
Angiogenin Levels and Their Association with Cardiometabolic Indices Following Vitamin D Status Correction in Saudi Adults

 , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects, Vitamin D Supplementation and Clinical Assessment
2.2. Biochemical Measurements
2.3. Data Analysis
3. Results
3.1. Changes in Biochemical Characteristics in All Subjects Post Intervention
3.2. Change in Biochemical Characteristics Post Intervention According to Gender
3.3. Correlation of Circulating Levels of ANG with Other Measured Parameters
3.4. Association of Change in ANG Levels Post Intervention with Other Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manakhov, A.; Permyakova, E.; Ershov, S.; Miroshnichenko, S.; Pykhtina, M.; Beklemishev, A.; Kovalskii, A.; Solovieva, A. XPS modeling of immobilized recombinant angiogenin and apoliprotein A1 on biodegradable nanofibers. Nanomaterials 2020, 10, 879. [Google Scholar] [CrossRef]
- Sheng, J.; Xu, Z. Three decades of research on angiogenin: A review and perspective. Acta Biochim. Biophys. Sin. 2016, 48, 399–410. [Google Scholar] [CrossRef] [Green Version]
- Matkar, P.N.; Ariyagunarajah, R.; Leong-Poi, H.; Singh, K.K. Friends turned foes: Angiogenic growth factors beyond angiogenesis. Biomolecules 2017, 7, 74. [Google Scholar] [CrossRef]
- Aliashrafi, S.; Ebrahimi-Mameghani, M. 7: A systematic review on vitamin d and angiogenesis. BMJ Open 2017, 7, bmjopen-2016. [Google Scholar]
- Woloszynska-Read, A.; Johnson, C.S.; Trump, D.L. Vitamin D and cancer: Clinical aspects. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 605–615. [Google Scholar] [CrossRef] [Green Version]
- Lagishetty, V.; Misharin, A.V.; Liu, N.Q.; Lisse, T.S.; Chun, R.F.; Ouyang, Y.; McLachlan, S.M.; Adams, J.S.; Hewison, M. Vitamin D deficiency in mice impairs colonic antibacterial activity and predisposes to colitis. Endocrinology 2010, 151, 2423–2432. [Google Scholar] [CrossRef] [Green Version]
- Lương, K.V.Q.; Nguyễn, L.T.H. The role of vitamin D in alzheimer’s disease: Possible genetic and cell signaling mechanisms. Am. J. Alzheimer’s Dis. Other Dement. 2013, 28, 126–136. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Mohammed, A.K.; Bukhari, I.; Rikli, M.; Abdi, S.; Ansari, M.G.A.; Sabico, S.; Hussain, S.D.; Alenad, A.; Al-Saleh, Y. Efficacy of vitamin D supplementation according to vitamin D-binding protein polymorphisms. Nutrition 2019, 63, 148–154. [Google Scholar] [CrossRef]
- Al Saleh, Y.; Beshyah, S.A.; Hussein, W.; Almadani, A.; Hassoun, A.; Al Mamari, A.; Ba-Essa, E.; Al-Dhafiri, E.; Hassanein, M.; Fouda, M.A.; et al. Diagnosis and management of vitamin D deficiency in the Gulf Cooperative Council (GCC) countries: An expert consensus summary statement from the GCC vitamin D advisory board. Arch. Osteoporos. 2020, 15, 35. [Google Scholar] [CrossRef]
- Gombart, A.F.; Pierre, A.; Maggini, S. A review of micronutrients and the immune system–working in harmony to reduce the risk of infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef] [Green Version]
- Al-Daghri, N.M.; Al-Saleh, Y.; Khan, N.; Sabico, S.; Aljohani, N.; Alfawaz, H.; Alsulaimani, M.; Al-Othman, A.M.; Alokail, M.S. Sun exposure, skin color and vitamin D status in Arab children and adults. J. Steroid. Biochem. Mol. Biol. 2016, 164, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Aljohani, N.J.; Al-Daghri, N.M.; Al-Attas, O.S.; Alokail, M.S.; Alkhrafy, K.M.; Al-Othman, A.; Yakout, S.; Alkabba, A.F.; Al-Ghamdi, A.S.; Almalki, M. Differences and associations of metabolic and vitamin D status among patients with and without sub-clinical hypothyroid dysfunction. BMC Endocr. Disord. 2013, 13, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Amer, O.E.; Khattak, M.N.K.; Sabico, S.; Ghouse Ahmed Ansari, M.; Al-Saleh, Y.; Aljohani, N.; Alfawaz, H.; Alokail, M.S. Effects of different vitamin D supplementation strategies in reversing metabolic syndrome and its component risk factors in adolescents. J. Steroid Biochem. Mol. Biol. 2019, 191, 105378. [Google Scholar] [CrossRef]
- Zhou, A.; Selvanayagam, J.B.; Hyppönen, E. Non-linear mendelian randomization analyses support a role for vitamin d deficiency in cardiovascular disease risk. Eur. Heart J. 2021; in press. [Google Scholar] [CrossRef]
- Acharya, P.; Dalia, T.; Ranka, S.; Sethi, P.; Oni, O.A.; Safarova, M.S.; Parashara, D.; Gupta, K.; Barua, R.S. The effects of vitamin d supplementation and 25-hydroxyvitamin d levels on the risk of myocardial infarction and mortality. J. Endocr. Soc. 2021, 5, bvab124. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez–Curiel, I.; Marin-Luevano, P.; Trujillo, V.; Enciso-Moreno, J.A.; Gonzalez-Castillo, C.; Rivas-Santiago, B. Calcitriol prevents inflammatory gene expression in macrovascular endothelial cells. Br. J. Biomed. Sci. 2016, 73, 74–78. [Google Scholar] [CrossRef]
- Mohd, S.; Sharma, S.; Mishra, A.; Ashraf, M.Z. Vitamin D and its relationship with the pathways related to thrombosis and various diseases. In Vitamin D; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Wattanapitayakul, S.K.; Weinstein, D.M.; Holycross, B.J.; Bauer, J.A. Endothelial dysfunction and peroxynitrite formation are early events in angiotensin-induced cardiovascular disorders. FASEB J. 2000, 14, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Yu, D.; Cai, Y.; Zhou, W.; Sheng, J.; Xu, Z. The potential of angiogenin as a serum biomarker for diseases: Systematic review and meta-analysis. Dis. Markers 2018, 2018, 1984718. [Google Scholar] [CrossRef]
- Bargieł, W.; Cierpiszewska, K.; Maruszczak, K.; Pakuła, A.; Szwankowska, D.; Wrzesińska, A.; Gutowski, Ł.; Formanowicz, D. Recognized and potentially new biomarkers—their role in diagnosis and prognosis of cardiovascular disease. Medicina 2021, 57, 701. [Google Scholar] [CrossRef]
- Grundy, S.M. Obesity, metabolic syndrome, and cardiovascular disease. J. Clin. Endocrinol. Metab. 2004, 89, 2595–2600. [Google Scholar] [CrossRef]
- Al-Daghri, N.M.; Al-Shuwaie, A.Y.A.; Alghamdi, A.; Amer, O.E.; Khattak, M.N.K.; Ansari, M.G.A.; Alnaami, A.M.; Sabico, S. Tristetraprolin, Inflammation, and Metabolic Syndrome in Arab Adults: A Case Control Study. Biology 2021, 10, 550. [Google Scholar] [CrossRef]
- Al-Saleh, Y.; Al-Daghri, N.M.; Sabico, S.; Alessa, T.; Al Emadi, S.; Alawadi, F.; Al Qasaabi, S.; Alfutaisi, A.; Al Izzi, M.; Mukhaimer, J.; et al. Diagnosis and management of osteoporosis in postmenopausal women in Gulf Cooperation Council (GCC) countries: Consensus statement of the GCC countries’ osteoporosis societies under the auspices of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Arch. Osteoporos. 2020, 15, 109. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Shi, X.; Chen, M.; Xu, N.; Sun, D.; Bai, R.; Chen, H.; Ding, K.; Sheng, J.; Xu, Z. Angiogenin promotes colorectal cancer metastasis via tirna production. Int. J. Cancer 2019, 145, 1395–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, D.; Sun, J.; Weng, Y.; Luo, L.; Sheng, J.; Xu, Z. Serum angiogenin as a potential biomarker for early detection of colorectal adenomas and colorectal cancer. Anti-Cancer Drugs 2021, 32, 703–708. [Google Scholar] [CrossRef]
- Aalami, A.H.; Abdeahad, H.; Mesgari, M.; Sathyapalan, T.; Sahebkar, A. Urinary angiogenin as a marker for bladder cancer: A meta-analysis. BioMed Res. Int. 2021, 2021, 5557309. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, V.; Marín-Luevano, P.; González-Curiel, I.; Rodríguez-Carlos, A.; Ramírez-Reyes, M.; Layseca-Espinosa, E.; Enciso-Moreno, J.A.; Díaz, L.; Rivas-Santiago, B. Calcitriol promotes proangiogenic molecules in keratinocytes in a diabetic foot ulcer model. J. Steroid Biochem. Mol. Biol. 2017, 174, 303–311. [Google Scholar] [CrossRef]
- Gruber, H.E.; Hoelscher, G.; Ingram, J.A.; Chow, Y.; Loeffler, B.; Hanley, E.N., Jr. 1,25(OH)2-vitamin D3 inhibits proliferation and decreases production of monocyte chemoattractant protein-1, thrombopoietin, VEGF, and angiogenin by human annulus cells in vitro. Spine 2008, 33, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Hooper, L.V.; Stappenbeck, T.S.; Hong, C.V.; Gordon, J.I. Angiogenins: A new class of microbicidal proteins involved in innate immunity. Nat. Immunol. 2003, 4, 269–273. [Google Scholar] [CrossRef]
- Packey, C.D.; Sartor, R.B. Commensal bacteria, traditional and opportunistic pathogens, dysbiosis and bacterial killing in inflammatory bowel diseases. Curr. Opin. Infect. Dis. 2009, 22, 292. [Google Scholar] [CrossRef] [Green Version]
- Kontush, A.; Chapman, M.J. Functionally defective high-density lipoprotein: A new therapeutic target at the crossroads of dyslipidemia, inflammation, and atherosclerosis. Pharmacol. Rev. 2006, 58, 342–374. [Google Scholar] [CrossRef]
- Arora, S.; Patra, S.K.; Saini, R. Hdl—A molecule with a multi-faceted role in coronary artery disease. Clin. Chim. Acta 2016, 452, 66–81. [Google Scholar] [CrossRef]
- Dworacka, M.; Krzyżagórska, E.; Wesołowska, A.; Zharmakhanova, G.; Iskakova, S.; Dworacki, G. Circulating monocyte chemotactic protein 1 (mcp-1), vascular cell adhesion molecule 1 (vcam-1) and angiogenin in type 2 diabetic patients treated with statins in low doses. Eur. J. Pharmacol. 2014, 740, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.V.; Sosin, M.; Gunarathne, A.; Hussain, I.; Davis, R.C.; Hughes, E.A.; Lip, G.Y. Elevated angiogenin levels in chronic heart failure. Ann. Med. 2008, 40, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Eren, E.; Yilmaz, N.; Aydin, O. High density lipoprotein and it’s dysfunction. Open Biochem. J. 2012, 6, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Wani, K.; Sabico, S.; Garbis, S.D.; Chrousos, G.P.; Amer, O.E.; Ansari, M.G.A.; Al-Saleh, Y.; Aljohani, N.J.; Al-Attas, O.S. Sex-specific expression of apolipoprotein levels following replenishment of vitamin d. J. Steroid Biochem. Mol. Biol. 2018, 180, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martínez, A.B.; Torres-Perez, E.; Devanney, N.; Del Moral, R.; Johnson, L.A.; Arbones-Mainar, J.M. Beyond the cns: The many peripheral roles of apoe. Neurobiol. Dis. 2020, 138, 104809. [Google Scholar] [CrossRef] [PubMed]
- van der Vorst, E.P. High-density lipoproteins and apolipoprotein A1. Subcell. Biochem. 2020, 94, 399–420. [Google Scholar] [PubMed]
- Miroshnichenko, S.; Usynin, I.; Dudarev, A.; Nimaev, V.; Solovieva, A. Apolipoprotein ai supports mscs survival under stress conditions. Int. J. Mol. Sci. 2020, 21, 4062. [Google Scholar] [CrossRef]
- Fiori, A.; Hammes, H.-P.; Bieback, K. Adipose-derived mesenchymal stromal cells reverse high glucose–induced reduction of angiogenesis in human retinal microvascular endothelial cells. Cytotherapy 2020, 22, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.J.; Jeon, S.Y.; Hong, W.K.; Jung, S.E.; Kang, H.J.; Kim, J.-W.; Jeon, J.-P.; Han, B.-G. Effect of glucose ingestion in plasma markers of inflammation and oxidative stress: Analysis of 16 plasma markers from oral glucose tolerance test samples of normal and diabetic patients. Diabetes Res. Clin. Pract. 2013, 99, e27–e31. [Google Scholar] [CrossRef] [PubMed]
- Das, N.A.; Carpenter, A.J.; Belenchia, A.; Aroor, A.R.; Noda, M.; Siebenlist, U.; Chandrasekar, B.; DeMarco, V.G. Empagliflozin reduces high glucose-induced oxidative stress and mir-21-dependent traf3ip2 induction and reck suppression, and inhibits human renal proximal tubular epithelial cell migration and epithelial-to-mesenchymal transition. Cell. Signal. 2020, 68, 109506. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Li, D.; Li, Y.; Zhang, X.; Song, Y.; Li, X. Effects of vitamin D supplementation on glucose and insulin homeostasis and incident diabetes among nondiabetic adults: A meta-analysis of randomized controlled trials. Int. J. Endocrinol. 2018, 2018, 7908764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirhosseini, N.; Vatanparast, H.; Mazidi, M.; Kimball, S.M. Vitamin D supplementation, glycemic control, and insulin resistance in prediabetics: A meta-analysis. J. Endocr. Soc. 2018, 2, 687–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, E.J.; Lamon-Fava, S.; Cohn, S.D.; Schaefer, M.M.; Ordovas, J.; Castelli, W.; Wilson, P. Effects of age, gender, and menopausal status on plasma low density lipoprotein cholesterol and apolipoprotein b levels in the framingham offspring study. J. Lipid Res. 1994, 35, 779–792. [Google Scholar] [CrossRef]
- Öhlund, I.; Lind, T.; Hernell, O.; Silfverdal, S.-A.; Liv, P.; Karlsland Åkeson, P. Vitamin D status and cardiometabolic risk markers in young swedish children: A double-blind randomized clinical trial comparing different doses of vitamin d supplements. Am. J. Clin. Nutr. 2020, 111, 779–786. [Google Scholar] [CrossRef]
- Schwetz, V.; Scharnagl, H.; Trummer, C.; Stojakovic, T.; Pandis, M.; Gruebler, M.R.; Verheyen, N.; Gaksch, M.; Zittermann, A.; Aberer, F. Vitamin D supplementation and lipoprotein metabolism: A randomized controlled trial. J. Clin. Lipidol. 2018, 12, 588–596.e4. [Google Scholar] [CrossRef]
- Zhao, C.; Tsapanou, A.; Manly, J.; Schupf, N.; Brickman, A.M.; Gu, Y. Vitamin D intake is associated with dementia risk in the washington heights-inwood columbia aging project (whicap). Alzheimer’s Dement. 2020, 16, 1393–1401. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | All Subjects | ||
|---|---|---|---|
| Baseline | Follow-Up | p-Value | |
| N (Males/Females) | 100 (54/46) | ||
| Age (years) | 40.8 ± 9.9 | ||
| BMI (kg/m2) | 29.6 ± 5.2 | ||
| WHR | 0.93 ± 0.1 | ||
| Systolic BP (mmHg) | 127.1 ± 13.3 | ||
| Diastolic BP (mmHg) | 79.5 ± 9.3 | ||
| Glucose (mmol/L) | 5.75 ± 1.2 | 5.79 ± 1.1 | 0.82 |
| Total Cholesterol (mmol/L) | 4.9 ± 1.0 | 5.1 ± 1.2 | 0.24 |
| HDL-Cholesterol (mmol/L) | 1.01 ± 0.4 | 1.09 ± 0.4 | 0.12 |
| Triglycerides (mmol/L) | 1.5 (1.1, 2.2) | 1.7 (1.1, 2.3) | 0.22 |
| 25(OH)D (nmol/L) | 36.2 ± 10.4 | 55.2 ± 19.3 | <0.001 |
| Apo-CI (µg/mL) | 35.3 (28.2, 48.3) | 35.5 (29.8, 52.2) | 0.32 |
| Apo-H (µg/mL) | 412.3 ± 139.2 | 378.8 ± 157.8 | 0.15 |
| Apo-Al (mg/mL) | 19.78 (5.7, 7.5) | 18.82 (7.3, 61.3) | 0.64 |
| Apo-CIII (µg/mL) | 137.8 (66.9, 211.8) | 200.2 (63.5, 358.9) | 0.001 |
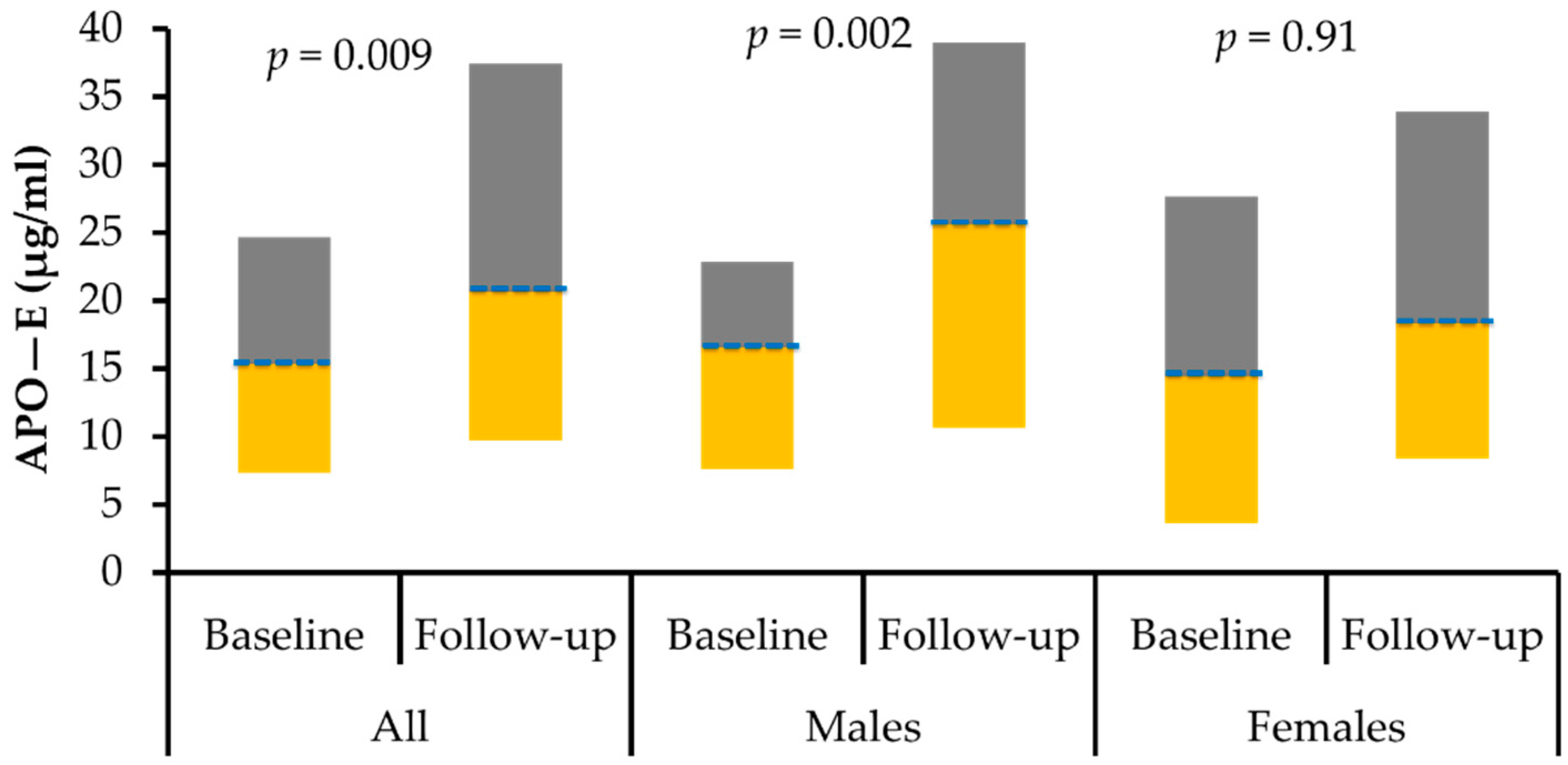
| Apo-E (µg/mL) | 14.8 (7.3, 24.3) | 19.6 (8.7, 36.6) | 0.009 |
| Apo-AII (mg/mL) | 0.93 (0.6, 0.9) | 0.91 (0.4, 1.4) | 0.36 |
| Apo-B (mg/mL) | 7.99 (5.2, 11.3) | 6.26 (3.5, 9.7) | 0.003 |
| Apo-CII (µg/mL) | 115.4 (69.4, 209.6) | 136.1 (71.9, 219.6) | 0.26 |
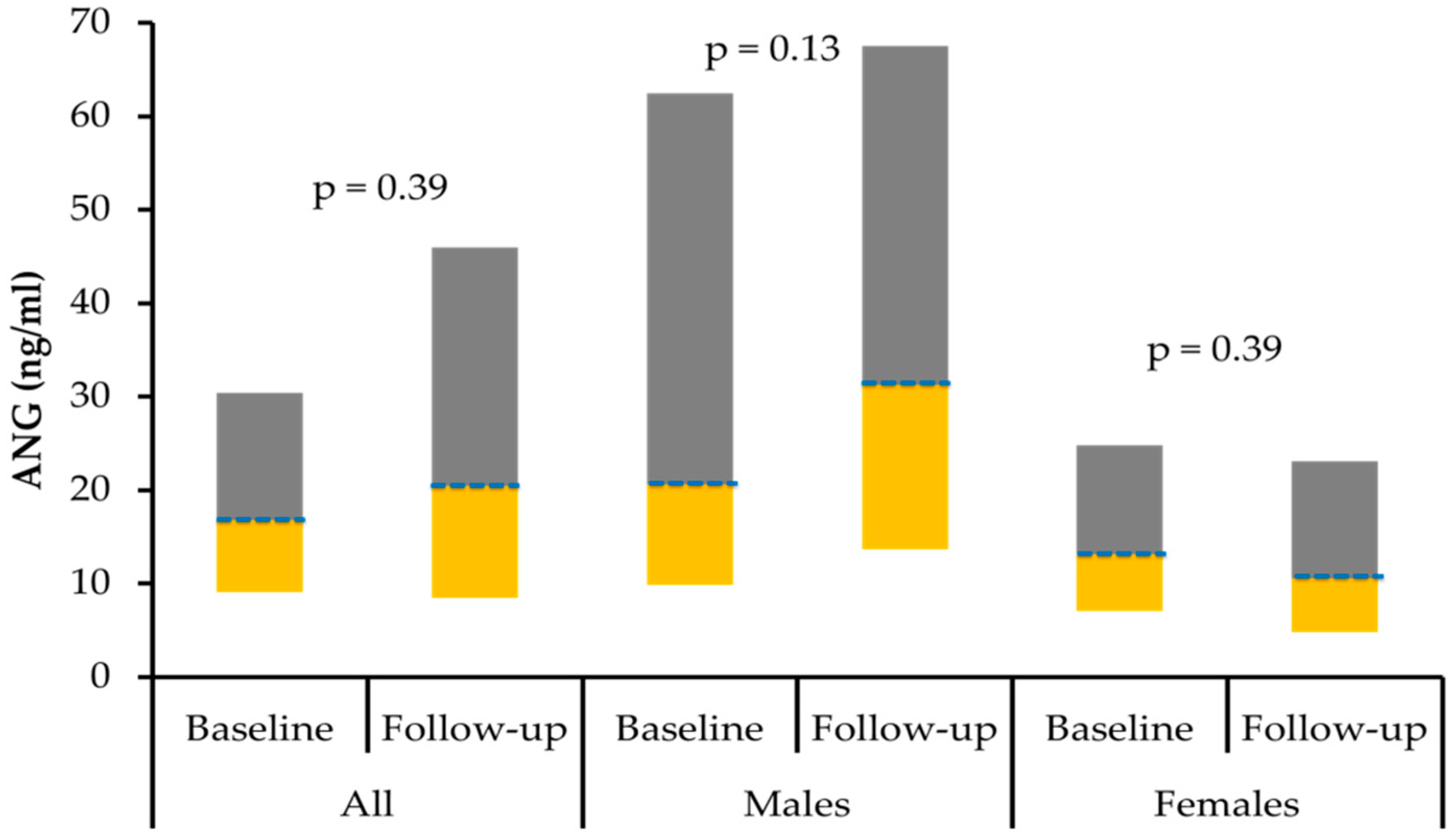
| ANG (ng/mL) | 16.5 (8.9, 27.8) | 19.1 (7.9, 36.9) | 0.39 |
| Parameters | Males | Females | ||||
|---|---|---|---|---|---|---|
| Baseline | Follow-Up | p-Value | Baseline | Follow-Up | p-Value | |
| N (M/F) | 54 | 54 | 46 | 46 | ||
| Age (years) | 41.9 ± 9.8 | 39.5 ± 9.9 | ||||
| BMI (kg/m2) | 28.8 ± 4.7 | 30.6 ± 5.5 | ||||
| WHR | 0.97 ± 0.1 | 0.88 ± 0.1 | ||||
| Systolic BP (mmHg) | 129.9 ± 11.1 | 123.5 ± 14.9 | ||||
| Diastolic BP (mmHg) | 80.6 ± 8.0 | 78.1 ± 10.7 | ||||
| Glucose (mmol/L) | 6.02 ± 1.2 | 6.03 ± 1.3 | 0.97 | 5.5 ± 1.3 | 5.6 ± 0.9 | 0.74 |
| T. Chol. (mmol/L) | 4.9 ± 1.0 | 5.1 ± 1.1 | 0.34 | 4.9 ± 0.9 | 5.0 ± 1.2 | 0.49 |
| HDL-C (mmol/L) | 0.98 ± 0.4 | 1.04 ± 0.4 | 0.22 | 1.05 ± 0.4 | 1.14 ± 0.4 | 0.29 |
| Trig.(mmol/L) | 1.50 (1.1, 2.4) | 1.60 (1.2, 2.0) | 0.45 | 1.4 (1.1, 1.9) | 1.8 (1.1, 2.4) | 0.26 |
| 25(OH) D (nmol/L) | 38.8 ± 9.6 | 55.1 ± 12.8 | <0.001 | 33.1 ± 10.6 | 55.2 ± 24.9 | <0.001 |
| Apo-CI (µg/mL) | 32.6 (23.8, 36.5) | 31.8 (26.6, 35.5) | 0.86 | 44.4 (32.2, 61.1) | 44.8 (36.6, 75.6) | 0.15 |
| Apo-H (µg/mL) | 396.7 ± 131.4 | 374.2 ± 159.9 | 0.53 | 424.9 ± 145.4 | 382.5 ± 157.8 | 0.18 |
| Apo-Al (mg/mL) | 19.37 (6.3, 49.2) | 18.28 (7.2, 26.6) | 0.24 | 23.40 (4.2, 212.3) | 22.98 (6.9, 161.9) | 0.09 |
| Apo-CIII (µg/mL) | 139.1 (70.8, 280.9) | 256.6 (124.1, 451.4) | <0.001 | 120.9 (57.9, 178.4) | 148.1 (24.5, 271.7) | 0.53 |
| Apo-E (µg/mL) | 15.9 (7.5, 23.3) | 25.6 (10.5, 39.4) | 0.002 | 13.8 (2.8, 27.5) | 16.6 (2.8, 29.0) | 0.91 |
| Apo-AII (mg/mL) | 1.23 (0.8, 1.6) | 1.25 (0.8, 1.7) | 0.55 | 0.72 (0.4, 1.2) | 0.62 (0.3, 0.9) | 0.07 |
| Apo-B (mg/mL) | 8.12 (6.4, 12.3) | 8.46 (4.5, 10.0) | 0.08 | 7.86 (3.8, 9.5) | 4.58 (1.8, 8.0) | 0.02 |
| Apo-CII (µg/mL) | 153.3 (90.3, 223.1) | 194.8 (112.1, 257.4) | 0.02 | 100.8 (56.9, 166.1) | 101.9 (28.3, 142.9) | 0.24 |
| ANG (ng/mL) | 19.1 (9.4, 38.4) | 27.5 (11.6, 51.0) | 0.13 | 13.3 (7.2, 25.3) | 10.3 (4.4, 22.9) | 0.39 |
| Parameters | Baseline | Follow-Up | ||||
|---|---|---|---|---|---|---|
| All | Males | Females | All | Males | Females | |
| N (M/F) | 100 | 54 | 46 | 100 | 54 | 46 |
| Age | −0.21 * | −0.11 | −0.34 * | −0.04 | −0.03 | 0.15 |
| BMI | −0.24 * | −0.26 | −0.18 | −0.29 ** | −0.16 | −0.24 |
| WHR | −0.26 * | −0.43 ** | −0.36 * | 0.08 | −0.06 | −0.31 |
| Systolic BP | 0.02 | 0.03 | −0.10 | −0.03 | −0.02 | −0.30 |
| Diastolic BP | −0.06 | −0.12 | −0.04 | 0.13 | 0.18 | −0.05 |
| Glucose | −0.20 | −0.38 ** | −0.15 | −0.12 | −0.05 | −0.36 * |
| Total-Cholesterol | 0.02 | 0.01 | 0.10 | 0.10 | 0.10 | 0.10 |
| HDL-Cholesterol | −0.25 * | −0.41 ** | −0.06 | 0.12 | 0.15 | 0.25 |
| Triglycerides # | −0.22 * | −0.24 | −0.25 | −0.13 | −0.05 | −0.22 |
| Vitamin D | 0.26 * | 0.08 | 0.43 ** | −0.23 * | −0.18 | −0.32 * |
| Apo-CI # | −0.26 * | −0.15 | −0.24 | −0.37 ** | −0.01 | −0.51 ** |
| Apo-H | −0.10 | −0.02 | −0.01 | −0.26 * | −0.36 * | −0.17 |
| Apo-Al # | 0.44 ** | 0.41 ** | 0.49 ** | 0.13 | −0.10 | 0.45 ** |
| Apo-CIII # | 0.45 ** | 0.42 ** | 0.51 ** | 0.45 ** | 0.26 | 0.48 ** |
| Apo-E # | 0.54 ** | 0.60 ** | 0.51 ** | 0.49 ** | 0.35 * | 0.56 ** |
| Apo-AII # | 0.42 ** | 0.43 ** | 0.32 * | 0.44 ** | 0.11 | 0.58 ** |
| Apo-B # | 0.27 * | 0.31 * | 0.18 | 0.34 ** | 0.10 | 0.47 ** |
| Apo-CII # | 0.39 ** | 0.38 ** | 0.36 * | 0.41 ** | 0.22 | 0.37 * |
| Parameters | Difference Post Intervention (ANG) | Δ Post Intervention (ANG) | ||||
|---|---|---|---|---|---|---|
| Δ (All) | Δ (Males) | Δ (Females) | ||||
| N (M/F) | 100 | 54 | 46 | 100 | 54 | 46 |
| Glucose | 0.10 | 0.16 | 0.10 | 0.10 | 0.21 | 0.03 |
| Total-Cholesterol | 0.02 | 0.01 | 0.02 | −0.02 | −0.10 | 0.01 |
| HDL-Cholesterol | −0.10 | −0.21 | −0.01 | −0.06 | −0.28 | 0.05 |
| Triglycerides # | 0.06 | 0.04 | 0.12 | −0.04 | −0.10 | 0.02 |
| Vitamin D | 0.03 | 0.10 | −0.10 | −0.01 | 0.16 | −0.15 |
| Apo-CI # | 0.10 | 0.14 | 0.13 | 0.07 | 0.17 | −0.01 |
| Apo-H | −0.20 | −0.25 | −0.12 | −0.22 | −0.26 | −0.15 |
| Apo-Al # | −0.11 | −0.18 | 0.04 | 0.10 | 0.01 | 0.20 |
| Apo-CIII # | 0.03 | 0.03 | −0.16 | 0.12 | 0.14 | 0.03 |
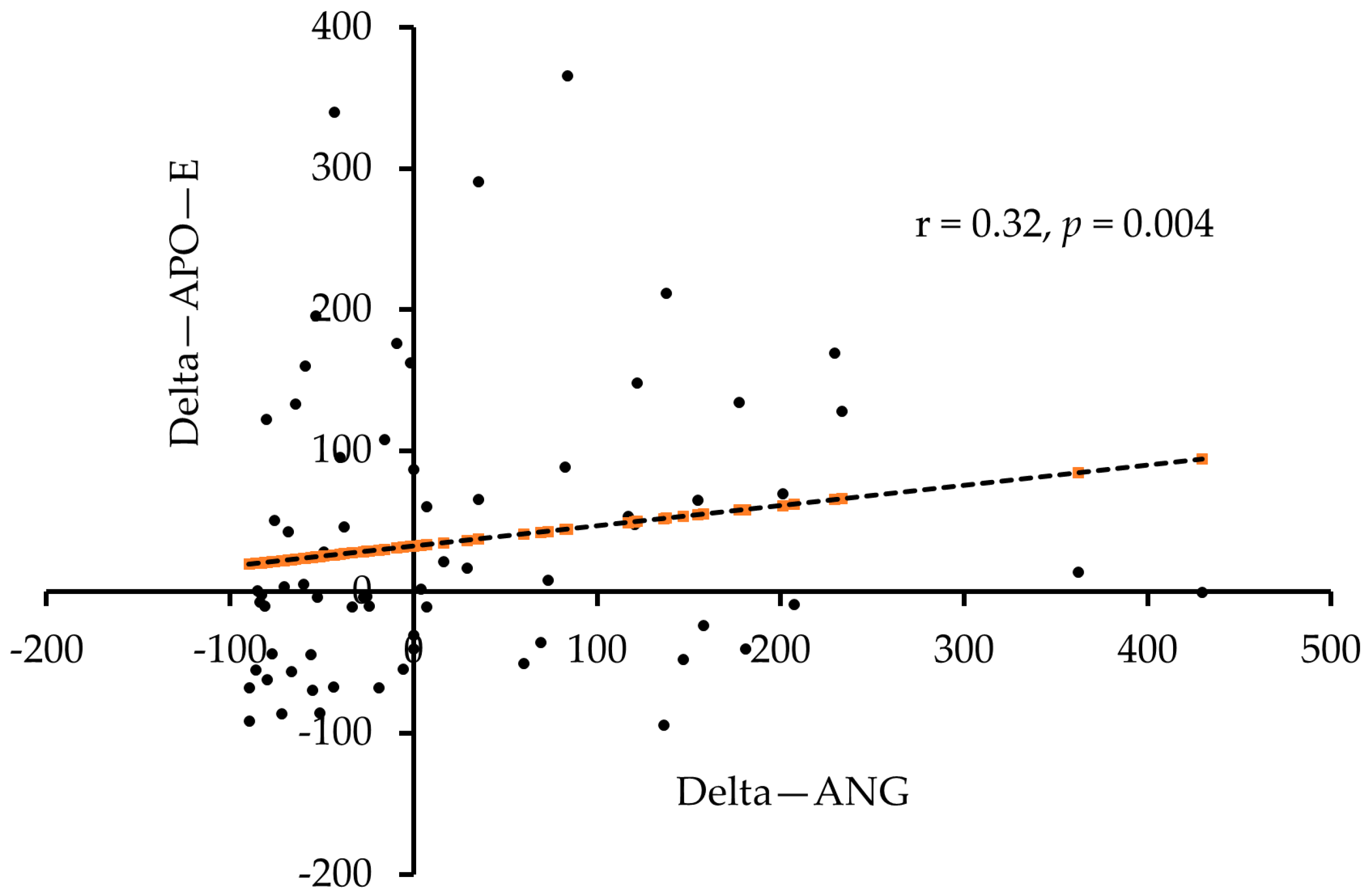
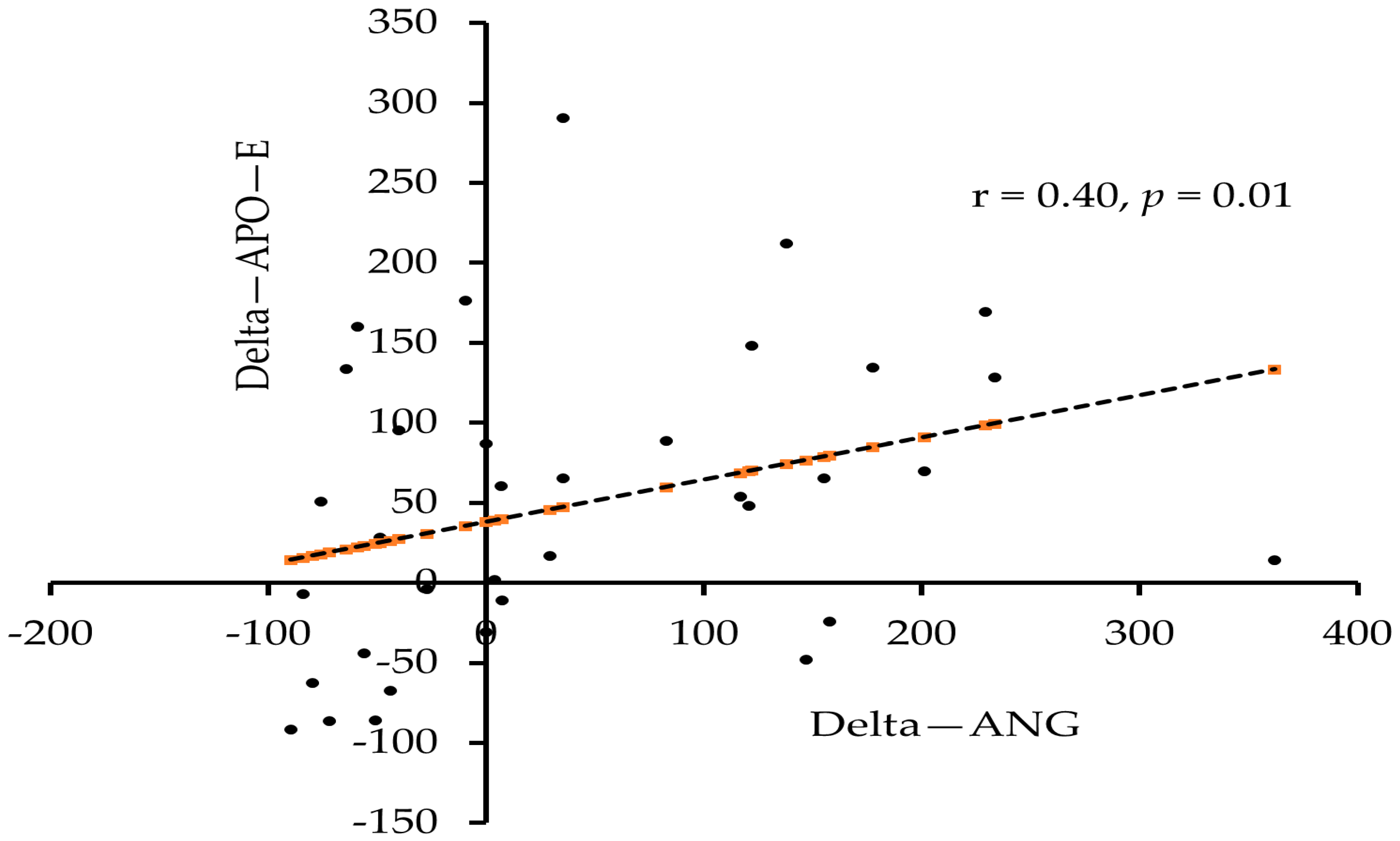
| Apo-E # | 0.26 * | 0.24 | 0.01 | 0.32 ** | 0.40 * | 0.11 |
| Apo-AII # | 0.04 | −0.08 | 0.03 | 0.20 | 0.12 | 0.27 |
| Apo-B # | 0.08 | 0.11 | −0.15 | 0.20 | 0.19 | 0.18 |
| Apo-CII # | 0.02 | 0.05 | −0.23 | 0.16 | 0.16 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldawsari, G.M.; Sabico, S.; Alamro, A.A.; Alenad, A.; Wani, K.; Alnaami, A.M.; Khattak, M.N.K.; Masoud, M.S.; Al-Daghri, N.M.; Alokail, M.S. Angiogenin Levels and Their Association with Cardiometabolic Indices Following Vitamin D Status Correction in Saudi Adults. Biology 2022, 11, 286. https://doi.org/10.3390/biology11020286
Aldawsari GM, Sabico S, Alamro AA, Alenad A, Wani K, Alnaami AM, Khattak MNK, Masoud MS, Al-Daghri NM, Alokail MS. Angiogenin Levels and Their Association with Cardiometabolic Indices Following Vitamin D Status Correction in Saudi Adults. Biology. 2022; 11(2):286. https://doi.org/10.3390/biology11020286
Chicago/Turabian StyleAldawsari, Ghadeer M., Shaun Sabico, Abir A. Alamro, Amal Alenad, Kaiser Wani, Abdullah M. Alnaami, Malak N. K. Khattak, Mohammad S. Masoud, Nasser M. Al-Daghri, and Majed S. Alokail. 2022. "Angiogenin Levels and Their Association with Cardiometabolic Indices Following Vitamin D Status Correction in Saudi Adults" Biology 11, no. 2: 286. https://doi.org/10.3390/biology11020286
APA StyleAldawsari, G. M., Sabico, S., Alamro, A. A., Alenad, A., Wani, K., Alnaami, A. M., Khattak, M. N. K., Masoud, M. S., Al-Daghri, N. M., & Alokail, M. S. (2022). Angiogenin Levels and Their Association with Cardiometabolic Indices Following Vitamin D Status Correction in Saudi Adults. Biology, 11(2), 286. https://doi.org/10.3390/biology11020286