Increased Azithromycin Susceptibility of Multidrug-Resistant Gram-Negative Bacteria on RPMI-1640 Agar Assessed by Disk Diffusion Testing

 , ,
, ,
Abstract
:1. Introduction
2. Results
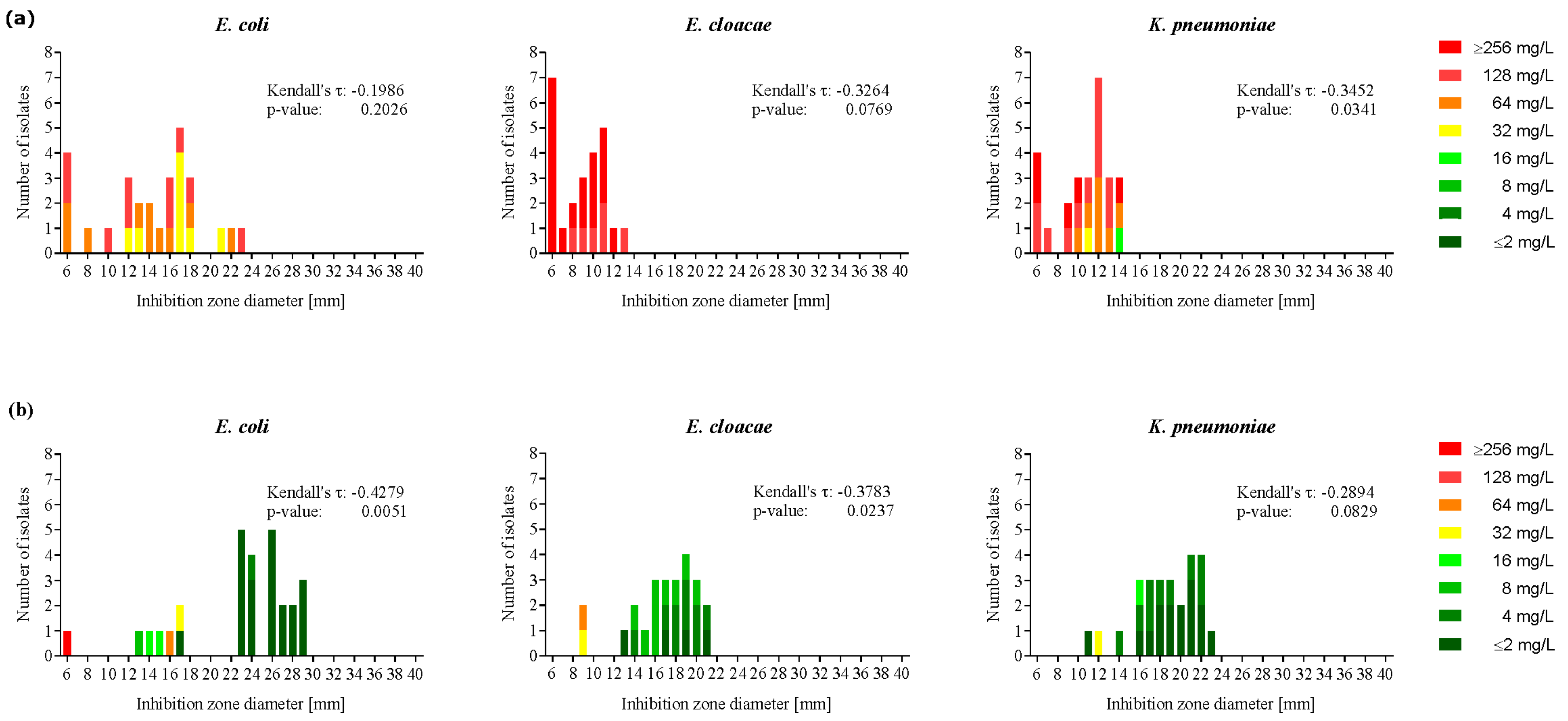
2.1. Enterobacteriaceae Showed Enhanced Azithromycin Susceptibility on RPMI-1640 Agar
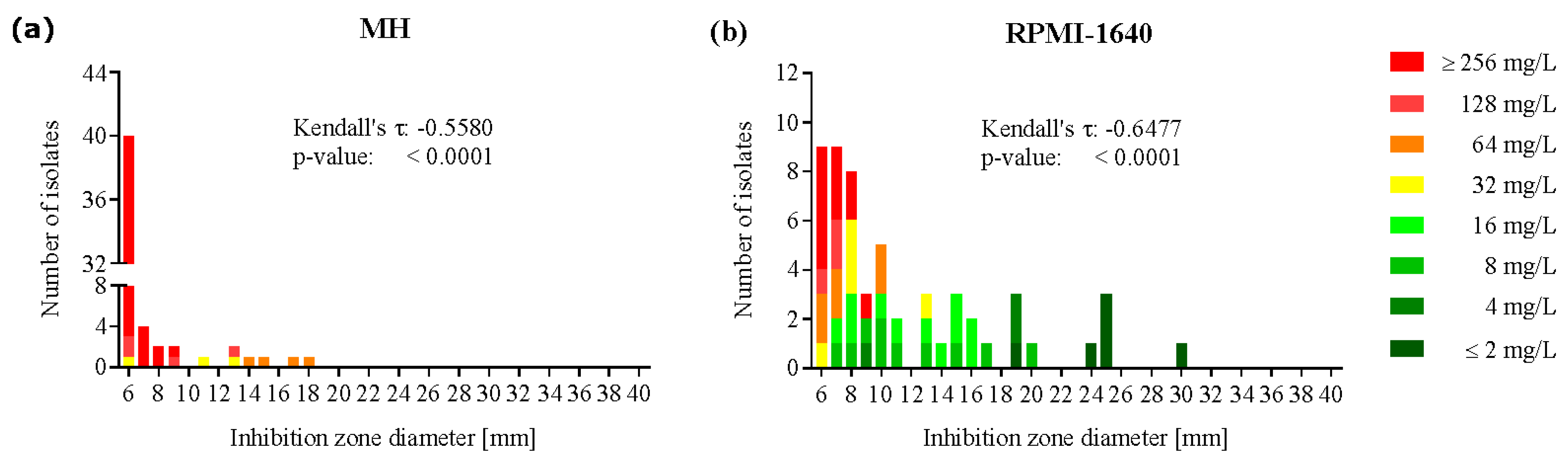
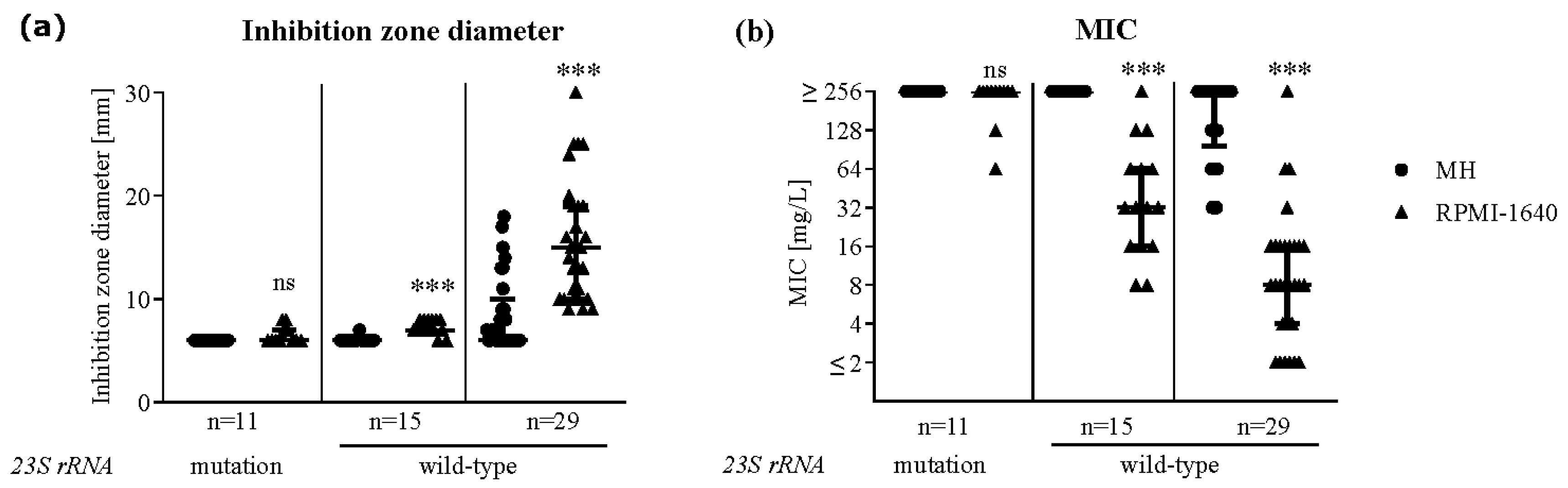
2.2. Azithromycin Susceptibility Increased on RPMI-1640 Agar in a Subgroup of P. aeruginosa
3. Discussion
4. Materials and Methods
4.1. Bacterial Strains and Media
4.2. Disk Diffusion Testing
4.3. Broth Microdilution Susceptibility Testing
4.4. Sequencing of the Gene Coding for Domain V of the 23S Ribosomal Subunit
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deak, D.; Outterson, K.; Powers, J.H.; Kesselheim, A.S. Progress in the Fight against Multidrug-Resistant Bacteria? A Review of U.S. Food and Drug Administration—Approved Antibiotics, 2010–2015. Ann. Intern. Med. 2016, 165, 363. [Google Scholar] [CrossRef]
- Outterson, K.; Powers, J.H.; Daniel, G.W.; McClellan, M.B. Repairing the Broken Market for Antibiotic Innovation. Health Aff. 2015, 34, 277–285. [Google Scholar] [CrossRef]
- Laopaiboon, M.; Panpanich, R.; Mya, K.S. Azithromycin for acute lower respiratory tract infections. Cochrane Database Syst. Rev. 2015, 2015, CD001954. [Google Scholar] [CrossRef]
- Leclercq, R. Mechanisms of Resistance to Macrolides and Lincosamides: Nature of the Resistance Elements and Their Clinical Implications. Clin. Infect. Dis. 2002, 34, 482–492. [Google Scholar] [CrossRef] [Green Version]
- Vaara, M. Outer membrane permeability barrier to azithromycin, clarithromycin, and roxithromycin in gram-negative enteric bacteria. Antimicrob. Agents Chemother. 1993, 37, 354–356. [Google Scholar] [CrossRef] [Green Version]
- Schweizer, H.P. Efflux as a mechanism of resistance to antimicrobials in Pseudomonas aeruginosa and related bacteria: Unanswered questions. Genet. Mol. Res. 2003, 2, 48–62. [Google Scholar] [PubMed]
- Gomes, C.; Martínez-Puchol, S.; Palma, N.; Horna, G.; Ruiz-Roldán, L.; Pons, M.J.; Ruiz, J. Macrolide resistance mechanisms in Enterobacteriaceae: Focus on azithromycin. Crit. Rev. Microbiol. 2016, 43, 1–30. [Google Scholar] [CrossRef]
- Lübbert, C. Antimicrobial therapy of acute diarrhoea: A clinical review. Expert Rev. Anti-infective Ther. 2015, 14, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Giamarellos-Bourboulis, E.J.; Mylona, V.; Antonopoulou, A.; Tsangaris, I.; Koutelidakis, I.; Marioli, A.; Raftogiannis, M.; Kopterides, P.; Lymberopoulou, K.; Mouktaroudi, M.; et al. Effect of clarithromycin in patients with suspected Gram-negative sepsis: Results of a randomized controlled trial. J. Antimicrob. Chemother. 2013, 69, 1111–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giamarellos-Bourboulis, E.J.; Pechère, J.-C.; Routsi, C.; Plachouras, D.; Kollias, S.; Raftogiannis, M.; Zervakis, D.; Baziaka, F.; Koronaios, A.; Antonopoulou, A.; et al. Effect of Clarithromycin in Patients with Sepsis and Ventilator-Associated Pneumonia. Clin. Infect. Dis. 2008, 46, 1157–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, Y.; Chai, D.; Wang, R.; Bai, N.; Liang, B.-B.; Liu, Y. Effectiveness and safety of macrolides in cystic fibrosis patients: A meta-analysis and systematic review. J. Antimicrob. Chemother. 2011, 66, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.W.; Kirby, W.M.M.; Sherris, J.C.; Turck, M. Antibiotic Susceptibility Testing by a Standardized Single Disk Method. Am. J. Clin. Pathol. 1966, 45, 493–496. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 8.1. 2018. Available online: https://www.eucast.org/ast_of_bacteria/previous_versions_of_documents/ (accessed on 28 April 2020).
- Gomes, C.; Ruiz-Roldán, L.; Mateu, J.; Ochoa, T.J.; Ruiz, J. Azithromycin resistance levels and mechanisms in Escherichia coli. Sci. Rep. 2019, 9, 6089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, L.; Nonejuie, P.; Munguia, J.; Hollands, A.; Olson, J.; Dam, Q.; Kumaraswamy, M.; Rivera, H.; Corriden, R.; Rohde, M.; et al. Azithromycin Synergizes with Cationic Antimicrobial Peptides to Exert Bactericidal and Therapeutic Activity Against Highly Multidrug-Resistant Gram-Negative Bacterial Pathogens. EBioMedicine 2015, 2, 690–698. [Google Scholar] [CrossRef] [Green Version]
- Kumaraswamy, M.; Lin, L.; Olson, J.; Sun, C.-F.; Nonejuie, P.; Corriden, R.; Döhrmann, S.; Ali, S.R.; Amaro, D.; Rohde, M.; et al. Standard susceptibility testing overlooks potent azithromycin activity and cationic peptide synergy against MDR Stenotrophomonas maltophilia. J. Antimicrob. Chemother. 2016, 71, 1264–1269. [Google Scholar] [CrossRef] [Green Version]
- Buyck, J.M.; Plesiat, P.; Traore, H.; Vanderbist, F.; Tulkens, P.M.; Van Bambeke, F. Increased Susceptibility of Pseudomonas aeruginosa to Macrolides and Ketolides in Eukaryotic Cell Culture Media and Biological Fluids Due to Decreased Expression of oprM and Increased Outer-Membrane Permeability. Clin. Infect. Dis. 2012, 55, 534–542. [Google Scholar] [CrossRef] [Green Version]
- Ersoy, S.C.; Heithoff, D.M.; Barnes, L.; Tripp, G.K.; House, J.K.; Marth, J.D.; Smith, J.W.; Mahan, M.J. Correcting a Fundamental Flaw in the Paradigm for Antimicrobial Susceptibility Testing. EBioMedicine 2017, 20, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, E.B.; Tam, V.H. Detection and treatment options for Klebsiella pneumoniae carbapenemases (KPCs): An emerging cause of multidrug-resistant infection. J. Antimicrob. Chemother. 2010, 65, 1119–1125. [Google Scholar] [CrossRef] [Green Version]
- Kronvall, G.; Giske, C.G.; Kahlmeter, G. Setting interpretive breakpoints for antimicrobial susceptibility testing using disk diffusion. Int. J. Antimicrob. Agents 2011, 38, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Mustafa, M.-H.; Khandekar, S.; Tunney, M.; Elborn, J.S.; Kahl, B.C.; Denis, O.; Plésiat, P.; Traore, H.; Tulkens, P.M.; Vanderbist, F.; et al. Acquired resistance to macrolides in Pseudomonas aeruginosa from cystic fibrosis patients. Eur. Respir. J. 2017, 49, 1601847. [Google Scholar] [CrossRef] [Green Version]
- Li, X.Z.; Nikaido, H.; Poole, K. Role of mexA-mexB-oprM in antibiotic efflux in Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 1995, 39, 1948–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuda, N.; Sakagawa, E.; Ohya, S.; Gotoh, N.; Tsujimoto, H.; Nishino, T. Substrate Specificities of MexAB-OprM, MexCD-OprJ, and MexXY-OprM Efflux Pumps in Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2000, 44, 3322–3327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marvig, R.L.; Søndergaard, M.S.R.; Damkiær, S.; Høiby, N.; Johansen, H.K.; Molin, S.; Jelsbak, L. Mutations in 23S rRNA Confer Resistance against Azithromycin in Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 2012, 56, 4519–4521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Retsema, J.A.; Girard, A.E.; Milisen, W.B. Relationship of high tissue concentrations of azithromycin to bactericidal activity and efficacy in vivo. J. Antimicrob. Chemother. 1990, 25, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Phelan, V.; Fang, J.; Dorrestein, P.C. Mass Spectrometry Analysis of Pseudomonas aeruginosa Treated with Azithromycin. J. Am. Soc. Mass Spectrom. 2015, 26, 873–877. [Google Scholar] [CrossRef] [Green Version]
- Wolter, J.; Seeney, S.; Bell, S.C.; Bowler, S.; Masel, P.; McCormack, J. Effect of long term treatment with azithromycin on disease parameters in cystic fibrosis: A randomised trial. Thorax 2002, 57, 212–216. [Google Scholar] [CrossRef] [Green Version]
- Kanoh, S.; Rubin, B.K. Mechanisms of Action and Clinical Application of Macrolides as Immunomodulatory Medications. Clin. Microbiol. Rev. 2010, 23, 590–615. [Google Scholar] [CrossRef] [Green Version]
- Saini, H.; Chhibber, S.; Harjai, K. Azithromycin and ciprofloxacin: A possible synergistic combination against Pseudomonas aeruginosa biofilm-associated urinary tract infections. Int. J. Antimicrob. Agents 2015, 45, 359–367. [Google Scholar] [CrossRef]
- Matuschek, E.; Brown, D.; Kahlmeter, G. Development of the EUCAST disk diffusion antimicrobial susceptibility testing method and its implementation in routine microbiology laboratories. Clin. Microbiol. Infect. 2014, 20, O255–O266. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Routine and Extended Internal Quality Control for MIC Determination and Disk Diffusion as Recommended by EUCAST. Version 6.1. 2016. Available online: https://www.eucast.org/ast_of_bacteria/previous_versions_of_documents/ (accessed on 28 April 2020).
- European Committee on Antimicrobial Susceptibility Testing. Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by broth dilution. Clin. Microbiol. Infect. 2003, 9, 9–15. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Family | Species | n | MH [mm] | RPMI-1640 [mm] |
|---|---|---|---|---|
| E. coli | 28 | 15.5 (12–17) | 24 (18.5–26.75) *** | |
| Enterobacteriaceae | E. cloacae | 24 | 9 (6–11) | 17.5 (15.25–19) *** |
| K. pneumoniae | 26 | 11.5 (9–12.25) | 19 (16.75–21) *** | |
| Pseudomonadaceae | P. aeruginosa | 55 | 6 (6–7) | 9 (7–15) *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meerwein, M.; Tarnutzer, A.; Böni, M.; Van Bambeke, F.; Hombach, M.; Zinkernagel, A.S. Increased Azithromycin Susceptibility of Multidrug-Resistant Gram-Negative Bacteria on RPMI-1640 Agar Assessed by Disk Diffusion Testing. Antibiotics 2020, 9, 218. https://doi.org/10.3390/antibiotics9050218
Meerwein M, Tarnutzer A, Böni M, Van Bambeke F, Hombach M, Zinkernagel AS. Increased Azithromycin Susceptibility of Multidrug-Resistant Gram-Negative Bacteria on RPMI-1640 Agar Assessed by Disk Diffusion Testing. Antibiotics. 2020; 9(5):218. https://doi.org/10.3390/antibiotics9050218
Chicago/Turabian StyleMeerwein, Milton, Andrea Tarnutzer, Michelle Böni, Françoise Van Bambeke, Michael Hombach, and Annelies S. Zinkernagel. 2020. "Increased Azithromycin Susceptibility of Multidrug-Resistant Gram-Negative Bacteria on RPMI-1640 Agar Assessed by Disk Diffusion Testing" Antibiotics 9, no. 5: 218. https://doi.org/10.3390/antibiotics9050218
APA StyleMeerwein, M., Tarnutzer, A., Böni, M., Van Bambeke, F., Hombach, M., & Zinkernagel, A. S. (2020). Increased Azithromycin Susceptibility of Multidrug-Resistant Gram-Negative Bacteria on RPMI-1640 Agar Assessed by Disk Diffusion Testing. Antibiotics, 9(5), 218. https://doi.org/10.3390/antibiotics9050218