
Modeling Vaccine Efficacy for COVID-19 Outbreak in New York City





Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
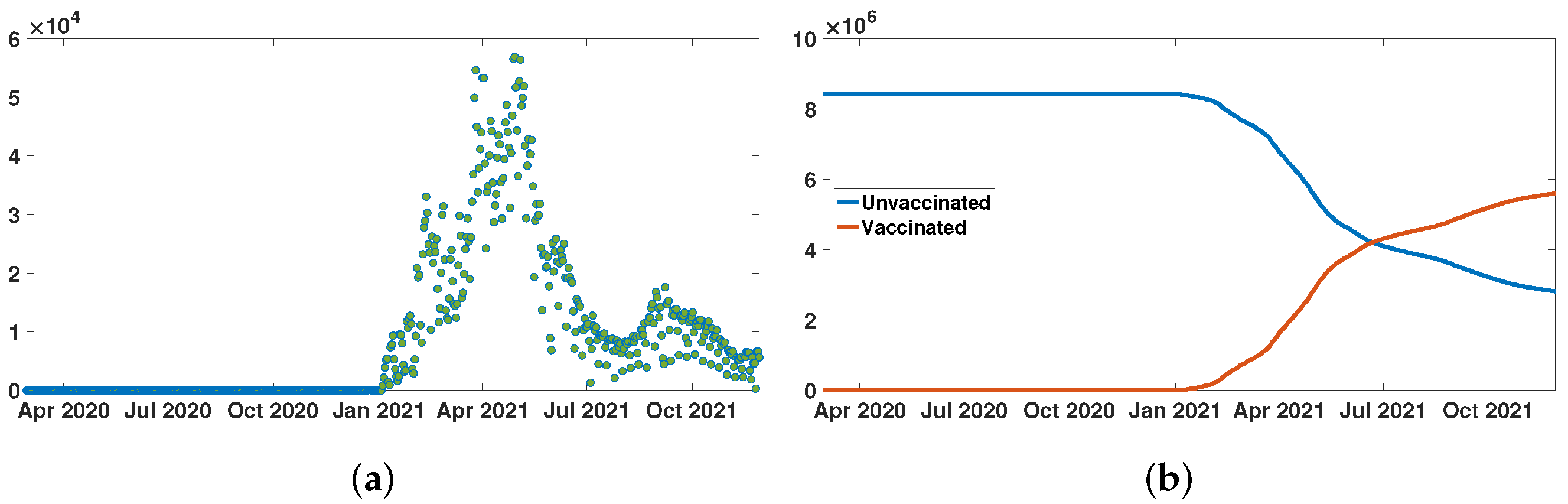
2.1. Data
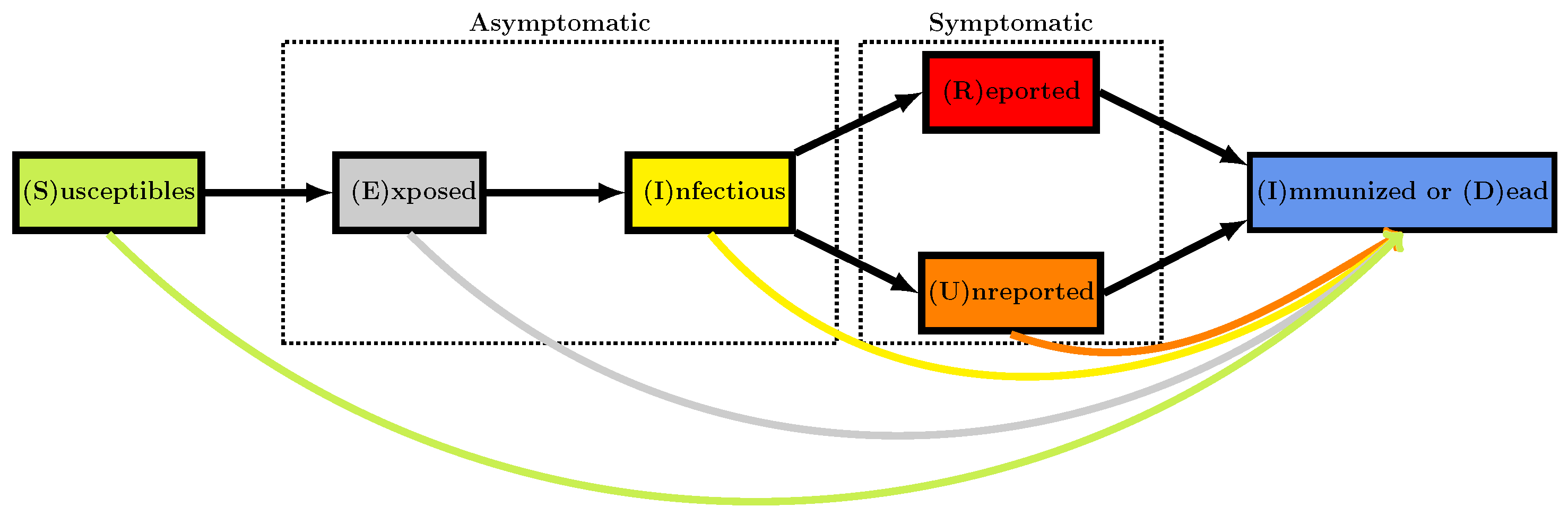
2.2. Epidemic Model
2.3. Equations of the SEIU Vaccination Model
- In the model, the data are represented by , the daily number of reported cases, and , the daily number of vaccinations.
- In order to compare the model and the data, it is assumed that the known parameters areThe three remaining parameters are estimated from the above quantities:
2.4. Identification Problem
- The transmission rate is fully determined by the parameters and by using the five following equations forwhere for ,where
- The data that are represented by the functions cumulative number of reported cases, and the cumulative number of second doses of vaccine are involved in the Formula (6) to define .
2.5. Data Normalized by
2.6. Phenomenological Model
2.7. Instantaneous Reproduction Numbers
3. Results
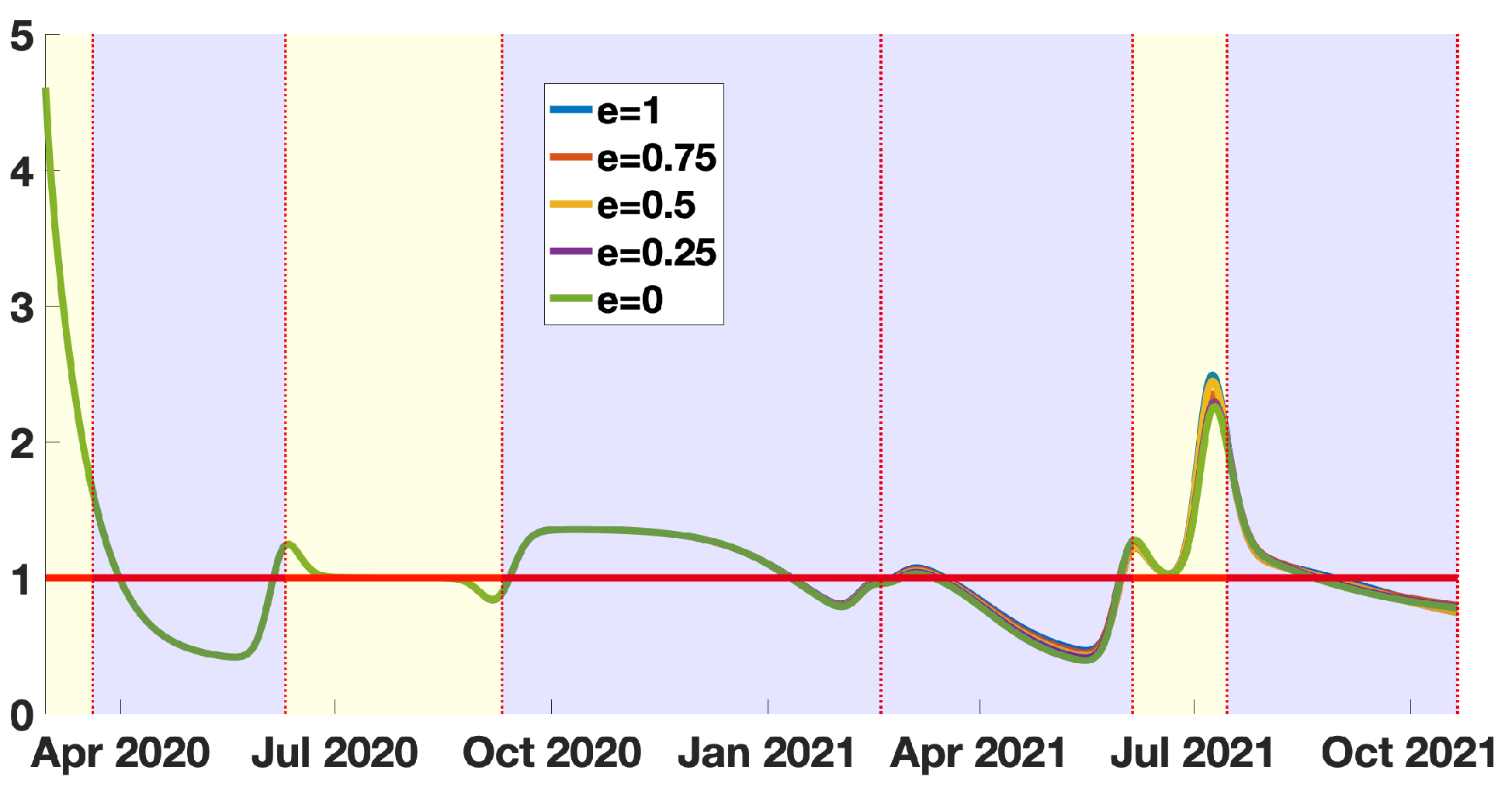
3.1. The Instantaneous Reproduction Number
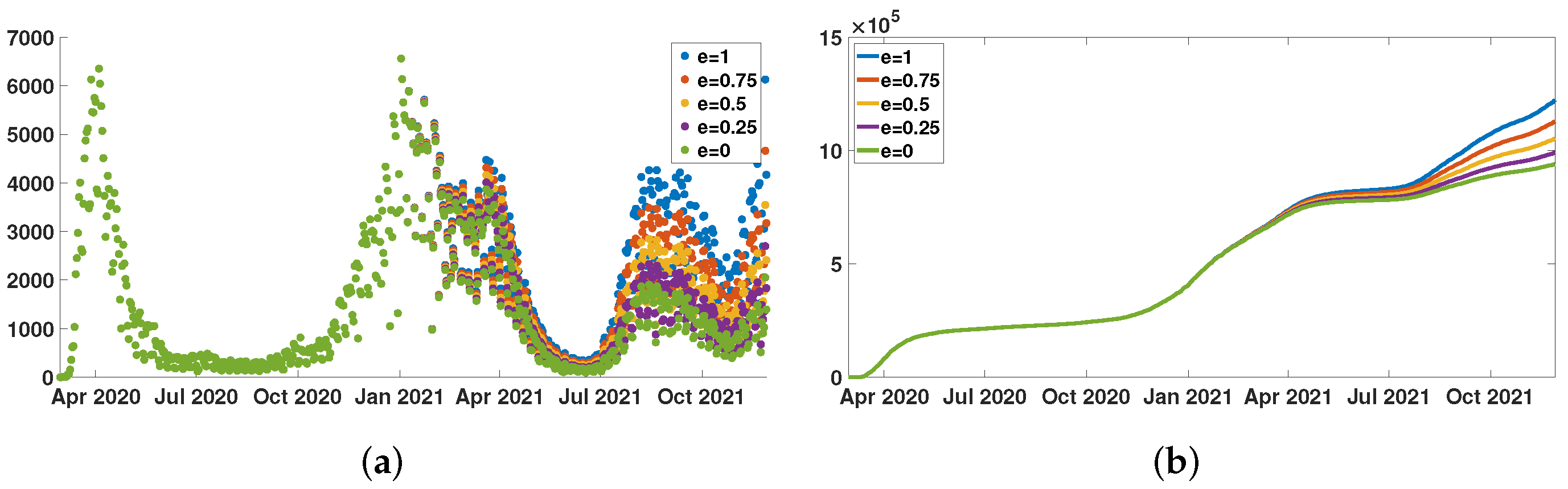
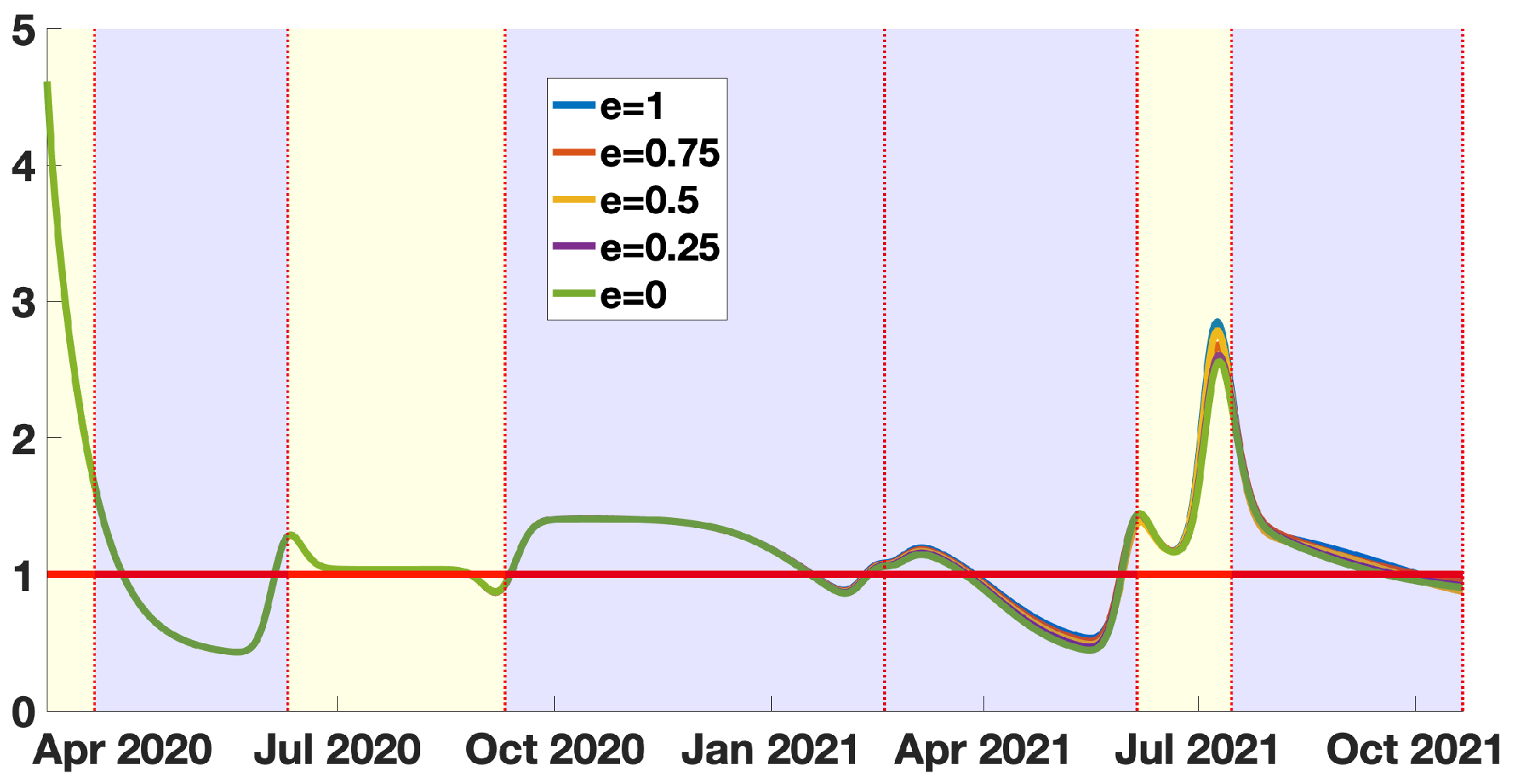
3.2. The Quasi-Instantaneous Reproduction Number
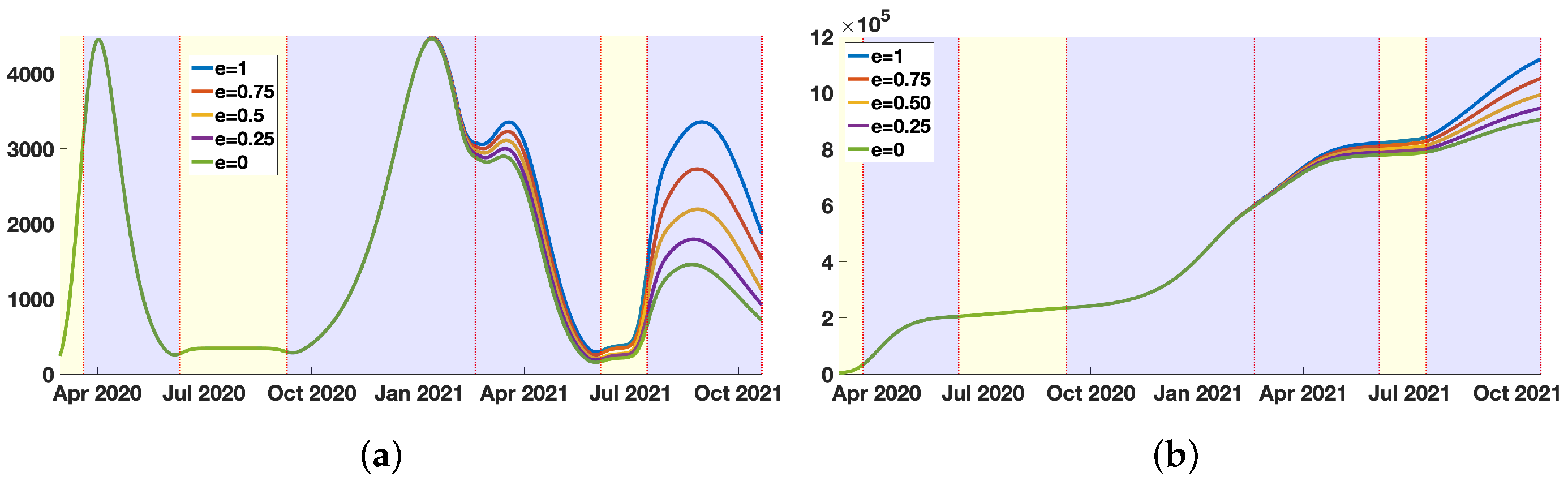
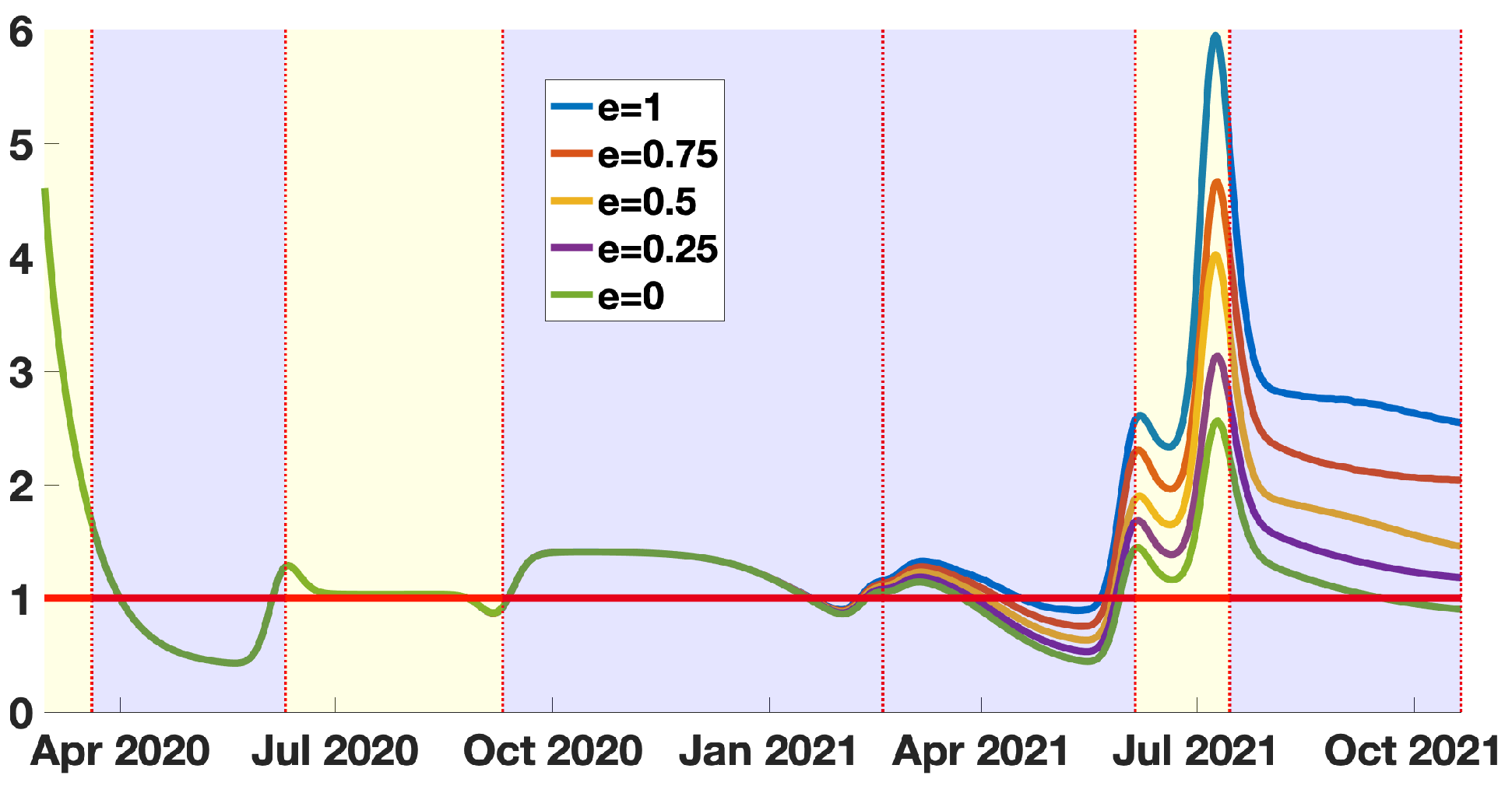
3.3. The Quasi-Instantaneous Reproduction Number without Vaccination
4. Discussion
4.1. Inclusion of Vaccination Data in the Model
4.2. Instantaneous and Quasi-Instantaneous Reproduction Numbers in the Model
4.3. Impact of Vaccination Policies in the Model
4.4. Extensions of the Model and Future Work
- (1)
- (2)
- In the development of mRNA vaccines, cross-immunity was overlooked entirely [29]. There are anti-coronavirus antibodies and many epitopes common to the various endemic known coronaviruses, conserved with SARS-CoV-2. Vaccination ignores pre-existing cross-immunity, which is unfortunate, as the doses injected could be adjusted for a response via cross-immunity against epitopes common to coronaviruses. Young individuals are those whose cross-immunity is still active, and it would be helpful to design a vaccination policy to obtain the best efficacy per target population at risk.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Transformation of the System into a System into a Standard Epidemic Model
Appendix B. Table of Parameters

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Period | Interpretation | Parameters Value | Method |
|---|---|---|---|
| Number of susceptible individuals at time | [32] | ||
| Number of exposed individuals at time | Computed | ||
| Number of asymptomatic infectious individuals at time | Computed | ||
| Number of unreported symptomatic infectious at time | 0 | Fixed | |
| Transmission rate | Computed | ||
| f | Fraction of reported symptomatic infectious | Fixed | |
| Fraction of unreported symptomatic infectious capable to transmit the pathogen | 1 | Fixed | |
| Average duration of the exposed period | 3 days | Fixed | |
| Average duration of the asymptomatic infectious period | 7 days | Fixed | |
| Average duration of the symptomatic infectious period | 7 days | Fixed | |
| e | Vaccine efficacy | Fixed |
References
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M. Waning of BNT162b2 vaccine protection against SARS-CoV-2 infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef] [PubMed]
- Puranik, A.; Lenehan, P.J.; Silvert, E.; Niesen, M.J.; Corchado-Garcia, J.; O’Horo, J.C. Comparison of two highly-effective mRNA vaccines for COVID-19 during periods of Alpha and Delta variant prevalence. MedRxiv 2021. [Google Scholar] [CrossRef]
- Anika, S.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B. 1.617. 2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet Infect. Dis. 2021, 22, 183–195. [Google Scholar]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Demongeot, J.; Griette, Q.; Magal, P. SI epidemic model applied to COVID-19 data in mainland China. R. Soc. Open Sci. 2020, 7, 201878. [Google Scholar] [CrossRef] [PubMed]
- Griette, Q.; Demongeot, J.; Magal, P. A robust phenomenological approach to investigate COVID-19 data for France. Math. Appl. Sci. Eng. 2021, 2, 149–218. [Google Scholar] [CrossRef]
- Griette, Q.; Demongeot, J.; Magal, P. What can we learn from COVID-19 data by using epidemic models with unidentified infectious cases? Math. Biosci. Eng. 2021, 19, 537–594. [Google Scholar] [CrossRef] [PubMed]
- Griette, Q.; Magal, P. Clarifying predictions for COVID-19 from testing data: The example of New York State. Infect. Dis. Model. 2021, 6, 273–283. [Google Scholar]
- Iboi, E.A.; Ngonghala, C.N.; Gumel, A.B. Will an imperfect vaccine curtail the COVID-19 pandemic in the US? Infect. Dis. Model. 2020, 5, 510–524. [Google Scholar] [PubMed]
- Li, Q.; Tang, B.; Bragazzi, N.L.; Xiao, Y.; Wu, J. Modeling the impact of mass influenza vaccination and public health interventions on COVID-19 epidemics with limited detection capability. Math. Biosci. 2020, 325, 108378. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Zhao, Y.; Chen, B.; He, D. Model Analysis of Vaccination Effectiveness by State in the United States. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3987537&download=yes (accessed on 16 December 2021).
- Moore, S.; Hill, E.; Dyson, L.; Tildesley, M.; Keeling, M. Modelling optimal vaccination strategy for SARS-CoV-2 in the UK. PLoS Comput. Biol. 2021, 17, e1008849. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Hill, E.; Tildesley, M.; Dyson, L.; Keeling, M. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Perra, N. Non-pharmaceutical interventions during the COVID-19 pandemic: A review. Phys. Rep. 2021, 913, 1–52. [Google Scholar] [CrossRef] [PubMed]
- Webb, G. A COVID-19 epidemic model predicting the effectiveness of vaccination. Math. Appl. Sci. Eng. 2021, 2, 134–148. [Google Scholar] [CrossRef]
- Webb, G. A COVID-19 epidemic model predicting the effectiveness of vaccination in the US. Infect. Dis. Rep. 2021, 13, 654–667. [Google Scholar] [CrossRef] [PubMed]
- New York City Department of Health and Mental Hygiene. Available online: https://www1.nyc.gov/site/doh/covid/covid-19-data.page (accessed on 17 December 2021).
- Wu, J.T.; Leung, K.; Bushman, M.; Kishore, N.; Niehus, R.; de Salazar, P.M. Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China. Nat. Med. 2020, 26, 506–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the transmission risk of the 2019-nCoV and its implication for public health interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.M.; May, R.M. Infectious Diseases of Humans: Dynamics and Control; Oxford University Press: Oxford, UK, 1992. [Google Scholar]
- Bailey, N.T.J. The Mathematical Theory of Epidemics; Hafner Publishing Co.: New York, NY, USA, 1957. [Google Scholar]
- Brauer, F.; van den Driessche, P.; Wu, J. Mathematical Epidemiology; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Brauer, F.; Castillo-Chavez, C. Mathematical Models in Population Biology and Epidemiology, 2nd ed.; Springer: New York, NY, USA, 2012. [Google Scholar]
- Brauer, F.; Castillo-Chavez, C.; Feng, Z. Mathematical Models in Epidemiology; Springer: New York, NY, USA, 2019. [Google Scholar]
- Busenberg, S.; Cooke, K. Vertically Transmitted Diseases; Springer: Berlin/Heidelberg, Germany, 1993. [Google Scholar]
- Diekmann, O.; Heesterbeek, H.; Britton, T. Mathematical Tools for Understanding Infectious Disease Dynamics; Princeton University Press: Princeton, NJ, USA, 2013. [Google Scholar]
- Murray, J.D. Mathematical Biology; Springer: Berlin/Heidelberg, Germany, 1989. [Google Scholar]
- Thieme, H.R. Mathematics in Population Biology; Princeton University Press: Princeton, NJ, USA, 2003. [Google Scholar]
- Simula, E.R.; Manca, M.A.; Jasemi, S.; Uzzau, S.; Rubino, S.; Manchia, P. HCoV-NL63 and SARS-CoV-2 share recognized epitopes by the humoral response in sera of people collected pre-and during CoV-2 pandemic. Microorganisms 2020, 8, 1993. [Google Scholar] [CrossRef] [PubMed]
- Yahi, N.; Chahinian, H.; Fantini, J. Infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants. A potential risk for mass vaccination? J. Infect. 2021, 83, 607–635. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, K.B.; Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Vihta, K.D. Effect of Delta variant on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. Nat. Med. 2021, 27, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- United States Census Bureau. Available online: https://www.census.gov/en.html (accessed on 17 December 2021).








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demongeot, J.; Griette, Q.; Magal, P.; Webb, G. Modeling Vaccine Efficacy for COVID-19 Outbreak in New York City. Biology 2022, 11, 345. https://doi.org/10.3390/biology11030345
Demongeot J, Griette Q, Magal P, Webb G. Modeling Vaccine Efficacy for COVID-19 Outbreak in New York City. Biology. 2022; 11(3):345. https://doi.org/10.3390/biology11030345
Chicago/Turabian StyleDemongeot, Jacques, Quentin Griette, Pierre Magal, and Glenn Webb. 2022. "Modeling Vaccine Efficacy for COVID-19 Outbreak in New York City" Biology 11, no. 3: 345. https://doi.org/10.3390/biology11030345
APA StyleDemongeot, J., Griette, Q., Magal, P., & Webb, G. (2022). Modeling Vaccine Efficacy for COVID-19 Outbreak in New York City. Biology, 11(3), 345. https://doi.org/10.3390/biology11030345