect”, all community pharmacies were not informed before the visit. Given that we used the standardized client method, the committee permitted a waiver of informed consent from pharmacies. Ethics approval was obtained before the pilot study.
- Pilot visits, before field surveys, were conducted to confirm the feasibility of the study and to test the validity of the data collection form. Additionally, these visits helped in ensuring that the information collected was enough to reflect the issue we wanted to analyze.
- After pilot visits, several additional visits outside the formal sampling frame were taken for training purposes. Once the interaction with pharmacy staff in real community pharmacies was made, the simulated client built confidence and became familiar with the standardized simulated visit process.
- During the formal simulated visits in the survey, the simulated client was presented with acute cough associated with the common cold of either the pediatric or adult case in community pharmacies. Three levels of demand, (level 1: client required some medicine for cough) and (level 2: client explicitly expressed the requirement of antibiotics, and demand level 3: client specifically required roxithromycin), were designed to quantify antibiotic dispensing practices in community pharmacies. The major items to evaluate pharmacy service included inquiries about symptoms, medical history, previous treatment, allergies, and advice provision. After the visit, the standardized client found an excuse to leave without telling the pharmacy about her real identity. A standardized data collection form (Appendix B Data collection form), consisted of pharmacy demographics including location, type, and scale of pharmacy, pharmacy staff characteristics, drug dispensing practices, and planned inquiry and counseling items, was filled out within 15 minutes after leaving the pharmacy (out of sight of the pharmacy staff).
4.4. Data Analysis
4.5. Ethics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
| Case | Demand level | Macrolides | Beta-lactam | Quinolones | ||||
|---|---|---|---|---|---|---|---|---|
| Azithromycin | Roxithromycin | Others * | Amoxicillin | Cephalosporins | Others ** | Levofloxacin | ||
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | ||
| Pediatric | First | 10 (12.3) | 3 (3.7) | 5 (6.2) | / | 6 (7.4) | 1 (1.2) | / |
| Second | 14 (17.3) | 10 (12.4) | 8 (9.9) | 1 (1.2) | 23 (28.4) | / | / | |
| Total | 24 (29.6) | 13 (16.1) | 13 (16.1) | 1 (1.2) | 29 (35.8) | 1 (1.2) | 0(0.0) | |
| Adult | First | 7 (7.0) | 4 (4.0) | 2 (2.0) | 1 (1.0) | 6 (6.0) | 1 (1.0) | 2 (2.0) |
| Second | 23 (23.0) | 22 (22.0) | 4 (4.0) | 5 (5.0) | 22 (22.0) | 1 (1.0) | / | |
| Total | 30 (30.0) | 26 (26.0) | 6 (6.0) | 6 (6.0) | 28 (28.0) | 2 (2.0) | 2 (2.0) | |
| Dispensing of Antibiotics | Scenarios | Types of Drugs (n = 147, the Number of Community Pharmacies) |
|---|---|---|
| Did not dispense antibiotics | Pediatric case (n = 15) | Cough medicine (3) Anti-inflammatory Chinese patent medicine (1) Cough medicine + other1 (11) (other1: Anti-inflammatory Chinese patent medicine (8); ribavirin (1); cold medicine (1); cold medicine + vitamin C (1)) |
| Adult case (n = 2) | Cough medicine + Anti-inflammatory Chinese patent medicine (1) Anti-inflammatory Chinese patent medicine (1) | |
| Dispensed antibiotics | Pediatric case (n = 58) | Antibiotics + cough medicine (43) Antibiotics + cough medicine + other2 (15) (other2: Anti-inflammatory Chinese patent medicine (6); cold medicine (8); cold medicine + vitamin C (1)) |
| Adult case (n = 72) | Antibiotics + cough medicine (54) Antibiotic + Anti-inflammatory Chinese patent medicine (1) Antibiotics + cough medicine + other3 (17) (other3: Anti-inflammatory Chinese patent medicine (8); cold medicine (8); cold medicine + Anti-inflammatory Chinese patent medicine (1)) |
| Location | District | Population (10,000) | Proportion of Population | Sampling Size * |
|---|---|---|---|---|
| Central urban district | Heping | 65.2 | 0.12 | 18 |
| Shenhe | 71.2 | 0.13 | 20 | |
| Dadong | 68.2 | 0.14 | 19 | |
| Huanggu | 81.8 | 0.15 | 23 | |
| Teixi | 90.9 | 0.17 | 26 | |
| Total | 377.3 | 0.71 | 106 | |
| Surrounding urban district | Sujia tun | 42.7 | 0.08 | 12 |
| Hunnan | 33.4 | 0.06 | 10 | |
| Shenbei | 32 | 0.06 | 10 | |
| Yuhong | 44.6 | 0.09 | 12 | |
| Total | 152.7 | 0.29 | 44 | |
| Total | 530 | 150 | ||
Appendix B

References
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.; Wertheim, H.F.; Sumpradit, N.; Vlieghe, E.; LevyHara, G.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance—The need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Antibiotic Resistance. 2018. Available online: http://www.who.int/zh/news-room/fact-sheets/detail/antibiotic-resistance.html (accessed on 5 February 2018).
- Qiao, M.; Ying, G.G.; Singer, A.C.; Zhu, Y.G. Review of antibiotic resistance in China and its environment. Environ. Int. 2018, 110, 160–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, W.; Sun, Y.; Ding, X.; Zhang, Y.; Zhong, X.; Liang, W.; Zeng, Z. Responses of plasmid-mediated quinolone resistance genes and bacterial taxa to (fluoro) quinolones-containing manure in arable soil. Chemosphere 2015, 119, 473–478. [Google Scholar] [CrossRef] [PubMed]
- National Medical Products Administration. Notice on Strengthening the Classified Management of Prescription Drugs and Nonprescription Drugs in Circulation. 2004. Available online: http://www.nmpa.gov.cn/WS04/CL2196/323402.html (accessed on 25 May 2004).
- National medical products administration. Provisions for Supervision of Drug Distribution. 2007. Available online: http://www.nmpa.gov.cn/WS04/CL2174/300626.html (accessed on 31 January 2007).
- National medical products administration. Good Supply Practice. 2016. Available online: http://www.nmpa.gov.cn/WS04/CL2174/300691.html (accessed on 20 July 2016).
- Fang, Y. China should curb non-prescription use of antibiotics in the community. BMJ 2014, 348, g4233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, M.C.; Norris, P.; Granas, A.G. A systematic review of the use of simulated clients and pharmacy practice research. Int. J. Pharm. Pract. 2006, 14, 83–93. [Google Scholar] [CrossRef]
- Sakeena, M.H.F.; Bennett, A.A.; McLachlan, A.J. Non-prescription sales of antimicrobial agents at community pharmacies in developing countries: A systematic review. Int. J. Antimicrob. Agents 2018, 52, 771–782. [Google Scholar] [CrossRef]
- Morgan, D.J.; Okeke, I.N.; Laxminarayan, R.; Perencevich, E.N.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect. Dis. 2011, 11, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Madden, J.M.; Quick, J.D.; Ross-Degnan, D.; Kafle, K.K. Undercover careseekers: Simulated clients in the study of health provider behavior in developing countries. Soc. Sci. Med. 1997, 45, 1465–1482. [Google Scholar] [CrossRef]
- Xu, T.; de Almeida Neto, A.C.; Moles, R.J. A systematic review of simulated-patient methods used in community pharmacy to assess the provision of non-prescription medicines. Int. J. Pharm. Pract. 2012, 20, 307–319. [Google Scholar] [CrossRef]
- Chang, J.; Ye, D.; Lv, B.; Jiang, M.; Zhu, S.; Yan, K.; Tian, Y.; Fang, Y. Sale of antibiotics without a prescription at community pharmacies in urban China: A multicenter cross-sectional survey. J. Antimicrob. Chemother. 2017, 72, 1235–1242. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.; Xu, S.; Zhu, S.; Li, Z.; Yu, J.; Zhang, Y.; Zu, J.; Fang, Y.; Ross-Degnan, D. Assessment of non-prescription antibiotic dispensing at community pharmacies in China with simulated clients: A mixed cross-sectional and longitudinal study. Lancet Infect. Dis. 2019, 19, 1345–1354. [Google Scholar] [CrossRef]
- The State Council. Reply of the State Council on the Overall Urban Planning of Shenyang. 2017. Available online: http://www.gov.cn/zhengce/content/2017-07/14/content_5210472.htm (accessed on 14 July 2017).
- Klassen, T.P.; Hartling, L.; Craig, J.C.; Offringa, M. Children are not just small adults: The urgent need for high-quality trial evidence in children. PLoS Med. 2008, 5, 1180–1182. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’s Republic of China. Guiding Principles of Clinical Use of Antibiotic. 2015. Available online: http://www.nhc.gov.cn/ewebeditor/uploadfile/2015/09/20150928170007470.pdf (accessed on 27 August 2015).
- ShengYang Municipal Bureau of statistics. Statistical Yearbook of Shenyang in 2016. 2017. Available online: http://tjj.shenyang.gov.cn/html/SYTJJ/15620336218981/15620336218981/15620336218981/3621898123676350.html (accessed on 10 December 2017).
- Bi, P.; Tong, S.; Parton, K.A. Family self-medication and antibiotics abuse for children and juveniles in a Chinese city. Soc. Sci. Med. 2000, 50, 1445–1450. [Google Scholar] [CrossRef]
- Jiang, M.; Xie, Y.Q.; Xie, J.X.; Zou, X.W.; Lai, K.F. Methodology for development of the Chinese evidence-based Clinical Practice Guideline of the Diagnosis and Management of Cough. J. Thorac. Dis. 2018, 10, 6310–6313. [Google Scholar] [CrossRef]
- National institute for health and care excellence. Cough (acute): Antimicrobial prescribing. 2019. Available online: https://www.nice.org.uk/guidance/ng120.htm (accessed on 20 February 2019).
- Rhee, C.K.; Jung, J.Y.; Lee, S.W.; Kim, J.H.; Park, S.Y.; Yoo, K.H.; Park, D.A.; Koo, H.-K.; Kim, Y.H.; Jeong, I.; et al. The Korean cough guideline: Recommendation and summary statement. Tuberc. Resipir. Dis. 2016, 79, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Malesker, M.A.; Callahan-Lyon, P.; Ireland, B.; Irwin, R.S.; Adams, T.M.; Altman, K.W.; Azoulay, E.; Barker, A.F.; Birring, S.S.; Blackhall, F.; et al. Pharmacologic and Nonpharmacologic Treatment for Acute Cough Associated With the Common Cold: CHEST Expert Panel Report. Chest 2017, 152, 1021–1037. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Fahey, T.; Smucny, J.; Becker, L.A. Antibiotics for acute bronchitis. Cochrane Database Syst Rev 2017, 6, CD000245. [Google Scholar] [CrossRef]
- Alhomoud, F.; Aljamea, Z.; Almahasnah, R.; Alkhalifah, K.; Basalelah, L.; Alhomoud, F.K. Self-medication and self-prescription with antibiotics in the Middle East-do they really happen? A systematic review of the prevalence, possible reasons, and outcomes. Int. J. Infect. Dis. 2017, 57, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Auta, A.; Hadi, M.A.; Oga, E.; Adewuyi, E.O.; Abdu-Aguye, S.N.; Adeloye, D.; Strickland-Hodge, B.; Morgan, D.J. Global access to antibiotics without prescription in community pharmacies: A systematic review and meta-analysis. J. Infect. 2019, 78, 8–18. [Google Scholar] [CrossRef]
- Contopoulos-Ioannidis, D.G.; Koliofoti, I.D.; Koutroumpa, I.C.; Giannakakis, I.A.; Ioannidis, J.P. Pathways for inappropriate dispensing of antibiotics for rhinosinusitis: A randomized trial. Clin. Infect. Dis. 2001, 33, 76–82. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey. 2015. Available online: http://apps.who.int/iris/bitstream/10665/194460/1/ 9789241509817_eng.pdf (accessed on 15 February 2019).
- Jin, G.; Chen, C.; Liu, Y.; Zhao, Y.; Chen, L.; Du, J.; Lu, X.; Chen, J. Prescribing patterns of encounters in fourteen general practice clinics in rural Beijing: A cross-sectional study. BMC Health Serv. Res. 2019, 19, 807. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Zhang, Z.; Walley, J.D.; Hicks, J.P.; Zeng, J.; Deng, S.; Zhou, Y.; Yin, J.; Newell, J.N.; Sun, Q.; et al. Effect of a training and educational intervention for physicians and caregivers on antibiotic prescribing for upper respiratory tract infections in children at primary care facilities in rural China: A cluster-randomised controlled trial. Lancet Glob. Health 2017, 5, e1258–e1267. [Google Scholar] [CrossRef] [Green Version]
- Zapata-Cachafeiro, M.; Piñeiro-Lamas, M.; Guinovart, M.C.; López-Vázquez, P.; Vázquez-Lago, J.M.; Figueiras, A. Magnitude and determinants of antibiotic dispensing without prescription in Spain: A simulated patient study. J. Antimicrob. Chemother. 2019, 74, 511–514. [Google Scholar] [CrossRef] [PubMed]
- Lv, B.; Zhou, Z.; Xu, G.; Yang, D.; Wu, L.; Shen, Q.; Jiang, M.; Wang, X.; Zhao, G.; Yang, S. Knowledge, attitudes and practices concerning self-medication with antibiotics among university students in western China. Trop Med. Int. Health. 2014, 19, 769–779. [Google Scholar] [CrossRef]
- Li, R.; Xiao, F.; Zheng, X.; Yang, H.; Wang, L.; Yin, D.; Yin, T.; Xin, Q.; Chen, B. Antibiotic misuse among children with diarrhea in China: Results from a national survey. Peer J. 2016, 4, e2668. [Google Scholar] [CrossRef]
- Satyanarayana, S.; Kwan, A.; Daniels, B.; Subbaraman, R.; McDowell, A.; Bergkvist, S.; Das, R.K.; Das, V.; Das, J.; Pai, M. Use of standardised patients to assess antibiotic dispensing for tuberculosis by pharmacies in urban India: A cross-sectional study. Lancet Infect. Dis. 2016, 16, 1261–1268. [Google Scholar] [CrossRef] [Green Version]
- Formoso, G.; Paltrinieri, B.; Marata, A.M.; Gagliotti, C.; Pan, A.; Moro, M.L.; Capelli, O.; Magrini, N. Feasibility and effectiveness of a low cost campaign on antibiotic prescribing in Italy: Community level, controlled, non-randomised trial. BMJ. 2013, 347, f5391. [Google Scholar] [CrossRef] [Green Version]
- Wiysonge, C.S.; Abdullahi, L.H.; Ndze, V.N.; Hussey, G.D. Public stewardship of private for-profit healthcare providers in low- and middle-income countries. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]


| Variables | Total Number | Nonprescription Antibiotic Dispensing | Multiple Logistic Regression | |||
|---|---|---|---|---|---|---|
| n(%) | Yes, n(%) | No n(%) | OR | 95%CI | p-Value | |
| Case | ||||||
| Adult case | 74(50.3) | 72(97.3) | 2(2.7) | ref | ||
| Pediatric case | 73(49.7) | 58(79.5) | 15(20.5) | 0.099 | 0.020–0.505 | 0.005 |
| Pharmacy characteristics | ||||||
| Socioeconomic1 | ||||||
| Low socioeconomic level | 96(65.3) | 85(88.3) | 11(11.7) | ref | ||
| High socioeconomic level | 51(34.7) | 45(88.2) | 6(11.8) | 0.814 | 0.225–2.943 | 0.753 |
| Type | ||||||
| Independent | 18(12.2) | 18(100) | 0(0) | ref | ||
| Chain | 129(87.8) | 112(86.8) | 17(13.2) | 0.000 | 0.000– | 0.998 |
| Area | ||||||
| Suburb district | 43(39.3) | 40(93.0) | 3(7.0) | ref | ||
| Urban district | 104(60.7) | 90(86.5) | 14(13.5) | 0.892 | 0.204–3.914 | 0.881 |
| Distribution | ||||||
| Community center | 112(76.2) | 103(91.9) | 9(8.1) | ref | ||
| Medical center | 17(11.6) | 13(76.4) | 4(23.6) | 0.317 | 0.069–1.463 | 0.141 |
| Shopping center | 18(12.2) | 14(77.8) | 4(22.2) | 0.370 | 0.078–1.765 | 0.212 |
| Size2 | ||||||
| Small (<100 m2) | 68(46.3) | 60(88.2) | 8(11.8) | ref | ||
| Medium (100–300 m2) | 70(47.6) | 61(87.1) | 9(13.9) | 1.479 | 0.446–4.906 | 0.522 |
| Larger (≥300 m2) | 9(6.1) | 9(100) | 0(0) | 1.841E8 | 0.000– | 0.999 |
| Staff characteristics | ||||||
| Gender | ||||||
| Female | 144(97.9) | 127(88.2) | 17(11.8) | ref | ||
| Male | 3(2.1) | 3(100) | 0(0) | 8.938E8 | 0.000– | 0.999 |
| Ages (years) | ||||||
| >50 | 6(4.1) | 5(83.3) | 1(16.7) | ref | ||
| 30–50 | 96(65.3) | 86(89.6) | 10(10.4) | 10.613 | 0.313–359.761 | 0.189 |
| ≤30 | 45(30.6) | 39(86.7) | 6(13.3) | 16.852 | 0.439–647.711 | 0.129 |
| Question Items | All Cases (n = 147) | Pediatric Case (n = 73) | Adult Case (n = 74) | χ2 | p-Value |
|---|---|---|---|---|---|
| n (%) | |||||
| Inquiries about the symptom | 121 (82.3) | 60 (82.2) | 61 (82.4) | 0.021 | 0.885 |
| Asked about the length of cough | 24 (16.3) | 13 (17.8) | 11 (14.9) | ||
| Asked about cough duration | 1 (0.7) | 0 (0.0) | 1 (1.3) | ||
| Asked about whether had sputum or not | 113 (76.9) | 54 (74.0) | 59 (79.7) | ||
| Asked about the color of sputum | 15 (10.2) | 5 (6.9) | 10 (13.5) | ||
| Asked about other accompanying symptoms (sore throat, runny nose) | 49 (33.3) | 27 (37.0) | 22 (29.7) | ||
| Other question (asking the cause or severity of cough) | 32 (21.8) | 17 (23.3) | 15 (20.3) | ||
| Other question (asking about specific symptoms) | 14 (9.5) | 4 (5.5) | 10 (13.5) | ||
| Inquiries about previous treatment(s) | 24 (16.3) | 16 (21.9) | 8 (10.8) | 3.319 | 0.069 |
| Asked whether had taken any other medicine or not | 22 (15.0) | 14 (19.2) | 8 (10.8) | ||
| Asked whether had seen a doctor or not | 2 (2.7) | 2 (2.7) | 0 (0.0) | ||
| Inquiries about drug allergy and medical history | 57 (38.8) | 31 (42.5) | 26 (35.1) | 0.832 | 0.362 |
| Asked history of drug allergy | 52 (35.4) | 29 (39.7) | 23 (31.1) | ||
| Asked other medical history | 5 (3.4) | 2 (2.7) | 3 (4.0) | ||
| Medication advice and other recommendations * | 56 (38.1) | 21 (28.8) | 35 (47.3) | 5.039 | 0.025 |
| Introduced the usage of the dispensed medicines | 46 (31.3) | 16 (21.9) | 30 (40.5) | ||
| Introduced the side effects of the dispensed medicines | 5 (3.4) | 2 (2.7) | 3 (4.0) | ||
| Others (advice on diet or other lifestyle factors) | 6 (4.1) | 1 (1.4) | 5 (6.8) | ||
| Recommended a referral to healthcare facilities | 4 (2.7) | 4 (5.5) | 0 (0.0) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, L.; Chang, J.; Liu, X.; Zhai, P.; Hu, S.; Li, P.; Hayat, K.; Kabba, J.A.; Feng, Z.; Yang, C.; et al. Dispensing Antibiotics without a Prescription for Acute Cough Associated with Common Cold at Community Pharmacies in Shenyang, Northeastern China: A Cross-Sectional Study. Antibiotics 2020, 9, 163. https://doi.org/10.3390/antibiotics9040163
Shi L, Chang J, Liu X, Zhai P, Hu S, Li P, Hayat K, Kabba JA, Feng Z, Yang C, et al. Dispensing Antibiotics without a Prescription for Acute Cough Associated with Common Cold at Community Pharmacies in Shenyang, Northeastern China: A Cross-Sectional Study. Antibiotics. 2020; 9(4):163. https://doi.org/10.3390/antibiotics9040163
Chicago/Turabian StyleShi, Li, Jie Chang, Xiaoxi Liu, Panpan Zhai, Shuchen Hu, Pengchao Li, Khezar Hayat, John Alimamy Kabba, Zhitong Feng, Caijun Yang, and et al. 2020. "Dispensing Antibiotics without a Prescription for Acute Cough Associated with Common Cold at Community Pharmacies in Shenyang, Northeastern China: A Cross-Sectional Study" Antibiotics 9, no. 4: 163. https://doi.org/10.3390/antibiotics9040163
APA StyleShi, L., Chang, J., Liu, X., Zhai, P., Hu, S., Li, P., Hayat, K., Kabba, J. A., Feng, Z., Yang, C., Jiang, M., Zhao, M., Hu, H., & Fang, Y. (2020). Dispensing Antibiotics without a Prescription for Acute Cough Associated with Common Cold at Community Pharmacies in Shenyang, Northeastern China: A Cross-Sectional Study. Antibiotics, 9(4), 163. https://doi.org/10.3390/antibiotics9040163