The Predictive Value of Plasma Brain Natriuretic Peptide and Galectin-3 in Elderly Patients Admitted for Heart Failure †


Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
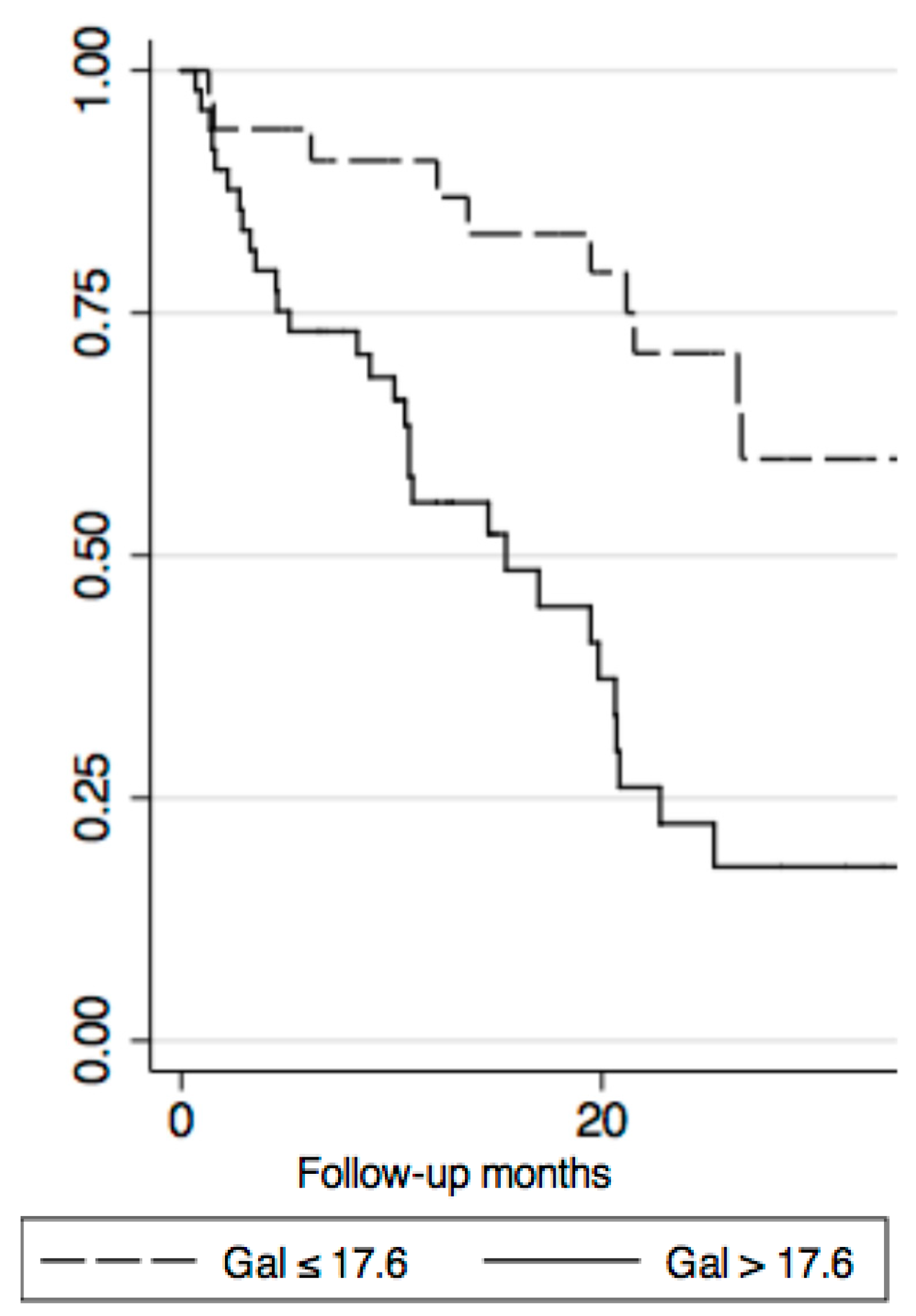
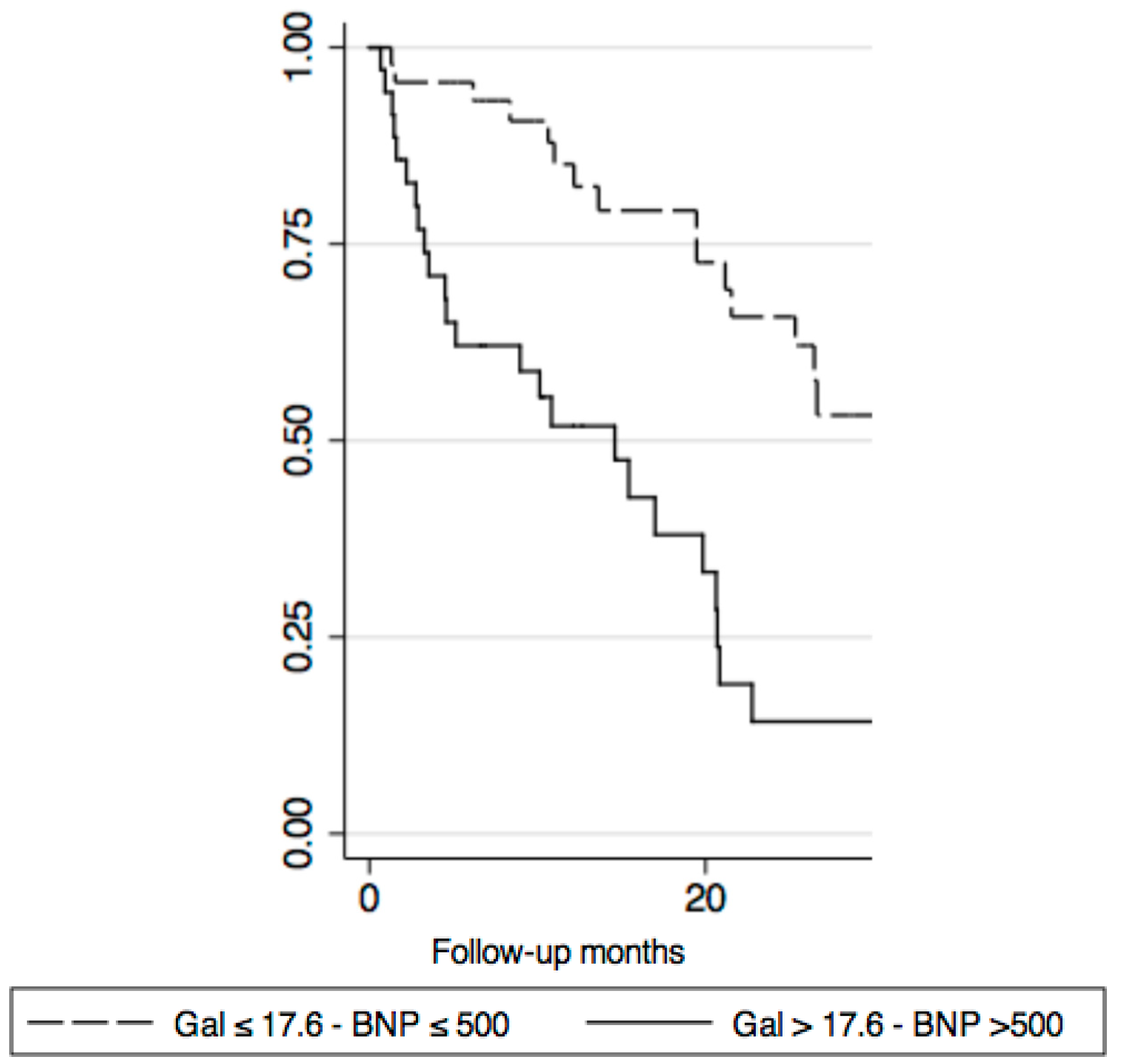
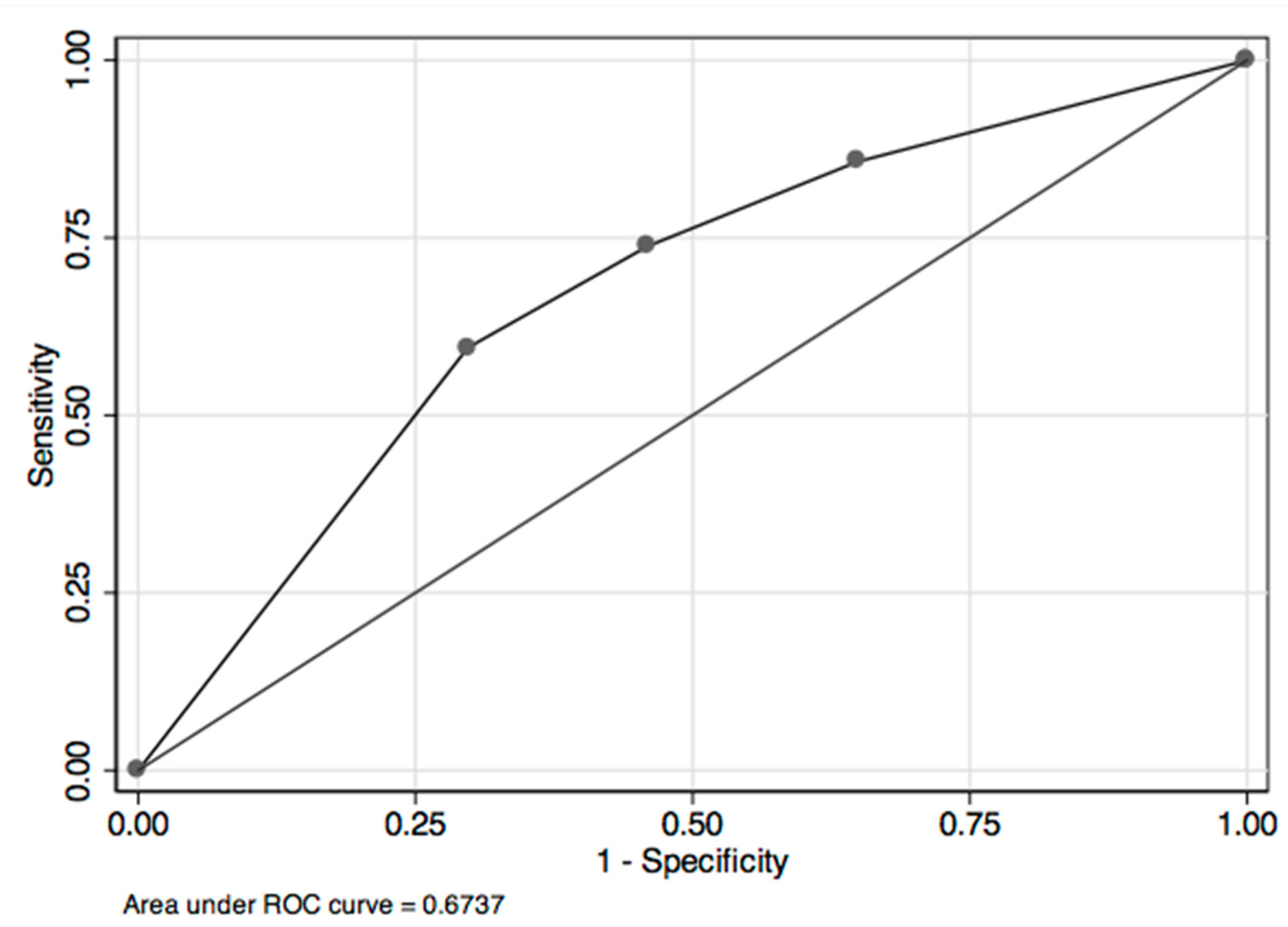
4. Results
5. Discussion
Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Di Lenarda, A.; Scherillo, M.; Maggioni, A.P.; Acquarone, N.; Ambrosio, G.B.; Anniccharico, M.; Bellis, P.; Bellotti, P.; DeMaria, R.; Lavechhia, R.; et al. Current presentation and management of heart failure in cardiology and internal medicine hospital units: A tale of words. The TEMISTOCLE study. Am. Heart J. 2003, 146, E12. [Google Scholar] [CrossRef]
- Abraham, W.T.; Perl, L. Implantable hemodynamic monitoring for heart failure patients. J. Am. Coll. Cardiol. 2017, 70, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Di Tano, G.; De Maria, R.; Gonzini, L.; Aspromonte, N.; Di Lenarda, A.; Feola, M.; Marini, M.; Milli, M.; Misuraca, G.; Mortara, A.; et al. The 30-day metric in acute heart failure revisited: Data from IN-HF Outcome, an Italian nationwide cardiology registry. Eur. J. Heart Fail. 2015, 17, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Swedberg, K.; Cleland, J.; Dargie, H.; Drexler, H.; Follath, F.; Komajda, M.; Tavazzi, L.; Smiseth, O.A.; Gavazzi, A.; Haverich, A.; et al. Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Guidelines for the diagnosis and treatment of chronic heartf ailure: Executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur. Heart J. 2005, 26, 1115–1140. [Google Scholar] [PubMed]
- Fonarow, G.C.; Adams, K.F.; Abraham, W.T.; Yancy, C.W.; Boscardin, W.J. for the ADHERE Scientific Advisory Committee. Risk stratification for in-hospital mortality in acutely decompensated heart failure. JAMA 2005, 293, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Berger, R.; Huelsman, M.; Strecker, K.; Bojic, A.; Moser, P.; Stanek, B.; Pacher, R. B-type Natriuretic Peptide predicts sudden death in patients with chronic heart failure. Circulation 2002, 105, 2392–2397. [Google Scholar] [CrossRef] [PubMed]
- Feola, M.; Aspromonte, N.; Canali, C.; Ceci, V.; Giovinazzo, P.; Milani, L.; Quarta, G.; Ricci, R.; Scardovi, A.B.; Uslenghi, E.; et al. Prognostic value of plasma brain natriuretic peptide, urea nitrogen and creatinine in outpatients >70 years of age with heart failure. Am. J. Cardiol. 2005, 965, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Lupón, J.; de Antonio, M.; Vila, J.; Peñafiel, J.; Galán, A.; Zamora, E.; Urrutia, A.; Bayes-Genis, A. Development of a novel heart failure risk tool: The Barcelona bioheart failure risk calculator (BCN bio-HF calculator). PLoS ONE 2014, 9, e85466. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, K.; Bennett, D.; Conrad, N.; Williams, T.M.; Basu, J.; Dwight, J.; Woodward, M.; Patel, A.; McMurray, J.; MacMahon, S. Risk prediction in patients with heart failure. JACC Heart Fail. 2014, 2, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Ouwerkerk, W.; Voors, A.A.; Zwinderman, A.H. Factors influencing the predictive power of models for predicting mortality and/or heart-failure hospitalization in patients with heart failure. JACC Heart Fail. 2014, 2, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Van Kimmenade, R.R.; Januzzi, J.L.; Ellinor, P.T.; Sharma, U.C.; Bakker, J.A.; Low, A.F.; Martinez, A.; Crijns, H.J.; MacRae, C.A.; Menheere, P.P.; et al. Utility of amino-terminal pro-brain natriuretic peptide, galectin-3, and apelin for the evaluation of patients with acute heart failure. J. Am. Coll. Cardiol. 2006, 48, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.V.; Chen-Tournoux, A.A.; Picard, M.H.; van Kimmenade, R.R.; Januzzi, J.L. Galectin-3, cardiac structure and function, and long-term mortality in patients with acutely decompensated heart failure. Eur. J. Heart Fail. 2010, 12, 826–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, R.A.; Lok, D.J.; Jaarsma, T.; van der Meer, P.; Voors, A.A.; Hillege, H.L.; van Veldhuisen, D.J. Predictive value of plasma galectin-3 levels in heart failure with reduced and preserved ejection fraction. Ann. Med. 2011, 43, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Peacock, W.F. Rapid optimization: Strategies for optimal care of decompensated congestive heart failure patients in the emergency department. Rev. Cardiovasc. Med. 2003, 3, S41–S48. [Google Scholar]
- Sahn, D.J.; Demaria, A.; Kisslo, J. The committee on M mode standardisation of the American Society of Echocardiography: Recommendations regarding quantification in M-mode echocardiography: Results of a survey of echocardiographic measurements. Circulation 1978, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.J.; Thomas, J.D.; Klein, A.L. New Doppler echocardiographic applications for the study of diastolic function. J. Am. Coll. Cardiol. 1998, 32, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Christenson, R.H.; Duh, S.H.; Wu, A.H.; Smith, A.; Abel, G.; Wang, S.; Adourian, A.; Adiletto, C.; Gardiner, P. Multi-center determination of galectin-3 assay performance characteristics: Anatomy of a novel assay for use in heart failure. Clin. Biochem. 2010, 43, 683–690. [Google Scholar] [CrossRef] [PubMed]
- ATS Statement. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar]
- Mahoney, F.; Barthel, D. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Katz, S.; Ford, A.B. Studies of illness in the aged: The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.F.; Greiner, M.A.; Fonarow, G.C.; Hammill, B.G.; Heidenreich, P.A.; Yanchy, C.W.; Peterson, E.D.; Curtis, L.H. Relationship between early physician follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA 2010, 303, 1716–1722. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Lin, L.Y.; Wu, Y.W.; Chien, K.L.; Lee, C.M.; Hsu, R.B.; Chao, C.L.; Wang, S.S.; Hsein, Y.C.; Liao, L.C.; et al. The relationship between serum galectin-3 and serum markers of cardiac extracellular matrix turnover in heart failure patients. Clin. Chim. Acta 2009, 409, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Lok, D.J.; Lok, S.I.; Bruggink-André de la Porte, P.W.; Badings, E.; Lipsic, E.; van Wijngaarden, J.; de Boer, R.A.; van Veldhuisen, D.J.; van der Meer, P. Galectin-3 is an independent marker for ventricular remodeling and mortality in patients with chronic heart failure. Clin. Res. Cardiol. 2013, 102, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Meijers, W.C.; de Boer, R.A.; van Veldhuisen, D.J.; Jaarsma, T.; Hillege, H.L.; Maisel, A.S.; Di Somma, S.; Voors, A.A.; Peacock, W.F. Biomarkers and low risk in heart failure. Data from COACH and TRIUMPH. Eur. J. Heart Fail. 2015, 17, 1271–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijers, W.C.; Januzzi, J.L.; Adourian, A.S.; Shah, S.J.; van Veldhuisen, D.J.; de Boer, R.A. Elevated plasma galectin-3 is associated with near-term rehospitalisation in heart failure: A pooled analysis of 3 clinical trials. Am. Heart J. 2014, 167, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Fernández, S.; Boronat-Garcia, M.; Albaladejo-Otón, M.D.; Pastor, P.; Garrido, I.P.; Pastor-Pérez, F.J.; Martínez-Hernández, P.; Valdés, M.; Pascual-Figal, D.A. Complementary prognostic value of cystatin C, N-terminal pro-Btype natriuretic peptide and cardiac troponin T in patients with acute heart failure. Am. J. Cardiol. 2009, 103, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.A.; van Kimmenade, R.R.; Richards, M.; Bayes-Genis, A.; Pinto, Y.; Moore, S.A.; Januzzi, J.L., Jr. Hyponatremia, natriuretic peptides, and outcomes in acutely decompensated heart failure: Results from the International Collaborative of NT-proBNP Study. Circ. Heart Fail. 2010, 3, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Feola, M.; Testa, M.; Leto, L.; Cardone, M.; Sola, M.; Rosso, G.L. Role of galectin-3 and plasma B type-natriuretic peptide in predicting prognosis in discharged chronic heart failure patients. Medicine 2016, 95, e4014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troughton, R.W.; Frampton, C.M.; Brunner-La Rocca, H.P.; Pfisterer, M.; Eurlings, L.W. Effect of B-type natriuretic peptide-guided treatment of chronic heart failure on total mortality and hospitalization: An individual patient meta-analysis. Eur. Heart J. 2014, 35, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.; Taylor, J. Chronic heart failure care planning: Considerations in older patients. Cardiac. Fail. Rev. 2017, 3, 46–51. [Google Scholar] [CrossRef]
- Correale, M.; Monaco, I.; Brunetti, N.D.; Di Biase, M.; Metra, M.; Nodari, S.; Butler, J.; Gheorghiade, M. redefining biomarkers in heart failure. Heart Fail. Rev. 2018, 23, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Brunner-La Rocca, H.P.; Eurlings, L.; Richards, A.M.; Jannuzzi, J.L.; Pfisterer, M.E.; Dahlstrom, U.; Pinto, Y.M.; Karlstrom, P.; Emtell, H.; Berger, R.; et al. Which heart failure patients profit from natriuretic peptide guided therapy? A meta-analysis from individual patient data of randomized trials. Eur. J. Heart Fail. 2015, 17, 1252–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Digitalis Intervention Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N. Engl. J. Med. 1997, 336, 525–535. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n = 84 | |
|---|---|
| Age (years) | 77.5 ± 5.9 (65–90) |
| Males | 63 (75%) |
| CABG/PTCA | 23 (27.4%)/21 (25%) |
| VALV | 38 (45.2%) |
| CMP | 10 (12.5%) |
| CAD | 35 (41.7%) |
| ICD | 25 (29.8%) |
| Diabetes | 31 (36.9%) |
| Sinus Rhythm | 38 (45.2%) |
| Creatinine (mg/dL) | 1.5 ± 0.9 |
| eGFR (mL/min/1.73 m2) | 50.9 ± 21.7 |
| Haemoglobin (g/dL) | 12.6 ± 1.8 |
| Sodium (mEq/L) | 139.8 ± 3.3 |
| BNP (pg/mL) | 1156.8 ± 1108.7 |
| Galectin-3 (ng/mL) | 25.1 ± 15.1 |
| LVEF (%) | 37.8 ± 16.6 |
| LVEF < 50% | 60 (71.4%) |
| LVESD (mm) | 47.3 ± 13.6 |
| LVEDD (mm) | 58.5 ± 11.2 |
| PAPs (mmHg) | 39.6 ± 9.9 |
| NYHA admission | 3.1 ± 0.8 |
| NYHA discharge | 2.2 ± 0.5 |
| 6-min WT admission (m) | 248.4 ± 117.2 |
| ADL admission | 4.6 ± 2.1 |
| ADL discharge | 5.4 ± 1.2 |
| IADL | 1.4 ± 2.3 |
| Barthel Index admission | 83.8 ± 21.8 |
| Barthel Index discharge | 91.3 ± 15.4 |
| Length of Hospital stay (days) | 11.7 ± 5.5 |
| Diuretics | 82 (97.6%) |
| B-blockers | 73 (86.9%) |
| ACE-Inibitor/ARB | 42/34 (90.5%) |
| Spironolactone | 40 (47.6%) |
| No-Event Group (39 pts) | Event Group (45 pts) | p | |
|---|---|---|---|
| Age (years) | 77.5 ± 0.8 | 77.6 ± 0.9 | 0.97 |
| Sodium (mEq/L) | 139.8 ± 0.6 | 139.7 ± 0.4 | 0.94 |
| Haemoglobin (g/dL) | 12.8 ± 0.3 | 12.5 ± 0.3 | 0.60 |
| Creatinine (mg/dL) | 1.3 ± 0.1 | 1.6 ± 0.2 | 0.08 |
| eGFR (mL/min/1.73 m2) | 53.3 ± 3.6 | 48.6 ± 3.5 | 0.35 |
| BNP (pg/mL) | 844.5 ± 160.8 | 1431.9 ± 178.1 | 0.02 |
| Galectin-3 (ng/mL) | 21.7 ± 2.4 | 28.1 ± 2.2 | 0.05 |
| LVEF (%) | 41.6 ± 2.7 | 34.1 ± 2.5 | 0.04 |
| LVESD (mm) | 44.5 ± 2.3 | 49.9 ± 2.2 | 0.098 |
| LVEDD (mm) | 56.7 ± 1.7 | 60.4 ± 2.1 | 0.17 |
| TAPSE (mm) | 15.8 ± 1.6 | 16.6 ± 0.8 | 0.65 |
| PAP (mmHg) | 38.0 ± 1.7 | 41.2 ± 1.7 | 0.19 |
| 6 MinWT admission (m) (n = 43) | 261.6 ± 26.8 | 233.2 ± 23.2 | 0.43 |
| 6 MinWT discharge (m) (n = 42) | 290.8 ± 20.1 | 261.0 ± 24.6 | 0.36 |
| Length of Hospital stay (days) | 11.5 ± 0.9 | 11.8 ± 0.8 | 0.78 |
| Barthel Index admission | 83.5 ± 4.5 | 84.1 ± 4.2 | 0.93 |
| Barthel Index discharge | 91.8 ± 3.5 | 90.9 ± 3.0 | 0.83 |
| IADL | 1.4 ± 0.4 | 1.4 ± 0.4 | 0.89 |
| ADL at admission | 4.8 ± 0.4 | 4.5 ± 0.4 | 0.53 |
| ADL at discharge | 5.4 ± 0.3 | 5.5 ± 0.3 | 0.68 |
| Diabetes mellitus | 12 | 19 | 0.95 |
| Diuretics | 38 (97.4%) | 44 (97.7%) | 0.5 |
| B-blockers | 34 (87.1%) | 39 (86.6%) | 0.79 |
| ACE-Inibitor/ARB | 17/19 (92.3%) | 25/15 (88.8%) | 0.8 |
| Spironolactone | 22 (56.4%) | 18 (40%) | 0.2 |
| Total Events | Death | Rehospitalization | ||||
|---|---|---|---|---|---|---|
| (Death and Rehospitalization) | ||||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Gal-3 > 17.6 ng/mL | 2.87 (1.17–7.07) | 0.022 | 4.43 (1.17–16.75) | 0.028 | 1.24 (0.48–3.17) | 0.659 |
| Adjusted for age | 2.89 (1.17–7.13) | 0.022 | 4.35 (1.15–16.51) | 0.031 | 1.27 (0.49–3.28) | 0.622 |
| Adjusted for LVEF | 2.38 (0.92–6.16) | 0.075 | 5.51 (1.12–27.18) | 0.036 | 0.99 (0.37–2.72) | 0.990 |
| Adjusted for creatinine (eGFR) | 2.35 (0.91–6.04) | 0.077 | 4.17 (1.06–16.46) | 0.041 | 1.07 (0.39–2.89) | 0.890 |
| Adjusted for diabetes | 2.56 (1.02–6.41) | 0.045 | 3.90 (1.00–15.22) | 0.050 | 1.23 (0.46–3.29) | 0.675 |
| Adjusted for Barthel Index | 3.76 (0.89–15.85) | 0.071 | 0.98 (0.94–1.02) | 0.333 | 1.73 (0.41–7.32) | 0.454 |
| Total Events | Death | Rehospitalization | ||||
|---|---|---|---|---|---|---|
| (Death and Rehospitalization) | ||||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Gal-3 > 17.6 ng/mL + BNP > 500 pg/mL | 3.54 (1.40–8.91) | 0.007 | 5.25 (1.52–18.10) | 0.009 | 1.29 (0.51–3.26) | 0.580 |
| Adjusted for age | 3.56 (1.41–9.01) | 0.007 | 5.64 (1.59–19.88) | 0.007 | 1.27 (0.50–3.21) | 0.618 |
| Adjusted for LVEF | 2.98 (1.04–8.54) | 0.042 | 6.20 (1.31–29.31) | 0.021 | 1.08 (0.37–3.17) | 0.892 |
| Adjusted for creatinine (eGFR) | 2.99 (1.15–7.80) | 0.025 | 5.26 (1.47–18.85) | 0.011 | 1.10 (0.41–2.92) | 0.851 |
| Adjusted for diabetes | 3.61 (1.38–9.41) | 0.009 | 4.57 (1.30–16.04) | 0.018 | 1.47 (0.55–3.87) | 0.441 |
| Adjusted for Barthel Index | 5.43 (1.49–19,7) | 0.010 | 0.98 (0.93–1.02) | 0.317 | 1.49 (0.42–5.21) | 0.535 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Testa, M.; Rosso, G.L.; Ferreri, C.; Feola, M. The Predictive Value of Plasma Brain Natriuretic Peptide and Galectin-3 in Elderly Patients Admitted for Heart Failure. Diseases 2018, 6, 88. https://doi.org/10.3390/diseases6040088
Testa M, Rosso GL, Ferreri C, Feola M. The Predictive Value of Plasma Brain Natriuretic Peptide and Galectin-3 in Elderly Patients Admitted for Heart Failure. Diseases. 2018; 6(4):88. https://doi.org/10.3390/diseases6040088
Chicago/Turabian StyleTesta, Marzia, Gian Luca Rosso, Cinzia Ferreri, and Mauro Feola. 2018. "The Predictive Value of Plasma Brain Natriuretic Peptide and Galectin-3 in Elderly Patients Admitted for Heart Failure" Diseases 6, no. 4: 88. https://doi.org/10.3390/diseases6040088
APA StyleTesta, M., Rosso, G. L., Ferreri, C., & Feola, M. (2018). The Predictive Value of Plasma Brain Natriuretic Peptide and Galectin-3 in Elderly Patients Admitted for Heart Failure. Diseases, 6(4), 88. https://doi.org/10.3390/diseases6040088