
Early-Stage Lung Tumor Detection Based on Super-Wideband Microwave Reflectometry



Abstract
:1. Introduction
- Studying the dielectric properties of human torso tissues over a super-wideband (SWB) frequency range.
- Custom designing antennas for SWB microwave reflectometry to detect early-stage lung tumors in deep-seated and superficial locations.
- Enhancing the resolution of reconstructed tumor images using backscattering datasets acquired over a super-wide frequency range.
- Demonstrating for the first time, the potential of SWB microwave reflectometry in precisely determining the size of early-stage tumors, even in deep locations.
2. Related Works
3. Investigation of Human Torso Dielectric Properties
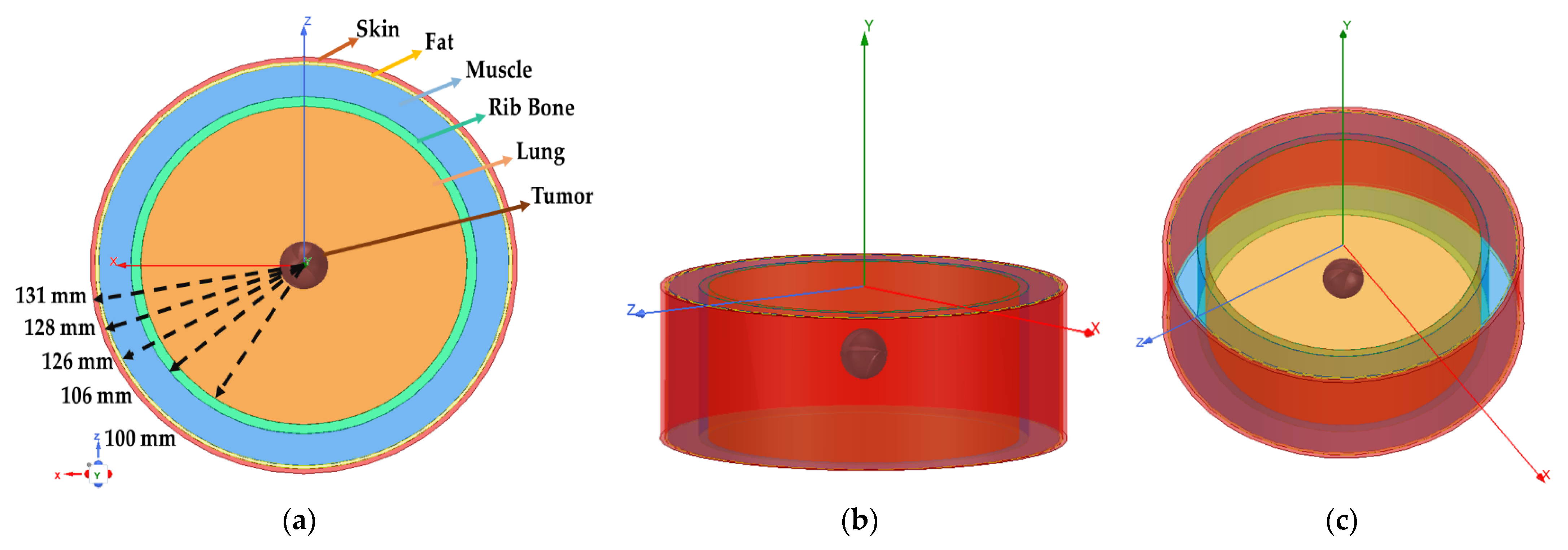
4. Modeling of Human Lung Phantom
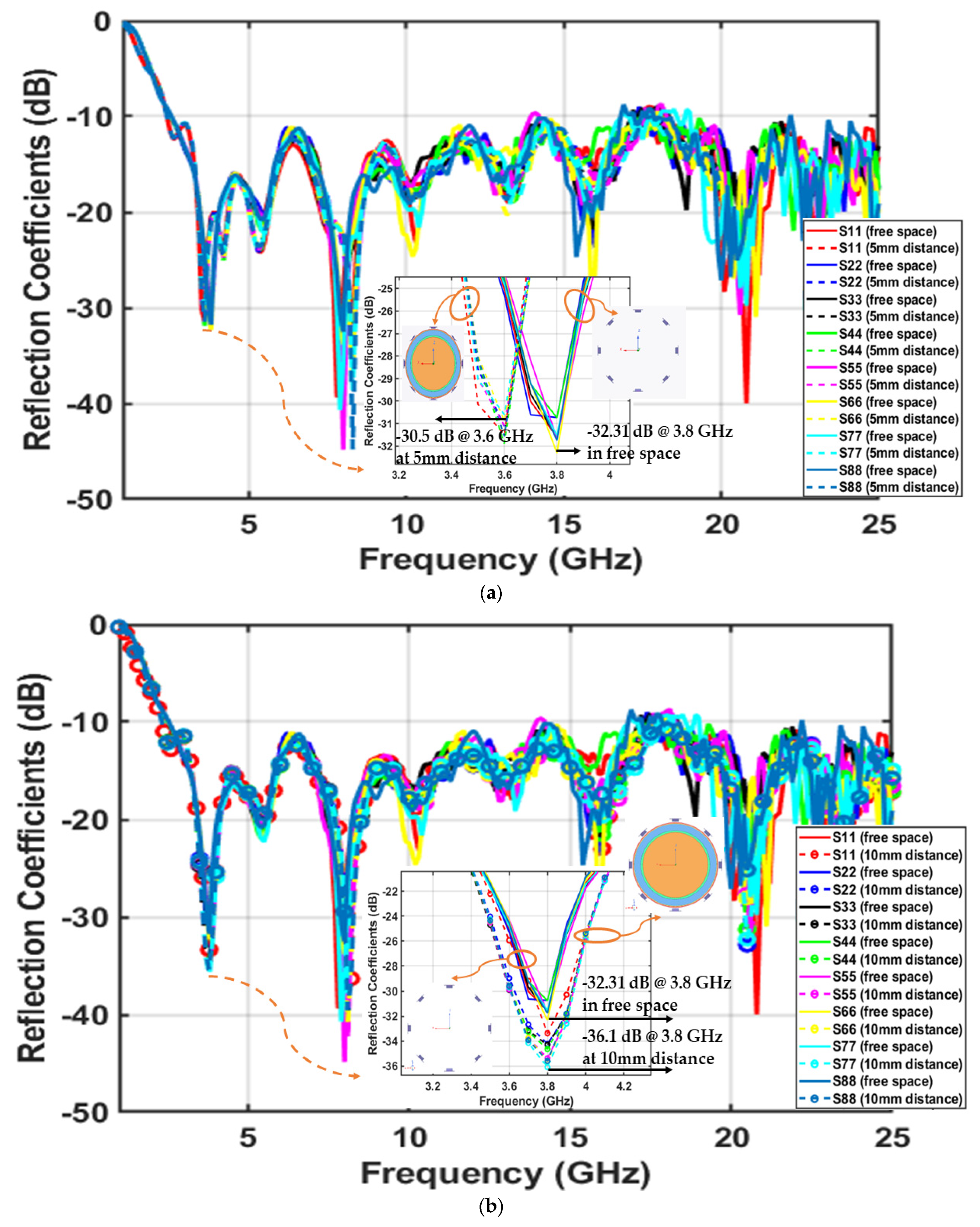
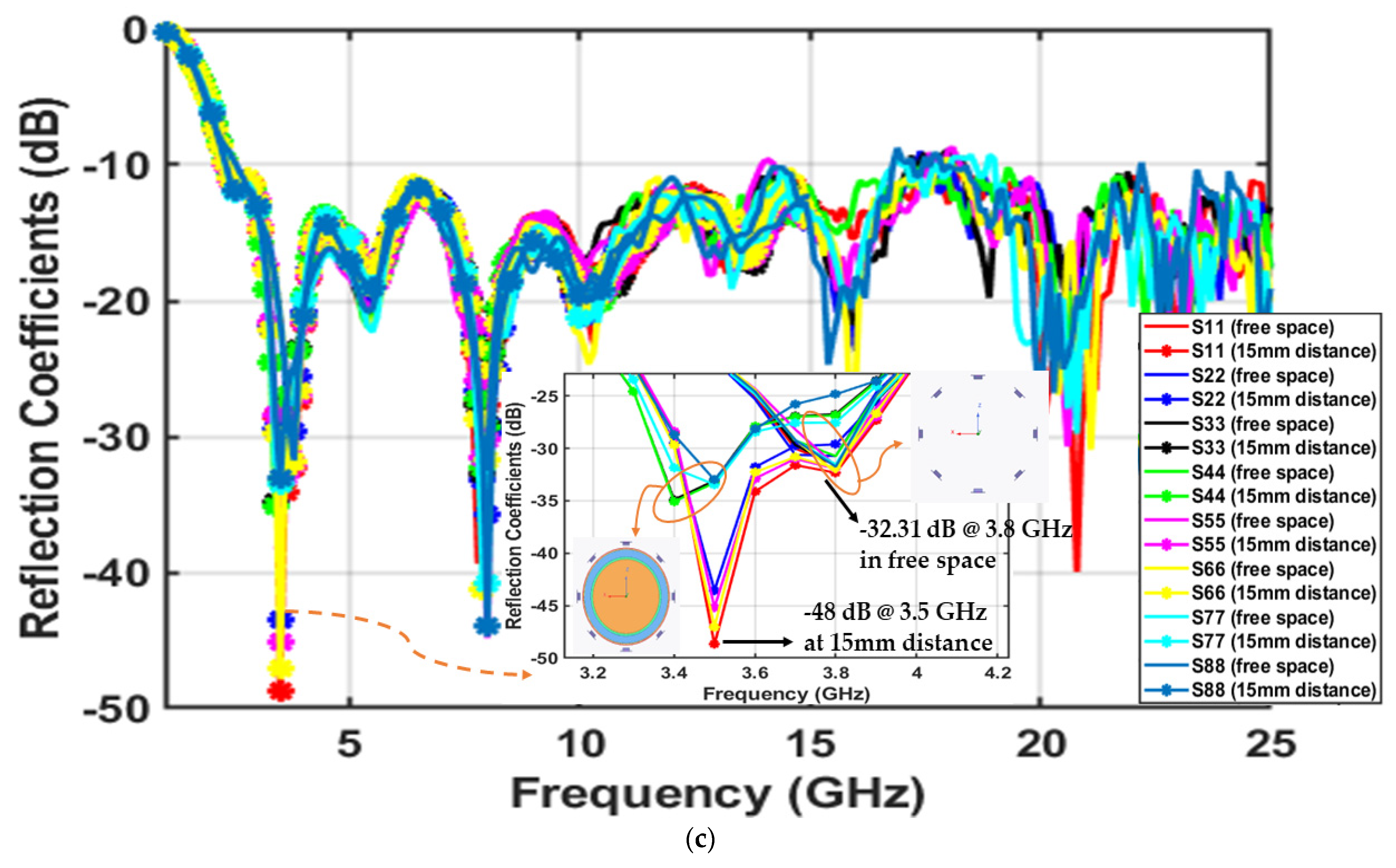
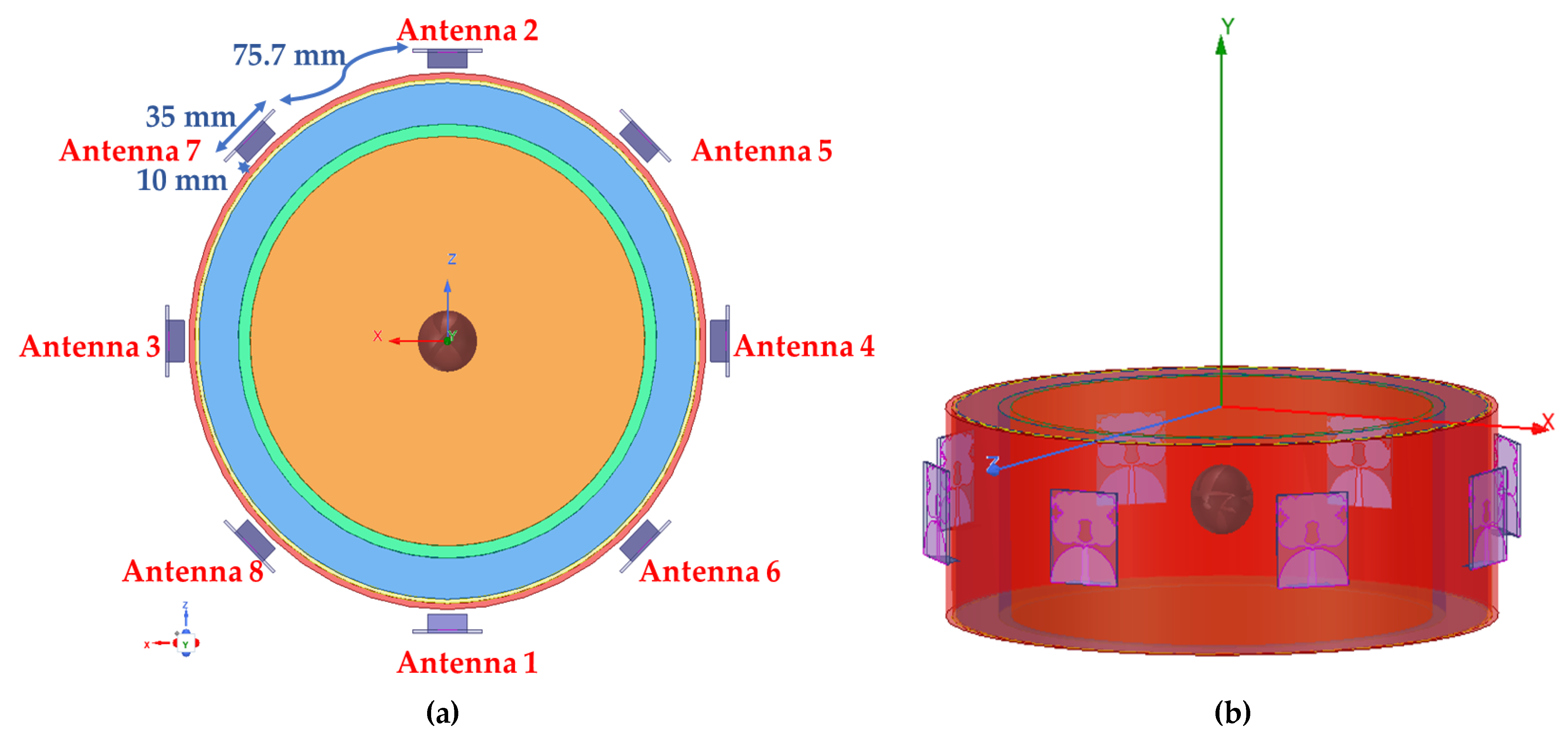
5. Lung Anomaly Detection Based on SWB Microwave Reflectometry
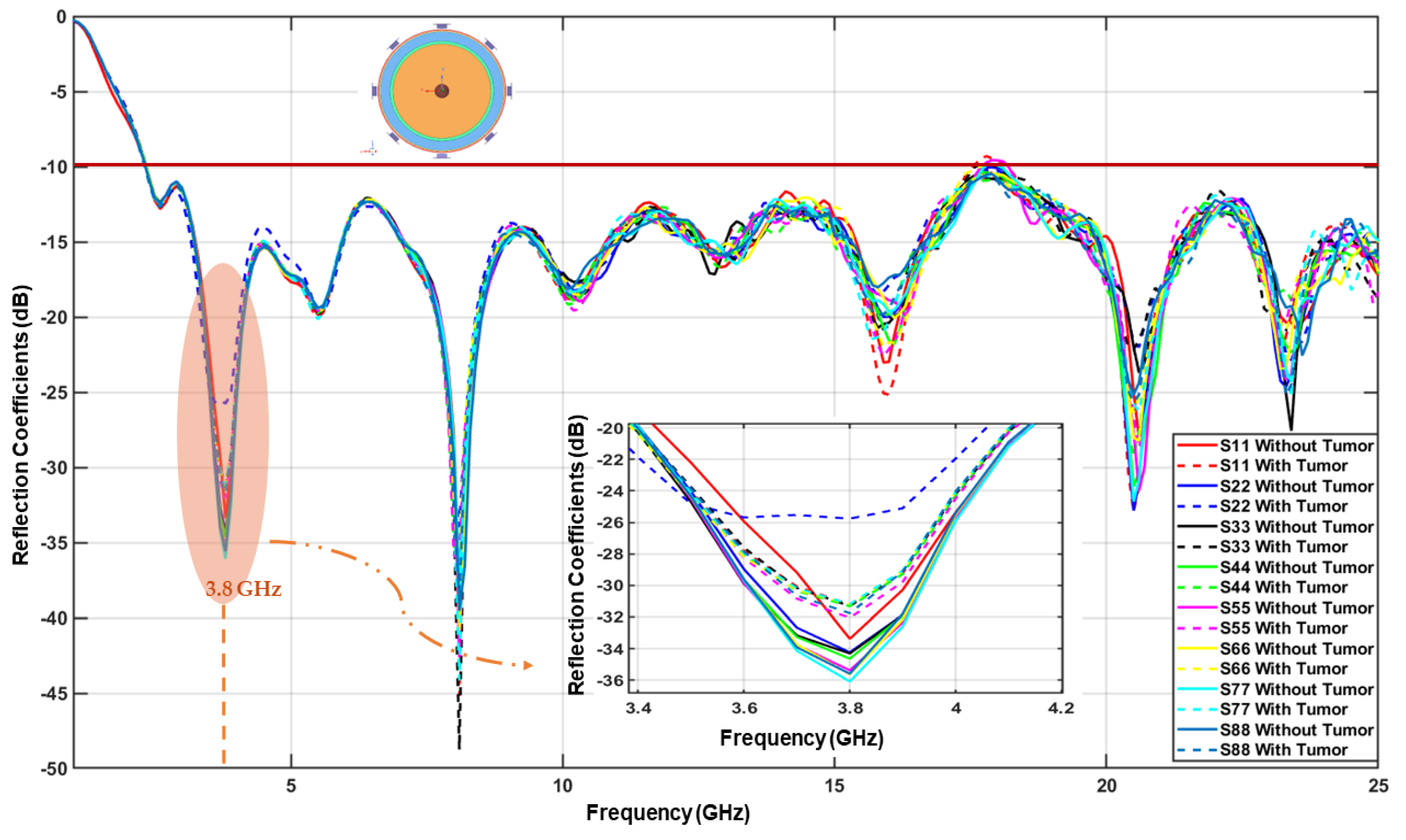
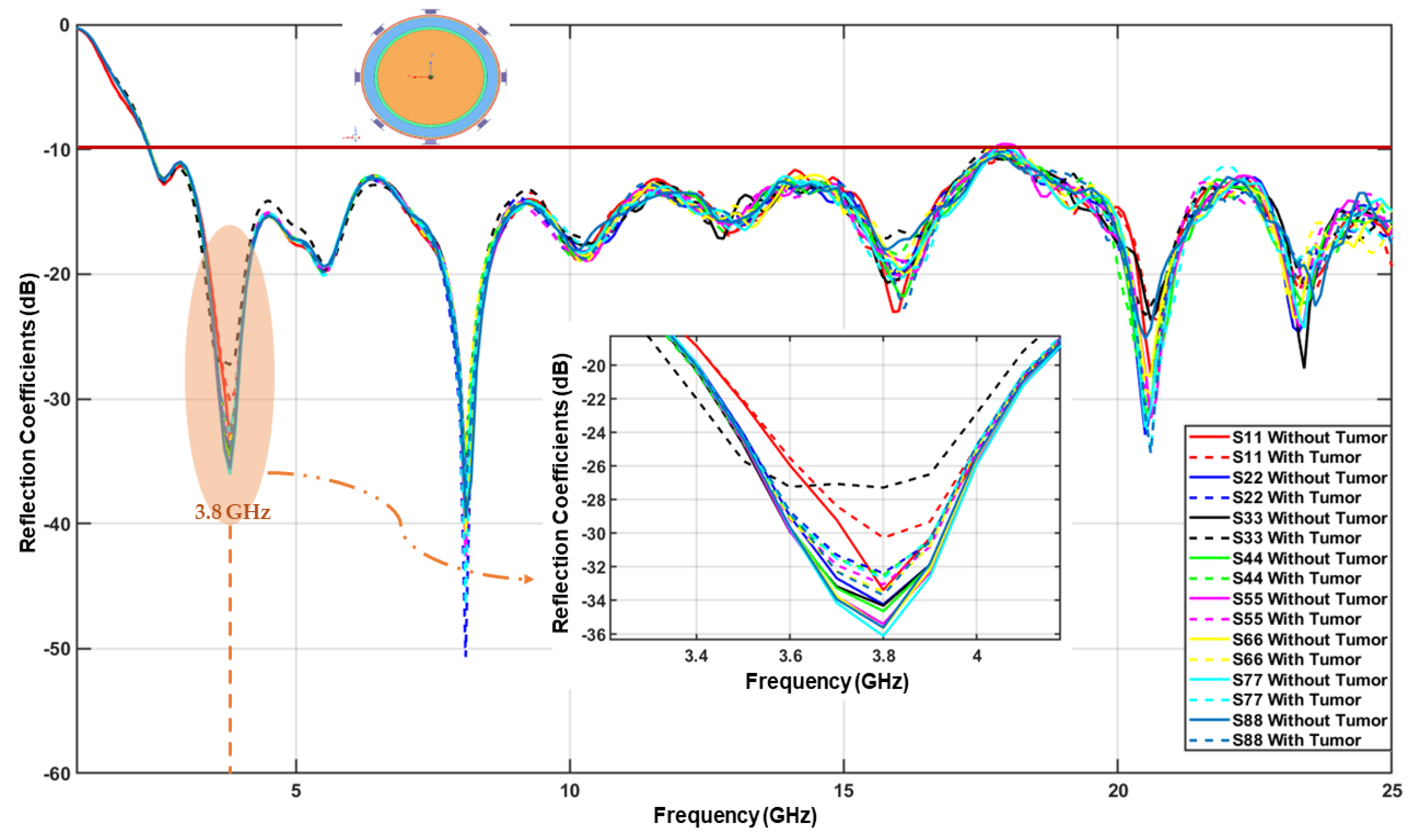
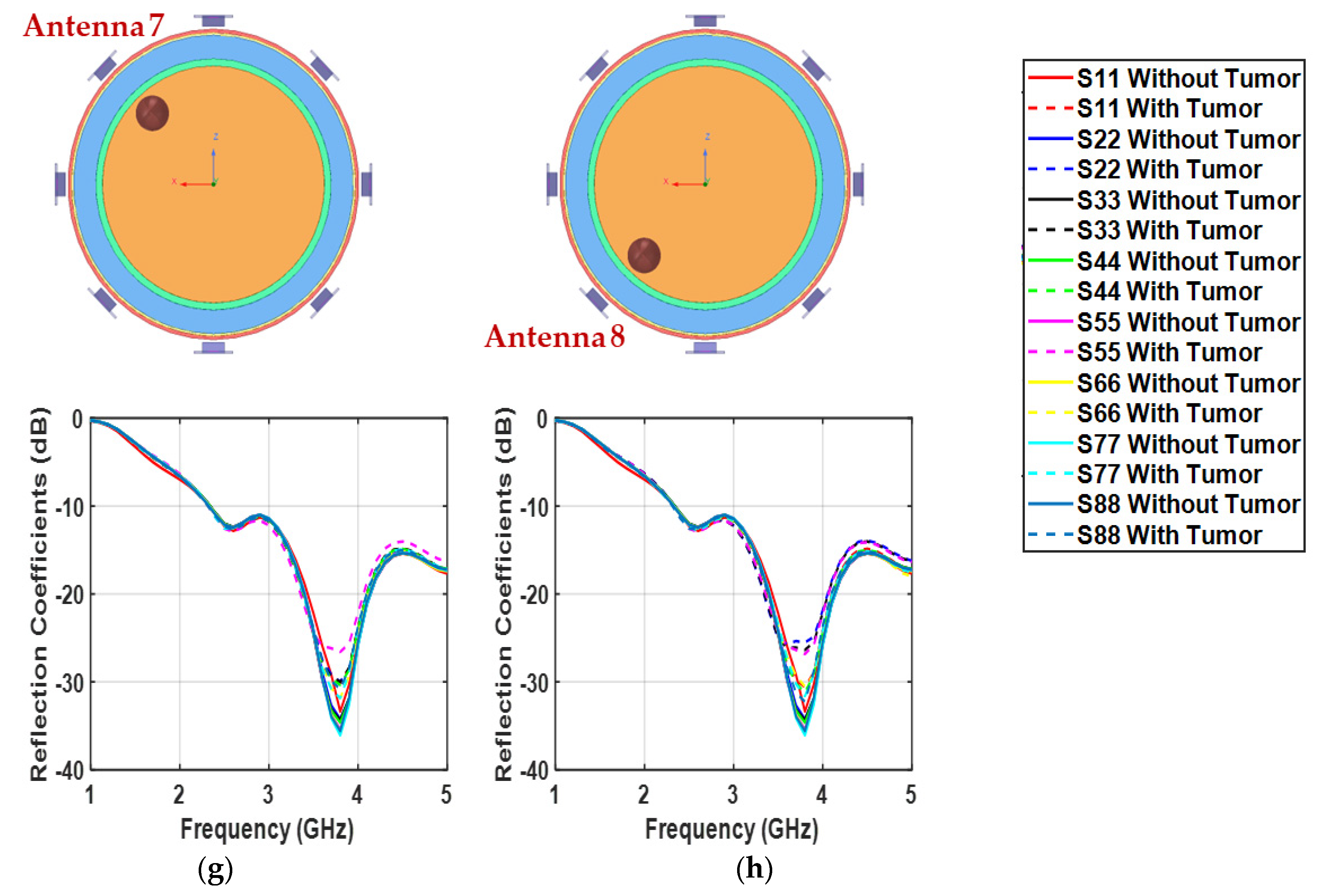
5.1. Detection of Deep-Seated Lung Tumor
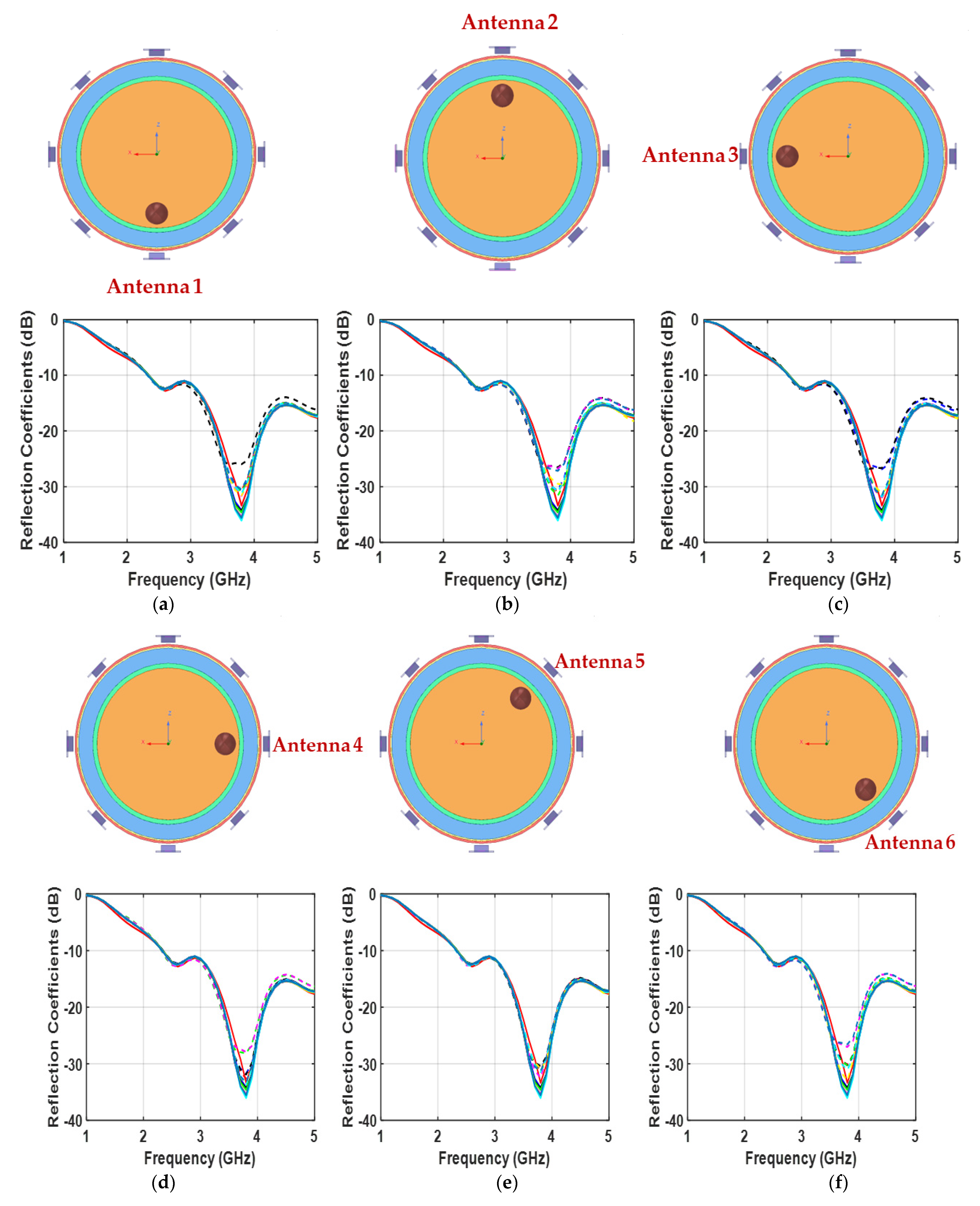
5.2. Detection of Superficially-Located Lung Tumor
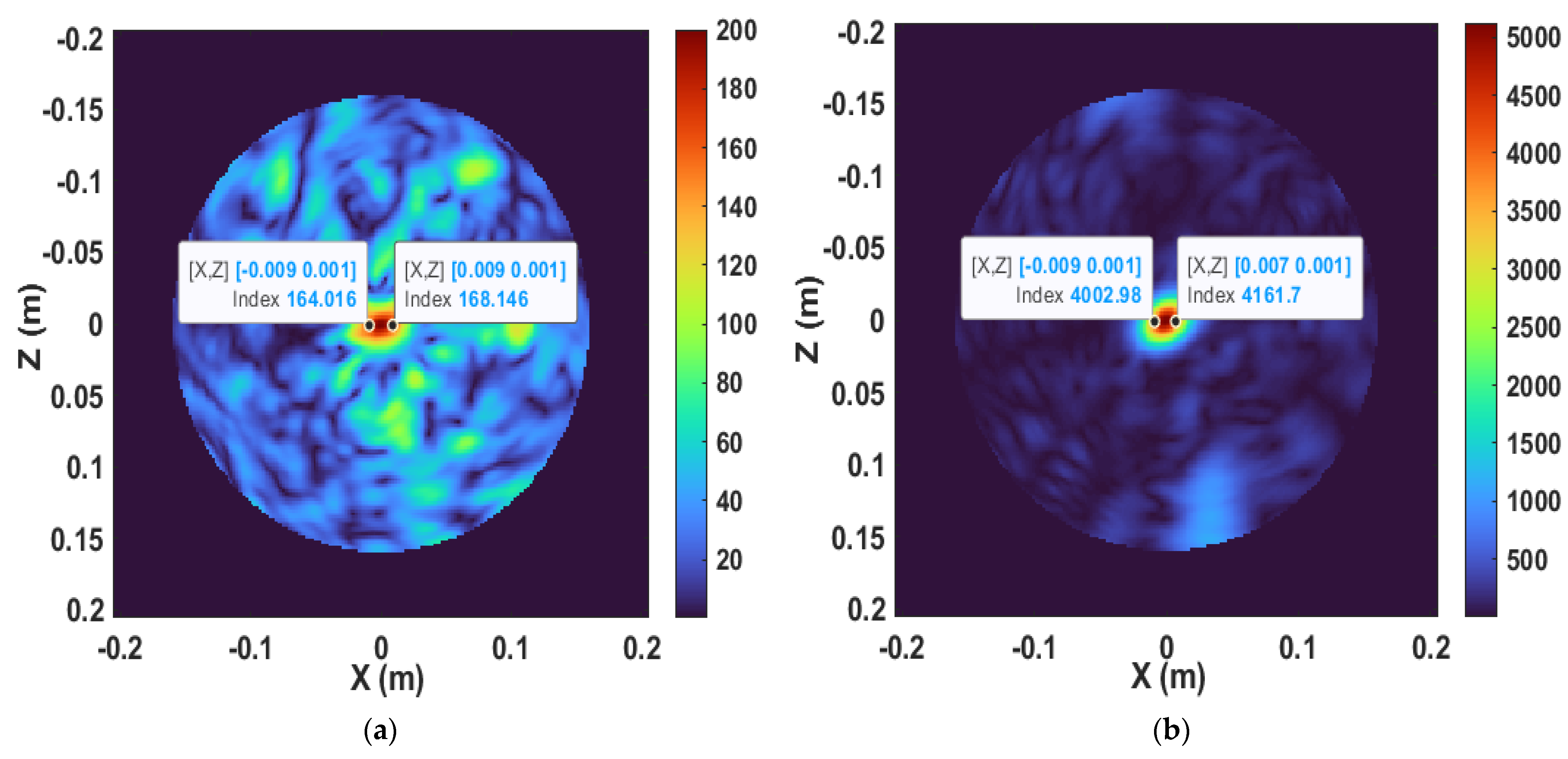
6. Reconstructed Imaging Results
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Beckert, L.; Laking, G. All the cancer you cannot see. N. Z. Med. J. 2022, 135, 8–10. [Google Scholar] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Bao, N.; Chen, Y.; Liu, Y.; Chakraborty, C. Multi-objective path planning for lung biopsy surgery. Multimed. Tools Appl. 2022, 81, 36153–36170. [Google Scholar] [CrossRef]
- Alamro, W.; Seet, B.-C. Review of practical antennas for microwave and millimetre-wave medical imaging. In Electromagnetic Waves and Antennas for Biomedical Applications, 1st ed.; Wang, L., Ed.; IET: London, UK, 2021; pp. 185–207. [Google Scholar]
- Wang, L. Multi-Frequency Holographic Microwave Imaging for Breast Lesion Detection. IEEE Access 2019, 7, 83984–83993. [Google Scholar] [CrossRef]
- Porter, E.; Bahrami, H.; Santorelli, A.; Gosselin, B.; Rusch, L.A.; Popovic, M. A Wearable Microwave Antenna Array for Time-Domain Breast Tumor Screening. IEEE Trans. Med. Imaging 2016, 35, 1501–1509. [Google Scholar] [CrossRef] [Green Version]
- Wang, L. Terahertz Imaging for Breast Cancer Detection. Sensors 2021, 21, 6465. [Google Scholar] [CrossRef]
- Wang, L. Three-Dimensional Holographic Electromagnetic Imaging for Accessing Brain Stroke. Sensors 2018, 18, 3852. [Google Scholar] [CrossRef] [Green Version]
- Tobon Vasquez, J.A.; Scapaticci, R.; Turvani, G.; Bellizzi, G.; Rodriguez-Duarte, D.O.; Joachimowicz, N.; Duchêne, B.; Tedeschi, E.; Casu, M.R.; Crocco, L.; et al. A Prototype Microwave System for 3D Brain Stroke Imaging. Sensors 2020, 20, 2607. [Google Scholar] [CrossRef]
- Sohani, B.; Khalesi, B.; Ghavami, N.; Ghavami, M.; Dudley, S.; Rahmani, A.; Tiberi, G. Detection of haemorrhagic stroke in simulation and realistic 3-D human head phantom using microwave imaging. Biomed. Signal Process. Control 2020, 61, 102001. [Google Scholar] [CrossRef]
- Inum, R.; Rana, M.; Shushama, K.N.; Quader, A. EBG Based Microstrip Patch Antenna for Brain Tumor Detection via Scattering Parameters in Microwave Imaging System. Int. J. Biomed. Imaging 2018, 2018, 12. [Google Scholar] [CrossRef]
- Darvazehban, A.; Rezaeieh, S.A.; Zamani, A.; Abbosh, A.M. Pattern Reconfigurable Metasurface Antenna for Electromagnetic Torso Imaging. IEEE Trans. Antennas Propag. 2019, 67, 5453–5462. [Google Scholar] [CrossRef]
- Darvazehban, A.; Rezaeieh, S.A.; Abbosh, A. Pattern-Reconfigurable Loop–Dipole Antenna for Electromagnetic Pleural Effusion Detection. IEEE Trans. Antennas Propag. 2020, 68, 5955–5964. [Google Scholar] [CrossRef]
- Rezaeieh, S.A.; Zamani, A.; Bialkowski, K.S.; Mahmoud, A.; Abbosh, A.M. Feasibility of Using Wideband Microwave System for Non-Invasive Detection and Monitoring of Pulmonary Oedema. Sci. Rep. 2015, 5, 14047. [Google Scholar] [CrossRef] [Green Version]
- Mirbeik-Sabzevari, A.; Li, S.; Garay, E.; Nguyen, H.-T.; Wang, H.; Tavassolian, N. Synthetic Ultra-High-Resolution Millimeter-Wave Imaging for Skin Cancer Detection. IEEE Trans. Biomed. Eng. 2018, 66, 61–71. [Google Scholar] [CrossRef]
- Tripathi, A.C.; Rao, P.K.; Mishra, R. An AMC Inspired Wearable UWB Antenna for Skin Cancer Detection. In Proceedings of the International Conference on Electrical and Electronics Engineering (ICE3), Gorakhpur, India, 14–15 February 2020. [Google Scholar]
- Rodriguez-Duarte, D.O.; Vasquez, J.A.T.; Scapaticci, R.; Crocco, L.; Vipiana, F. Brick-Shaped Antenna Module for Microwave Brain Imaging Systems. IEEE Antennas Wirel. Propag. Lett. 2020, 19, 2057–2061. [Google Scholar] [CrossRef]
- Zamani, A.; Rezaeieh, S.A.; Abbosh, A.M. Lung cancer detection using frequency domain microwave imaging. Electron. Lett. 2015, 51, 740–741. [Google Scholar] [CrossRef]
- Ahmed, A.; Kumari, V.; Sheoran, G. Experimental investigation of microwave holographic reflectometry for lung tumor detection. Measurement 2022, 197, 111336. [Google Scholar] [CrossRef]
- Khalesi, B.; Khalid, B.; Ghavami, N.; Raspa, G.; Ghavami, M.; Dudley-McEvoy, S.; Tiberi, G. A Microwave Imaging Procedure for Lung Lesion Detection: Preliminary Results on Multilayer Phantoms. Electronics 2022, 11, 2105. [Google Scholar] [CrossRef]
- Alhawari, A.R.H. Lung Tumour Detection Using Ultra-Wideband Microwave Imaging Approach. J. Fundam. Appl. Sci. 2018, 10, 222–234. [Google Scholar]
- Ameer, W.; Awan, D.; Bashir, S.; Waheed, A. Use of Directional UWB Antenna for Lung Tumor Detection. In Proceedings of the 2nd International Conference on Advancements in Computational Sciences (ICACS), Lahore, Pakistan, 18–20 February 2019. [Google Scholar]
- Abdelhamid, M.M.; Allam, A.M. Detection of Lung Cancer Using Ultra Wide Band Antenna. In Proceedings of the 2016 Loughborough Antennas & Propagation Conference (LAPC), Loughborough, UK, 14–15 November 2016. [Google Scholar]
- Alani, S.; Zakaria, Z.; Saeidi, T.; Ahmad, A.; Imran, M.A.; Abbasi, Q.H. Microwave Imaging of Breast Skin Utilizing Elliptical UWB Antenna and Reverse Problems Algorithm. Micromachines 2021, 12, 647. [Google Scholar] [CrossRef]
- Bahramiabarghouei, H.; Porter, E.; Santorelli, A.; Gosselin, B.; Popovic, M.; Rusch, L.A. Flexible 16 Antenna Array for Microwave Breast Cancer Detection. IEEE Trans. Biomed. Eng. 2015, 62, 10. [Google Scholar] [CrossRef] [PubMed]
- Hossain, K.; Sabapathy, T.; Jusoh, M.; Lee, S.-H.; Rahman, K.S.A.; Kamarudin, M.R. Negative Index Metamaterial-Based Frequency-Reconfigurable Textile CPW Antenna for Microwave Imaging of Breast Cancer. Sensors 2022, 22, 1626. [Google Scholar] [CrossRef] [PubMed]
- Hossain, A.; Islam, M.T.; Islam, M.T.; Chowdhury, M.E.H.; Rmili, H.; Samsuzzaman, M. A Planar Ultrawideband Patch Antenna Array for Microwave Breast Tumor Detection. Materials 2020, 13, 4918. [Google Scholar] [CrossRef] [PubMed]
- Shahidul Islam, M.; Islam, M.T.; Hoque, A.; Islam, M.T.; Amin, N.; Chowdhury, M.E.H. A Portable Electromagnetic Head Imaging System Using Metamaterial Loaded Compact Directional 3D Antenna. IEEE Access 2021, 9, 50893–50906. [Google Scholar] [CrossRef]
- Bashri, M.S.R.; Arslan, T. Low-cost and compact RF switching system for wearable microwave head imaging with performance verification on artificial head phantom. IET Microw. Antennas Propag. 2018, 12, 706–711. [Google Scholar] [CrossRef] [Green Version]
- Kaur, K.; Kaur, A. In vitro detection of skin cancer using an UWB stacked micro strip patch antenna with microwave imaging. Int. J. RF Microw. Comput. Eng. 2022, 32, e23407. [Google Scholar] [CrossRef]
- Khan, M.A.; Rafique, U.; Savci, H.Ş.; Nordin, A.N.; Kiani, S.H.; Abbas, S.M. Ultra-Wideband Pentagonal Fractal Antenna with Stable Radiation Characteristics for Microwave Imaging Applications. Electronics 2022, 11, 2061. [Google Scholar] [CrossRef]
- Ullah, S.; Ruan, C.; Sadiq, M.S.; Haq, T.U.; He, W. High Efficient and Ultra Wide Band Monopole Antenna for Microwave Imaging and Communication Applications. Sensors 2020, 20, 115. [Google Scholar] [CrossRef] [Green Version]
- Balani, W.; Sarvagya, M.; Samasgikar, A.; Ali, T.; Kumar, P. Design and Analysis of Super Wideband Antenna for Microwave Applications. Sensors 2021, 21, 477. [Google Scholar] [CrossRef]
- Chew, K.M.; Sudirman, R.; Seman, N.; Yong, C.Y. Reflection coefficient detection of simulation models for microwave imaging simulation system. Biomed. Mater. Eng. 2014, 24, 199–207. [Google Scholar] [CrossRef]
- Mohammed, B.J.; Abbosh, A.M.; Ireland, D. Stroke detection based on variations in reflection coefficients of wideband antennas. In Proceedings of the IEEE International Symposium on Antennas and Propagation, Chicago, IL, USA, 8–14 July 2012. [Google Scholar]
- Hasgall, P.A.; Neufeld, E.; Gosselin, M.C.; Klingenböck, A.; Kuster, N.; Kuster, N.; Hasgall, P.; Gosselin, M. IT’IS Database for Thermal and Electromagnetic Parameters of Biological Tissues, Version 4.0; Science Open: Berlin, Germany, 2018. [Google Scholar]
- Gabriel, C.; Gabriel, S.; Corthout, E. The dielectric properties of biological tissues: I. literature survey. Phys. Med. Biol. 1996, 41, 2231–2249. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Wake, K.; Watanabe, S. Development of best fit Cole-Cole parameters for measurement data from biological tissues and organs between 1 MHz and 20 GHz. Radio Sci. 2014, 49, 459–472. [Google Scholar] [CrossRef]
- Xuyang, L. Body Matched Antennas for Microwave Medical Applications. In Karlsruher Forschungsberichte aus dem Institut fuer Hochfrequenztechnik und Elektronik; KIT Scientific Publishing: Karlsruhe, Germany, 2014; Volume 72. [Google Scholar]
- Alamro, W.; Seet, B.-C.; Wang, L.; Parthiban, P. Compact Super-Wideband Antenna for Medical Imaging Applications. In Proceedings of the IEEE Conference on Antenna Measurements & Applications (CAMA), Antibes Juan-les-Pins, France, 15–17 November 2021. [Google Scholar]
- Elahi, M.A.; O’Loughlin, D.; Lavoie, B.R.; Glavin, M.; Jones, E.; Fear, E.C.; O’Halloran, M. Evaluation of Image Reconstruction Algorithms for Confocal Microwave Imaging: Application to Patient Data. Sensors 2018, 18, 1678. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, D.; Elahi, M.A.; Porter, E.; Shahzad, A.; Oliveira, B.L.; Glavin, M.; Jones, E.; O’Halloran, M. Open-Source Software for Microwave Radar-Based Image Reconstruction. In Proceedings of the 12th European Conference on Antennas and Propagation (EuCAP), London, UK, 9–13 April 2018. [Google Scholar]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue | σ | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Skin | 4 | 39 | 7.96 | 0.1 | 2.8 | 79.58 | 0 | 3 | 1.59 | 0.16 | 0.03 | 1.592 | 0.2 | 0.4 |
| Fat | 2.5 | 3 | 7.96 | 0.2 | 0.15 | 15.92 | 0.1 | 3.3 | 159.15 | 0.05 | 10 | 7.958 | 0.01 | 10 |
| Muscle | 4 | 50 | 7.23 | 0.1 | 70 | 353.6 | 0.1 | 120 | 318.31 | 0.1 | 25 | 2.274 | 0 | 200 |
| Rib bone | 2.5 | 18 | 13.3 | 0.22 | 3 | 79.58 | 0.25 | 2 | 159.15 | 0.2 | 20 | 15.91 | 0 | 700 |
| Lung | 4.44 | 14.6 | 16.1 | 0.0001 | 6.46 | 3.22 | 0.181 | 2.2 | 159.15 | 0.18 | 10 | 7.958 | 0 | 84.2 |
| Tissue | Thickness (mm) | Relative Dielectric Constant εr | Conductivity σ (S/m) | tan δ |
|---|---|---|---|---|
| Skin | 3 | 36.8 | 2.15 | 0.283 |
| Fat | 2 | 10.4 | 0.453 | 0.211 |
| Muscle | 20 | 51.2 | 2.74 | 0.259 |
| Rib Bone | 6 | 17.2 | 1.28 | 0.361 |
| Lung | 100 | 19.7 | 1.21 | 0.298 |
| Tumor | 5–15 (radius) | 61.8 | 5.454 | 0.428 |
| Reflection Coefficient | Healthy Phantom | With 15 mm Tumor (|∆|) | With 5 mm Tumor (|∆|) |
|---|---|---|---|
| |S11| | −33.37 | −31.20 (2.17) | −30.26 (3.11) |
| |S22| | −34.23 | −25.70 (8.53) | −32.37 (1.86) |
| |S33| | −34.30 | −31.30 (3.00) | −27.27 (7.03) |
| |S44| | −34.63 | −31.32 (3.31) | −32.49 (2.14) |
| |S55| | −35.37 | −32.05 (3.32) | −33.05 (2.32) |
| |S66| | −35.62 | −31.19 (4.43) | −33.48 (2.14) |
| |S77| | −36.10 | −31.18 (4.92) | −32.68 (3.42) |
| |S88| | −35.60 | −31.76 (3.84) | −33.68 (1.92) |
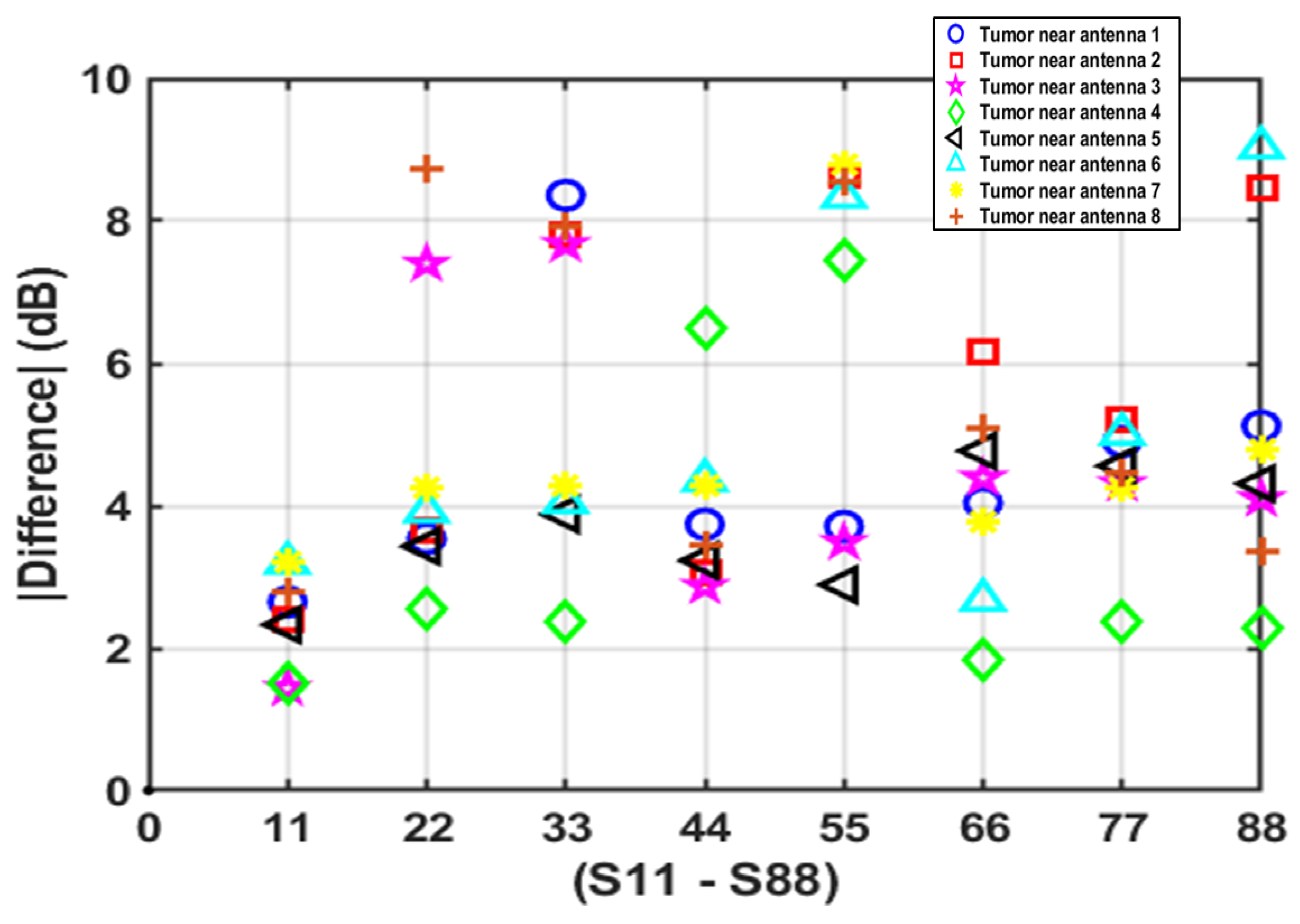
| ∆ Reflection Coefficient | Case 1 (dB) | Case 2 (dB) | Case 3 (dB) | Case 4 (dB) | Case 5 (dB) | Case 6 (dB) | Case 7 (dB) | Case 8 (dB) |
|---|---|---|---|---|---|---|---|---|
| |∆S11| | 2.65 | 2.40 | 1.44 | 1.5 | 2.33 | 3.2 | 3.22 | 2.78 |
| |∆S22| | 3.54 | 3.65 | 7.4 | 2.55 | 3.43 | 3.92 | 4.26 | 8.72 |
| |∆S33| | 8.36 | 7.81 | 7.67 | 2.37 | 3.88 | 4.05 | 4.28 | 7.94 |
| |∆S44| | 3.74 | 3.07 | 2.87 | 6.49 | 3.23 | 4.36 | 4.29 | 3.45 |
| |∆S55| | 3.71 | 8.65 | 3.49 | 7.45 | 2.89 | 8.34 | 8.79 | 8.55 |
| |∆S66| | 4.04 | 6.15 | 4.39 | 1.84 | 4.77 | 2.68 | 3.79 | 5.10 |
| |∆S77| | 4.9 | 5.20 | 4.31 | 2.38 | 4.56 | 5.01 | 4.25 | 4.47 |
| |∆S88| | 5.12 | 8.47 | 4.1 | 2.27 | 4.31 | 9.03 | 4.8 | 3.35 |
| Real Tumor Radius | Predicted Radius (DAS) | Predicted Radius (DMAS) | MAPE (DAS) | MAPE (DMAS) |
|---|---|---|---|---|
| 5 mm | 9 mm | 8 mm | 80% | 60% |
| 15 mm | 16 mm | 14 mm | 6.66% | 6.66% |
| Ref. | Freq. (GHz) | Tumor Size | Type of Antenna(s) Deployed | Tumor Detection Depth | Tumor Detection Accuracy |
|---|---|---|---|---|---|
| [17] | 1.5−3 | 10 mm radius | 1× rotated antenna around the phantom | N/A | Accurate |
| [18] | 10 | 5 mm radius | 2× Vivaldi antenna | Superficial (60 mm) | Weak detection |
| [19] | 1–5 | 15 mL (tube-shaped) | 2× horn TX antenna, 2× Vivaldi RX antenna | Superficial (50 mm) | Accurate |
| [20] | 3–4 | 4, 10 mm radius | 1× circular shaped antenna | 60 mm | Weak detection |
| [21] | 3–10.7 | N/A | 2× elliptical shaped antenna | 70 mm | Weak detection |
| [22] | 2.9–12 | N/A | 1× cupcake shaped antenna | N/A | Weak detection |
| This work | 2.45–25 | 5, 15 mm radius | 8× custom-designed SWB array element around the phantom | Deep-seated (141 mm) Superficial (61 mm) | Accurate with size measurement capability |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alamro, W.; Seet, B.-C.; Wang, L.; Parthiban, P. Early-Stage Lung Tumor Detection Based on Super-Wideband Microwave Reflectometry. Electronics 2023, 12, 36. https://doi.org/10.3390/electronics12010036
Alamro W, Seet B-C, Wang L, Parthiban P. Early-Stage Lung Tumor Detection Based on Super-Wideband Microwave Reflectometry. Electronics. 2023; 12(1):36. https://doi.org/10.3390/electronics12010036
Chicago/Turabian StyleAlamro, Wasan, Boon-Chong Seet, Lulu Wang, and Prabakar Parthiban. 2023. "Early-Stage Lung Tumor Detection Based on Super-Wideband Microwave Reflectometry" Electronics 12, no. 1: 36. https://doi.org/10.3390/electronics12010036
APA StyleAlamro, W., Seet, B. -C., Wang, L., & Parthiban, P. (2023). Early-Stage Lung Tumor Detection Based on Super-Wideband Microwave Reflectometry. Electronics, 12(1), 36. https://doi.org/10.3390/electronics12010036