
Observational Study Regarding Possible Side Effects of Miniscrew-Assisted Rapid Palatal Expander (MARPE) with or without the Use of Corticopuncture Therapy

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Method
- Transverse maxillary deficiency;
- Stage D or E palatal fusion (as seen in Angelieri et al. [18]) confirmed on CBCT prior to MARPE insertion;
- A medical history without orthodontic treatment;
- Crossbite (unilateral or bilateral).
2.1. Outcome Measures
2.2. Clinical Outcomes
2.3. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suri, L.; Taneja, P. Surgically assisted rapid palatal expansion: A literature review. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 290–302. [Google Scholar] [CrossRef]
- Lee, K.J.; Park, Y.C.; Park, J.Y.; Hwang, W.S. Miniscrew-assisted nonsurgical palatal expansion before orthog-nathic surgery for a patient with severe mandibular prognathism. Am. J. Orthod. Dentofacial. Orthop. 2010, 137, 830–839. [Google Scholar] [CrossRef]
- Bell, R.A. A review of maxillary expansion in relation to rate of expansion and patient’s age. Am. J. Orthod. 1982, 81, 32–37. [Google Scholar] [CrossRef]
- Lagravère, M.O.; Carey, J.; Heo, G.; Toogood, R.W.; Major, P.W. Transverse, vertical, and anteroposterior changes from bone-anchored maxillary expansion vs traditional rapid maxillary expansion: A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 304–312. [Google Scholar] [CrossRef]
- Nojima, L.I.; Nojima, M.D.C.G.; Da Cunha, A.C.; Guss, N.O.; Sant’Anna, E.F. Mini-implant selection protocol applied to MARPE. Dent. Press J. Orthod. 2018, 23, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Fattori, L.; Sendyk, M.; De Paiva, J.B.; Normando, D.; Neto, J.R. Micro-osteoperforation effectiveness on tooth movement rate and impact on oral health related quality of life. Angle Orthod. 2020, 90, 640–647. [Google Scholar] [CrossRef]
- Nimeri, G.; Kau, C.H.; Abou-Kheir, N.S.; Corona, R. Acceleration of tooth movement during orthodontic treat-ment—A frontier in orthodontics. Prog. Orthod. 2013, 29, 14–42. [Google Scholar]
- Suzuki, S.S.; Braga, L.F.S.; Fujii, D.N.; Moon, W.; Suzuki, H. Corticopuncture Facilitated Microimplant-Assisted Rapid Palatal Expansion. Case Rep. Dent. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Aboalnaga, A.A.; Fayed, M.M.S.; El-Ashmawi, N.A.; Soliman, S.A. Effect of micro-osteoperforation on the rate of canine retraction: A split-mouth randomized controlled trial. Prog. Orthod. 2019, 20, 21. [Google Scholar] [CrossRef]
- AlQadasi, B.; Aldhorae, K.; Halboub, E.; Mahgoub, N.; Alnasri, A.; Assiry, A.; Xia, H.Y. The Effectiveness of Micro-osteoperforations during Canine Retraction: A Three-dimensional Randomized Clinical Trial. J. Int. Soc. Prev. Community Dent. 2019, 9, 637–645. [Google Scholar] [CrossRef]
- Brunetto, D.P.; Sant’Anna, E.F.; Machado, A.W.; Moon, W. Non-surgical treatment of transverse deficiency in adults using Microimplant-assisted Rapid Palatal Expansion (MARPE). Dent. Press J. Orthod. 2017, 22, 110–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanjideh, P.A.; Rossouw, P.E.; Campbell, P.M.; Opperman, L.A.; Buschang, P.H. Tooth movements in foxhounds after one or two alveolar corticotomies. Eur. J. Orthod. 2009, 32, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Melo, A.C.E.D.O.; Carneiro, L.O.T.; Pontes, L.F.; Cecim, R.L.; De Mattos, J.N.R.; Normando, D. Factors related to orthodontic treatment time in adult patients. Dent. Press J. Orthod. 2013, 18, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Giudice, A.L.; Quinzi, V.; Ronsivalle, V.; Martina, S.; Bennici, O.; Isola, G. Description of a Digital Work-Flow for CBCT-Guided Construction of Micro-Implant Supported Maxillary Skeletal Expander. Materials 2020, 13, 1815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garib, D.G.; Henriques, J.F.C.; Janson, G.; de Freitas, M.R.; Fernandes, A.Y. Periodontal effects of rapid maxillary expansion with tooth-tissue-borne and tooth-borne expanders: A computed tomography evaluation. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 749–758. [Google Scholar] [CrossRef]
- Baysal, A.; Karadede, I.; Hekimoglu, S.; Ucar, F.; Ozer, T.; Veli, I.; Uysal, T. Evaluation of root resorption following rapid maxillary expansion using cone-beam computed tomography. Angle Orthod. 2012, 82, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Giudice, A.L.; Galletti, C.; Gay-Escoda, C.; Leonardi, R. CBCT assessment of radicular volume loss after rapid maxillary expansion: A systematic review. J. Clin. Exp. Dent. 2018, 10, e484–e494. [Google Scholar] [CrossRef] [PubMed]
- Angelieri, F.; Cevidanes, L.H.; Franchi, L.; Gonçalves, J.R.; Benavides, E.; McNamara, J.A., Jr. Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Carlson, C.; Sung, J.; McComb, R.W.; Machado, A.W.; Moon, W. Microimplant-assisted rapid palatal expansion appliance to orthopedically correct transverse maxillary deficiency in an adult. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 716–728. [Google Scholar] [CrossRef]
- Suzuki, H.; Moon, W.; Previdente, L.H.; Suzuki, S.S.; Garcez, A.S.; Consolaro, A. Miniscrew-assisted rapid palatal expander (MARPE): The quest for pure orthopedic movement. Dent. Press J. Orthod. 2016, 21, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.S.-Y.; Kyung, H.-M.; Buschang, P.H. Continuous forces are more effective than intermittent forces in expanding sutures. Eur. J. Orthod. 2010, 32, 371–380. [Google Scholar] [CrossRef] [Green Version]
- Tausche, E.; Hansen, L.; Schneider, M.; Harzer, W. Bone-supported rapid maxillary expansion with an implant-borne Hyrax screw: The Dresden Distractor. Orthod. Franc. 2008, 79, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Northway, W.M.; Meade, J.B., Jr. Surgically assisted rapid maxillary expansion: A comparison of technique, response, and stability. Angle Orthod. 1997, 67, 309–320. [Google Scholar] [PubMed]
- Choi, S.-H.; Shi, K.-K.; Cha, J.-Y.; Park, Y.-C.; Lee, K.-J. Nonsurgical miniscrew-assisted rapid maxillary expansion results in acceptable stability in young adults. Angle Orthod. 2016, 86, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Deeb, W.; Hansen, L.; Hotan, T.; Hietschold, V.; Harzer, W.; Tausche, E. Changes in nasal volume after surgically assisted bone-borne rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Haas, A.J. Palatal expansion: Just the beginning of dentofacial orthopedics. Am. J. Orthod. 1970, 57, 219–255. [Google Scholar] [CrossRef]
- Sun, Z.; Hueni, S.; Tee, B.C.; Kim, H. Mechanical strain at alveolar bone and circummaxillary sutures during acute rapid palatal expansion. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e219–e228. [Google Scholar] [CrossRef] [PubMed]
- Melsen, B.; Melsen, F. The postnatal development of the palatomaxillary region studied on human autopsy ma-terial. Am. J. Orthod. 1982, 82, 329–342. [Google Scholar] [CrossRef]
- Lee, S.P.; Paik, K.S.; Kim, M.K. Anatomical study of the pyramidal process of the palatine bone in relation to im-plant placement in the posterior maxilla. J. Oral Rehabil. 2001, 28, 125–132. [Google Scholar] [CrossRef]
- Cantarella, D.; Dominguez-Mompell, R.; Mallya, S.M.; Moschik, C.; Pan, H.C.; Miller, J.; Moon, W. Changes in the midpalatal and pterygopalatine sutures induced by micro-implant-supported skeletal expander, analyzed with a novel 3D method based on CBCT imaging. Prog. Orthod. 2017, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Stuart, D.A.; Wiltshire, W.A. Rapid palatal expansion in the young adult: Time for a paradigm shift? J. Can. Dent. Assoc. 2003, 69, 374–377. [Google Scholar]
- MacGinnis, M.; Chu, H.; Youssef, G.; Wu, K.W.; Machado, A.W.; Moon, W. The effects of micro-implant assisted rapid palatal expansion (MARPE) on the nasomaxillary complex—A finite element method (FEM) analysis. Prog. Orthod. 2014, 15, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaconas, S.J.; Caputo, A.A. Observation of orthopedic force distribution produced by maxillary orthodontic appliances. Am. J. Orthod. 1982, 82, 492–501. [Google Scholar] [CrossRef]
- Pulver, R.J.; Campbell, P.M.; Opperman, L.A.; Buschang, P.H. Miniscrew-assisted slow expansion of mature rabbit sutures. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Hartono, N.; Soegiharto, B.M.; Widayati, R. The difference of stress distribution of maxillary expansion using rapid maxillary expander (RME) and maxillary skeletal expander (MSE)—A finite element analysis. Prog. Orthod. 2018, 19, 33. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.-Y.; Yang, T.-K.; Hsieh, H.-Y.; Yang, L.-Y. Comparison of the effects of micro-osteoperforation and corticision on the rate of orthodontic tooth movement in rats. Angle Orthod. 2015, 86, 558–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, A.H.; Al-Fraidi, A.A.; Al-Saeed, S.H. Corticotomy-assisted orthodontic treatment: Review. Open Dent. J. 2010, 4, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winsauer, H.; Walter, A.; Muchitsch, A.P.; Winsauer, C.; Jaeschke, D.; Katsaros, C. Pure bone borne maxillary expansion with 4 mini-implants in adults with and without SARPE: A consecutive study of 35 patients. In Proceedings of the Oral Presentation at the 91st Congress of the European Orthodontic Society, Venice, Italy, 13 June 2015. [Google Scholar]
- Vaida, L.; Todor, B.I.; Corega, C.; Băciuţ, M.; Băciuţ, G. A rare case of canine anomaly—A possible algorithm for treating it. Rom. J. Morphol. Embryol. 2014, 55, 1197–1202. [Google Scholar]
- Farronato, G.; Giannini, L.; Galbiati, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Maspero, C. Tessuti orali e trattamento ortodontico: Effetti avversi più comuni. Minerva Stomatol. 2013, 62, 431–446. [Google Scholar] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
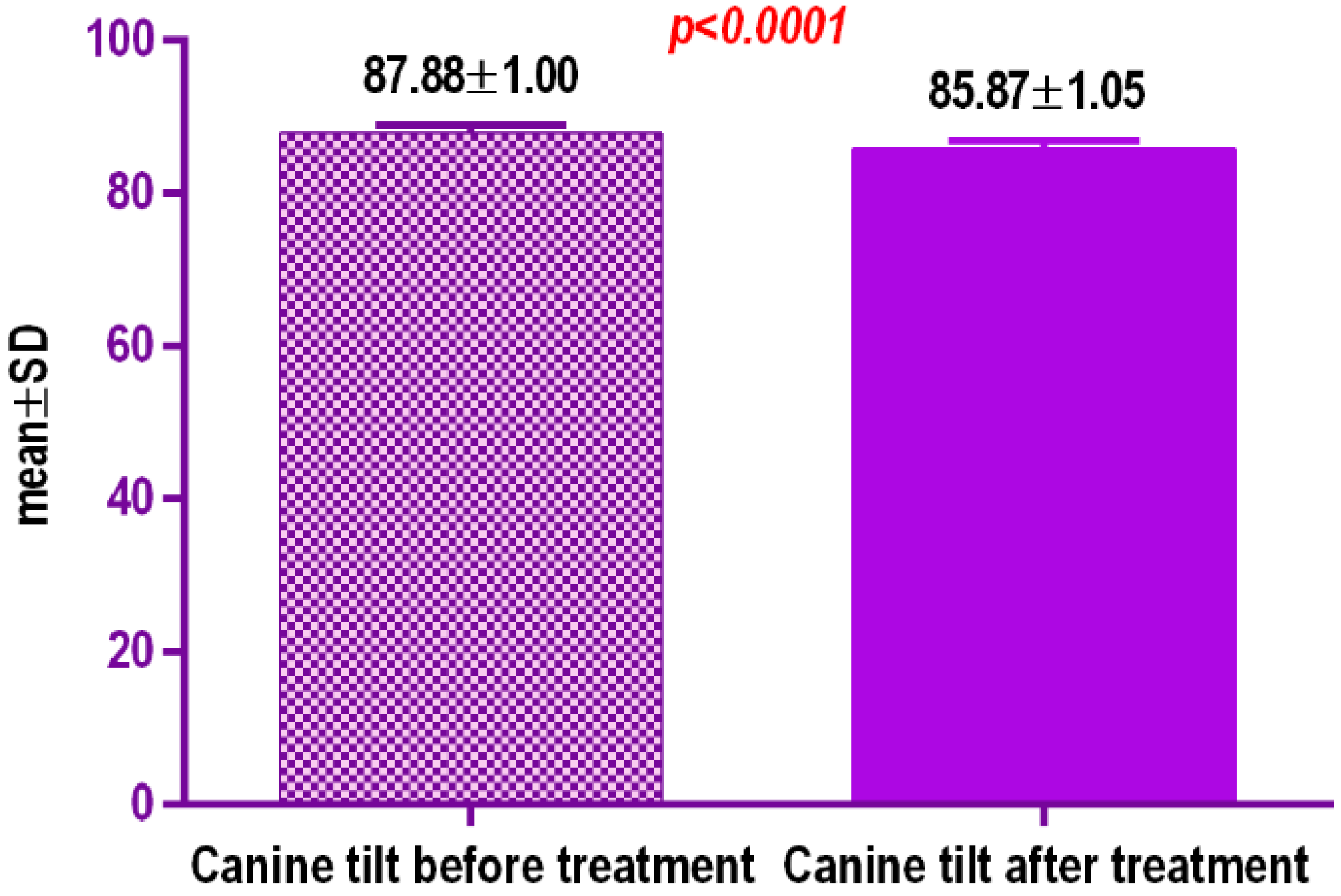
| Data Values | Data 1 |
|---|---|
| p value | <0.0001 |
| p value summary | |
| Significantly different? (p < 0.05) | Yes |
| One-or two-tailed p value? | Two-tailed |
| t, df | t = 12.33, df = 19 |
| Number of pairs | 48 |
| Mean of differences | 4.10 |
| SD of differences | 0.7273 |
| SEM of differences | 0.1626 |
| 95% confidence interval | 2.345 to 1.665 |
| R square | 0.8889 |
| Correlation coefficient (r) | 0.7515 |
| p value (one tailed) | <0.0001 |
| p value summary | |
| Significant correlation? (p > 0.05) | Yes |
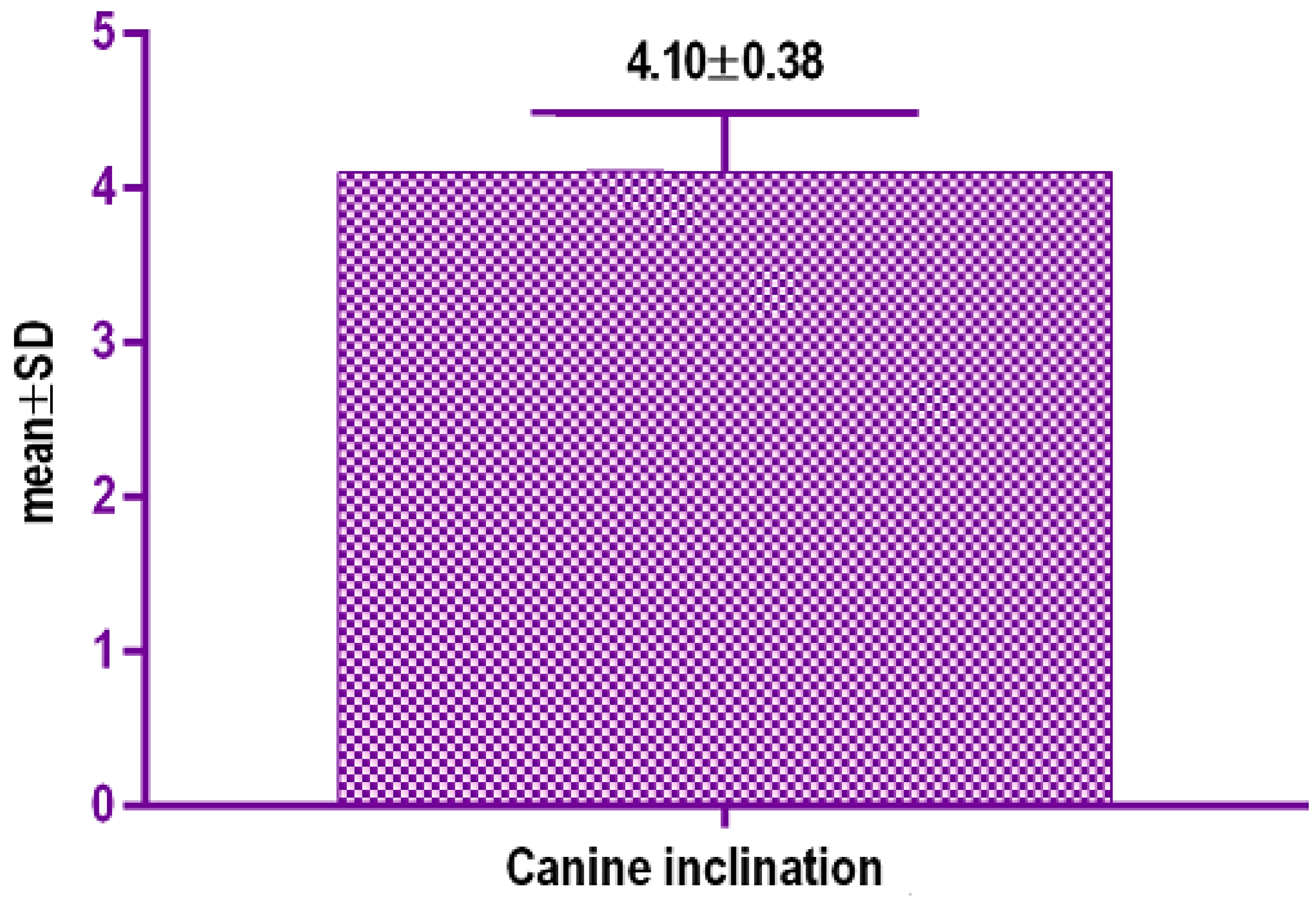
| Data | Canine Inclination/° |
|---|---|
| Mean | 4.10 |
| 25% Percentile | 2.783 |
| Median | 3.21 |
| 75% Percentile | 3.865 |
| Maximum | 4.77 |
| Mean | 4.103 |
| Std. Deviation | 0.3881 |
| Std. Error of Mean | 0.08679 |
| Lower 95% CI of mean | 2.921 |
| Upper 95% CI of mean | 3.784 |
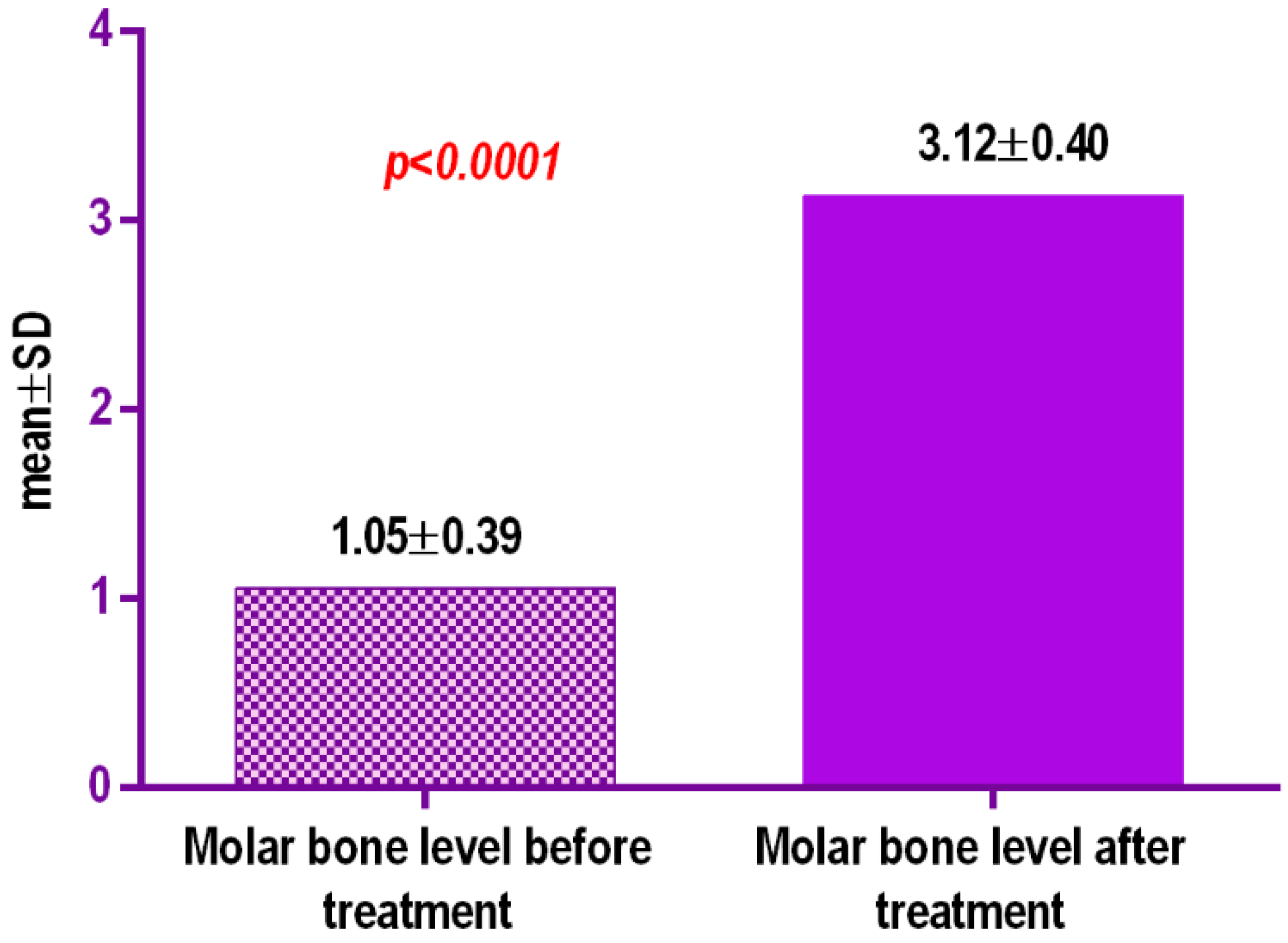
| Molar Bone Level Before Treatment | Molar Bone Level after Split | |
|---|---|---|
| Number of values | 30 | 30 |
| Minimum | 1.97 | 3.67 |
| 25% Percentile | 2.25 | 3.78 |
| Median | 2.2 | 3.995 |
| 75% Percentile | 4.165 | 2.385 |
| Maximum | 4.54 | 6.11 |
| Mean | 1.056 | 3.125 |
| Std. Deviation | 0.3956 | 0.407 |
| Std. Error of Mean | 0.1108 | 0.09102 |
| Lower 95% CI of mean | 1.534 | 2.934 |
| Upper 95% CI of mean | 1.998 | 3.316 |
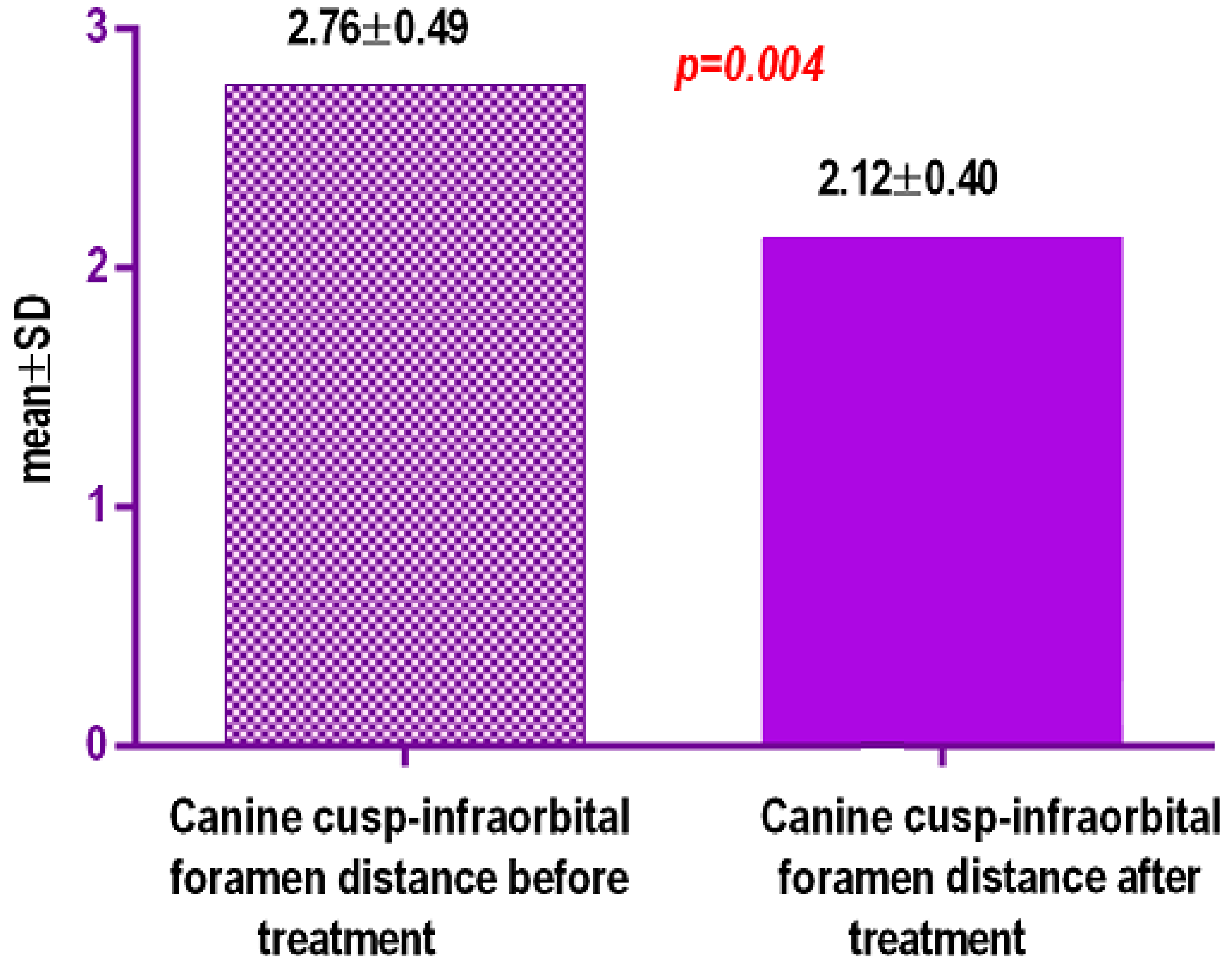
| Canine Cusp-Infraorbital Foramen Distance before Treatment/mm | Canine Cusp-Infraorbital Foramen Distance after Treatment/mm | |
|---|---|---|
| Number of values | 48 | 48 |
| Minimum | 41.97 | 38.67 |
| 25% Percentile | 41.25 | 37.82 |
| Median | 41.8 | 39.155 |
| 75% Percentile | 40.655 | 38.5 |
| Maximum | 42.4 | 41.11 |
| Mean | 2.766 | 2.125 |
| Std. Deviation | 0.4956 | 0.407 |
| Std. Error of Mean | 0.1108 | 0.09102 |
| Lower 95% CI of mean | 2.534 | 1.934 |
| Upper 95% CI of mean | 2.998 | 2.316 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bud, E.S.; Bică, C.I.; Păcurar, M.; Vaida, P.; Vlasa, A.; Martha, K.; Bud, A. Observational Study Regarding Possible Side Effects of Miniscrew-Assisted Rapid Palatal Expander (MARPE) with or without the Use of Corticopuncture Therapy. Biology 2021, 10, 187. https://doi.org/10.3390/biology10030187
Bud ES, Bică CI, Păcurar M, Vaida P, Vlasa A, Martha K, Bud A. Observational Study Regarding Possible Side Effects of Miniscrew-Assisted Rapid Palatal Expander (MARPE) with or without the Use of Corticopuncture Therapy. Biology. 2021; 10(3):187. https://doi.org/10.3390/biology10030187
Chicago/Turabian StyleBud, Eugen Silviu, Cristina Ioana Bică, Mariana Păcurar, Petru Vaida, Alexandru Vlasa, Krisztina Martha, and Anamaria Bud. 2021. "Observational Study Regarding Possible Side Effects of Miniscrew-Assisted Rapid Palatal Expander (MARPE) with or without the Use of Corticopuncture Therapy" Biology 10, no. 3: 187. https://doi.org/10.3390/biology10030187
APA StyleBud, E. S., Bică, C. I., Păcurar, M., Vaida, P., Vlasa, A., Martha, K., & Bud, A. (2021). Observational Study Regarding Possible Side Effects of Miniscrew-Assisted Rapid Palatal Expander (MARPE) with or without the Use of Corticopuncture Therapy. Biology, 10(3), 187. https://doi.org/10.3390/biology10030187