
Inflammatory Bowel Disease: An Indication to Screen for Thrombophilia?



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
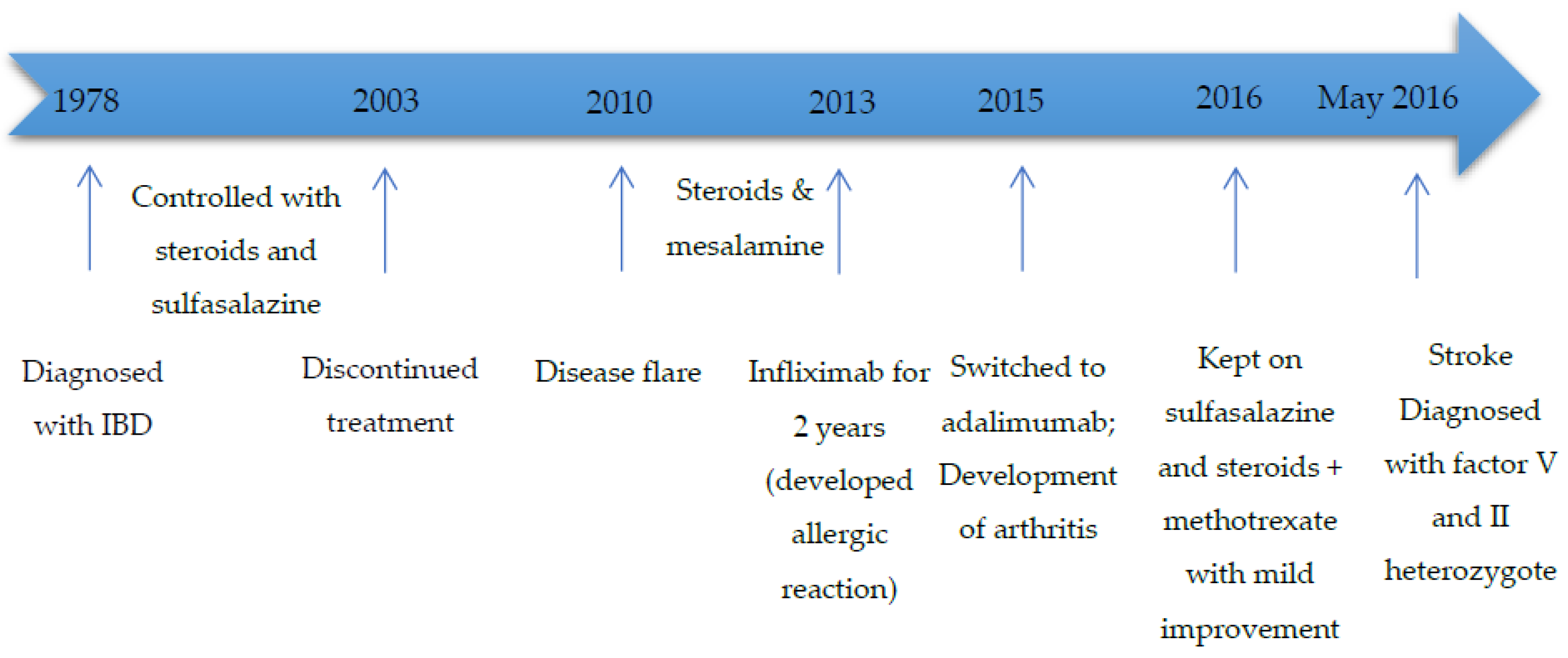
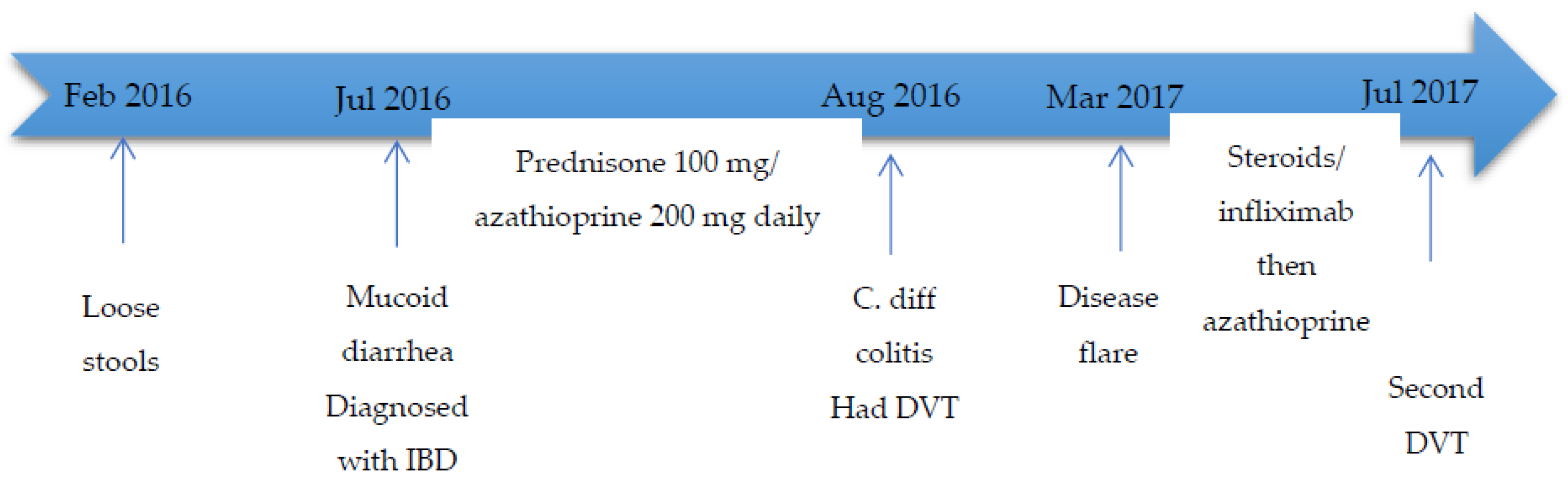
2. Cases
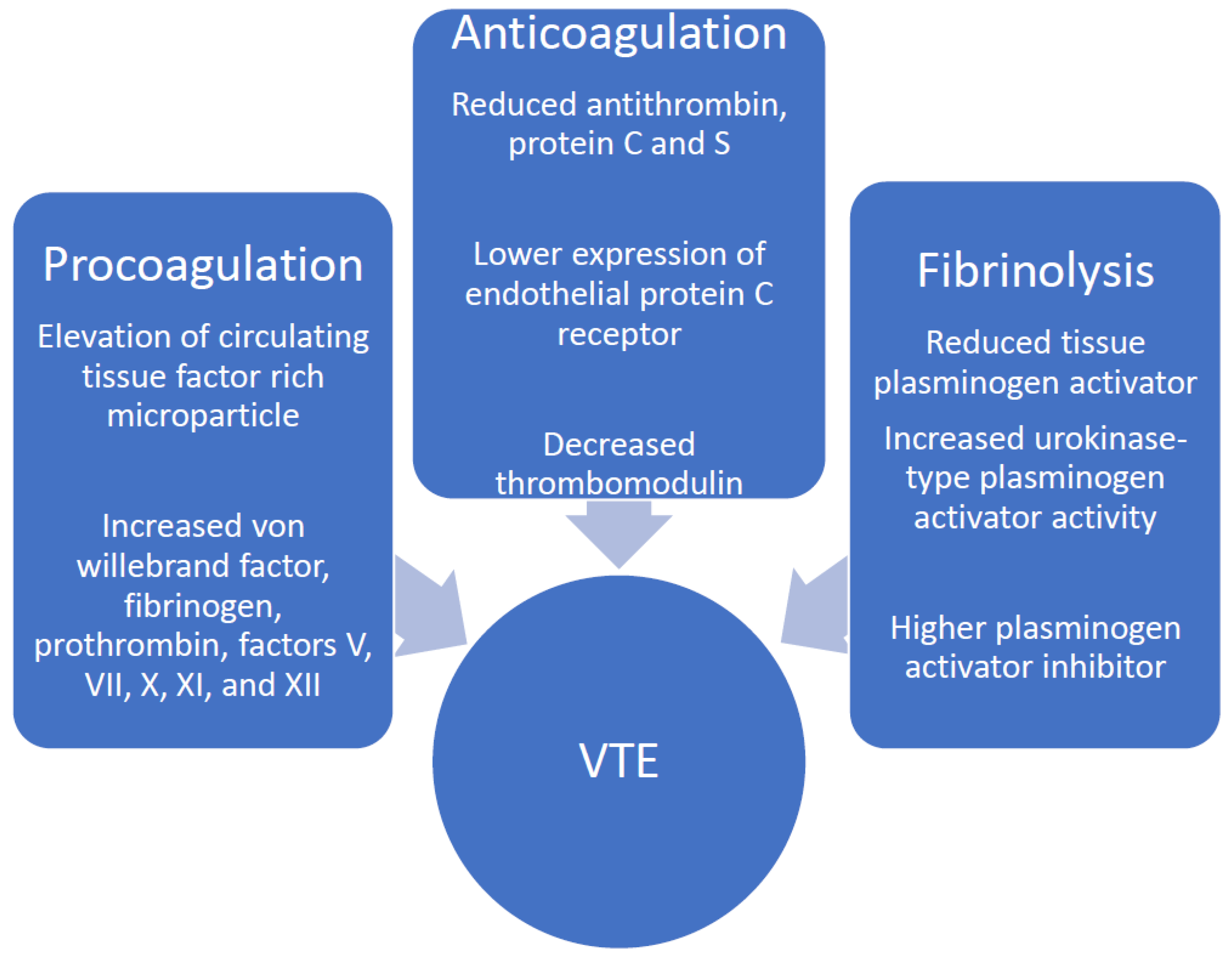
3. Literature Review
4. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Owczarek, D.; Cibor, D.; Głowacki, M.K.; Rodacki, T.; Mach, T. Inflammatory bowel disease: Epidemiology, pathology and risk factors for hypercoagulability. World J. Gastroenterol. 2014, 20, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Twig, G.; Zandman-Goddard, G.; Szyper-Kravitz, M.; Shoenfeld, Y. Systemic thromboembolism in inflammatory bowel disease: Mechanisms and clinical applications. Ann. N. Y. Acad. Sci. 2005, 1051, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.; Nguyen, G. Venous thromboembolism in inflammatory bowel disease: An epidemiological review. Am. J. Gastroenterol. 2011, 106, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Miehsler, W.; Reinisch, W.; Valic, E.; Osterode, W.; Tillinger, W.; Feichtenschlager, T.; Grisar, J.; Machold, K.; Scholz, S.; Vogelsang, H.; et al. Is inflammatory bowel disease an independent and disease specific factor for thromboembolism? Gut 2004, 53, 542–548. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, C.N.; Blanchard, J.F.; Houston, D.S.; Wajda, A. The incidence of deep venous thrombosis and pulmonary embolism among patients with inflammatory bowel disease: A population-based cohort study. Thromb. Haemost. 2001, 85, 430–434. [Google Scholar]
- Yuhara, H.; Steinmaus, C.; Corley, D.; Koike, J.; Igarashi, M.; Suzuki, T.; Mine, T. Meta-analysis: The riskof venous thromboembolism in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 37, 953–962. [Google Scholar] [CrossRef]
- Nguyen, G.C.; Bernstein, C.N.; Bitton, A.; Chan, A.K.; Griffiths, A.M.; Leontiadis, G.I.; Geerts, W.; Bressler, B.; Butzner, J.D.; Carrier, M.; et al. Consensus statements on the risk, prevention, and treatment of venous thromboembolism in inflammatory bowel disease: Canadian Association of Gastroenterology. Gastroenterology 2014, 146, 835–848. [Google Scholar] [CrossRef] [Green Version]
- Grainge, M.; West, J.; Card, T. Venous thromboembolism during active disease andremission in inflammatory bowel disease: A cohort study. Lancet 2010, 375, 657–663. [Google Scholar] [CrossRef]
- Grip, O.; Svensson, P.J.; Lindgren, S. Inflammatory bowel disease promotes venous thrombosis earlier in life. Scand. J. Gastroenterol. 2000, 35, 619–623. [Google Scholar] [CrossRef]
- Papa, A.; Papa, V.; Marzo, M.; Scaldaferri, F.; Sofo, L.; Rapaccini, G.L.; Danese, S.; Gasbarrini, A. Prevention and Treatment of Venous Thromboembolism in Patients with IBD: A Trail Still Climbing. Inflamm. Bowel. Dis. 2015, 21, 1204–1213. [Google Scholar] [CrossRef]
- Papa, A.; Santoliquido, A.; Danese, S.; Covino, M.; Di Campli, C.; Urgesi, R.; Grillo, A.; Guglielmo, S.; Tondi, P.; Guidi, L.; et al. Increased carotid intima-media thickness in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2005, 22, 839–846. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Venous Thromboembolic Diseases: Diagnosis, Management and Thrombophilia Testing [Internet]; NICE Guideline [NG158]; NICE: London, UK, 2020; Available online: https://www.nice.org.uk/guidance/ng158 (accessed on 20 December 2021).
- Hicks, L.K.; Bering, H.; Carson, K.R.; Kleinerman, J.; Kukreti, V.; Ma, A.; Mueller, B.U.; O’Brien, S.H.; Pasquini, M.; Sarode, R.; et al. The ASH Choosing Wisely campaign: Five hematologic tests and treatments to question. Blood 2013, 122, 3879–3883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connors, J. Thrombophilia testing and venous thrombosis. N. Engl. J. Med. 2017, 377, 1177–1187. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.; Sam, J. Rising prevalence of venous thromboembolism and its impact on mortality among hospitalized inflammatory bowel disease patients. Am. J. Gastroenterol. 2008, 103, 2272–2280. [Google Scholar] [CrossRef]
- Magro, F.; Soares, J.; Fernandes, D. Venous thrombosis and prothrombotic factors in inflammatory bowel disease. World J. Gastroenterol. 2014, 20, 4857–4872. [Google Scholar] [CrossRef]
- Scaldaferri, F.; Lancellotti, S.; Pizzoferrato, M.; De Cristofaro, R. Haemostatic system in inflammatory bowel diseases: New players in gut inflammation. World J. Gastroenterol. 2011, 17, 594–608. [Google Scholar] [CrossRef]
- Spina, L.; Saibeni, S.; Battaglioli, T.; Peyvandi, F.; De Franchis, R.; Vecchi, M. Thrombosis in inflammatory bowel diseases: Role of inherited thrombophilia. Am. J. Gastroenterol. 2005, 100, 2036–2041. [Google Scholar] [CrossRef]
- Kornbluth, A.; Sachar, D. Ulcerative colitis practice guidelines in adults: American College Of Gastroenterology, Practice Parameters Committee. Am. J. Gastroenterol. 2010, 105, 501–523. [Google Scholar] [CrossRef]
- Scoville, E.A.; Konijeti, G.G.; Nguyen, D.D.; Sauk, J.; Yajnik, V.; Ananthakrishnan, A.N. Venous Thromboembolism in Patients with: Inflammatory Bowel Diseases: A case-control study of risk factors. Inflamm. Bowel. Dis. 2014, 20, 631–636. [Google Scholar] [CrossRef] [Green Version]
- van Bodegraven, A.; Schoorl, M.; Linskens, R.; Bartels, P.; Tuynman, H. Persistent activation of coagulation and fibrinolysis after treatment of active ulcerative colitis. Eur. J. Gastroenterol. Hepatol. 2002, 14, 413–418. [Google Scholar] [CrossRef]
- Tsiolakidou, G.; Koutroubakis, I. Thrombosis and inflammatory bowel disease-the role of genetic risk factors. World J. Gastroenterol. 2008, 14, 4440–4444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irving, P.; Macey, M.G.; Shah, U.; Webb, L.; Langmead, L.; Rampton, D.S. Formation of platelet-leukocyte aggregates in inflammatory bowel disease. Inflamm. Bowel. Dis. 2004, 10, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Novacek, G.; Weltermann, A.; Sobala, A.; Tilg, H.; Petritsch, W.; Reinisch, W.; Mayer, A.; Haas, T.; Kaser, A.; Feichtenschlager, T.; et al. Inflammatory bowel disease is a risk factor for recurrent venous thromboembolism. Gastroenterology 2010, 139, 779–787.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappelman, M.D.; Horvath-Puho, E.; Sandler, R.S.; Rubin, D.T.; Ullman, T.A.; Pedersen, L.; Baron, J.A.; Sørensen, H.T. Thromboembolic risk among Danish children and adults with inflammatory bowel diseases: A population-based nationwide study. Gut 2011, 60, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Solem, C.A.; Loftus, E.V.; Tremaine, W.J.; Sandborn, W.J. Venous thromboembolism in inflammatory bowel disease. Am. J. Gastroenterol. 2004, 99, 97–101. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, V.; Chiusolo, P.; Paciaroni, K.; Leone, G. Epidemiology of factor V Leiden: Clinical implications. Semin Thromb. Hemost. 1998, 24, 367–379. [Google Scholar] [CrossRef]
- Koutroubakis, I.E.; Sfiridaki, A.; Tsiolakidou, G.; Theodoropoulou, A.; Livadiotaki, A.; Paspatis, G.; Kouroumalis, E.A. Genetic risk factors in patients with inflammatory bowel disease and vascular complications: Case-control study. Inflamm. Bowel. Dis. 2007, 13, 410–415. [Google Scholar] [CrossRef]
- Zhong, M.; Dong, X.W.; Zheng, Q.; Tong, J.L.; Ran, Z.H. Factor V Leiden and thrombosis in patients with inflammatory bowel disease (IBD): A meta-analysis. Thromb. Res. 2011, 128, 403–409. [Google Scholar] [CrossRef]
- Liang, J.; Wu, S.; Feng, B.; Lei, S.; Luo, G.; Wang, J.; Li, K.; Li, X.; Xie, H.; Zhang, D.; et al. Factor V Leiden and inflammatory bowel disease: A systematic review and meta-analysis. J. Gastroenterol. 2011, 46, 1158–1166. [Google Scholar] [CrossRef]
- Huisman, M.; Rosendaal, F. Thrombophilia. Curr. Opin. Hematol. 1999, 6, 291–297. [Google Scholar] [CrossRef]
- Saibeni, S.; Ciscato, C.; Vecchi, M.; Anzoletti, M.B.; Kaczmarek, E.; Caccia, S.; De Franchis, R.; Cugno, M. Antibodies to tissue-type plasminogen activator (t-PA) in patients with inflammatory bowel disease: High prevalence, interactions with functional domains of t-PA and possible implications in thrombosis. J. Thromb. Haemost. 2006, 4, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Den Heijer, M.; Lewington, S.; Clarke, R. Homocysteine, MTHFR and risk of venous thrombosis: A meta-analysis of published epidemiological studies. J. Thromb. Haemost. 2005, 3, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Hickey, S.E.; Curry, C.J.; Toriello, H.V. ACMG Practice Guideline: Lack of evidence for MTHFR polymorphism testing. Genet. Med. 2013, 15, 153–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papa, A.; Danese, S.; Grillo, A.; Gasbarrini, G.; Gasbarrini, A. Review Article: Inherited Thrombophilia in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2003, 98, 1247–1251. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T.B.; Nielsen, J.N.; Fredholm, L.; Brandslund, I.; Munkholm, P.; Hey, H. Hyperhomocysteinemia, coagulation pathway activation and thrombophilia in patients with inflammatory bowel disease. Scand. J. Gastroenterol. 2002, 37, 62–67. [Google Scholar] [CrossRef]
- Mahmud, N.; Molloy, A.; McPartlin, J.; Corbally, R.; Whitehead, A.S.; Scott, J.M.; Weir, D.G. Increased prevalence of methylenetetrahydrofolate reductase C677T variant in patients with inflammatory bowel disease, and its clinical implications. Gut 1999, 45, 389–394. [Google Scholar] [CrossRef] [Green Version]
- Alhenc-Gelas, M.; Plu-Bureau, G.; Horellou, M.H.; Rauch, A.; Suchon, P. GEHT genetic thrombophilia group PROS1 Genotype Phenotype Relationships in a Large Cohort of Adults with Suspicion of Inherited Quantitative Protein S Deficiency. Thromb. Haemost. 2016, 115, 570–579. [Google Scholar]
- Khider, L.; Gendron, N.; Mauge, L. Inherited Thrombophilia in the Era of Direct Oral Anticoagulants. Int. J. Mol. Sci. 2022, 23, 1821. [Google Scholar] [CrossRef]
- Taher, A.; Khalil, I.; Shamseddine, A.; El-Ahdab, F.; Bazarbachi, A. High prevalence of Factor V Leiden mutation among healthy individuals and patients with deep venous thrombosis in Lebanon: Is the Eastern Mediterranean region the area of origin of this mutation? Thromb. Haemost. 2001, 86, 723–724. [Google Scholar] [CrossRef]
- Tamim, H.; Finan, R.R.; Almawi, W. Prevalence of two thrombophilia predisposing mutations: Factor V G1691A (R506Q; Leiden) and prothrombin G20210A, among healthy Lebanese. Thromb. Haemost. 2002, 88, 691–692. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moukalled, N.M.; Hashash, J.G.; Taher, A.T. Inflammatory Bowel Disease: An Indication to Screen for Thrombophilia? Diseases 2022, 10, 14. https://doi.org/10.3390/diseases10010014
Moukalled NM, Hashash JG, Taher AT. Inflammatory Bowel Disease: An Indication to Screen for Thrombophilia? Diseases. 2022; 10(1):14. https://doi.org/10.3390/diseases10010014
Chicago/Turabian StyleMoukalled, Nour M., Jana G. Hashash, and Ali T. Taher. 2022. "Inflammatory Bowel Disease: An Indication to Screen for Thrombophilia?" Diseases 10, no. 1: 14. https://doi.org/10.3390/diseases10010014
APA StyleMoukalled, N. M., Hashash, J. G., & Taher, A. T. (2022). Inflammatory Bowel Disease: An Indication to Screen for Thrombophilia? Diseases, 10(1), 14. https://doi.org/10.3390/diseases10010014