The Effectiveness of Chlorhexidine and Air Polishing System in the Treatment of Candida albicans Infected Dental Implants: An Experimental In Vitro Study


 ,
,  ,
, 
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. In Vitro Biofilm Formation
4.2. Implant Surface Decontamination
- Group 1: one machined and one rough implant treated with chlorhexidine 0.2% (Curasept ADS 0.2%, Curaden HealthCare Spa, Saronno, Italy) for 30 s.
- Group 2: one machined and one rough implant first treated with air polishing with sodium bicarbonate powder and then immersed in chlorhexidine 0.2% for 30 s.
- Group 3: one machined and one rough implant treated with chlorhexidine 0.2% for 1 min.
- Group 4: one machined and one rough implant first treated with air polishing with sodium bicarbonate powder and then immersed in chlorhexidine 0.2% for 1 min.
- Group 5: one machined and one rough implant treated with chlorhexidine 0.2% for 5 min.
- Group 6: one machined and one rough implant first treated with air polishing with sodium bicarbonate powder and then immersed in chlorhexidine 0.2% for 5 min.
4.3. Quantification of Biofilms
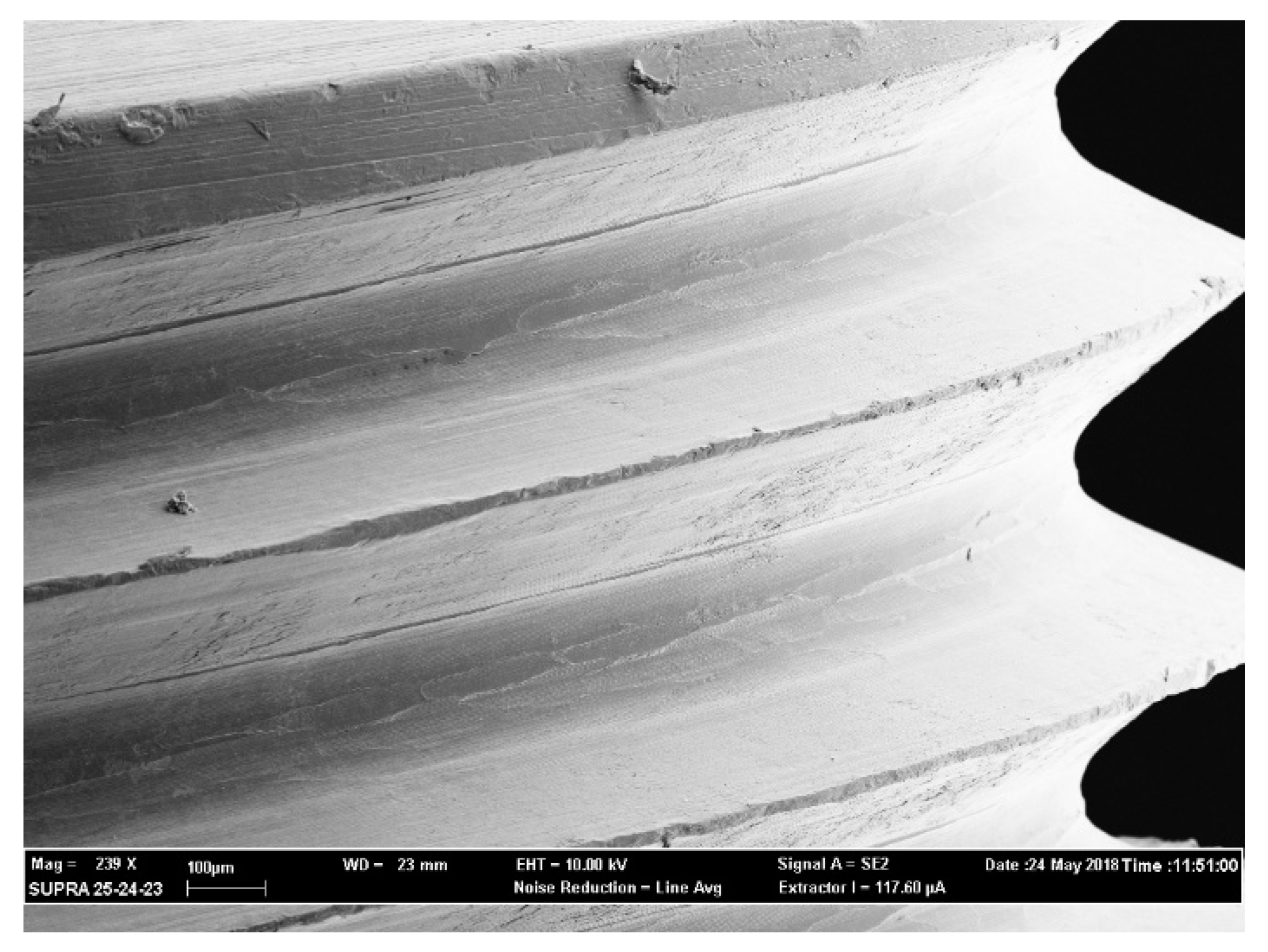
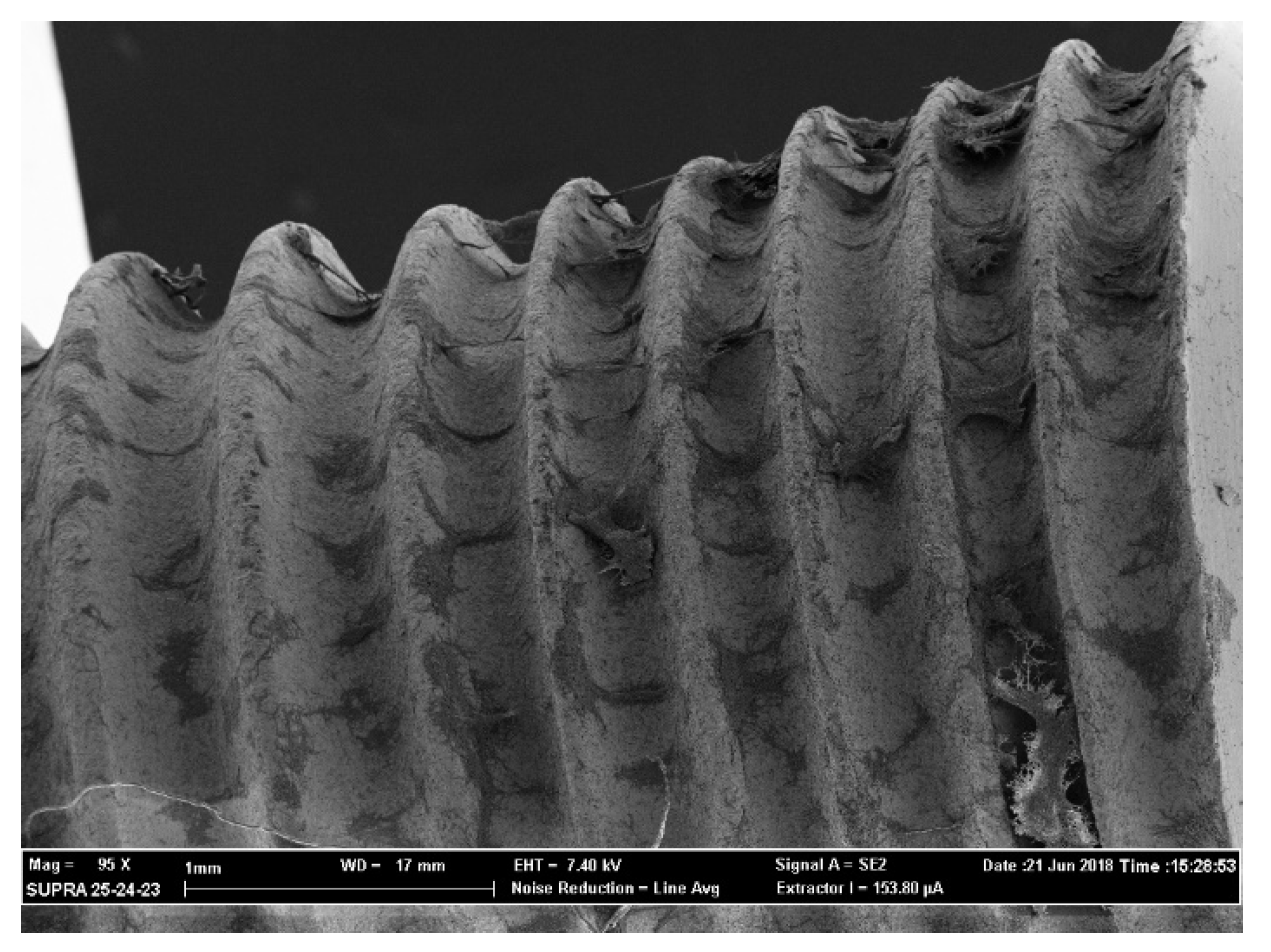
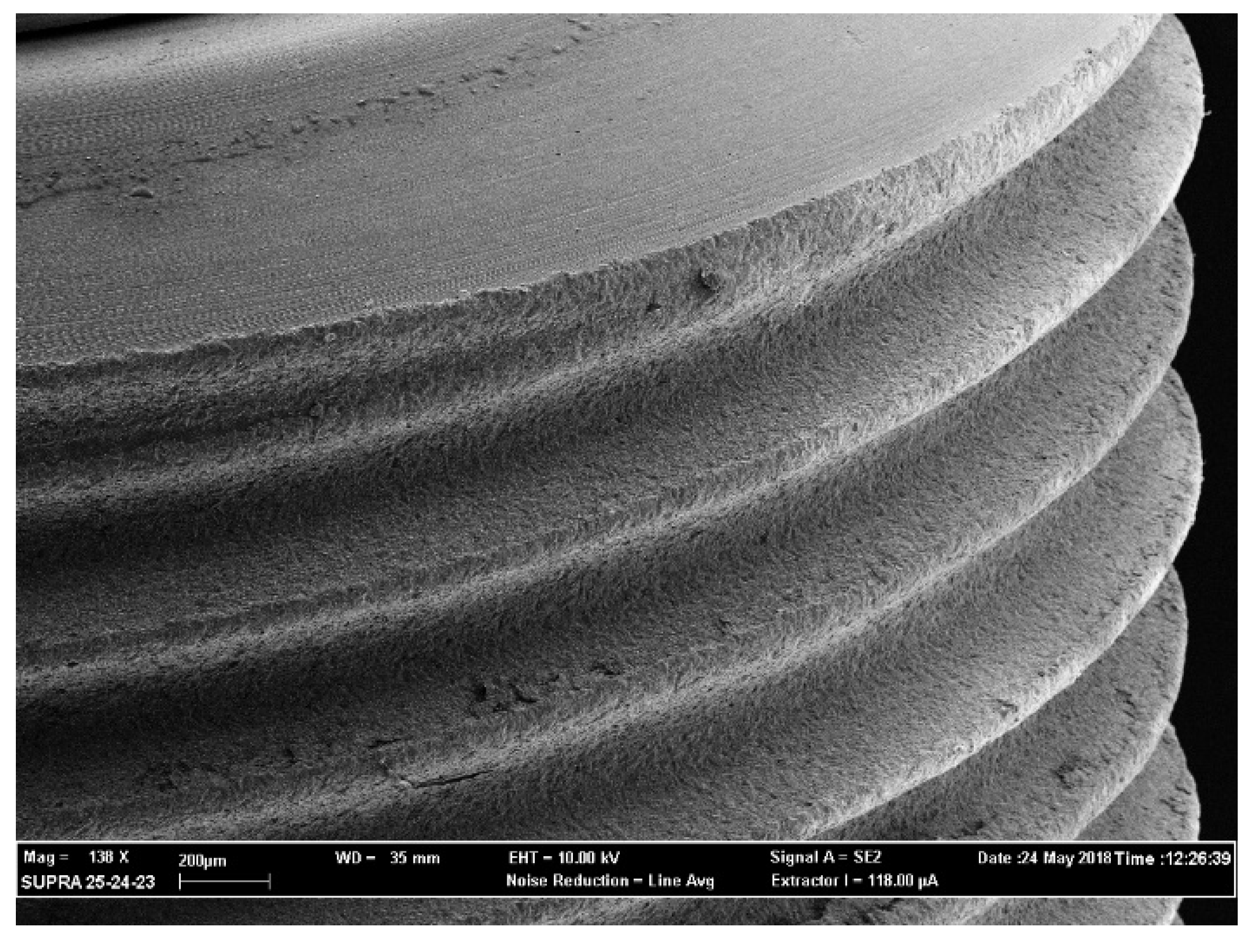
4.4. SEM Observation
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- De Angelis, P.; Passarelli, P.C.; Gasparini, G.; Boniello, R.; D’Amato, G.; De Angelis, S. Monolithic CAD-CAM lithium disilicate versus monolithic CAD-CAM zirconia for single implant-supported posterior crowns using a digital workflow: A 3-year cross-sectional retrospective study. J. Prosthet. Dent. 2020, 123, 252–256. [Google Scholar] [CrossRef]
- Manicone, P.F.; Passarelli, P.C.; Bigagnoli, S.; Pastorino, R.; Manni, A.; Pasquantonio, G.; D’Addona, A. Clinical and radiographic assessment of implant-supported rehabilitation of partial and complete edentulism: A 2 to 8 years clinical follow-up. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 4045–4052. [Google Scholar] [CrossRef]
- Vinci, R.; Tetè, G.; Lucchetti, F.R.; Capparé, P.; Gherlone, E.F. Implant survival rate in calvarial bone grafts: A retrospective clinical study with 10 year follow-up. Clin. Implant. Dent. Relat. Res. 2019, 21, 662–668. [Google Scholar] [CrossRef]
- Esposito, M.; Hirsch, J.-M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- Azzolino, D.; Passarelli, P.C.; De Angelis, P.; Piccirillo, G.B.; D’Addona, A.; Cesari, M. Poor Oral Health as a Determinant of Malnutrition and Sarcopenia. Nutrients 2019, 11, 2898. [Google Scholar] [CrossRef] [Green Version]
- Passarelli, P.C.; Pasquantonio, G.; Manicone, P.F.; Cerroni, L.; Condo, R.; Mancini, M.; D’Addona, A. Orofacial signs and dental abnormalities in patients with Mulvihill-Smith syndrome: A literature review on this rare progeroid pathology. Medicine 2018, 97, e0656. [Google Scholar] [CrossRef]
- Bollero, P.; Passarelli, P.C.; D’Addona, A.; Pasquantonio, G.; Mancini, M.; Condò, R. Oral management of adult patients undergoing hematopoietic stem cell transplantation. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 876–887. [Google Scholar] [CrossRef]
- Passarelli, P.C.; De Angelis, P.; Pasquantonio, G.; Manicone, P.F.; Verdugo, F.; D’Addona, A. Management of Single Uncomplicated Dental Extractions and Postoperative Bleeding Evaluation in Patients with Factor V Deficiency: A Local Antihemorrhagic Approach. J. Oral Maxillofac. Surg. 2018, 76, 2280–2283. [Google Scholar] [CrossRef]
- Passarelli, P.C.; Pasquantonio, G.; D’Addona, A. Management of Surgical Third Lower Molar Extraction and Postoperative Progress in Patients with Factor VII Deficiency: A Clinical Protocol and Focus on This Rare Pathologic Entity. J. Oral Maxillofac. Surg. 2017, 75, 2070.e1–2070.e4. [Google Scholar] [CrossRef]
- De Angelis, P.; De Angelis, S.; Passarelli, P.C.; Liguori, M.G.; Manicone, P.F.; D’Addona, A. Hard and Soft Tissue Evaluation of Different Socket Preservation Procedures Using Leukocyte and Platelet-Rich Fibrin: A Retrospective Clinical and Volumetric Analysis. J. Oral Maxillofac. Surg. 2019, 77, 1807–1815. [Google Scholar] [CrossRef]
- Moro, A.; De Angelis, P.; Pelo, S.; Gasparini, G.; D’Amato, G.; Passarelli, P.C.; Saponaro, G. Alveolar ridge augmentation with maxillary sinus elevation and split crest: Comparison of 2 surgical procedures. Medicine 2018, 97, e11029. [Google Scholar] [CrossRef] [PubMed]
- Saccomanno, S.; Passarelli, P.C.; Oliva, B.; Grippaudo, C. Comparison between Two Radiological Methods for Assessment of Tooth Root Resorption: An In Vitro Study. BioMed Res. Int. 2018, 2018, 5152172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stacchi, C.; Spinato, S.; Lombardi, T.; Bernardello, F.; Bertoldi, C.; Zaffe, D.; Nevins, M. Minimally Invasive Management of Implant-Supported Rehabilitation in the Posterior Maxilla, Part I. Sinus Floor Elevation: Biologic Principles and Materials. Int. J. Periodontics Restor. Dent. 2020, 40, e85–e93. [Google Scholar] [CrossRef]
- Stacchi, C.; Spinato, S.; Lombardi, T.; Bernardello, F.; Bertoldi, C.; Zaffe, D.; Nevins, M. Minimally Invasive Management of Implant-Supported Rehabilitation in the Posterior Maxilla, Part II. Surgical Techniques and Decision Tree. Int. J. Periodontics Restor. Dent. 2020, 40, e95–e102. [Google Scholar] [CrossRef]
- Esposito, M.; Hirsch, J.-M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis. Eur. J. Oral Sci. 1998, 106, 721–764. [Google Scholar] [CrossRef]
- Lindhe, J.; Meyle, J. On behalf of Group D of the European Workshop on Periodontology Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [Green Version]
- Roos-Jansåker, A.-M.; Renvert, S.; Egelberg, J. Treatment of peri-implant infections: A literature review. J. Clin. Periodontol. 2003, 30, 467–485. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Lang, N.P. Comparative biology of chronic and aggressive periodontitis vs. peri-implantitis. Periodontology 2010, 53, 167–181. [Google Scholar] [CrossRef]
- Martellacci, L.; Quaranta, G.; Patini, R.; Isola, G.; Gallenzi, P.; Masucci, L. A Literature Review of Metagenomics and Culturomics of the Peri-implant Microbiome: Current Evidence and Future Perspectives. Materials 2019, 12, 3010. [Google Scholar] [CrossRef] [Green Version]
- Leonhardt, A.; Bergström, C.; Lekholm, U. Microbiologic diagnostics at titanium implants. Clin. Implant. Dent. Relat. Res. 2003, 5, 226–232. [Google Scholar] [CrossRef]
- Albertini, M.; López-Cerero, L.; O’Sullivan, M.G.; Chereguini, C.F.; Ballesta, S.; Ríos-Santos, J.V.; Herrero-Climent, M.; Bullón, P. Assessment of periodontal and opportunistic flora in patients with peri-implantitis. Clin. Oral Implant. Res. 2014, 26, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Bürgers, R.; Hahnel, S.; Reichert, T.E.; Rosentritt, M.; Behr, M.; Gerlach, T.; Handel, G.; Gosau, M. Adhesion of Candida albicans to various dental implant surfaces and the influence of salivary pellicle proteins. Acta Biomater. 2010, 6, 2307–2313. [Google Scholar] [CrossRef] [PubMed]
- Dahlén, G.; Wikström, M. Occurrence of enteric rods, staphylococci and Candida in subgingival samples. Oral Microbiol. Immunol. 1995, 10, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-L. Virulence factors of Candida species. J. Microbiol. Immunol. Infect. 2003, 36, 223–228. [Google Scholar]
- O’Sullivan, J.M.; Jenkinson, H.F.; Cannon, R.D. Adhesion of Candida albicans to oral streptococci is promoted by selective adsorption of salivary proteins to the streptococcal cell surface. Microbiology 2000, 146, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Harriott, M.M.; Noverr, M.C. Importance of Candida–bacterial polymicrobial biofilms in disease. Trends Microbiol. 2011, 19, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Cavalcanti, Y.W.; Wilson, M.; Lewis, M.; Cury, A.D.B.; Da Silva, W.J.; Williams, D.W. Modulation of Candida albicans virulence by bacterial biofilms on titanium surfaces. Biofouling 2016, 32, 123–134. [Google Scholar] [CrossRef]
- Järvensivu, A.; Hietanen, J.; Rautemaa, R.; Sorsa, T.; Rautemaa, R. Candida yeasts in chronic periodontitis tissues and subgingival microbial biofilms in vivo. Oral Dis. 2004, 10, 106–112. [Google Scholar] [CrossRef]
- Quirynen, M.; Bollen, C.M.L. The influence of surface roughness and surface-free energy on supra- and subgingival plaque formation in man: A review of the literature. J. Clin. Periodontol. 2005, 22, 1–14. [Google Scholar] [CrossRef]
- Subramani, K.; Jung, R.E.; Molenberg, A.; Hämmerle, C.H.F. Biofilm on dental implants: A review of the literature. Int. J. Oral Maxillofac. Implant. 2009, 24, 616–626. [Google Scholar]
- Claffey, N.; Clarke, E.; Polyzois, I.; Renvert, S. Surgical treatment of peri-implantitis. J. Clin. Periodontol. 2008, 35, 316–332. [Google Scholar] [CrossRef] [PubMed]
- Suarez, F.; Monje, A.; Galindo-Moreno, P.; Wang, H.L. Implant surface detoxification: A comprehensive review. Implant. Dent. 2013, 22, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Isola, G. Antibiotics and Antimicrobials for Treatment of the Oral Microbiota: Myths and Facts in Research and Clinical Practice. Antibiotics 2020, 9, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mombelli, A.; Lang, N.P. Antimicrobial treatment of peri-implant infections. Clin. Oral Implant. Res. 1992, 3, 162–168. [Google Scholar] [CrossRef]
- Renvert, S.; Claffey, N.; Roos-Jansåker, A.-M. Non-surgical treatment of peri-implant mucositis and peri-implantitis: A literature review. J. Clin. Periodontol. 2008, 35, 305–315. [Google Scholar] [CrossRef]
- Schwarz, F.; Becker, K.; Renvert, S. Efficacy of air polishing for the non-surgical treatment of peri-implant diseases: A systematic review. J. Clin. Periodontol. 2015, 42, 951–959. [Google Scholar] [CrossRef]
- Ramage, G.; Martãnez, J.P.; Lopez-Ribot, J.L.; Martínez, J.P.; López-Ribot, J.L. Candida biofilms on implanted biomaterials: A clinically significant problem. FEMS Yeast Res. 2006, 6, 979–986. [Google Scholar] [CrossRef] [Green Version]
- Tsang, C.S.P.; Ng, H.; McMillan, A.S.; Tsang, C.S.P. Antifungal susceptibility of Candida albicans biofilms on titanium discs with different surface roughness. Clin. Oral Investig. 2007, 11, 361–368. [Google Scholar] [CrossRef]
- Isola, G.; Polizzi, A.; Alibrandi, A.; Indelicato, F.; Ferlito, S. Analysis of Endothelin-1 Concentrations in Individuals with Periodontitis. Sci. Rep. 2020, 10, 1652. [Google Scholar] [CrossRef]
- Bürgers, R.; Gerlach, T.; Hahnel, S.; Schwarz, F.; Handel, G.; Gosau, M. In vivo and in vitro biofilm formation on two different titanium implant surfaces. Clin. Oral Implant. Res. 2010, 21, 156–164. [Google Scholar] [CrossRef]
- Gosau, M.; Hahnel, S.; Schwarz, F.; Gerlach, T.; Reichert, T.E.; Bürgers, R. Effect of six different peri-implantitis disinfection methods on in vivo human oral biofilm. Clin. Oral Implant. Res. 2010, 21, 866–872. [Google Scholar] [CrossRef]
- Fathilah, A.; Himratul-Aznita, W.; Fatheen, A.; Suriani, K. The antifungal properties of chlorhexidine digluconate and cetylpyrinidinium chloride on oral Candida. J. Dent. 2012, 40, 609–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rismanchian, M.; Nosouhian, S.; Shahabouee, M.; Davoudi, A.; Nourbakhshian, F. Effect of conventional and contemporary disinfectant techniques on three peri-implantitis associated microbiotas. Am. J. Dent. 2017, 30, 23–26. [Google Scholar] [PubMed]
- Suci, P.; Tyler, B.J. Action of Chlorhexidine Digluconate against Yeast and Filamentous Forms in an Early-Stage Candida albicans Biofilm. Antimicrob. Agents Chemother. 2002, 46, 3522–3531. [Google Scholar] [CrossRef] [Green Version]
- Zablotsky, M.H.; Diedrich, D.L.; Meffert, R.M. Detoxification of endotoxin-contaminated titanium and hydroxyapatite-coated surfaces utilizing various chemotherapeutic and mechanical modalities. Implant. Dent. 1992, 1, 154–158. [Google Scholar] [CrossRef]
- Dennison, D.K.; Huerzeler, M.B.; Quinones, C.; Caffesse, R.G. Contaminated implant surfaces: An in vitro comparison of implant surface coating and treatment modalities for decontamination. J. Periodontol. 1994, 65, 942–948. [Google Scholar] [CrossRef]
- Ziebolz, D.; Klipp, S.; Schmalz, G.; Schmickler, J.; Rinke, S.; Kottmann, T.; Fresmann, S.; Einwag, J. Comparison of different maintenance strategies within supportive implant therapy for prevention of peri-implant inflammation during the first year after implant restoration. A randomized, dental hygiene practice-based multicenter study. Am. J. Dent. 2017, 30, 190–196. [Google Scholar]
- Chandra, J.; Kuhn, D.M.; Mukherjee, P.K.; Hoyer, L.L.; McCormick, T.; Ghannoum, M.A. Biofilm formation by the fungal pathogen Candida albicans: Development, architecture, and drug resistance. J. Bacteriol. 2001, 183, 5385–5394. [Google Scholar] [CrossRef] [Green Version]
- Chandra, J.; Mukherjee, P.K.; Ghannoum, M.A. In vitro growth and analysis of Candida biofilms. Nat. Protoc. 2008, 3, 1909–1924. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
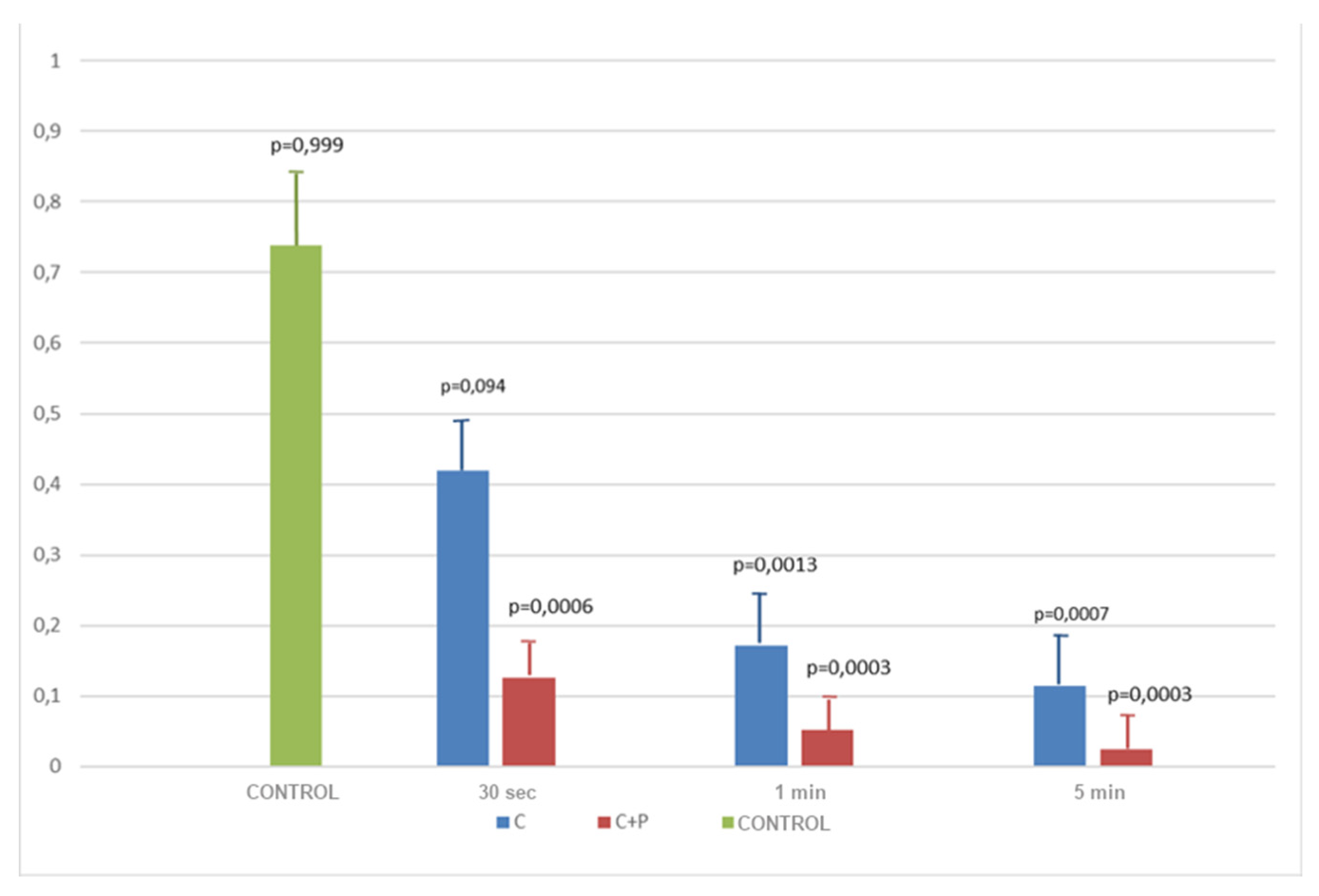
| Machined Implants | Treatment | Timing | Optical Density | Mean | SD | p-Value | ||
| CHX | 30 s | 0.407 | 0.419 | 0.045 | 0.419 | 0.045 | 0.0094 | |
| CHX | 1 min | 0.088 | 0.171 | 0.051 | 0.171 | 0.051 | 0.0013 | |
| CHX | 5 min | 0.124 | 0.113 | 0.041 | 0.113 | 0.041 | 0.0007 | |
| C + P | 30 s | 0.103 | 0.126 | 0.016 | 0.126 | 0.016 | 0.0006 | |
| C + P | 1 min | 0.043 | 0.052 | 0.011 | 0.051 | 0.011 | 0.0003 | |
| C + P | 5 min | 0.017 | 0.024 | 0.014 | 0.023 | 0.014 | 0.0003 | |
| Control | - | 0.826 | 0.738 | 0.084 | 0.738 | 0.084 | 0.999 | |
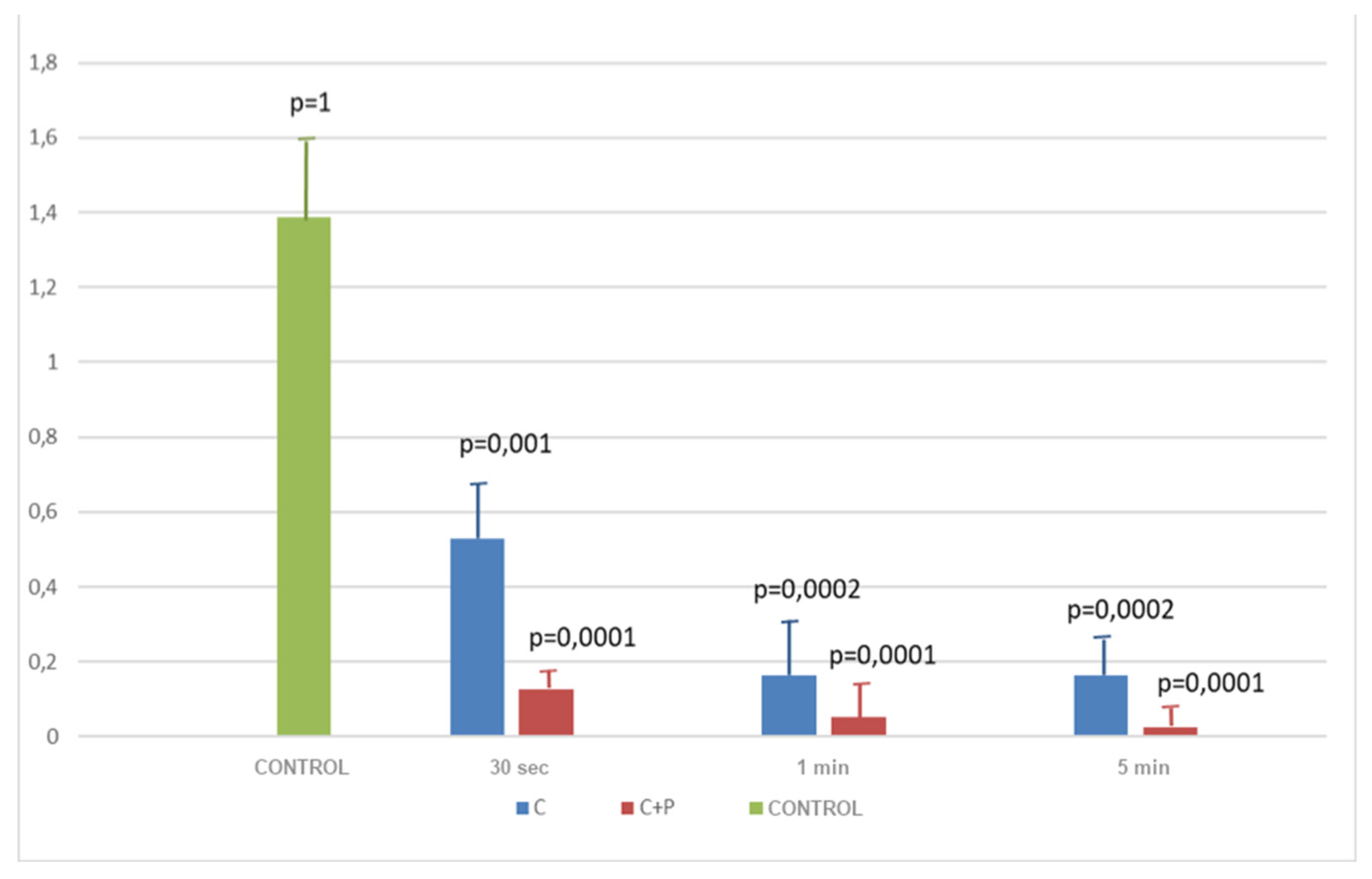
| Rough Implants | CHX | 30 s | 0.543 | 0.471 | 0.573 | 0.529 | 0.043 | 0.001 |
| CHX | 1 min | 0.205 | 0.17 | 0.144 | 0.163 | 0.037 | 0.0002 | |
| CHX | 5 min | 0.188 | 0.158 | 0.142 | 0.162 | 0.019 | 0.0002 | |
| C + P | 30 s | 0.045 | 0.041 | 0.043 | 0.042 | 0.001 | 0.0001 | |
| C + P | 1 min | 0.035 | 0.014 | 0.018 | 0.043 | 0.012 | 0.0001 | |
| C + P | 5 min | 0.035 | 0.059 | 0.033 | 0.022 | 0.009 | 0.0001 | |
| Control | - | 1.563 | 1.356 | 1.239 | 1.386 | 0.133 | 1 | |
| BLK | - | - | 0 | −0.001 | 0.002 | - | - | - |
| Surface | Timing | Treatment | Mean | p-Value |
|---|---|---|---|---|
| Machined | 30 s | CHX | 0.419 | 0.001 |
| Machined | 30 s | C + P | 0.126 | |
| Machined | 1 min | CHX | 0.114 | 0.1054 |
| Machined | 1 min | C + P | 0.052 | |
| Machined | 5 min | CHX | 0.172 | 0.0173 |
| Machined | 5 min | C + P | 0.024 |
| Surface | Timing | Treatment | Mean | p-Value |
|---|---|---|---|---|
| Rough | 30 s | CHX | 0.529 | <0.0001 |
| Rough | 30 s | C + P | 0.043 | |
| Rough | 1 min | CHX | 0.163 | 0.0067 |
| Rough | 1 min | C + P | 0.022 | |
| Rough | 5 min | CHX | 0.163 | 0.0016 |
| Rough | 5 min | C + P | 0.042 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Passarelli, P.C.; De Leonardis, M.; Piccirillo, G.B.; Desantis, V.; Papa, R.; Rella, E.; Mastandrea Bonaviri, G.N.; Papi, P.; Pompa, G.; Pasquantonio, G.; et al. The Effectiveness of Chlorhexidine and Air Polishing System in the Treatment of Candida albicans Infected Dental Implants: An Experimental In Vitro Study. Antibiotics 2020, 9, 179. https://doi.org/10.3390/antibiotics9040179
Passarelli PC, De Leonardis M, Piccirillo GB, Desantis V, Papa R, Rella E, Mastandrea Bonaviri GN, Papi P, Pompa G, Pasquantonio G, et al. The Effectiveness of Chlorhexidine and Air Polishing System in the Treatment of Candida albicans Infected Dental Implants: An Experimental In Vitro Study. Antibiotics. 2020; 9(4):179. https://doi.org/10.3390/antibiotics9040179
Chicago/Turabian StylePassarelli, Pier Carmine, Marta De Leonardis, Giovan Battista Piccirillo, Viviana Desantis, Raffaele Papa, Edoardo Rella, Giuseppe Niccolò Mastandrea Bonaviri, Piero Papi, Giorgio Pompa, Guido Pasquantonio, and et al. 2020. "The Effectiveness of Chlorhexidine and Air Polishing System in the Treatment of Candida albicans Infected Dental Implants: An Experimental In Vitro Study" Antibiotics 9, no. 4: 179. https://doi.org/10.3390/antibiotics9040179
APA StylePassarelli, P. C., De Leonardis, M., Piccirillo, G. B., Desantis, V., Papa, R., Rella, E., Mastandrea Bonaviri, G. N., Papi, P., Pompa, G., Pasquantonio, G., Manicone, P. F., & D’Addona, A. (2020). The Effectiveness of Chlorhexidine and Air Polishing System in the Treatment of Candida albicans Infected Dental Implants: An Experimental In Vitro Study. Antibiotics, 9(4), 179. https://doi.org/10.3390/antibiotics9040179