
Lymphocytes as a Biomarker of Frailty Syndrome: A Scoping Review



Abstract
:1. Introduction
2. Materials and Methods
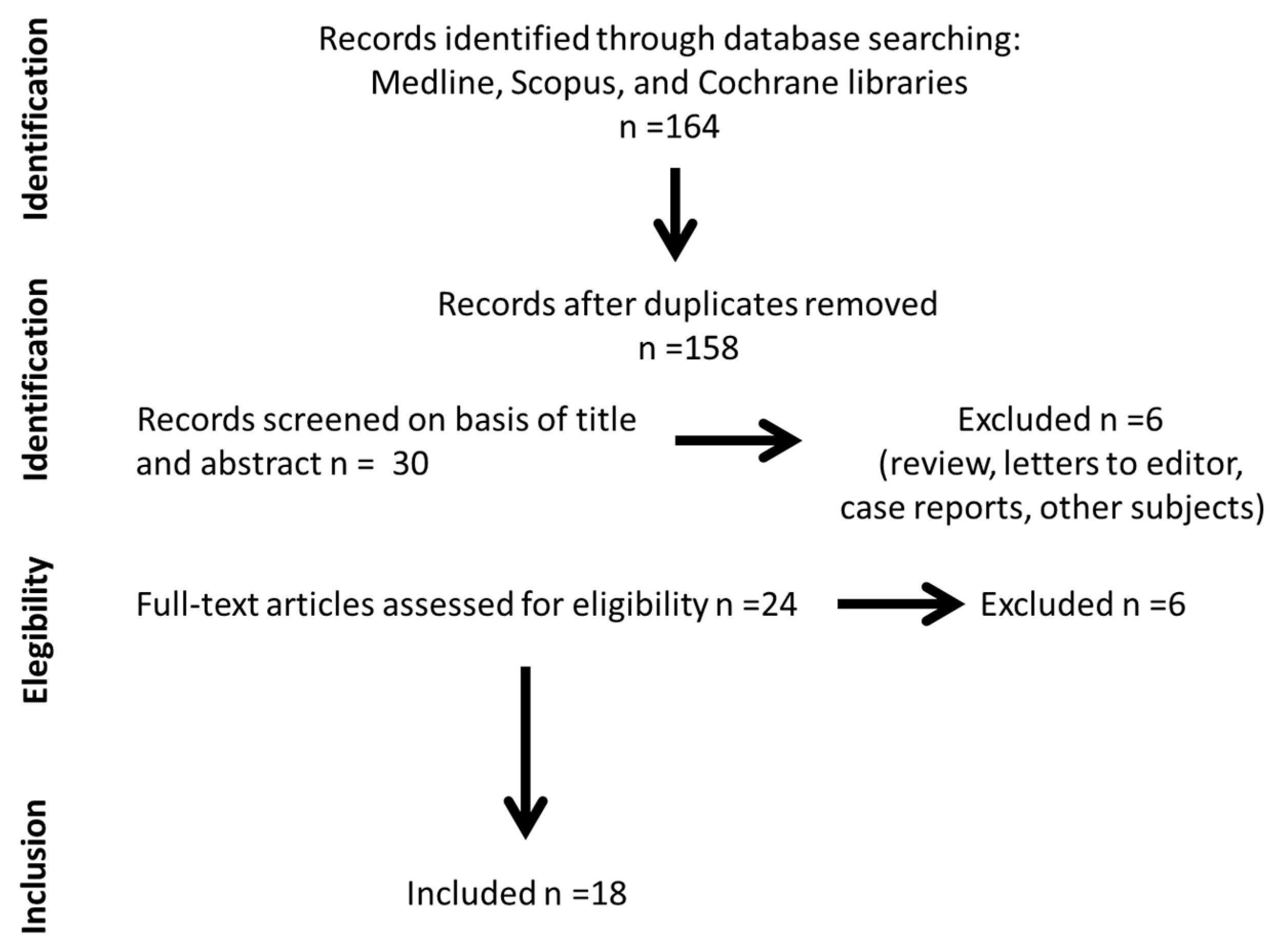
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Collection and Analysis
3. Results
3.1. Relationship between Total Lymphocytes and Frailty Syndrome Prevalence

{kind=link}
| Reference Sorted by Year of Publication | Study Design | Sample Size (n) | Subjects (Sex and Age) | Participants | Frailty Assessment | Relationship between Total Lymphocyte Count and Frailty |
|---|---|---|---|---|---|---|
| Semba et al., 2005 [20] | Case-control study. | 122 | Community dwelling-women (cases) who died during 5 years of follow-up (mean age 76.9 ± 6,4 years) and women (controls) matched by age, frailty, and morbidities who survived during 7 years of follow-up (mean age 77.3 ± 6.8 years). | Community-dwelling adults. | Fried’s criteria. | There were no significant differences in counts or percentages of lymphocytes between frail, pre-frail, and non-frail women. |
| De Fanis et al., 2008 [23] | Case-control study. | 26 | 22 women and 4 men with a mean age of 83.8 ± 5.3 years (range 72–94). | Community-dwelling adults. | Fried’s criteria | No significant differences in total lymphocyte counts between frail and non-frail participants were observed. |
| Leng et al., 2009 [10] | Observational cohort study. | 1106 | Women from the WHAS I cohorts with an age range of 65–102 years and women from the merged WHAS I and II cohorts with an age range of 70–79 years. | Community-dwelling woman. | Fried’s criteria. | No significant association between total counts of lymphocytes with frailty was identified. |
| Collerton et al., 2012 [12] | Cross-sectional study. | 845 | Different cohorts with a percentage of women in each cohort ranging from 60 to 75%. All participants were over 85 years old. | Community-dwelling or institutionalized older people. | Rockwood frailty index and Fried’s criteria. | The total lymphocyte count was inversely related to both measures of frailty, Fried scale and the Rockwood frailty index. |
| Fernández-Garrido et al., 2014 [16] | Cross-sectional study. | 42 | Women with an average age of 84.2 (±6.5) years (range, 70–99 years). | Non-demented institutionalized older population. | Fried’s criteria. | There was a significant and inverse relationship between the number of fulfilled frailty criteria and the lymphocyte count. |
| Nishijima et al., 2017 [21] | Cross-sectional study. | 133 | 54 women and 79 men with a median age of 74 years (range 65–92). | Cancer patients. | 36-item CFI. | Although the lymphocyte count in isolation was not related to frailty, the NLR was positively correlated with the frailty. Patients with a higher NLR also had increased odds of being frail/pre-frail. |
| Hou et al., 2018 [36] | Cross-sectional study. | 345 | 154 women and 191 men with a median age of 71.0 years (IQR 65.0–77.0 years). | Elderly patients with coronary heart disease, (ACS (83.6%) and single-vessel disease (66.4%)). | Fried’s criteria. | A significant positive correlation was observed between NLR and the frailty score, and increased odds of being frail. |
| Fernández-Garrido et al., 2018 [32] | Two-year follow-up study. | 94 | Women with an average age of 82 (±7) years. | Non-demented institutionalized older women. | Fried’s criteria. | There was a significant inverse correlation between the frailty scores and lymphocyte counts at baseline, but not at follow-up. |
| Bernabeu-Wittel et al., 2019 [27] | Multicenter cohort study. | 444 | 200 women and 244 men with an average age of 77.3 (±8.4) years. | Community-dwelling (93.7%) and institutionalized (6.3%) older patients (outpatients in the Internal Medicine and Geriatric areas). | Fried’s criteria. | The combined presence of frailty and sarcopenia was associated with a lower lymphocyte count. |
| Wilson et al., 2019 [19] | Observational cohort study. | 377 | 185 women and 192 men with an average of 73.7 years (range, 50–98 years). | Patients hip fracture. | Modified 11-item frailty index score. | Total lymphocyte count weakly inversely correlated with frailty. |
| Navarro Martínez et al., 2019 [37] | Cross-sectional clinical trial. | 46 | Men with an average age of 72.2 (±9.4) years (range, 51–92 years). | Patients with prostate cancer undergoing antiandrogen therapy. | Fried’s criteria. | The lymphocyte counts were significantly lower in both frail and prefrail individuals than in robust individuals. |
| Marcos-Pérez et al., 2019 [38] | Cross-sectional study. | 259 | 174 women and 85 men with an age range of 65–102 years. | Patients were contacted through associations of older or retired people, day care centers, and nursing homes. | Fried’s criteria. | The relationship between frailty and lymphocyte count was not studied in isolation. |
| Núñez et al., 2020 [18] | Observational study. | 488 | 200 women and 188 men with an average age of 78 (±7) years. | Patients surviving an episode of an ACS. | Fried’s criteria. | The low percentage of lymphocytes was associated with frailty and a higher risk of being frail. |
| Buigues et al., 2020 [28] | One-year follow-up study. | 39 | Men with an average age of 71.9 (± 9.8) years. | Patients with prostate cancer undergoing antiandrogen therapy. | Fried’s criteria | At baseline lower lymphocytes count were significantly correlated with the frailty syndrome severity and predicted its progression at one year of follow-up. |
| Samson et al., 2020 [39] | Observational cohort study. | 289 | 144 women and 145 men between 60–87 years of age. | Elderly people. | Frailty index containing 36 possible “health deficits”. | The relationship between frailty and the total lymphocyte count was not studied (they studied separately subpopulations of T cells, B cells, NK cells counts). |
| Bodolea et al., 2020 [26] | Observational cohort study. | 179 | 101 women and 78 men with an average age of 65.07 (±12.9) years (range, 23–90 years). | Patients with cardiovascular disease | Fried’s criteria. | Lower lymphocyte count and NLR were significantly correlated with the frailty syndrome and its severity. |
| Bilgin et al., 2021 [30] | Observational cohort study. | 108 | 57 women and 51 men. Median ages of the frail and non-frail groups were 65 (50–78) years and 62 (50–79) years, respectively. | Patients with type 2 diabetes mellitus. | Edmonton Frail Scale. | Elevated MPVLR were significantly correlated with the frailty syndrome and its severity. |
| Gilmore et al., 2021 [29] | Longitudinal cohort study. | 581 | Women. Age range, 22–81 years. | Women with stage I-IIIC breast cancer. | Fried’s criteria modified | Low lymphocyte counts and the NLR were associated with post-chemotherapy frailty, as well as changes in frailty from pre-chemotherapy to post-chemotherapy. |
3.2. Relationship between Lymphocyte Subtypes and the Presence of Frailty Syndrome and Its Severity
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Fernández-Garrido, J.; Ruiz-Ros, V.; Buigues, C.; Navarro-Martinez, R.; Cauli, O. Clinical features of prefrail older individuals and emerging peripheral biomarkers: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 7–17. [Google Scholar] [CrossRef]
- Leng, S.; Chen, X.; Mao, G. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Gill, T.M.; Gahbauer, E.A.; Allore, H.G.; Han, L. Transitions between frailty states among community-living older persons. Arch. Intern. Med. 2006, 166, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Jansen-Duerr, P.; Viña, J. Laboratory biomarkers and frailty: Presentation of the FRAILOMIC initiative. Clin. Chem. Lab. Med. 2015, 53, e253–e255. [Google Scholar] [CrossRef] [PubMed]
- Howlett, S.E.; Rockwood, M.R.H.; Mitnitski, A.; Rockwood, K. Standard laboratory tests to identify older adults at increased risk of death. BMC Med. 2014, 12, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchis, J.; Núñez, E.; Ruiz, V.; Bonanad, C.; Fernández, J.; Cauli, O.; García-Blas, S.; Mainar, L.; Valero, E.; Rodríguez-Borja, E.; et al. Usefulness of Clinical Data and Biomarkers for the Identification of Frailty After Acute Coronary Syndromes. Can. J. Cardiol. 2015, 31, 1462–1468. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.X.; Xue, Q.L.; Tian, J.; Huang, Y.; Yeh, S.H.; Fried, L.P. Associations of neutrophil and monocyte counts with frailty in community-dwelling disabled older women: Results from the Women’s Health and Aging Studies I. Exp. Gerontol. 2009, 44, 511–516. [Google Scholar] [CrossRef]
- Yao, X.; Li, H.; Leng, S.X. Inflammation and Immune System Alterations in Frailty. Clin. Geriatr. Med. 2011, 27, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collerton, J.; Martin-Ruiz, C.; Davies, K. Frailty and the role of inflammation, immunosenescence and cellular ageing in the very old: Cross-sectional findings from the Newcastle 85+ Study. Mech. Ageing Dev. 2012, 133, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Bencivenga, L.; Poto, R.; Pecoraro, A.; Shamji, M.H.; Rengo, G. The emerging role of T follicular helper (TFH) cells in aging: Influence on the immune frailty. Ageing Res. Rev. 2020, 61, 101071. [Google Scholar] [CrossRef]
- De Araújo, A.L.; Silva, L.C.R.; Fernandes, J.R.; Benard, G. Preventing or reversing immunosenescence: Can exercise be an immunotherapy? Immunotherapy 2013, 5, 879–893. [Google Scholar] [CrossRef] [Green Version]
- Izaks, G.J.; Remarque, E.J.; Becker, S.V.; Westendorp, R.G.J. Lymphocyte count and mortality risk in older persons. The Leiden 85-plus study. J. Am. Geriatr. Soc. 2003, 51, 1461–1465. [Google Scholar] [CrossRef]
- Fernández-Garrido, J.; Navarro-Martínez, R.; Buigues-González, C.; Martínez-Martínez, M.; Ruiz-Ros, V.; Cauli, O. The value of neutrophil and lymphocyte count in frail older women. Exp. Gerontol. 2014, 54, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Pérez, D.; Sánchez-Flores, M.; Maseda, A. Frailty in older adults is associated with plasma concentrations of inflammatory mediators but not with lymphocyte subpopulations. Front. Immunol. 2018, 9, 1056. [Google Scholar] [CrossRef] [Green Version]
- Núñez, J.; Sastre, C.; D’Ascoli, G. Relation of Low Lymphocyte Count to Frailty and its Usefulness as a Prognostic Biomarker in Patients >65 Years of Age With Acute Coronary Syndrome. Am. J. Cardiol. 2020, 125, 1033–1038. [Google Scholar] [CrossRef]
- Wilson, J.M.; Boissonneault, A.R.; Schwartz, A.M.; Staley, C.A.; Schenker, M.L. Frailty and Malnutrition Are Associated With Inpatient Postoperative Complications and Mortality in Hip Fracture Patients. J. Orthop. Trauma 2019, 33, 143–148. [Google Scholar] [CrossRef]
- Semba, R.D.; Margolick, J.B.; Leng, S.; Walston, J.; Ricks, M.O.; Fried, L.P. T cell subsets and mortality in older community-dwelling women. Exp. Gerontol. 2005, 40, 81–87. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Deal, A.M.; Williams, G.R.; Guerard, E.J.; Nyrop, K.A.; Muss, H.B. Frailty and inflammatory markers in older adults with cancer. Aging 2017, 9, 650–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmaltz, H.N.; Fried, L.P.; Xue, Q.L.; Walston, J.; Leng, S.X.; Semba, R.D. Chronic cytomegalovirus infection and inflammation are associated with prevalent frailty in community-dwelling older women. J. Am. Geriatr. Soc. 2005, 53, 747–754. [Google Scholar] [CrossRef] [PubMed]
- De Fanis, U.; Wang, G.C.; Fedarko, N.S.; Walston, J.D.; Casolaro, V.; Leng, S.X. T-lymphocytes expressing CC chemokine receptor-5 are increased in frail older adults. J. Am. Geriatr. Soc. 2008, 56, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Abizanda Soler, P.; Gómez-Pavón, J.; Martín Lesende, I.; Baztán Cortés, J.J. Frailty detection and prevention: A new challenge in elderly for dependence prevention. Med. Clin. 2010, 135, 713–719. [Google Scholar] [CrossRef]
- Nielsen, H.B. Lymphocyte responses to maximal exercise: A physiological perspective. Sport. Med. 2003, 33, 853–867. [Google Scholar] [CrossRef] [PubMed]
- Bodolea, C.; Hiriscau, E.I.; Buzdugan, E.-C. The Association between Peripheral Blood Cells and the Frailty Syndrome in Patients with Cardiovascular Diseases. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 1419–1433. [Google Scholar] [CrossRef]
- Bernabeu-Wittel, M.; González-Molina, Á.; Fernández-Ojeda, R. Impact of Sarcopenia and Frailty in a Multicenter Cohort of Polypathological Patients. J. Clin. Med. 2019, 8, 535. [Google Scholar] [CrossRef] [Green Version]
- Buigues, C.; Navarro-Martínez, R.; Sánchez-Martínez, V.; Serrano-Carrascosa, M.; Rubio-Briones, J.; Cauli, O. Interleukin-6 and lymphocyte count associated and predicted the progression of frailty syndrome in prostate cancer patients undergoing antiandrogen therapy. Cancers 2020, 12, 1716. [Google Scholar] [CrossRef]
- Gilmore, N.; Mohile, S.; Lei, L. The longitudinal relationship between immune cell profiles and frailty in patients with breast cancer receiving chemotherapy. Breast Cancer Res. 2021, 23, 19. [Google Scholar] [CrossRef]
- Bilgin, S.; Aktas, G.; Kahveci, G.; Tel, A.B.; Kurtkulagi, O.; Duman, T.T. Does mean platelet volume/lymphocyte count ratio associate with frailty in type 2 diabetes mellitus? Bratisl. Med. J. 2021, 122, 116–119. [Google Scholar] [CrossRef]
- Faria, S.S.; Fernandes, P.C.; Silva, M.J.B. The neutrophil-to-lymphocyte ratio: A narrative review. Ecancermedicalscience 2016, 10, 702. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Garrido, J.; Ruiz-Ros, V.; Navarro-Martínez, R. Frailty and leucocyte count are predictors of all-cause mortality and hospitalization length in non-demented institutionalized older women. Exp. Gerontol. 2018, 103, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Falandry, C.; Gilson, E.; Rudolph, K.L. Are aging biomarkers clinically relevant in oncogeriatrics? Crit. Rev. Oncol. Hematol. 2013, 85, 257–265. [Google Scholar] [CrossRef]
- Brodin, P.; Davis, M.M. Human immune system variation. Nat. Rev. Immunol. 2017, 17, 21–29. [Google Scholar] [CrossRef]
- Globerson, A.; Effros, R.B. Ageing of lymphocytes and lymphocytes in the aged. Immunol. Today 2000, 21, 515–521. [Google Scholar] [CrossRef]
- Hou, P.; Xue, H.P.; Mao, X.E.; Li, Y.N.; Wu, L.F.; Liu, Y.B. Inflammation markers are associated with frailty in elderly patients with coronary heart disease. Aging 2018, 10, 2636–2645. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Martínez, R.; Serrano-Carrascosa, M.; Buigues, C. Frailty syndrome is associated with changes in peripheral inflammatory markers in prostate cancer patients undergoing androgen deprivation therapy. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 976–987. [Google Scholar] [CrossRef]
- Marcos-Pérez, D.; Sánchez-Flores, M.; Maseda, A.; Lorenzo-López, L.; Millán-Calenti, J.C.; Pásaro, E.; Laffon, B.; Valdiglesias, V. Serum cortisol but not oxidative stress biomarkers are related to frailty: Results of a cross-sectional study in Spanish older adults. J. Toxicol. Environ. Health A 2019, 82, 815–825. [Google Scholar] [CrossRef]
- Samson, L.D.; Boots, A.M.; Ferreira, J.A. In-depth immune cellular profiling reveals sex-specific associations with frailty. Immun. Ageing 2020, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Johar, H.; Emeny, R.T.; Bidlingmaier, M. Blunted diurnal cortisol pattern is associated with frailty: A cross-sectional study of 745 participants aged 65 to 90 years. J. Clin. Endocrinol. Metab. 2014, 99, E464–E468. [Google Scholar] [CrossRef]
- Varadhan, R.; Walston, J.; Cappola, A.R.; Carlson, M.C.; Wand, G.S.; Fried, L.P. Higher levels and blunted diurnal variation of cortisol in frail older women. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 190–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubbard, R.E.; O’Mahony, M.S.; Calver, B.L.; Woodhouse, K.W. Nutrition, inflammation, and leptin levels in aging and frailty. J. Am. Geriatr. Soc. 2008, 56, 279–284. [Google Scholar] [CrossRef]
- Cross, M.B.; Yi, P.H.; Thomas, C.F.; Garcia, J.; Della Valle, C.J. Evaluation of malnutrition in orthopaedic surgery. J. Am. Acad. Orthop. Surg. 2014, 22, 193–199. [Google Scholar] [CrossRef]
- Imtiaz, F.; Shafique, K.; Mirza, S.; Ayoob, Z.; Vart, P.; Rao, S. Neutrophil lymphocyte ratio as a measure of systemic inflammation in prevalent chronic diseases in Asian population. Int. Arch. Med. 2012, 5, 2. [Google Scholar] [CrossRef]
- Mazari, L.; Lesourd, B.M. Nutritional influences on immune response in healthy aged persons. Mech. Ageing Dev. 1998, 104, 25–40. [Google Scholar] [CrossRef]
- Wikby, A.; Johansson, B.; Olsson, J.; Löfgren, S.; Nilsson, B.O.; Ferguson, F. Expansions of peripheral blood CD8 T-lymphocyte subpopulations and an association with cytomegalovirus seropositivity in the elderly: The Swedish NONA immune study. Exp. Gerontol. 2002, 37, 445–453. [Google Scholar] [CrossRef]
- Michel, J.J.; Griffin, P.; Vallejo, A.N. Functionally diverse NK-like T cells are effectors and predictors of successful aging. Front. Immunol. 2016, 7, 530. [Google Scholar] [CrossRef] [Green Version]
- Tian, Y.; Babor, M.; Lane, J. Unique phenotypes and clonal expansions of human CD4 effector memory T cells re-expressing CD45RA. Nat. Commun. 2017, 8, 1473. [Google Scholar] [CrossRef]
- Sallusto, F.; Lenig, D.; Mackay, C.R.; Lanzavecchia, A. Flexible programs of chemokine receptor expression on human polarized T helper 1 and 2 lymphocytes. J. Exp. Med. 1998, 187, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Pennock, N.D.; White, J.T.; Cross, E.W.; Cheney, E.E.; Tamburini, B.A.; Kedl, R.M. T cell responses: Naïve to memory and everything in between. Am. J. Physiol. Adv. Physiol. Educ. 2013, 37, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.E.C.; De Oda, J.M.M.; Losi Guembarovski, R. CC chemokine receptor 5: The interface of host immunity and cancer. Dis. Markers. 2014, 2014, 126954. [Google Scholar] [CrossRef]
- Theou, O.; Jones, G.R.; Overend, T.J.; Kloseck, M.; Vandervoort, A.A. An exploration of the association between frailty and muscle fatigue. Appl. Physiol. Nutr. Metab. 2008, 33, 651–665. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Aran, L.; Bulli, G.; Curcio, F.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Sarcopenia: Assessment of disease burden and strategies to improve outcomes. Clin. Interv. Aging 2018, 13, 913–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, W.J.; Paolisso, G.; Abbatecola, A.M.; Corsonello, A.; Bustacchini, S.; Strollo, F.; Lattanzio, F. Frailty and muscle metabolism dysregulation in the elderly. Biogerontology 2010, 11, 527–536. [Google Scholar] [CrossRef]
- Ávila-Funes, J.A.; Helmer, C.; Amieva, H.; Barberger-Gateau, P.; Le Goff, M.; Ritchie, K.; Portet, F.; Carrière, I.; Tavernier, B.; Gutiérrez-Robledo, L.M.; et al. Frailty among community-dwelling elderly people in France: The three-city study. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 1089–1096. [Google Scholar] [CrossRef]
- Shinkai, S.; Konishi, M.; Shephard, R.J. Aging and immune response to exercise. Can. J. Physiol. Pharmacol. 1998, 76, 562–572. [Google Scholar] [CrossRef]
- Senchina, D.S.; Kohut, M.L. Immunological outcomes of exercise in older adults. Clin. Interv. Aging 2007, 2, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Kapasi, Z.F.; Ouslander, J.G.; Schnelle, J.F.; Kutner, M.; Fahey, J.L. Effects of an exercise intervention on immunologic parameters in frail elderly nursing home residents. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, 636–643. [Google Scholar] [CrossRef] [Green Version]
- Leng, S.X.; Yang, H.; Walston, J.D. Decreased cell proliferation and altered cytokine production in frail older adults. Aging Clin. Exp. Res. 2004, 16, 249–252. [Google Scholar] [CrossRef]
- Wu, I.C.; Shiesh, S.C.; Kuo, P.H.; Lin, X.Z. High oxidative stress is correlated with frailty in elderly Chinese. J. Am. Geriatr. Soc. 2009, 57, 1666–1671. [Google Scholar] [CrossRef]
- Coto Montes, A.; Boga, J.A.; Bermejo Mill, C.; Rubio González, A.; Potes Ochoa, Y.; Vega Naredo, I.; Martínez Reig, M.; Romero Rizos, L.; Sánchez Jurado, P.M.; Solano, J.J.; et al. Potential early biomarkers of sarcopenia among independent older adults. Maturitas 2017, 104, 117–122. [Google Scholar] [CrossRef]
- Everds, N.E.; Snyder, P.W.; Bailey, K.L.; Bolon, B.; Creasy, D.M.; Foley, G.L.; Rosol, T.J.; Sellers, T. Interpreting stress responses during routine toxicity studies: A review of the biology, impact, and assessment. Toxicol Pathol. 2013, 41, 560–614. [Google Scholar] [CrossRef]
- Schleimer, R.P. Glucocorticoids suppress inflammation but spare innate immune responses in airway epithelium. Proc. Am. Thorac. Soc. 2004, 1, 222–230. [Google Scholar] [CrossRef]
- Thomson, S.P.; McMahon, L.J.; Nugent, C.A. Endogenous cortisol: A regulator of the number of lymphocytes in peripheral blood. Clin. Immunol. Immunopathol. 1980, 17, 506–514. [Google Scholar] [CrossRef]
- Anisman, H.; Merali, Z. Cytokines, stress and depressive illness: Brain-immune interactions. Ann. Med. 2003, 35, 2–11. [Google Scholar] [CrossRef] [PubMed]

| Reference Sorted by Year of Publication | Study Design | Sample Size (n) | Subjects (Sex and Age) | Disease/Patients | Frailty Definition | Lymphocyte Subtypes Studied | Relationship between Lymphocyte and Subtypes Count and Frailty |
|---|---|---|---|---|---|---|---|
| Semba et al., 2005 [20] | Case-control study | 61 women who died (cases) to 61 women who did not die (controls) during follow-up were matched | Women (cases) with a mean age of 76.9 (6.4) years and women (controls) 77.3 (±6.8) years. | Community-dwelling adults. | Fried’s criteria. | Counts or percentages of CD4+, CD8+, CD4+CD28-, CD4+CD28+, CD8+CD28-, CD8+CD28-, CD4+CD45RA+, CD4+CD45RO+, CD8+CD45RA+, CD8+CD45RO+ T cells and CD4/CD8 T cells ratio. | Frail women appeared to have significantly higher CD8+ and CD8+CD28− lymphocyte counts. Frail women also had significantly lower CD4+, lower CD4+CD28+, higher CD8+, higher CD8+CD28-, and lower CD8+CD28+ percentages |
| De Fanis et al., 2008 [23] | Case-control study | 26 frail and no frail participants were matched. | 84,6 % were women and 15.4% men with a mean age of 83.8 ± 5.3 years (range 72–94). | Community-dwelling adults. | Fried’s criteria | Counts of CD3+, CD4+, CD8+, CD45RO+,CD45RO-, CCR5+, CCR5+ CD4+, CCR5+CD8+, CCR5+CD45RO+ and CCR5+CD45RO-T cells. | Frail participants had higher CCR5+, CCR5+CD8+, and CCR5+CD45RO- T-cell counts than matched non-frail controls. |
| Collerton et al., 2012 [12] | Cross-sectional study | 845 patients. | +85 year old. | Community-dwelling or institutionalized older people. | Rockwood frailty index and scale Fried. | Count and ratios of CD4/CD8 T cells, memory/naïve CD4 and CD8 T cells and memory/naïve B cells. | High levels lymphocytes memory/naïve CD8 T cell ratio were associated with a lower risk of frailty on the Fried scale and low levels of memory/naïve B cells were associated with a higher risk of frailty on the Rockwood frailty index. |
| Marcos-Pérez et al., 2019 [38] | Cross-sectional study | 259 patients. | 85 male and 174 female with an age range of 65–102 years. | Patients were contacted through associations of older or retired people, day-care centers, and nursing homes. | Fried’s criteria. | Percentages of CD3+, CD4+ and CD8+ T cells, CD19+ B cells, CD16+56+ NK cells and CD4/CD8 T cells ratio. | A significant increase in the CD4+/CD8+ ratio and a significant decrease in the % CD19+ cells were observed in the frail group. |
| Samson et al., 2020 [39] | Observational cohort study. | 289 patients. | 145 men and 144 women between 60–87 years of age. | Elderly people. | Frailty index with incorporates 36 possible “health deficits” | The numbers of CD16 and CD56 NK cells, CD56+ T cells and CCR7 + CD4 +/CD8 T cells, which were classified as naïve (CCR7+CD45RA+) or central memory (CCR7 + CD45RA-) T cells. CCR7-CD4 +/CD8 + T cells were divided into effector memory T cells (Tem, CCR7-CD45RA-) and effector memory T cells that re-express CD45RA T cells (TemRA, CCR7-CD45RA +). | More frail women, but not men, showed fewer CD56 + T cells and fewer CD4 + TemRA cells. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Martínez, R.; Cauli, O. Lymphocytes as a Biomarker of Frailty Syndrome: A Scoping Review. Diseases 2021, 9, 53. https://doi.org/10.3390/diseases9030053
Navarro-Martínez R, Cauli O. Lymphocytes as a Biomarker of Frailty Syndrome: A Scoping Review. Diseases. 2021; 9(3):53. https://doi.org/10.3390/diseases9030053
Chicago/Turabian StyleNavarro-Martínez, Rut, and Omar Cauli. 2021. "Lymphocytes as a Biomarker of Frailty Syndrome: A Scoping Review" Diseases 9, no. 3: 53. https://doi.org/10.3390/diseases9030053
APA StyleNavarro-Martínez, R., & Cauli, O. (2021). Lymphocytes as a Biomarker of Frailty Syndrome: A Scoping Review. Diseases, 9(3), 53. https://doi.org/10.3390/diseases9030053