
Metabolic Profiling of Pregnant Women with Obesity: An Exploratory Study in Women at Greater Risk of Gestational Diabetes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Study Procedures
2.3. Diagnosis of GDM
2.4. Metabolic Profiling
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
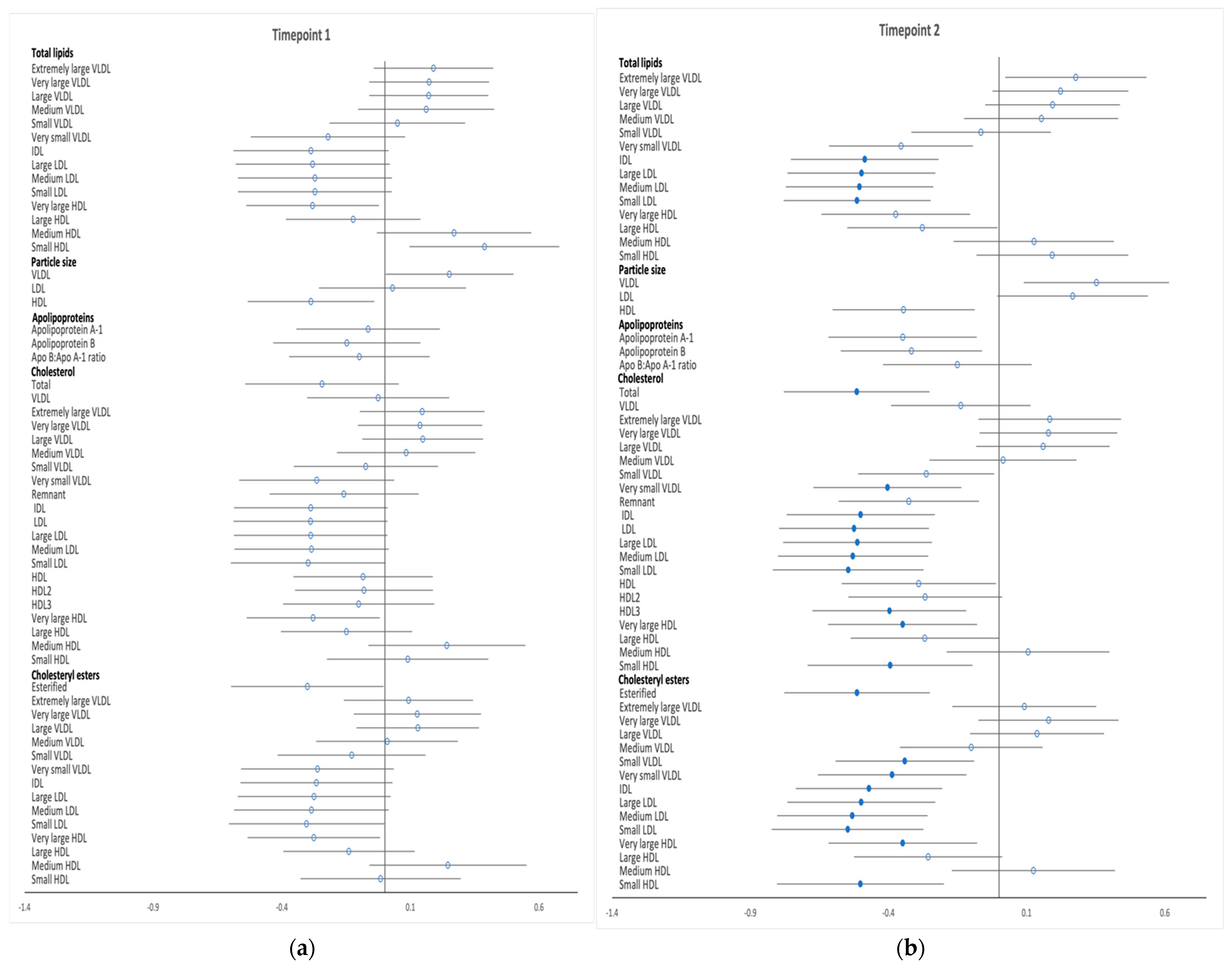
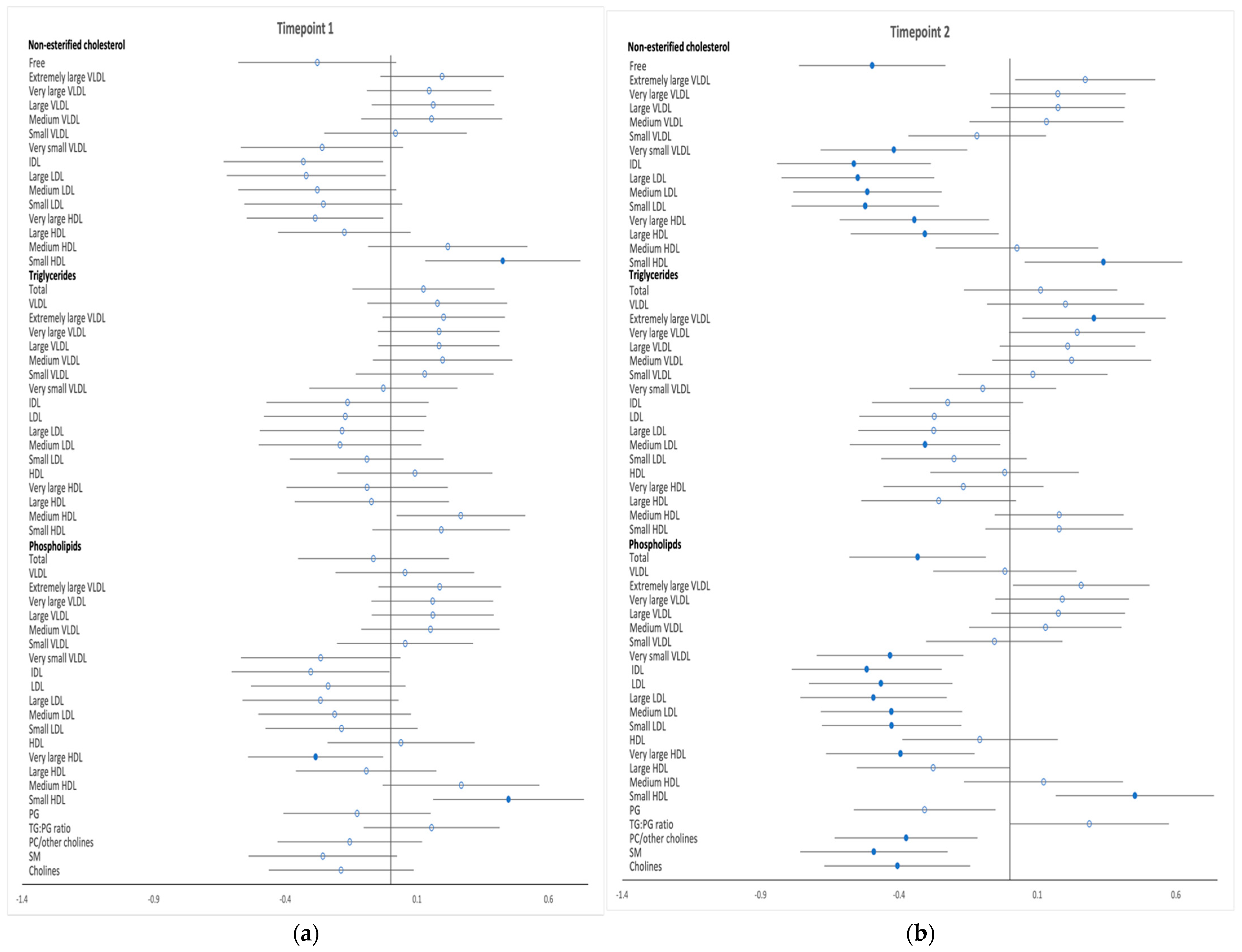
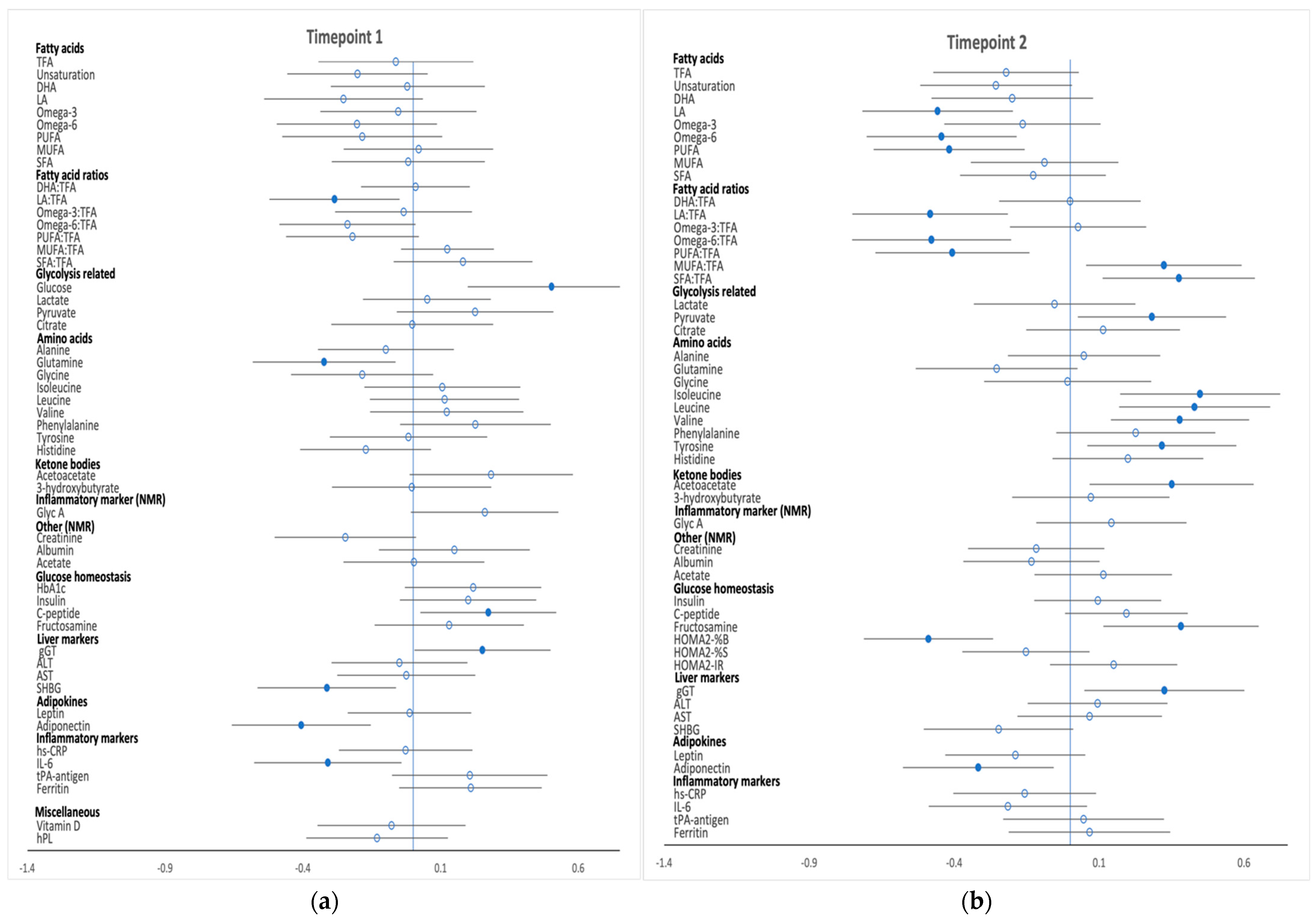
3.2. Metabolic Profiles
3.2.1. Timepoint 1 (15+0 to 18+6 Weeks Gestation)
3.2.2. Timepoint 2 (OGTT, 23+2 to 30+0 Weeks Gestation)
4. Discussion
4.1. Timepoint 1 (Non-Fasting Sample at Baseline; 15+0 to 18+6 Weeks’ Gestation)
4.2. Timepoint 2 (Fasting Sample at Time of Diagnostic OGTT; 23+2 to 30+0 Weeks’ Gestation)
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lain, K.Y.; Catalano, P.M. Metabolic Changes in Pregnancy. Clin. Obstet. Gynecol. 2007, 50, 938–948. [Google Scholar] [CrossRef] [PubMed]
- Johns, E.C.; Denison, F.C.; Norman, J.E.; Reynolds, R.M. Gestational Diabetes Mellitus: Mechanisms, Treatment, and Complications. Trends Endocrinol. Metab. 2018, 29, 743–754. [Google Scholar] [CrossRef] [PubMed]
- King, J.C. Maternal Obesity, Metabolism, and Pregnancy Outcomes. Annu. Rev. Nutr. 2006, 26, 271–291. [Google Scholar] [CrossRef] [PubMed]
- White, S.L.; Pasupathy, D.; Sattar, N.; Nelson, S.M.; Lawlor, D.A.; Briley, A.L.; Seed, P.T.; Welsh, P.; Poston, L. Metabolic Profiling of Gestational Diabetes in Obese Women during Pregnancy. Diabetologia 2017, 60, 1903–1912. [Google Scholar] [CrossRef]
- Catalano, P.M. The Impact of Gestational Diabetes and Maternal Obesity on the Mother and Her Offspring. J. Dev. Orig. Health Dis. 2010, 1, 208–215. [Google Scholar] [CrossRef]
- Bryson, C.L.; Ioannou, G.N.; Rulyak, S.J.; Critchlow, C. Association between Gestational Diabetes and Pregnancy-Induced Hypertension. Am. J. Epidemiol. 2003, 158, 1148–1153. [Google Scholar] [CrossRef]
- Billionnet, C.; Mitanchez, D.; Weill, A.; Nizard, J.; Alla, F.; Hartemann, A.; Jacqueminet, S. Gestational Diabetes and Adverse Perinatal Outcomes from 716,152 Births in France in 2012. Diabetologia 2017, 60, 636–644. [Google Scholar] [CrossRef]
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational Diabetes and the Risk of Cardiovascular Disease in Women: A Systematic Review and Meta-Analysis. Diabetologia 2019, 62, 905–914. [Google Scholar] [CrossRef]
- Pathirana, M.M.; Lassi, Z.S.; Ali, A.; Arstall, M.A.; Roberts, C.T.; Andraweera, P.H. Association between Metabolic Syndrome and Gestational Diabetes Mellitus in Women and Their Children: A Systematic Review and Meta-Analysis. Endocrine 2020, 71, 310–320. [Google Scholar] [CrossRef]
- Wishart, D.S. Metabolomics for Investigating Physiological and Pathophysiological Processes. Physiol. Rev. 2019, 99, 1819–1875. [Google Scholar] [CrossRef]
- Enquobahrie, D.A.; Denis, M.; Tadesse, M.G.; Gelaye, B.; Ressom, H.W.; Williams, M.A. Maternal Early Pregnancy Serum Metabolites and Risk of Gestational Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2015, 100, 4348–4356. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Ma, S.; You, Y.; Long, S.; Zhang, J.; Guo, C.; Wang, X.; Tan, H. Serum Metabolites as an Indicator of Developing Gestational Diabetes Mellitus Later in the Pregnancy: A Prospective Cohort of a Chinese Population. J. Diabetes Res. 2021, 2021, 8885954. [Google Scholar] [CrossRef] [PubMed]
- Pinto, J.; Almeida, L.M.; Martins, A.S.; Duarte, D.; Barros, A.S.; Galhano, E.; Pita, C.; Almeida, M.D.C.; Carreira, I.M.; Gil, A.M. Prediction of Gestational Diabetes through NMR Metabolomics of Maternal Blood. J. Proteome Res. 2015, 14, 2696–2706. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, D.M.; Muehlbauer, M.J.; Daya, N.R.; Stevens, R.D.; Dyer, A.R.; Lowe, L.P.; Metzger, B.E.; Newgard, C.B.; Bain, J.R.; Lowe, W.L. Metabolomics Reveals Broad-Scale Metabolic Perturbations in Hyperglycemic Mothers during Pregnancy. Diabetes Care 2014, 37, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Mokkala, K.; Vahlberg, T.; Pellonperä, O.; Houttu, N.; Koivuniemi, E.; Laitinen, K. Distinct Metabolic Profile in Early Pregnancy of Overweight and Obese Women Developing Gestational Diabetes. J. Nutr. 2020, 150, 31–37. [Google Scholar] [CrossRef]
- Guo, F.; Yang, S.; Zhang, Y.; Yang, X.; Zhang, C.; Fan, J. Nomogram for Prediction of Gestational Diabetes Mellitus in Urban, Chinese, Pregnant Women. BMC Pregnancy Childbirth 2020, 20, 43. [Google Scholar] [CrossRef]
- Harrison, C.L.; Lombard, C.B.; East, C.; Boyle, J.; Teede, H.J. Risk Stratification in Early Pregnancy for Women at Increased Risk of Gestational Diabetes. Diabetes Res. Clin. Pract. 2015, 107, 61–68. [Google Scholar] [CrossRef]
- Nanda, S.; Savvidou, M.; Syngelaki, A.; Akolekar, R.; Nicolaides, K.H. Prediction of Gestational Diabetes Mellitus by Maternal Factors and Biomarkers at 11 to 13 Weeks. Prenat. Diagn. 2011, 31, 135–141. [Google Scholar] [CrossRef]
- Abell, S.K.; Shorakae, S.; Boyle, J.A.; De Courten, B.; Stepto, N.K.; Teede, H.J.; Harrison, C.L. Role of Serum Biomarkers to Optimise a Validated Clinical Risk Prediction Tool for Gestational Diabetes. Aust. New Zeal. J. Obstet. Gynaecol. 2019, 59, 251–257. [Google Scholar] [CrossRef]
- Donovan, B.M.; Breheny, P.J.; Robinson, J.G.; Baer, R.J.; Saftlas, A.F.; Bao, W.; Greiner, A.L.; Carter, K.D.; Oltman, S.P.; Rand, L.; et al. Development and Validation of a Clinical Model for Preconception and Early Pregnancy Risk Prediction of Gestational Diabetes Mellitus in Nulliparous Women. PLoS ONE 2019, 14, e0215173. [Google Scholar] [CrossRef] [Green Version]
- Sweeting, A.N.; Appelblom, H.; Ross, G.P.; Wong, J.; Kouru, H.; Williams, P.F.; Sairanen, M.; Hyett, J.A. First Trimester Prediction of Gestational Diabetes Mellitus: A Clinical Model Based on Maternal Demographic Parameters. Diabetes Res. Clin. Pract. 2017, 127, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Thériault, S.; Forest, J.C.; Massé, J.; Giguère, Y. Validation of Early Risk-Prediction Models for Gestational Diabetes Based on Clinical Characteristics. Diabetes Res. Clin. Pract. 2014, 103, 419–425. [Google Scholar] [CrossRef]
- White, S.L.; Lawlor, D.A.; Briley, A.L.; Godfrey, K.M.; Nelson, S.M.; Oteng-Ntim, E.; Robson, S.C.; Sattar, N.; Seed, P.T.; Vieira, M.C.; et al. Early Antenatal Prediction of Gestational Diabetes in Obese Women: Development of Prediction Tools for Targeted Intervention. PLoS ONE 2016, 11, e0167846. [Google Scholar] [CrossRef] [PubMed]
- Poston, L.; Bell, R.; Croker, H.; Flynn, A.C.; Godfrey, K.M.; Goff, L.; Hayes, L.; Khazaezadeh, N.; Nelson, S.M.; Oteng-Ntim, E.; et al. Effect of a Behavioural Intervention in Obese Pregnant Women (the UPBEAT Study): A Multicentre, Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2015, 3, 767–777. [Google Scholar] [CrossRef]
- IADPSG Consensus Panel. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef]
- Würtz, P.; Wang, Q.; Niironen, M.; Tynkkynen, T.; Tiainen, M.; Drenos, F.; Kangas, A.J.; Soininen, P.; Skilton, M.R.; Heikkila, K.; et al. Metabolic Signatures of Birthweight in 18 288 Adolescents and Adults. Int. J. Epidemiol. 2016, 45, 1539–1550. [Google Scholar] [CrossRef]
- Würtz, P.; Havulinna, A.S.; Soininen, P.; Tynkkynen, T.; Prieto-Merino, D.; Tillin, T.; Ghorbani, A.; Artati, A.; Wang, Q.; Tiainen, M.; et al. Metabolite Profiling and Cardiovascular Event Risk: A Prospective Study of 3 Population-Based Cohorts. Circulation 2015, 131, 774–785. [Google Scholar] [CrossRef]
- Wang, Q.; Würtz, P.; Auro, K.; Morin-Papunen, L.; Kangas, A.J.; Soininen, P.; Tiainen, M.; Tynkkynen, T.; Joensuu, A.; Havulinna, A.S.; et al. Effects of Hormonal Contraception on Systemic Metabolism: Cross-Sectional and Longitudinal Evidence. Int. J. Epidemiol. 2016, 45, 1445–1457. [Google Scholar] [CrossRef]
- Wang, Q.; Würtz, P.; Auro, K.; Mäkinen, V.P.; Kangas, A.J.; Soininen, P.; Tiainen, M.; Tynkkynen, T.; Jokelainen, J.; Santalahti, K.; et al. Metabolic Profiling of Pregnancy: Cross-Sectional and Longitudinal Evidence. BMC Med. 2016, 14, 205. [Google Scholar] [CrossRef]
- Würtz, P.; Wang, Q.; Soininen, P.; Kangas, A.J.; Fatemifar, G.; Tynkkynen, T.; Tiainen, M.; Perola, M.; Tillin, T.; Hughes, A.D.; et al. Metabolomic Profiling of Statin Use and Genetic Inhibition of HMG-CoA Reductase. J. Am. Coll. Cardiol. 2016, 67, 1200–1210. [Google Scholar] [CrossRef] [Green Version]
- Soininen, P.; Kangas, A.J.; Würtz, P.; Suna, T.; Ala-Korpela, M. Quantitative Serum Nuclear Magnetic Resonance Metabolomics in Cardiovascular Epidemiology and Genetics. Circ. Cardiovasc. Genet. 2015, 8, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Soininen, P.; Kangas, A.J.; Würtz, P.; Tukiainen, T.; Tynkkynen, T.; Laatikainen, R.; Järvelin, M.R.; Kähönen, M.; Lehtimäki, T.; Viikari, J.; et al. High-Throughput Serum NMR Metabonomics for Cost-Effective Holistic Studies on Systemic Metabolism. Analyst 2009, 134, 1781–1785. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Wannamethee, S.G.; Forouhi, N.G. Novel Biochemical Risk Factors for Type 2 Diabetes: Pathogenic Insights or Prediction Possibilities? Diabetologia 2008, 51, 926–940. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing on JSTOR. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Bozkurt, L.; Göbl, C.S.; Leitner, K.; Pacini, G.; Kautzky-Willer, A. HbA1c during Early Pregnancy Reflects Beta-Cell Dysfunction in Women Developing GDM. BMJ Open Diab. Res. Care 2020, 8, 1751. [Google Scholar] [CrossRef]
- Corrado, F.; D’Anna, R.; Cannata, M.L.; Interdonato, M.L.; Pintaudi, B.; Di Benedetto, A. Correspondence between First-Trimester Fasting Glycaemia, and Oral Glucose Tolerance Test in Gestational Diabetes Diagnosis. Diabetes Metab. 2012, 38, 458–461. [Google Scholar] [CrossRef]
- Jones, A.G.; Hattersley, A.T. The Clinical Utility of C-Peptide Measurement in the Care of Patients with Diabetes. Diabet. Med. 2013, 30, 803. [Google Scholar] [CrossRef]
- Carlessi, R.; Rowlands, J.; Ellison, G.; Helena de Oliveira Alves, H.; Newsholme, P.; Mamotte, C. Glutamine Deprivation Induces Metabolic Adaptations Associated with Beta Cell Dysfunction and Exacerbate Lipotoxicity. Mol. Cell. Endocrinol. 2019, 491, 110433. [Google Scholar] [CrossRef]
- Tulipani, S.; Palau-Rodriguez, M.; Miñarro Alonso, A.; Cardona, F.; Marco-Ramell, A.; Zonja, B.; Lopez de Alda, M.; Muñoz-Garach, A.; Sanchez-Pla, A.; Tinahones, F.J.; et al. Biomarkers of Morbid Obesity and Prediabetes by Metabolomic Profiling of Human Discordant Phenotypes. Clin. Chim. Acta 2016, 463, 53–61. [Google Scholar] [CrossRef]
- Corcoran, S.M.; Achamallah, N.; Loughlin, J.O.; Stafford, P.; Dicker, P.; Malone, F.D.; Breathnach, F. First Trimester Serum Biomarkers to Predict Gestational Diabetes in a High-Risk Cohort: Striving for Clinically Useful Thresholds. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 222, 7–12. [Google Scholar] [CrossRef]
- Wallace, I.R.; McKinley, M.C.; Bell, P.M.; Hunter, S.J. Sex Hormone Binding Globulin and Insulin Resistance. Clin. Endocrinol. (Oxf.) 2013, 78, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Tawfeek, M.A.; Alfadhli, E.M.; Alayoubi, A.M.; El-Beshbishy, H.A.; Habib, F.A. Sex Hormone Binding Globulin as a Valuable Biochemical Marker in Predicting Gestational Diabetes Mellitus. BMC Women’s Health 2017, 17, 18. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.M.; Xu, F.; Darbinian, J.A.; Quesenberry, C.P.; Sridhar, S.; Kim, C.; Gunderson, E.P.; Ferrara, A. Prepregnancy SHBG Concentrations and Risk for Subsequently Developing Gestational Diabetes Mellitus. Diabetes Care 2014, 37, 1296–1303. [Google Scholar] [CrossRef] [PubMed]
- Retnakaran, R.; Hanley, A.J.G.; Raif, N.; Hirning, C.R.; Connelly, P.W.; Sermer, M.; Kahn, S.E.; Zinman, B. Adiponectin and Beta Cell Dysfunction in Gestational Diabetes: Pathophysiological Implications. Diabetologia 2005, 48, 993–1001. [Google Scholar] [CrossRef]
- Hedderson, M.M.; Darbinian, J.; Havel, P.J.; Quesenberry, C.P.; Sridhar, S.; Ehrlich, S.; Ferrara, A. Low Prepregnancy Adiponectin Concentrations Are Associated With a Marked Increase in Risk for Development of Gestational Diabetes Mellitus. Diabetes Care 2013, 36, 3930. [Google Scholar] [CrossRef]
- Iliodromiti, S.; Sassarini, J.; Kelsey, T.W.; Lindsay, R.S.; Sattar, N.; Nelson, S.M. Accuracy of Circulating Adiponectin for Predicting Gestational Diabetes: A Systematic Review and Meta-Analysis. Diabetologia 2016, 59, 692. [Google Scholar] [CrossRef]
- Turer, A.T.; Scherer, P.E. Adiponectin: Mechanistic Insights and Clinical Implications. Diabetologia 2012, 55, 2319–2326. [Google Scholar] [CrossRef]
- Rao, J.R.; Keating, D.J.; Chen, C.; Parkington, H.C. Adiponectin Increases Insulin Content and Cell Proliferation in MIN6 Cells via PPARγ-Dependent and PPARγ-Independent Mechanisms. Diabetes. Obes. Metab. 2012, 14, 983–989. [Google Scholar] [CrossRef]
- Nakamura, A.; Miyoshi, H.; Ukawa, S.; Nakamura, K.; Nakagawa, T.; Terauchi, Y.; Tamakoshi, A.; Atsumi, T. Serum Adiponectin and Insulin Secretion: A Direct or Inverse Association? J. Diabetes Investig. 2018, 9, 1106. [Google Scholar] [CrossRef]
- Kivelä, J.; Sormunen-Harju, H.; Girchenko, P.V.; Huvinen, E.; Stach-Lempinen, B.; Reynolds, R.M.; Hämäläinen, E.K.; Lahti-Pulkkinen, M.; Murtoniemi, K.K.; Räikkönen, K.; et al. Longitudinal Metabolic Profiling of Maternal Obesity, Gestational Diabetes, and Hypertensive Pregnancy Disorders. J. Clin. Endocrinol. Metab. 2021, 106, e4372–e4388. [Google Scholar] [CrossRef]
- Fakhrul-Alam, M.; Rakibul-Hasan, M.; Farid-Uddin, M.; Hasanat, M.A. Insulin Secretory Defect May Be the Major Determinant of GDM in Lean Mothers. J. Clin. Transl. Endocrinol. 2020, 20, 100226. [Google Scholar] [CrossRef] [PubMed]
- Xiang, A.H.; Kjos, S.L.; Takayanagi, M.; Trigo, E.; Buchanan, T.A. Detailed Physiological Characterization of the Development of Type 2 Diabetes in Hispanic Women with Prior Gestational Diabetes Mellitus. Diabetes 2010, 59, 2625–2630. [Google Scholar] [CrossRef]
- Kramer, C.K.; Swaminathan, B.; Hanley, A.J.; Connelly, P.W.; Sermer, M.; Zinman, B.; Retnakaran, R. Each Degree of Glucose Intolerance in Pregnancy Predicts Distinct Trajectories of β-Cell Function, Insulin Sensitivity, and Glycemia in the First 3 Years Postpartum. Diabetes Care 2014, 37, 3262–3269. [Google Scholar] [CrossRef] [PubMed]
- Xiang, A.H.; Kawakubo, M.; Trigo, E.; Kjos, S.L.; Buchanan, T.A. Declining β-Cell Compensation for Insulin Resistance in Hispanic Women With Recent Gestational Diabetes Mellitus. Diabetes Care 2010, 33, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Wang, L.; Liu, H.; Zhang, S.; Tian, H.; Shen, Y.; Tuomilehto, J.; Yu, Z.; Yang, X.; Hu, G.; et al. β-Cell Function or Insulin Resistance Was Associated with the Risk of Type 2 Diabetes among Women with or without Obesity and a History of Gestational Diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001060. [Google Scholar] [CrossRef] [PubMed]
- White, S.L.; Begum, S.; Vieira, M.C.; Seed, P.; Lawlor, D.L.; Sattar, N.; Nelson, S.M.; Welsh, P.; Pasupathy, D.; Poston, L. Metabolic Phenotyping by Treatment Modality in Obese Women with Gestational Diabetes Suggests Diverse Pathophysiology: An Exploratory Study. PLoS ONE 2020, 15, e0230658. [Google Scholar] [CrossRef]
- Bender, T.; Martinou, J.C. The Mitochondrial Pyruvate Carrier in Health and Disease: To Carry or Not to Carry? Biochim. Biophys. Acta—Mol. Cell Res. 2016, 1863, 2436–2442. [Google Scholar] [CrossRef]
- Patterson, J.N.; Cousteils, K.; Lou, J.W.; Manning Fox, J.E.; MacDonald, P.E.; Joseph, J.W. Mitochondrial Metabolism of Pyruvate Is Essential for Regulating Glucose-Stimulated Insulin Secretion. J. Biol. Chem. 2014, 289, 13335–13346. [Google Scholar] [CrossRef]
- Zhang, H.; Forman, H.J.; Choi, J. Gamma-Glutamyl Transpeptidase in Glutathione Biosynthesis. Methods Enzymol. 2005, 401, 468–483. [Google Scholar] [CrossRef]
- Kim, W.J.; Chung, Y.; Park, J.; Park, J.Y.; Han, K.; Park, Y.; Park, I.Y.; Ko, H.S. Influences of Pregravid Liver Enzyme Levels on the Development of Gestational Diabetes Mellitus. Liver Int. 2021, 41, 743–753. [Google Scholar] [CrossRef]
- Leenders, F.; Groen, N.; de Graaf, N.; Engelse, M.A.; Rabelink, T.J.; de Koning, E.J.P.; Carlotti, F. Oxidative Stress Leads to β-Cell Dysfunction Through Loss of β-Cell Identity. Front. Immunol. 2021, 12, 4313. [Google Scholar] [CrossRef]
- Ceriello, A.; Motz, E. Is Oxidative Stress the Pathogenic Mechanism Underlying Insulin Resistance, Diabetes, and Cardiovascular Disease? The Common Soil Hypothesis Revisited. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Maiese, K. New Insights for Oxidative Stress and Diabetes Mellitus. Oxid. Med. Cell. Longev. 2015, 2015, 875961. [Google Scholar] [CrossRef]
- Tangvarasittichai, S. Oxidative Stress, Insulin Resistance, Dyslipidemia and Type 2 Diabetes Mellitus. World J. Diabetes 2015, 6, 456. [Google Scholar] [CrossRef] [PubMed]
- Powe, C.E.; Huston Presley, L.P.; Locascio, J.J.; Catalano, P.M. Augmented Insulin Secretory Response in Early Pregnancy. Diabetologia 2019, 62, 1445–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | GDM (n = 119) | No GDM (n = 112) | p Value a |
|---|---|---|---|
| Ethnicity | 0.41 | ||
| African | 23 (19.3) | 13 (11.6) | |
| African-Caribbean | 11 (9.2) | 8 (7.1) | |
| South Asian | 9 (7.6) | 10 (8.9) | |
| European | 64 (53.8) | 72 (64.3) | |
| Other | 12 (10.1) | 9 (8.0) | |
| Parity | 0.97 | ||
| Nulliparous | 46 (38.7) | 43 (38.4) | |
| Multiparous | 73 (61.3) | 69 (61.6) | |
| Education level | 0.08 | ||
| Degree | 50 (42.0) | 47 (42.0) | |
| A level (or equivalent) | 16 (13.4) | 23 (20.5) | |
| Vocational qualification | 36 (30.2) | 18 (16.1) | |
| GCSE (or equivalent) | 12 (10.1) | 17 (15.2) | |
| None | 5 (4.2) | 7 (6.2) | |
| Smoking status | 0.53 | ||
| Non-smokers | 81 (68.1) | 83 (74.1) | |
| Smokers | 7 (5.9) | 4 (3.6) | |
| Ex-Smokers | 31 (26.0) | 25 (22.3) | |
| Maternal weight (kg) | |||
| At timepoint 1 | 101.9 (20.1) | 102.5 (15.1) | 0.82 |
| At timepoint 2 b | 105.5 (20.5) | 105.9 (15.5) | 0.86 |
| Previous GDM b | 6 (5.0) | 2 (1.8) | 0.24 |
| Family history | |||
| T1DM | 2 (1.7) | 5 (4.5) | 0.22 |
| T2DM | 42 (33.1) | 36 (26.1) | 0.41 |
| Pregnancy outcomes | |||
| Pre-eclampsia b | 6 (5.2) | 10 (9.3) | 0.22 |
| Caesarean section (all) b | 54 (45.8) | 49 (44.5) | 0.85 |
| Caesarean section (emergency) b | 22 (18.6) | 20 (18.2) | 0.93 |
| Preterm delivery (<37 weeks) b | 1 (0.9) | 1 (0.9) | 0.95 |
| LGA (90 th customised centile) b | 16 (13.6) | 5 (4.5) | 0.02 * |
| Birthweight (g) b | 3400 (3120–3720) | 3466 (3070–3785) | 0.44 |
| Gestational age (weeks) | |||
| At timepoint 1 | 16.0 (15.0–16.0) | 16.0 (15.0–17.0) | 0.33 |
| At timepoint 2 b | 27.0 (27.0–28.0) | 27.0 (27.0–28.0) | 0.82 |
| At delivery b | 39.0 (38.3–39.8) | 40.1 (38.8–40.8) | <0.001 * |
| Treatment group | 0.48 | ||
| Control | 64 (53.8) | 55 (49.1) | |
| Intervention | 55 (46.2) | 57 (50.9) | |
| GDM prediction model components (at timepoint 1) | |||
| Maternal age (years) | 32.6 ± 4.3 | 33.6 ± 5.3 | 0.13 |
| BMI (kg/m2) | 36.7 (33.8–40.4) | 36.9 (34.0–41.3) | 0.78 |
| Systolic blood pressure (mmHg) | 123.4 ± 11.1 | 122.3 ± 11.2 | 0.45 |
| Mid-arm circumference (cm) | 39.0 (36.0–41.0) | 38.0 (35.5–41.5) | 0.46 |
| HbA1c (mmol/mol) c | 32.9 ± 3.9 | 31.5 ± 3.4 | 0.006 * |
| Glucose (mmol/l) c | 5.5 ± 1.0 | 5.1 ± 0.7 | 0.001 * |
| Triglycerides (mmol/l) c | 1.0 ± 0.4 | 1.0 ± 0.4 | 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quotah, O.F.; Poston, L.; Flynn, A.C.; White, S.L. Metabolic Profiling of Pregnant Women with Obesity: An Exploratory Study in Women at Greater Risk of Gestational Diabetes. Metabolites 2022, 12, 922. https://doi.org/10.3390/metabo12100922
Quotah OF, Poston L, Flynn AC, White SL. Metabolic Profiling of Pregnant Women with Obesity: An Exploratory Study in Women at Greater Risk of Gestational Diabetes. Metabolites. 2022; 12(10):922. https://doi.org/10.3390/metabo12100922
Chicago/Turabian StyleQuotah, Ola F., Lucilla Poston, Angela C. Flynn, and Sara L. White. 2022. "Metabolic Profiling of Pregnant Women with Obesity: An Exploratory Study in Women at Greater Risk of Gestational Diabetes" Metabolites 12, no. 10: 922. https://doi.org/10.3390/metabo12100922
APA StyleQuotah, O. F., Poston, L., Flynn, A. C., & White, S. L. (2022). Metabolic Profiling of Pregnant Women with Obesity: An Exploratory Study in Women at Greater Risk of Gestational Diabetes. Metabolites, 12(10), 922. https://doi.org/10.3390/metabo12100922