
Comparisons of Baseline Obesity Prevalence and Its Association with Perceived Health and Physical Performance in Military Officers
 ,
,  , ,
, ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures and Procedures
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Obesity Classification Comparisons
3.2.1. Relationships among Body Composition Measures
3.2.2. Rates of Obesity by Body Composition Measures
3.2.3. Obesity Classification and APFT Scores
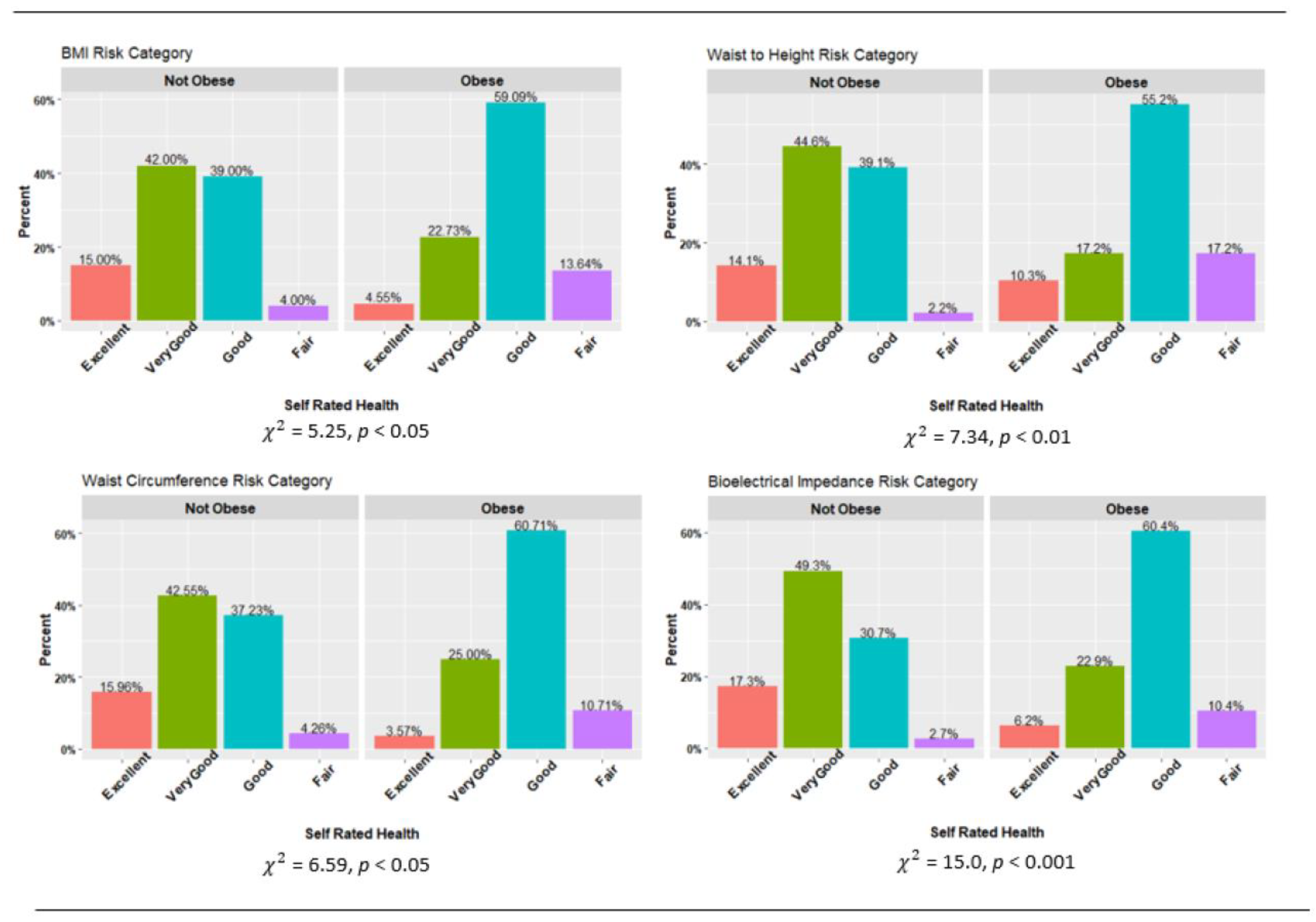
3.2.4. Obesity Classification and Self-Rated Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef]
- Meadows, S.; Engel, C.; Collins, R.; Beckman, R.; Breslau, J.; Bloom, E.L.; Dunbar, M.S.; Gilbert, M.L.; Grant, D.; Hawes-Dawson, J.; et al. 2018 Department of Defense Health Related Behaviors Survey (HRBS): Results for the Active Component; RAND Corporation: Santa Monica, CA, USA, 2021. [Google Scholar]
- Hoerster, K.D.; Lehavot, K.; Simpson, T.; McFall, M.; Reiber, G.; Nelson, K.M. Health and Health Behavior Differences: U.S. Military, Veteran, and Civilian Men. Am. J. Prev. Med. 2012, 43, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Trivette, E.T. Obesity and Army Readiness; U.S. Army Command and General Staff College: Fort Leavenworth, KS, USA, 2019. [Google Scholar]
- Shiozawa, B.; Madsen, C.; Banaag, A.; Patel, A.; Koehlmoos, T. Body Mass Index Effect on Health Service Utilization Among Active Duty Male United States Army Soldiers. Mil. Med. 2019, 184, 447–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voss, J.D.; Pavela, G.; Stanford, F.C. Obesity as a Threat to National Security: The Need for Precision Engagement. Int. J. Obes. 2019, 43, 437–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gattis, V.M. Obesity: A Threat to National Security? U.S. Army War College: Carlisle Barracks, PA, USA, 2011. [Google Scholar]
- Headquarters Department of the Army. Army Regulation 600-9; The Army Body Composition Program, Headquarters Department of the Army: Washington, DC, USA, 2019. [Google Scholar]
- Janssen, I.; Katzmarzyk, P.T.; Ross, R. Waist Circumference and Not Body Mass Index Explains Obesity-Related Health Risk. Am. J. Clin. Nutr. 2004, 79, 379–384. [Google Scholar] [CrossRef] [Green Version]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to-Height Ratio Is a Better Screening Tool than Waist Circumference and BMI for Adult Cardiometabolic Risk Factors: Systematic Review and Meta-Analysis. Obes. Rev. 2012, 13, 275–286. [Google Scholar] [CrossRef]
- Ashwell, M.; Mayhew, L.; Richardson, J.; Rickayzen, B. Waist-to-Height Ratio Is More Predictive of Years of Life Lost than Body Mass Index. PLoS ONE 2014, 9, e103483. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, S.A.; Lo, M.; Davis, W.S. Proposing Using Waist-to-Height Ratio as the Initial Metric for Body Fat Assessment Standards in the U.S. Army. Mil. Med. 2017, 182, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Griffith, J.R.; White, E.D.; Fass, R.D.; Lucas, B.M. Comparison of Body Composition Metrics for United States Air Force Airmen. Mil. Med. 2018, 183, E201–E207. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, D.J. Can Bioelectric Impedance Monitors Be Used to Accurately Estimate Body Fat in Chinese Adults? Asia Pac. J. Clin. Nutr. 2007, 16, 66–73. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Jitnarin, N.; Suminski, R.R.; Berkel, L.V.; Hunter, C.M.; Alvarez, L.; Brundige, A.R.; Peterson, A.L.; Foreyt, J.P.; Haddock, C.K.; et al. Obesity Classification in Military Personnel: A Comparison of Body Fat, Waist Circumference, and Body Mass Index Measurements. Mil. Med. 2008, 173, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shams-White, M.M.; Chui, K.; Deuster, P.A.; McKeown, N.M.; Must, A. Comparison of Anthropometric Measures in US Military Personnel in the Classification of Overweight and Obesity. Obesity 2020, 28, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Kukic, F.; Koropanovski, N.; Jankovic, R.; Cvorovic, A.; Dawes-J, J.; Lockie-G, R.; Orr, R.M.; Dopsaj, M. Association of Sex-Related Differences in Body Composition to Change of Direction Speed in Police Officers While Carrying Load. Int. J. Morphol. 2020, 38, 731–736. [Google Scholar] [CrossRef]
- U.S. Army CGSC Degree Programs. Available online: https://usacac.army.mil/organizations/cace/cgsc/CGSCDegreePrograms (accessed on 6 July 2021).
- Shea, K.P.; Fishback, S.J. Impact of Cumulative Combat Stress on Learning in an Academic Environment. In New Directions for Adult and Continuing Education; Wiley Online Library: Hoboken, NJ, USA, 2012; pp. 53–63. ISBN 1536-0717. [Google Scholar]
- Lythgoe, T.J. Some Modest Advice for the Command and General Staff Officer’s Course Class of 2020. Available online: http://fieldgradeleader.themilitaryleader.com/cgsc-advice/ (accessed on 10 July 2021).
- Meadows, S.; Engel, C.; Collins, R.; Beckman, R.; Cefalu, M.; Hawes-Dawson, J.; Doyle, M.; Kress, A.M.; Sontag-Padilla, L.; Ramchand, R.; et al. 2015 Department of Defense Health Related Behaviors Survey (HRBS); RAND Corporation: Santa Monica, CA, USA, 2018; ISBN 9780833098313. [Google Scholar]
- Golenbock, S.; Kazman, J.B.; Krauss, S.; Deuster, P.A. General Health Status in Army Personnel: Relations with Health Behaviors and Psychosocial Variables. Qual. Life Res. 2017, 26, 1839–1851. [Google Scholar] [CrossRef]
- Okosun, I.S.; Choi, S.; Matamoros, T.; Dever, G.E.A. Obesity Is Associated with Reduced Self-Rated General Health Status: Evidence from a Representative Sample of White, Black, and Hispanic Americans. Prev. Med. 2001, 32, 429–436. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Streetman, A.E.; Kukić, F.; Fong, C.; Hollerbach, B.S.; Goodman, B.D.; Haddock, C.K.; Poston, W.S.C. Baseline Physical Activity Behaviors and Relationships with Fitness in the Army Training at High Intensity Study. J. Funct. Morphol. Kinesiol. 2022, 7, 27. [Google Scholar] [CrossRef]
- Canadian Society for Exercise Physiology. Par-Q & You; University of Waterloo: Waterloo, ON, Canada, 2002. [Google Scholar]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical Impedance Analysis—Part I: Review of Principles and Methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef]
- Rubiano, F.; Nuñez, C.; Heymsfield, S.B. A Comparison of Body Composition Techniques. Ann. N. Y. Acad. Sci. 2000, 904, 335–338. [Google Scholar] [CrossRef]
- Strain, G.W.; Wang, J.; Gagner, M.; Pomp, A.; Inabnet, W.B.; Heymsfield, S.B. Bioimpedance for Severe Obesity: Comparing Research Methods for Total Body Water and Resting Energy Expenditure. Obesity 2008, 16, 1953–1956. [Google Scholar] [CrossRef]
- Beeson, W.L.; Batech, M.; Schultz, E.; Salto, L.; Firek, A.; Deleon, M.; Balcazar, H.; Cordero-Macintyre, Z. Comparison of Body Composition by Bioelectrical Impedance Analysis and Dual-Energy X-Ray Absorptiometry in Hispanic Diabetics. Int. J. Body Compos. Res. 2010, 8, 45–50. [Google Scholar]
- National Institutes of Health; National Heart Lung and Blood Institute; North American Society for the Study of Obesity. The Practical Guide: Identification, Evaluation and Treatment of Overweight and Obesity in Adults; National Institutes of Health: Bethesda, MD, USA, 2000; Volume 4084. [Google Scholar]
- Pierannunzi, C.; Hu, S.S.; Balluz, L. A Systematic Review of Publications Assessing Reliability and Validity of the Behavioral Risk Factor Surveillance System (BRFSS), 2004–2011. BMC Med. Res. Methodol. 2013, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Headquarters Department of the Army. FM 7–22: Army Physical Fitness Training, C1 ed.; Headquarters Department of the Army: Washington, DC, USA, 2012. [Google Scholar]
- R Core Team. The R Project for Statistical Consulting. Available online: https://www.r-project.org/ (accessed on 31 July 2019).
- Wickham, H. Ggplot2. Available online: https://www.ggplot2.org (accessed on 22 February 2018).
- Reyes-Guzman, C.M.; Bray, R.M.; Forman-Hoffman, V.L.; Williams, J. Overweight and Obesity Trends among Active Duty Military Personnel: A 13-Year Perspective. Am. J. Prev. Med. 2015, 48, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L.; Ph, D. Prevalence of Obesity and Severe Obesity Among Adults. NCHS Data Brief. 2020, 360, 107. [Google Scholar]
- Provencher, M.T.; Chahla, J.; Sanchez, G.; Cinque, M.E.; Kennedy, N.I.; Whalen, J.; Price, M.D.; Moatshe, G.; LaPrade, R.F. Body Mass Index Versus Body Fat Percentage in Prospective National Football League Athletes: Overestimation of Obesity Rate in Athletes at the National Football League Scouting Combine. J. Strength Cond. Res. 2018, 32, 1013–1019. [Google Scholar] [CrossRef]
- Lee, S.Y.; Gallagher, D. Assessment Methods in Human Body Composition. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 566–572. [Google Scholar] [CrossRef] [Green Version]
- Randhawa, A.K.; Jamnik, V.; Fung, M.D.T.; Fogel, A.S.; Kuk, J.L. No Differences in the Body Fat after Violating Core Bioelectrical Impedance Measurement Assumptions. BMC Public Health 2021, 21, 495. [Google Scholar] [CrossRef]
- Pierce, J.R.; DeGroot, D.W.; Grier, T.L.; Hauret, K.G.; Nindl, B.C.; East, W.B.; McGurk, M.S.; Jones, B.H. Body Mass Index Predicts Selected Physical Fitness Attributes but Is Not Associated with Performance on Military Relevant Tasks in U.S. Army Soldiers. J. Sci. Med. Sport 2017, 20, S79–S84. [Google Scholar] [CrossRef]
- Roberts, B.M.; Rushing, K.A.; Plaisance, E.P. Sex Differences in Body Composition and Fitness Scores in Military Reserve Officers’ Training Corps Cadets. Mil. Med. 2021, usaa496. [Google Scholar] [CrossRef]
- Steed, C.L.; Krull, B.R.; Morgan, A.L.; Tucker, R.M.; Ludy, M.-J. Relationship between Body Fat and Physical Fitness in Army ROTC Cadets. Mil. Med. 2016, 181, 1007–1012. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All (n = 136) | Male (n = 103) | Female (n = 33) |
|---|---|---|---|
| Mean Age ± SD | 34.0 ± 5.8 | 33.9 ± 5.8 | 34.2 ± 6.1 |
| Hispanic Ethnicity (%) | 4.8 | 5.3 | 3.4 |
| Race (%) White, Non-Hispanic Black Asian Amer Indian/Alaska Native Multi Race Other | 74.8 10.9 8.4 <1 1.7 3.4 | 78.9 8.9 6.7 1.1 1.1 3.3 | 62.1 17.2 13.8 0 3.4 3.4 |
| Rank (%) E1–E4 E5–E6 Officer Trainee O1–O3 O3E O4–O10 | 8.1 10.6 <1 46.3 <1 33.3 | 7.5 10.6 1.1 50.0 1.1 29.8 | 10.4 10.4 0 34.5 0 44.8 |
| Sex and Age Characteristics | BMI ≥ 30 | WHtR > 0.55 | WC > 102 cm Men WC > 88 cm Women | BF% > 25 Men BF% > 30 Women |
|---|---|---|---|---|
| Sex | ||||
| All | 18.5 | 24.6 | 23.0 | 39.7 |
| Men | 21.4 | 24.3 | 17.5 | 30.1 |
| Women | 9.4 | 25.8 | 40.6 | 69.7 |
| Age | ||||
| 19–29 | 11.8 | 5.9 | 11.8 | 17.6 |
| 30–39 | 19.6 | 27.1 | 23.7 | 40.8 |
| 40–49 | 19.1 | 28.6 | 28.6 | 52.3 |
| Paygrade | ||||
| E1–E4 | 10.0 | 10.0 | 10.0 | 20.0 |
| E5–E6 | 15.4 | 15.4 | 7.7 | 38.5 |
| Officer Trainee | 0.0 | 0.0 | 0.0 | 0.0 |
| O1–O3/O3E | 19.6 | 26.8 | 22.8 | 36.8 |
| O4–O10 | 19.5 | 27.5 | 32.5 | 48.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hollerbach, B.S.; Haddock, C.K.; Kukić, F.; Poston, W.S.C.; Jitnarin, N.; Jahnke, S.A.; DeBlauw, J.A.; Heinrich, K.M. Comparisons of Baseline Obesity Prevalence and Its Association with Perceived Health and Physical Performance in Military Officers. Biology 2022, 11, 1789. https://doi.org/10.3390/biology11121789
Hollerbach BS, Haddock CK, Kukić F, Poston WSC, Jitnarin N, Jahnke SA, DeBlauw JA, Heinrich KM. Comparisons of Baseline Obesity Prevalence and Its Association with Perceived Health and Physical Performance in Military Officers. Biology. 2022; 11(12):1789. https://doi.org/10.3390/biology11121789
Chicago/Turabian StyleHollerbach, Brittany S., Christopher K. Haddock, Filip Kukić, Walker S. C. Poston, Nattinee Jitnarin, Sara A. Jahnke, Justin A. DeBlauw, and Katie M. Heinrich. 2022. "Comparisons of Baseline Obesity Prevalence and Its Association with Perceived Health and Physical Performance in Military Officers" Biology 11, no. 12: 1789. https://doi.org/10.3390/biology11121789
APA StyleHollerbach, B. S., Haddock, C. K., Kukić, F., Poston, W. S. C., Jitnarin, N., Jahnke, S. A., DeBlauw, J. A., & Heinrich, K. M. (2022). Comparisons of Baseline Obesity Prevalence and Its Association with Perceived Health and Physical Performance in Military Officers. Biology, 11(12), 1789. https://doi.org/10.3390/biology11121789