
Salivary Metabolomics for Oral Squamous Cell Carcinoma Diagnosis: A Systematic Review





Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
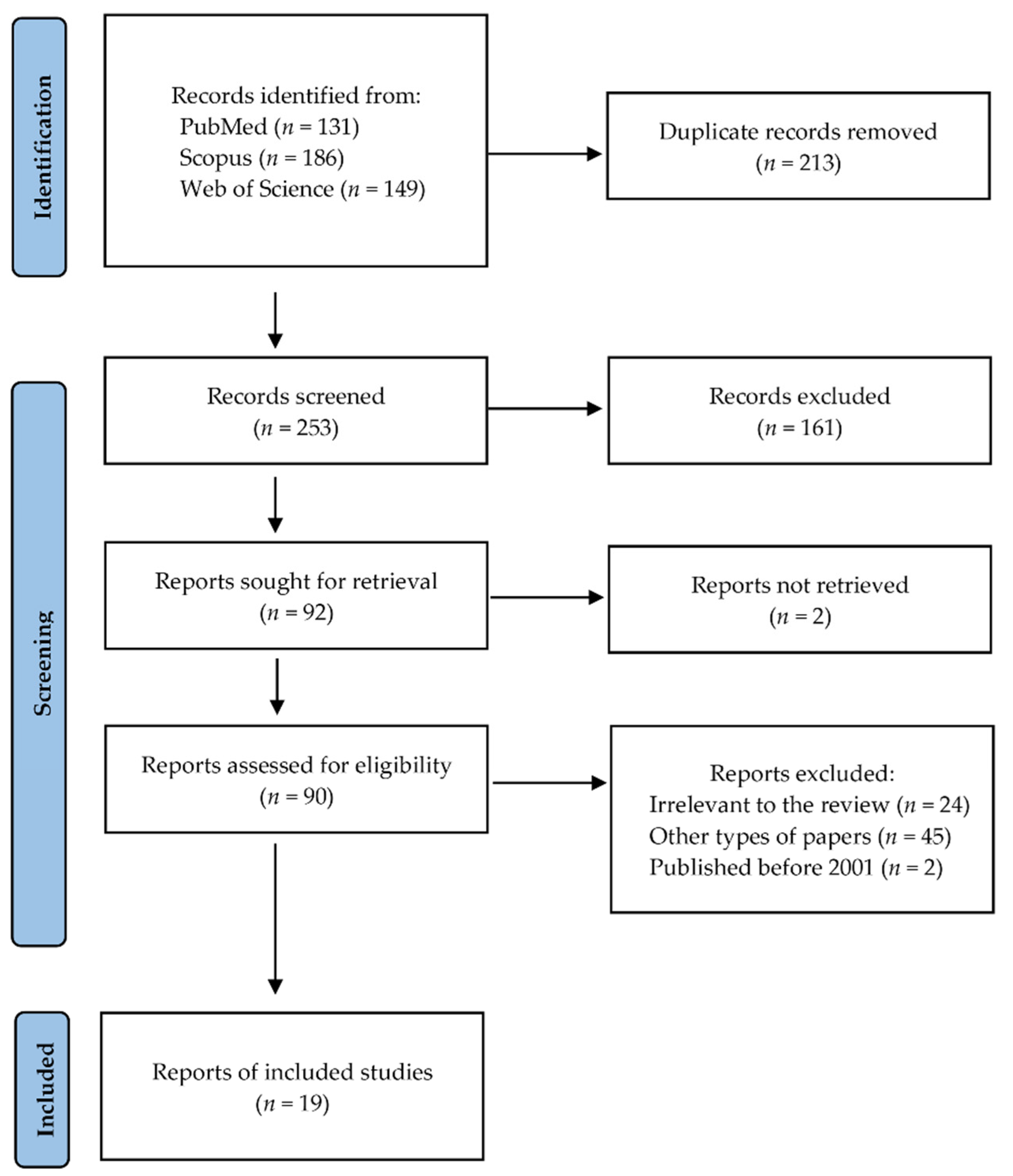
4.1. Search Strategy and Data Extraction
- -
- For PubMed: (((oral OR (head and neck)) AND (cancer OR carcinoma)) OR OSCC) AND saliva AND (metabolite OR metabolomics);
- -
- For Scopus: TITLE-ABS-KEY((((oral OR “head and neck”) AND (cancer OR carcinoma)) OR OSCC) AND saliva AND (metabolite OR metabolomics));
- -
- For Web of Science: TS = ((((oral OR (head and neck)) AND (cancer OR carcinoma)) OR OSCC) AND saliva AND (metabolite OR metabolomics)).
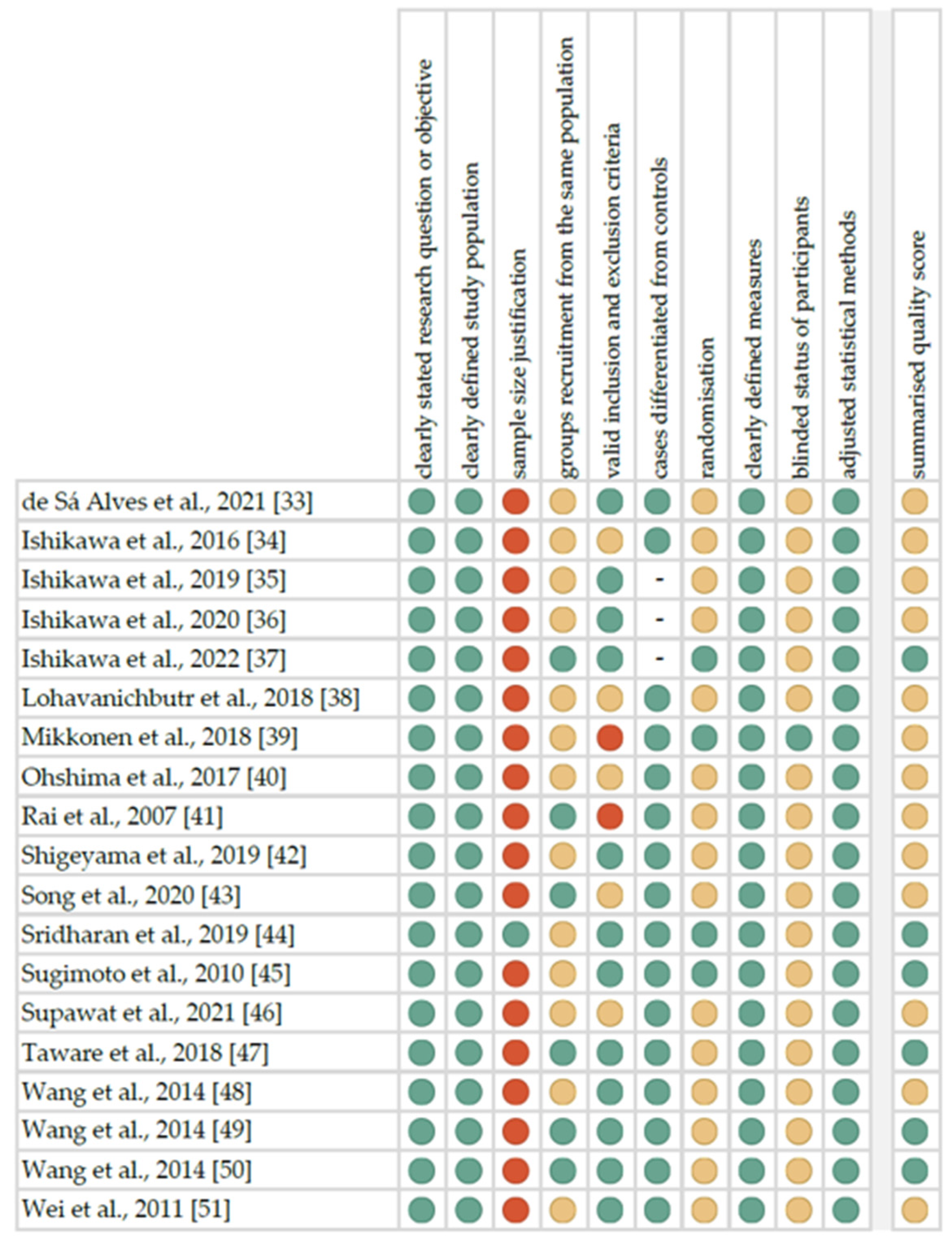
4.2. Quality Assessment and Critical Appraisal for the Systematic Review of Included Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Inchingolo, F.; Santacroce, L.; Ballini, A.; Topi, S.; Dipalma, G.; Haxhirexha, K.; Bottalico, L.; Charitos, I.A. Oral Cancer: A Historical Review. Int. J. Environ. Res. Public Health 2020, 17, 3168. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yu, D. Metabolomics Study of Oral Cancers. Metab. Off. J. Metab. Soc. 2019, 15, 22. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, G.-M.; Panico, R.-L.; Di Tada, C.; Piemonte, E.-D.; Brunotto, M.-N. Clinical and Immunohistochemical Epithelial Profile of Non-Healing Chronic Traumatic Ulcers. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e706–e713. [Google Scholar] [CrossRef]
- Mello, F.W.; Melo, G.; Pasetto, J.J.; Silva, C.A.B.; Warnakulasuriya, S.; Rivero, E.R.C. The Synergistic Effect of Tobacco and Alcohol Consumption on Oral Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2019, 23, 2849–2859. [Google Scholar] [CrossRef]
- Dhanuthai, K.; Rojanawatsirivej, S.; Thosaporn, W.; Kintarak, S.; Subarnbhesaj, A.; Darling, M.; Kryshtalskyj, E.; Chiang, C.-P.; Shin, H.-I.; Choi, S.-Y.; et al. Oral Cancer: A Multicenter Study. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e23–e29. [Google Scholar] [CrossRef]
- Anwar, N.; Pervez, S.; Chundriger, Q.; Awan, S.; Moatter, T.; Ali, T.S. Oral Cancer: Clinicopathological Features and Associated Risk Factors in a High Risk Population Presenting to a Major Tertiary Care Center in Pakistan. PLoS ONE 2020, 15, e0236359. [Google Scholar] [CrossRef]
- Markopoulos, A.K. Current Aspects on Oral Squamous Cell Carcinoma. Open Dent. J. 2012, 6, 126–130. [Google Scholar] [CrossRef]
- Rivera, C. Essentials of Oral Cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884–11894. [Google Scholar]
- Pillai, J.; Chincholkar, T.; Dixit, R.; Pandey, M. A Systematic Review of Proteomic Biomarkers in Oral Squamous Cell Cancer. World J. Surg. Oncol. 2021, 19, 315. [Google Scholar] [CrossRef]
- Scott, S.E.; Grunfeld, E.A.; McGurk, M. The Idiosyncratic Relationship between Diagnostic Delay and Stage of Oral Squamous Cell Carcinoma. Oral Oncol. 2005, 41, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Gómez, I.; Seoane, J.; Varela-Centelles, P.; Diz, P.; Takkouche, B. Is Diagnostic Delay Related to Advanced-Stage Oral Cancer? A Meta-Analysis. Eur. J. Oral Sci. 2009, 117, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Yakob, M.; Fuentes, L.; Wang, M.B.; Abemayor, E.; Wong, D.T.W. Salivary Biomarkers for Detection of Oral Squamous Cell Carcinoma-Current State and Recent Advances. Curr. Oral Health Rep. 2014, 1, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, P.; Verma, J.K.; Singh, J.K. Validation of Salivary Markers, IL-1β, IL-8 and Lgals3bp for Detection of Oral Squamous Cell Carcinoma in an Indian Population. Sci. Rep. 2020, 10, 7365. [Google Scholar] [CrossRef] [PubMed]
- Nijakowski, K.; Surdacka, A. Salivary Biomarkers for Diagnosis of Inflammatory Bowel Diseases: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 7477. [Google Scholar] [CrossRef] [PubMed]
- Motamayel, F.A.; Davoodi, P.; Dalband, M.; Hendi, S.S. Saliva as a Mirror of the Body Health. Avicenna J. Dent. Res. 2018, 1, 41–55. [Google Scholar]
- Chiappin, S.; Antonelli, G.; Gatti, R.; De Palo, E.F. Saliva Specimen: A New Laboratory Tool for Diagnostic and Basic Investigation. Clin. Chim. Acta Int. J. Clin. Chem. 2007, 383, 30–40. [Google Scholar] [CrossRef]
- Spielmann, N.; Wong, D.T. Saliva: Diagnostics and Therapeutic Perspectives. Oral Dis. 2011, 17, 345–354. [Google Scholar] [CrossRef] [Green Version]
- Chaleckis, R.; Meister, I.; Zhang, P.; Wheelock, C.E. Challenges, Progress and Promises of Metabolite Annotation for LC-MS-Based Metabolomics. Curr. Opin. Biotechnol. 2019, 55, 44–50. [Google Scholar] [CrossRef]
- Hynne, H.; Sandås, E.M.; Elgstøen, K.B.P.; Rootwelt, H.; Utheim, T.P.; Galtung, H.K.; Jensen, J.L. Saliva Metabolomics in Dry Mouth Patients with Head and Neck Cancer or Sjögren’s Syndrome. Cells 2022, 11, 323. [Google Scholar] [CrossRef]
- Iwasaki, Y.; Sawada, T.; Hatayama, K.; Ohyagi, A.; Tsukuda, Y.; Namekawa, K.; Ito, R.; Saito, K.; Nakazawa, H. Separation Technique for the Determination of Highly Polar Metabolites in Biological Samples. Metabolites 2012, 2, 496–515. [Google Scholar] [CrossRef]
- Segers, K.; Declerck, S.; Mangelings, D.; Heyden, Y.V.; Eeckhaut, A.V. Analytical Techniques for Metabolomic Studies: A Review. Bioanalysis 2019, 11, 2297–2318. [Google Scholar] [CrossRef] [PubMed]
- Ussher, J.R.; Elmariah, S.; Gerszten, R.E.; Dyck, J.R.B. The Emerging Role of Metabolomics in the Diagnosis and Prognosis of Cardiovascular Disease. J. Am. Coll. Cardiol. 2016, 68, 2850–2870. [Google Scholar] [CrossRef] [PubMed]
- Hyvärinen, E.; Savolainen, M.; Mikkonen, J.J.W.; Kullaa, A.M. Salivary Metabolomics for Diagnosis and Monitoring Diseases: Challenges and Possibilities. Metabolites 2021, 11, 587. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.; Geddes, T.; Han, B.; Bahado-Singh, R.O.; Wilson, G.D.; Imam, K.; Maddens, M.; Graham, S.F. Diagnostic Biomarkers of Alzheimer’s Disease as Identified in Saliva Using 1H NMR-Based Metabolomics. J. Alzheimers Dis. 2017, 58, 355–359. [Google Scholar] [CrossRef]
- Meoni, G.; Lorini, S.; Monti, M.; Madia, F.; Corti, G.; Luchinat, C.; Zignego, A.L.; Tenori, L.; Gragnani, L. The Metabolic Fingerprints of HCV and HBV Infections Studied by Nuclear Magnetic Resonance Spectroscopy. Sci. Rep. 2019, 9, 4128. [Google Scholar] [CrossRef]
- Citterio, F.; Romano, F.; Meoni, G.; Iaderosa, G.; Grossi, S.; Sobrero, A.; Dego, F.; Corana, M.; Berta, G.N.; Tenori, L.; et al. Changes in the Salivary Metabolic Profile of Generalized Periodontitis Patients after Non-Surgical Periodontal Therapy: A Metabolomic Analysis Using Nuclear Magnetic Resonance Spectroscopy. J. Clin. Med. 2020, 9, 3977. [Google Scholar] [CrossRef]
- de Oliveira, L.R.P.; Martins, C.; Fidalgo, T.K.S.; Freitas-Fernandes, L.B.; de Oliveira Torres, R.; Soares, A.L.; Almeida, F.C.L.; Valente, A.P.; de Souza, I.P.R. Salivary Metabolite Fingerprint of Type 1 Diabetes in Young Children. J. Proteome Res. 2016, 15, 2491–2499. [Google Scholar] [CrossRef]
- Gonzalez-Covarrubias, V.; Martínez-Martínez, E.; del Bosque-Plata, L. The Potential of Metabolomics in Biomedical Applications. Metabolites 2022, 12, 194. [Google Scholar] [CrossRef]
- Rapado-González, Ó.; Majem, B.; Muinelo-Romay, L.; López-López, R.; Suarez-Cunqueiro, M.M. Cancer Salivary Biomarkers for Tumours Distant to the Oral Cavity. Int. J. Mol. Sci. 2016, 17, 1531. [Google Scholar] [CrossRef] [Green Version]
- Klupczyńska, A.; Dereziński, P.; Kokot, Z.J. Metabolomics in Medical Sciences-Trends, Challenges and Perspectives. Acta Pol. Pharm. 2015, 72, 629–641. [Google Scholar] [PubMed]
- Meleti, M.; Quartieri, E.; Antonelli, R.; Pezzi, M.E.; Ghezzi, B.; Viani, M.V.; Setti, G.; Casali, E.; Ferrari, E.; Ciociola, T.; et al. Metabolic Profiles of Whole, Parotid and Submandibular/Sublingual Saliva. Metabolites 2020, 10, 318. [Google Scholar] [CrossRef] [PubMed]
- de Sá Alves, M.; de Sá Rodrigues, N.; Bandeira, C.M.; Chagas, J.F.S.; Pascoal, M.B.N.; Nepomuceno, G.L.J.T.; da Silva Martinho, H.; Alves, M.G.O.; Mendes, M.A.; Dias, M.; et al. Identification of Possible Salivary Metabolic Biomarkers and Altered Metabolic Pathways in South American Patients Diagnosed with Oral Squamous Cell Carcinoma. Metabolites 2021, 11, 650. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, S.; Sugimoto, M.; Kitabatake, K.; Sugano, A.; Nakamura, M.; Kaneko, M.; Ota, S.; Hiwatari, K.; Enomoto, A.; Soga, T.; et al. Identification of Salivary Metabolomic Biomarkers for Oral Cancer Screening. Sci. Rep. 2016, 6, 31520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, S.; Wong, D.T.W.; Sugimoto, M.; Gleber-Netto, F.O.; Li, F.; Tu, M.; Zhang, Y.; Akin, D.; Iino, M. Identification of Salivary Metabolites for Oral Squamous Cell Carcinoma and Oral Epithelial Dysplasia Screening from Persistent Suspicious Oral Mucosal Lesions. Clin. Oral Investig. 2019, 23, 3557–3563. [Google Scholar] [CrossRef]
- Ishikawa, S.; Sugimoto, M.; Edamatsu, K.; Sugano, A.; Kitabatake, K.; Iino, M. Discrimination of Oral Squamous Cell Carcinoma from Oral Lichen Planus by Salivary Metabolomics. Oral Dis. 2020, 26, 35–42. [Google Scholar] [CrossRef]
- Ishikawa, S.; Sugimoto, M.; Konta, T.; Kitabatake, K.; Ueda, S.; Edamatsu, K.; Okuyama, N.; Yusa, K.; Iino, M. Salivary Metabolomics for Prognosis of Oral Squamous Cell Carcinoma. Front. Oncol. 2022, 11, 789248. [Google Scholar] [CrossRef]
- Lohavanichbutr, P.; Zhang, Y.; Wang, P.; Gu, H.; Nagana Gowda, G.A.; Djukovic, D.; Buas, M.F.; Raftery, D.; Chen, C. Salivary Metabolite Profiling Distinguishes Patients with Oral Cavity Squamous Cell Carcinoma from Normal Controls. PLoS ONE 2018, 13, e0204249. [Google Scholar] [CrossRef] [Green Version]
- Mikkonen, J.J.W.; Singh, S.P.; Akhi, R.; Salo, T.; Lappalainen, R.; González-Arriagada, W.A.; Ajudarte Lopes, M.; Kullaa, A.M.; Myllymaa, S. Potential Role of Nuclear Magnetic Resonance Spectroscopy to Identify Salivary Metabolite Alterations in Patients with Head and Neck Cancer. Oncol. Lett. 2018, 16, 6795–6800. [Google Scholar] [CrossRef] [Green Version]
- Ohshima, M.; Sugahara, K.; Kasahara, K.; Katakura, A. Metabolomic Analysis of the Saliva of Japanese Patients with Oral Squamous Cell Carcinoma. Oncol. Rep. 2017, 37, 2727–2734. [Google Scholar] [CrossRef] [Green Version]
- Rai, B.; Kharb, S.; Jain, R.; Anand, S.C. Salivary Vitamins E and C in Oral Cancer. Redox Rep. 2007, 12, 163–164. [Google Scholar] [CrossRef] [PubMed]
- Shigeyama, H.; Wang, T.; Ichinose, M.; Ansai, T.; Lee, S.-W. Identification of Volatile Metabolites in Human Saliva from Patients with Oral Squamous Cell Carcinoma via Zeolite-Based Thin-Film Microextraction Coupled with GC-MS. J. Chromatogr. B Analyt. Technol. Biomed. Life. Sci. 2019, 1104, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Yang, X.; Narayanan, R.; Shankar, V.; Ethiraj, S.; Wang, X.; Duan, N.; Ni, Y.-H.; Hu, Q.; Zare, R.N. Oral Squamous Cell Carcinoma Diagnosed from Saliva Metabolic Profiling. Proc. Natl. Acad. Sci. USA 2020, 117, 16167–16173. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, G.; Ramani, P.; Patankar, S.; Vijayaraghavan, R. Evaluation of Salivary Metabolomics in Oral Leukoplakia and Oral Squamous Cell Carcinoma. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2019, 48, 299–306. [Google Scholar] [CrossRef]
- Sugimoto, M.; Wong, D.T.; Hirayama, A.; Soga, T.; Tomita, M. Capillary Electrophoresis Mass Spectrometry-Based Saliva Metabolomics Identified Oral, Breast and Pancreatic Cancer-Specific Profiles. Metab. Off. J. Metab. Soc. 2010, 6, 78–95. [Google Scholar] [CrossRef] [Green Version]
- Supawat, B.; Aye, K.T.; Ritpanja, J.; Nueangwong, W.; Kothan, S.; Pan, J.; Tungjai, M. Differences in Spectroscopic Properties of Saliva Taken From Normal Subjects and Oral Cancer Patients: Comparison Studies. J. Fluoresc. 2021, 31, 747–754. [Google Scholar] [CrossRef]
- Taware, R.; Taunk, K.; Pereira, J.A.M.; Shirolkar, A.; Soneji, D.; Câmara, J.S.; Nagarajaram, H.A.; Rapole, S. Volatilomic Insight of Head and Neck Cancer via the Effects Observed on Saliva Metabolites. Sci. Rep. 2018, 8, 17725. [Google Scholar] [CrossRef]
- Wang, Q.; Gao, P.; Cheng, F.; Wang, X.; Duan, Y. Measurement of Salivary Metabolite Biomarkers for Early Monitoring of Oral Cancer with Ultra Performance Liquid Chromatography-Mass Spectrometry. Talanta 2014, 119, 299–305. [Google Scholar] [CrossRef]
- Wang, Q.; Gao, P.; Wang, X.; Duan, Y. Investigation and Identification of Potential Biomarkers in Human Saliva for the Early Diagnosis of Oral Squamous Cell Carcinoma. Clin. Chim. Acta Int. J. Clin. Chem. 2014, 427, 79–85. [Google Scholar] [CrossRef]
- Wang, Q.; Gao, P.; Wang, X.; Duan, Y. The Early Diagnosis and Monitoring of Squamous Cell Carcinoma via Saliva Metabolomics. Sci. Rep. 2014, 4, 6802. [Google Scholar] [CrossRef]
- Wei, J.; Xie, G.; Zhou, Z.; Shi, P.; Qiu, Y.; Zheng, X.; Chen, T.; Su, M.; Zhao, A.; Jia, W. Salivary Metabolite Signatures of Oral Cancer and Leukoplakia. Int. J. Cancer 2011, 129, 2207–2217. [Google Scholar] [CrossRef] [PubMed]
- OCEBM. Levels of Evidence. Available online: https://www.cebm.net/2016/05/ocebm-levels-of-evidence/ (accessed on 22 August 2020).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Study Quality Assessment Tools | NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 22 August 2020).



{kind=link}
{kind=link}
| Author, Year | Setting | Study Group (F/M); Age | Control Group (F/M); Age | Diagnosis | Inclusion Criteria | Exclusion Criteria | Smoking Status | TNM Stages |
|---|---|---|---|---|---|---|---|---|
| de Sá Alves et al., 2021 [33] | Brazil | 27 (8/19); 57 ± 13.87 (28–88) | 41 (20/21); 57.34 ± 11.66 (31–86) | OSCC | OSCC: patients over 18 years of age concomitant with the diagnosis of OSCC; Ctrl: patients over 18 years of age, who wanted to participate in the research | OSCC: patients diagnosed with cancer anywhere on the body that had already undergone surgery, radiotherapy or chemotherapy; Ctrl: patients with some type of cancer during their lifetime | OSCC: 20 smokers; Ctrl: 8 smokers, 13 ex-smokers | I-15%, II-15%, III-22%, IV-48% |
| Ishikawa et al., 2016 [34] | Japan | 24 (10/14); 72 (23–94) | 44 (28/16); 68 (21–90) | OSCC (n = 21), malignant melanoma (n = 2), unknown (n = 1) | NR | OC: prior chemotherapy or radiotherapy; Ctrl: history of prior malignancy or autoimmune disorders | OC: 14 smokers; Ctrl: 9 smokers | I-21%, II-25%, III-33%, IV-21% |
| Ishikawa et al., 2019 [35] | Japan | OSCC: 6 (0/6); 63.5 (49–83), OED: 10 (4/6); 69.0 (57–81), PSOML: 32 (11/21); 62.5 (21–86) | - | OSCC, OED, PSOML | patients confirmed pathologically by open biopsy | prior chemotherapy or radiotherapy | NR | NR |
| Ishikawa et al., 2020 [36] | Japan | OSCC: 34 (14/20); 70.5 (29–87), OLP: 26 (21/5); 67.5 (34–98) | - | OSCC, OLP | OSCC patients confirmed pathologically by incisional open biopsy | prior chemotherapy or radiotherapy | NR | I-41.2%, II-26.5%, III-5.9%, IV-26.5% |
| Ishikawa et al., 2022 [37] | Japan | training group: 35 (15/20); 65.0 (26–89), validation group: 37 (19/18); 69 (23–94) | - | OSCC | prior curative treatment, such as radical surgery or chemoradiotherapy, OSCC patients confirmed pathologically by incisional open biopsy | prior non-curative treatment, such as palliative treatment or symptomatic treatment | training group: 2 smokers; validation group: 6 smokers | training group: 0 (CIS)-5.7%, I-45.7%, II-17.1%, III-8.6%, IV-22.9%; validation group: 0 (CIS)-2.7%, I-21.6%, II-21.6%, III-27.0%, IV-27.0% |
| Lohavanichbutr et al., 2018 [38] | USA | First set: 79 (23/56); <50—14 (17.7%), 50–59—24 (30.4%), 60–69—22 (27.8%), >70—19 (24.1%); Second set: 80 (17/63); <50—16 (20%), 50–59—37 (46.3%), 60–69—17 (21.3%), >70—10 (12.5%) | First set: 20 (8/12); <50—13 (65.0%), 50–59—4 (20.0%), 60–69—3 (15.0%), >70—0; Second set: 20 (5/15); <50—13 (65.0%), 50–59—3 (15.0%), 60–69—4 (20.0%), >70—0 | OSCC | Ctrl: patients without OSCC who had oral surgery such as tonsillectomy at the same institutions where the OSCC patients were treated during the same period | NR | First set: 37 current smokers, 42 never/former smokers, Ctrl: 5 current smokers, 9 never/former smokers, 6 unknown; Second set: 28 current smokers, 51 never/former smokers, 1 unknown, Ctrl: 5 current smokers, 12 never/former smokers, 3 unknown | First set: T1/T2-50.6%, T3/T4-49.4%; Second set: T1/T2-68.0%, T3/T4-32.0% |
| Mikkonen et al., 2018 [39] | Brazil | 8 (0/8); 61.7 ± 9.6 (52–76) | 30; 54.4 ± 9.0 (42–74) | HNSCC: larynx (n = 5), oral cavity (n = 3) | NR | NR | HNSCC: 7 smokers; Ctrl: non-smokers | I-12.5%, II-0%, III-37.5%, IV-50% |
| Ohshima et al., 2017 [40] | Japan | 22 (9/13); 68 ± 13 | 21 (13/8); 56 ± 8 | OSCC | NR | OSCC: prior chemotherapy or radiotherapy, history of prior malignancy; Ctrl: history of mucosal diseases in the oral cavity, immunodeficiency, autoimmune disorders, hepatitis or HIV infection | NR | I-31.8%, II-31.8%, III-4.6%, IV-31.8% |
| Rai et al., 2007 [41] | India | 50 (25/25); 17–50 | 24 (11/13); 18–50 | OC | NR | NR | NR | III-100% |
| Shigeyama et al., 2019 [42] | Japan | 12 (7/5); F: 60 ± 16.8, M: 64 ± 19 | 8 (1/7); F: 27, M:28.3 ± 10.3 | OSCC | histologically diagnosed OSCC patients | OSCC: prior chemotherapy, radiotherapy, surgery or alternative remedies before sample collection; Ctrl: history of malignancy, immunodeficiency, underlying diseases | OSCC: 2 smokers, 1 ex-smoker; Ctrl: 1 smoker | I-41.7%, II-50.0%, III-0%, IV-8.33% |
| Song et al., 2020 [43] | China | discovery group: OSCC: 65 (30/35); 35–65, PML: 64 (30/34); 35–65, validation group: OSCC: 60 (30/30); 35–65, PML: 60 (30/30); 35–65 | discovery group: 64 (30/34); 30–60, validation group: 60 (30/30); 30–60 | OSCC, PML | NR | prior therapy | NR | discovery group: I-23.1%, II-32.3%, III-18.4%, IV-26.2%; validation group: I-23.3%, II-31.7%, III-18.3%, IV-26.7% |
| Sridharan et al., 2019 [44] | India | OSCC: 22 (4/18); 43 (39.5–54), OLK: 21 (2/19); 48 (38–54.5) | 21 (7/14); 32 (27.5–45.5) | OSCC, OLK | OSCC: clinically and histopathologically confirmed OSCC; OLK: clinically diagnosed OLK; Ctrl: normal individuals without any oral lesions, tobacco habits and systemic illnesses | history of systemic illness and medications; history of therapy for OLK and OSCC and with recurrent oral lesions | OSCC: 2 smokers; OLK: 10 smokers | NR |
| Sugimoto et al., 2010 [45] | USA | OC: 69 (23/41/5 missing); 34–87 (59.5) (5 missing) | 87 (27/42/18 missing); 20–75 (43) (2 missing) | OC | diagnosed with primary disease without metastasis | prior chemotherapy, radiotherapy, surgery or alternative therapy, history of prior malignancy, immunodeficiency, autoimmune disorders, hepatitis or HIV infection | NR | NR |
| Supawat et al., 2021 [46] | Thailand | 15; 57.3 ± 8.9 (35–73) | 10; 50.5 ± 10.7 (21–60) | OC | NR | Ctrl: history of cancer disease | OC: NR; Ctrl: non-smokers | NR |
| Taware et al., 2018 [47] | India | 32 (13/19); 60 (36–82) | 27 (12/15); 55 (33–75) | OC | minimum 18 years old patient with histopathological confirmation of malignant lesion | OC: anticancer therapeutic intervention; Ctrl: hypertension, diabetes, any medication during last 3 months | OC: 8 smokers; Ctrl: 8 smokers | NR |
| Wang et al., 2014 [48] | China | 30 (5/25); 62 | 60 (25/35) | OSCC | clinical and histopathologic diagnosis | history of receiving medication, prior chemotherapy and radiotherapy | NR | I-23.3%, II-20%, III-6.7%, IV-50% |
| Wang et al., 2014 [49] | China | 30 (5/25); 55 (29–72) | 30 (5/25); 47 (25–69) | OSCC | clinical and histopathologic diagnosis | history of receiving medication and surgical operation, prior chemotherapy and radiotherapy | NR | I-13.3%, II-30%, III-10%, IV-46.7% |
| Wang et al., 2014 [50] | China | 30 (5/25); 55 (29–72) | 30 (5/25); 47 (25–69) | OSCC | clinical and histopathologic diagnosis | history of receiving medication and surgical operation, prior chemotherapy and radiotherapy | NR | I-13.3%, II-30%, III-10%, IV-46.7% |
| Wei et al., 2011 [51] | China | OSCC: 37 (11/26); 56 ± 11 (34–77), OLK: 32 (19/13); 60 ± 13 (34–80) | 34 (21/13); 43 ± 14 (21–73) | OSCC, OLK | clinical and histopathologic diagnosis | history of receiving medication and treatment with topical or systemical steroids | OSCC: 10 smokers, OLK: 9 smokers, Ctrl: 6 smokers | I-24.3%, II-32.4%, III-16.2%, IV-27.1% |
| Author, Year | Type of Saliva and Method of Collection | Centrifugation and Storing | Method of Analysis | Potential Discriminant Metabolites in Saliva |
|---|---|---|---|---|
| de Sá Alves et al., 2021 [33] | unstimulated whole saliva 3 mL collected in the plastic tubes, which were then hermetically closed, immersed in ice and transported within 1 h to the storage location | stored at −80 °C until analysis | GC-MS | 22 metabolites: up: malic acid, maltose, methionine, inosine, protocatechuic acid, dihydroxyacetone phosphate, galacturonic acid, uracil, isocitric acid, ribose 5-phosphate, o-phospho-serine, indole-3-acetic acid, 2-ketoglutaric acid, pantothenic acid and spermidine; down: lactose, catechol, 2-ketoadipic acid, urea, leucine, margaric acid, palmitic acid and maleic acid |
| Ishikawa et al., 2016 [34] | unstimulated whole saliva 400 μL collected for 5–10 min in a 50 mL Falcon tube on ice; between 8 a.m. and 12 noon | immediately stored at −80 °C | CE-TOF-MS | among 43 significantly elevated metabolites, 17 metabolites also in tissue: up: 3-phosphoglyceric acid, pipecolate, spermidine, methionine, S-adenosylmethionine, 2-aminobenzamide, tryptophan, valine, hypoxanthine, glycylglycine, trimethylamine N-oxide, guanine, guanosine, taurine, choline, cadaverine, threonine |
| Ishikawa et al., 2019 [35] | unstimulated whole saliva 4–5 mL collected for 5–15 min into 50 mL Falcon tubes in a paper cup filled with crushed ice | immediately stored at −80 °C | CE-TOF-MS | 6 metabolites: down: ornithine, carnitine, arginine, o-hydroxybenzoate, N-acetylglucosamine-1-phosphate and ribose 5-phosphate |
| Ishikawa et al., 2020 [36] | unstimulated whole saliva 3 mL collected for 5–10 min into 50 mL Falcon tubes in a paper cup filled with crushed ice | immediately stored at −80 °C | CE-TOF-MS | 14 metabolites: up: trimethylamine N-oxide, putrescine, creatinine, 5-aminovalerate, pipecolate, N-acetylputrescine, gamma-butyrobetaine, indole-3-acetate, N1-acetylspermine, 2’-deoxyinsine, ethanolamine phosphate and N-acetylglucosamine, down: N-acetylhistidine and o-acetylcarnitine |
| Ishikawa et al., 2022 [37] | unstimulated whole saliva 3 mL collected for 5 min into 50 mL Falcon tubes in a paper cup filled with crushed ice | stored at −80 °C | CE-TOF-MS | for predicting overall survival: in the training group identified proline, carnitine, 5-hydroxylysine, 3-methylhistidine, adenosine, inosine and N-acetylglucosamine, in the validation group only 3-methylhistidine (HR = 1.711) |
| Lohavanichbutr et al., 2018 [38] | unstimulated whole saliva into 50 mL sterile conical centrifuge tube and transferred on ice to the laboratory within two hours | centrifuged at 1300× g at 4 °C for 10 min; stored at −80 °C | NMR and LC-MS | 4 metabolites: citrulline and ornithine (only for T1/T2), proline and glycine |
| Mikkonen et al., 2018 [39] | unstimulated whole saliva sample collected into a sterile glass cup for 5 min; between 9 and 11 a.m. | centrifuged at 14,000 rpm for 6 min, stored at −20 °C | NMR spectroscopy | 3 metabolites: up: 1,2 propanediol and fucose, down: proline |
| Ohshima et al., 2017 [40] | unstimulated whole saliva 5 mL collected for 5–10 min into 50 mL tubes, which were placed in a Styrofoam cup filled with crushed; at 8 a.m. | centrifuged at 2600× g for 15 min at 4 °C, and spun for a further 20 min in case of incomplete separation | CE-TOF-MS | 25 metabolites: up: choline, p-hydroxyphenylacetic acid and 2-hydroxy-4-methylvaleric acid (p-value < 0.001), valine, 3-phenyllactic acid, leucine, hexanoic acid, octanoic acid, terephthalic acid, γ-butyrobetaine and 3-(4-hydroxyphenyl)propionic acid (p-value < 0.01), isoleucine, tryptophan, 3-phenylpropionic acid, 2-hydroxyvaleric acid, butyric acid, cadaverine, 2-oxoisovaleric acid, N6,N6,N6-trimethyllysine, taurine, glycolic acid, 3-hydroxybutyric acid, heptanoic acid and alanine (p-value < 0.05); down: urea (p-value < 0.05) |
| Rai et al., 2007 [41] | unstimulated whole saliva collected on ice | centrifuged and frozen at −20 °C until analysis | HPLC | vitamins E and C (p-value < 0.001) |
| Shigeyama et al., 2019 [42] | unstimulated whole saliva 2 mL, collected in a 10 mL glass bottle over a period of 5–10 min; for at least a period of 5 days between 7 and 10 a.m. | immediately stored at −80 °C | thin-film microextraction based on a ZSM-5/PDMS hybrid film coupled with GC-MS | among 27 volatile metabolites, 12 top metabolites: up: 3-heptanone, 1,3-butanediol, 1,2-pentanediol and 1-hexadecanol, down: ethanol, 2-pentanone, phenol, hexadecanoic acid, undecane, 1-octanol, butyrolactone and benzyl alcohol |
| Song et al., 2020 [43] | unstimulated whole saliva 500 μL, collected into an EP tube | centrifuged at 5000 rpm for 3 min, frozen at −80 °C until analysis | CPSI-MS | among 116 metabolites, top 10 metabolites: up: putrescine, cadaverine, thymidine, adenosine and 5-aminopentoate, down: hippuric acid, phosphocholine, glucose, serine and adrenic acid |
| Sridharan et al., 2019 [44] | unstimulated whole saliva was collected under aseptic conditions by drooling method in a collecting jar | immediately centrifuged and stored at −80 °C before analysis | UPLC-QTOF-MS | 37 upregulated and 11 downregulated metabolites |
| Sugimoto et al., 2010 [45] | unstimulated whole saliva 5 mL for 5–10 min, spitted into 50 mL Falcon tubes, placed in a Styrofoam cup filled with crushed ice | centrifuged at 2600× g for 15 min at 4 °C and spun for 20 min in case of incomplete separation, transferred to two fresh tubes and frozen within 30 min | CE-TOF-MS | 28 metabolites: up: pyrroline hydroxycarboxylic acid, leucine plus isoleucine, choline, tryptophan, valine, threonine, histidine, pipecolic acid, glutamic acid, carnitine, alanine, piperideine, taurine, C4H9N and C8H9N (p-value < 0.001); piperidine, alpha-aminobutyric acid, phenylalanine and C6H6N2O2 (p-value < 0.01); betaine, serine, tyrosine, glutamine, beta-alanine, cadaverine and C5H14N5, down: C4H5N2O11P (p-value < 0.05) |
| Supawat et al., 2021 [46] | unstimulated whole saliva collected on a sterile container kept in an ice pack | immediately stored at −20 °C until analysis | NMR spectroscopy | 13 metabolites: up: trimethylamine N-oxide, taurine, glycine and aspartate, down: propionate, isobutyrate, fucose, cisaconitate, choline, trimethylamine N-oxide, methanol, acetoacetate and glycine |
| Taware et al., 2018 [47] | unstimulated whole saliva 2 mL collected in 10 mL sterilised glass vial with screw cap and immediately placed on ice; between 9 a.m. and 12 at noon | transported to the laboratory within 1 h and stored at −80 °C until analysis | HS-SPME-GC-MS | among 27 volatile metabolites, 15 top metabolites: 1,4-dichlorobenzene, 1,2-decanediol, 2,5-Bis1,1-dimethylethylphenol, propanoic acid (ethyl ester), E-3-decen-2-ol, acetic acid, propanoic acid, ethyl acetate, 2,4-dimethyl-1-heptene, 1-chloro-2-propanol, 1-chloro-2-butanol, 2-propenoic acid, 2,3,3-trimethylpentane, ethanol, 1,2,3,4-tetrachlorobutane |
| Wang et al., 2014 [48] | unstimulated whole saliva 3 mL kept on ice | centrifuged at 12,000 rpm for 20 min at 4 °C and frozen at −40 °C until analysis | UPLC-ESI-MS | 2 metabolites: L-phenylalanine and L-leucine |
| Wang et al., 2014 [49] | unstimulated whole saliva 2 mL; between 9 and 11 a.m. | centrifuged at 12,000 rpm for 20 min at 4 °C and frozen at −40 °C until analysis | HILIC-UPLC-MS | 4 metabolites: choline, betaine, pipecolinic acid and L-carnitine |
| Wang et al., 2014 [50] | unstimulated whole saliva 3 mL; between 9 and 11 a.m. | centrifuged at 12,000 rpm for 20 min at 4 °C and frozen at −40 °C until analysis | RP-UPLC-MS, HILIC-UPLC-MS | 14 metabolites: up: lactic acid, hydroxyphenyllactic acid, N-nonanoylglycine, 5-hydroxymethyluracil, succinic acid, ornithine, hexanoylcarnitine and propionylcholine; down: carnitine, 4-hydroxy-L-glutamic acid, acetylphenylalanine, sphinganine, phytosphingosine and S-carboxymethyl-L-cysteine |
| Wei et al., 2011 [51] | unstimulated whole saliva; between 9 and 10 a.m. | centrifuged at 3500× g for 20 min at 4 °C and immediately stored at −80 °C until analysis | UPLC-QTOF-MS | among 41 metabolites, 5 top: gamma-aminobutyric acid, phenylalanine, valine, n-eicosanoic acid and lactic acid |
| Study | Most Discriminant Metabolites | AUC | −95% CI | +95% CI | Sensitivity [%] | Specificity [%] |
|---|---|---|---|---|---|---|
| de Sá Alves et al., 2021 [33] | Malic acid | 0.981 | - | - | - | - |
| Lactose | 0.964 | - | - | - | - | |
| Catechol | 0.947 | - | - | - | - | |
| 2-Ketoadipic acid | 0.941 | - | - | - | - | |
| Maltose | 0.934 | - | - | - | - | |
| Methionine | 0.925 | - | - | - | - | |
| Urea | 0.925 | - | - | - | - | |
| Leucine | 0.923 | - | - | - | - | |
| Inosine | 0.922 | - | - | - | - | |
| Protocatechuic acid | 0.911 | - | - | - | - | |
| Ishikawa et al., 2016 [34] | 3-Phosphoglyceric acid | 0.767 | 0.635 | 0.899 | - | - |
| Pipecolate | 0.755 | 0.637 | 0.873 | - | - | |
| Spermidine | 0.751 | 0.626 | 0.876 | - | - | |
| Methionine | 0.744 | 0.628 | 0.861 | - | - | |
| S-adenosylmethionine | 0.743 | 0.613 | 0.874 | - | - | |
| S-adenosylmethionine + pipecolate | 0.827 | 0.726 | 0.928 | - | - | |
| Ishikawa et al., 2019 [35] | Ribose 5-phosphate ** | 0.714 | - | - | - | - |
| Carnitine ** | 0.704 | - | - | - | - | |
| Arginine ** | 0.689 | - | - | - | - | |
| N-Acetylglucosamine1-phosphate ** | 0.682 | - | - | - | - | |
| Ornithine ** | 0.676 | - | - | - | - | |
| Ornithine + o-hydroxybenzoate + ribose 5-phosphate ** | 0.871 | 0.760 | 0.982 | - | - | |
| Ishikawa et al., 2020 [36] | 5-Aminovalerate * | 0.786 | - | - | - | - |
| Indole-3-acetate * | 0.786 | - | - | - | - | |
| Creatinine * | 0.766 | - | - | - | - | |
| Putrescine * | 0.712 | - | - | - | - | |
| N-Acetylglucosamine * | 0.704 | - | - | - | - | |
| Indole-3-acetate + ethanolamine phosphate * | 0.856 | 0.762 | 0.950 | - | - | |
| Mikkonen et al., 2018 [39] | Fucose + glycine + methanol + proline | - | - | - | 87.5 | 93.3 |
| Shigeyama et al., 2019 [42] | 2-Pentanone + undecane + 1,3-butanediol + hexadecanoic acid | - | - | - | 95.8 | 94.0 |
| Song et al., 2020 [43] | 62 metabolites | 0.992 | 0.978 | 1.000 | 90.0 | 98.3 |
| Sugimoto et al., 2010 [45] | Alanine + choline + “leucine + isoleucine” + glutamic acid + C8H9N + phenylalanine + alpha-aminobutyric acid + serine | 0.865 | - | - | - | - |
| Taware et al., 2018 [47] | 1,4-Dichlorobenzene | 0.998 | - | - | 100.0 | 100.0 |
| 1,2-Decanediol | 0.939 | - | - | 100.0 | 80.0 | |
| 2,5-Bis1,1-dimethylethylphenol | 0.913 | - | - | 90.0 | 80.0 | |
| E-3-Decen-2-ol | 0.889 | - | - | 80.0 | 80.0 | |
| Wang et al., 2014 [48] | L-Phenylalanine ^ | 0.695 | 0.560 | 0.830 | 84.6 | 61.7 |
| L-Leucine ^ | 0.863 | 0.747 | 0.979 | 84.6 | 81.7 | |
| L-Phenylalanine + L-leucine ^ | 0.871 | 0.767 | 0.974 | 92.3 | 81.7 | |
| L-Phenylalanine ^^ | 0.767 | 0.637 | 0.896 | 47.1 | 95.0 | |
| L-Leucine ^^ | 0.852 | 0.748 | 0.956 | 82.4 | 80.0 | |
| L-Phenylalanine + L-leucine^^ | 0.899 | 0.827 | 0.971 | 94.1 | 75.0 | |
| Wang et al., 2014 [49] | Choline ^ | 0.926 | 0.820 | 0.997 | 84.6 | 90.0 |
| Betaine ^ | 0.759 | 0.587 | 0.931 | 46.2 | 96.7 | |
| Pipecolinic acid ^ | 0.994 | 0.981 | 1.000 | 92.3 | 96.7 | |
| L-Carnitine ^ | 0.708 | 0.532 | 0.884 | 73.3 | 61.5 | |
| Choline + betaine + pipecolinic acid + L-carnitine ^ | 0.997 | 0.989 | 1.000 | 100.0 | 96.7 | |
| Choline ^^ | 0.898 | 0.781 | 1.000 | 82.4 | 96.7 | |
| Betaine ^^ | 0.665 | 0.501 | 0.828 | 47.1 | 80.0 | |
| Pipecolinic acid ^^ | 0.914 | 0.798 | 1.000 | 88.2 | 96.7 | |
| L-Carnitine ^^ | 0.731 | 0.563 | 0.900 | 96.7 | 52.9 | |
| Choline + betaine + pipecolinic acid + L-carnitine ^^ | 0.906 | 0.804 | 1.000 | 88.2 | 90.0 | |
| Wang et al., 2014 [50] | Propionylcholine ^ | 0.946 | 0.882 | 1.000 | 76.9 | 96.7 |
| S-carboxymethyl-L-cysteine ^ | 0.913 | 0.822 | 1.000 | 84.6 | 93.3 | |
| Phytosphingosine ^ | 0.910 | 0.816 | 1.000 | 92.3 | 83.3 | |
| Acetylphenylalanine ^ | 0.838 | 0.705 | 0.972 | 92.3 | 76.7 | |
| Sphinganine ^ | 0.818 | 0.660 | 0.976 | 84.6 | 83.3 | |
| Propionylcholine + acetylphenylalanine + sphinganine + phytosphingosine + S-carboxymethyl-L-cysteine ^ | 0.997 | - | - | 100.0 | 96.7 | |
| Propionylcholine + acetylphenylalanine + sphinganine + phytosphingosine + S-carboxymethyl-L-cysteine ^^ | 0.971 | - | - | 86.7 | 94.1 | |
| S-carboxymethyl-L-cysteine ^^ | 0.888 | 0.784 | 0.992 | 88.2 | 90.0 | |
| Phytosphingosine ^^ | 0.875 | 0.776 | 0.973 | 76.5 | 83.3 | |
| Lactic acid ^^ | 0.837 | 0.723 | 0.951 | 100.0 | 73.3 | |
| Propionylcholine ^^ | 0.788 | 0.655 | 0.921 | 64.7 | 80.0 | |
| Succinic acid ^^ | 0.786 | 0.658 | 0.914 | 88.2 | 66.7 | |
| Wei et al., 2011 [51] | Lactic acid | 0.800 | 0.700 | 0.904 | 73.0 | 70.6 |
| Gamma-Aminobutyric acid | 0.560 | 0.423 | 0.698 | 61.8 | 62.2 | |
| Valine | 0.810 | 0.706 | 0.911 | 82.4 | 75.7 | |
| Phenylalanine | 0.640 | 0.508 | 0.765 | 52.9 | 56.8 | |
| n-Eicosadienoic acid | 0.670 | 0.549 | 0.800 | 51.4 | 73.5 | |
| Lactic acid + valine | 0.890 | 0.813 | 0.972 | 86.5 | 82.4 | |
| Lactic acid *** | 0.820 | 0.724 | 0.918 | 73.0 | 75.0 | |
| gamma-Aminobutyric acid *** | 0.750 | 0.636 | 0.869 | 75.0 | 70.3 | |
| Valine *** | 0.830 | 0.736 | 0.925 | 78.1 | 75.8 | |
| Phenylalanine *** | 0.780 | 0.662 | 0.894 | 71.9 | 75.7 | |
| n-Eicosadienoic acid *** | 0.770 | 0.658 | 0.886 | 70.3 | 87.5 | |
| Lactic acid + valine + phenylalanine *** | 0.970 | 0.932 | 1.000 | 94.6 | 84.4 |
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | patients with oral cancer—aged from 0 to 99 years, both sexes | patients with other neoplasms |
| Intervention | not applicable | |
| Comparison | not applicable | |
| Outcomes | salivary metabolites as markers | other salivary components as markers |
| Study design | case-control, cohort and cross-sectional studies | literature reviews, case reports, expert opinion, letters to the editor, conference reports |
| published after 2000 | not published in English |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nijakowski, K.; Gruszczyński, D.; Kopała, D.; Surdacka, A. Salivary Metabolomics for Oral Squamous Cell Carcinoma Diagnosis: A Systematic Review. Metabolites 2022, 12, 294. https://doi.org/10.3390/metabo12040294
Nijakowski K, Gruszczyński D, Kopała D, Surdacka A. Salivary Metabolomics for Oral Squamous Cell Carcinoma Diagnosis: A Systematic Review. Metabolites. 2022; 12(4):294. https://doi.org/10.3390/metabo12040294
Chicago/Turabian StyleNijakowski, Kacper, Dawid Gruszczyński, Dariusz Kopała, and Anna Surdacka. 2022. "Salivary Metabolomics for Oral Squamous Cell Carcinoma Diagnosis: A Systematic Review" Metabolites 12, no. 4: 294. https://doi.org/10.3390/metabo12040294
APA StyleNijakowski, K., Gruszczyński, D., Kopała, D., & Surdacka, A. (2022). Salivary Metabolomics for Oral Squamous Cell Carcinoma Diagnosis: A Systematic Review. Metabolites, 12(4), 294. https://doi.org/10.3390/metabo12040294