Fibrinogen Fucosylation as a Prognostic Marker of End-Stage Renal Disease in Patients on Peritoneal Dialysis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Experimental Section
2.1. Blood Samples
2.2. Fibrinogen Isolation
2.3. Lectin-Based Protein Microarray
2.4. Lectin Blotting
2.5. Statistics
3. Results
3.1. Samples
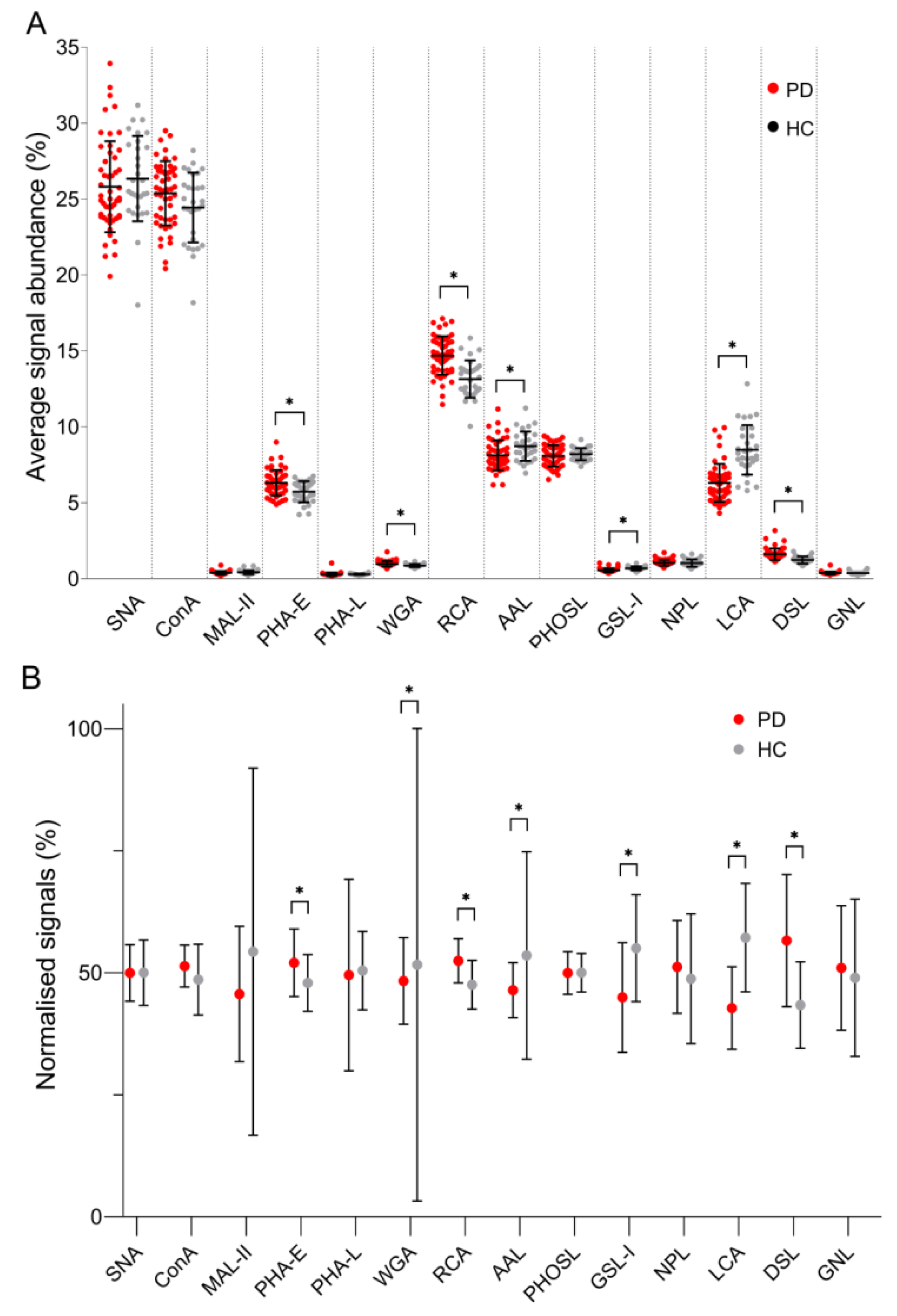
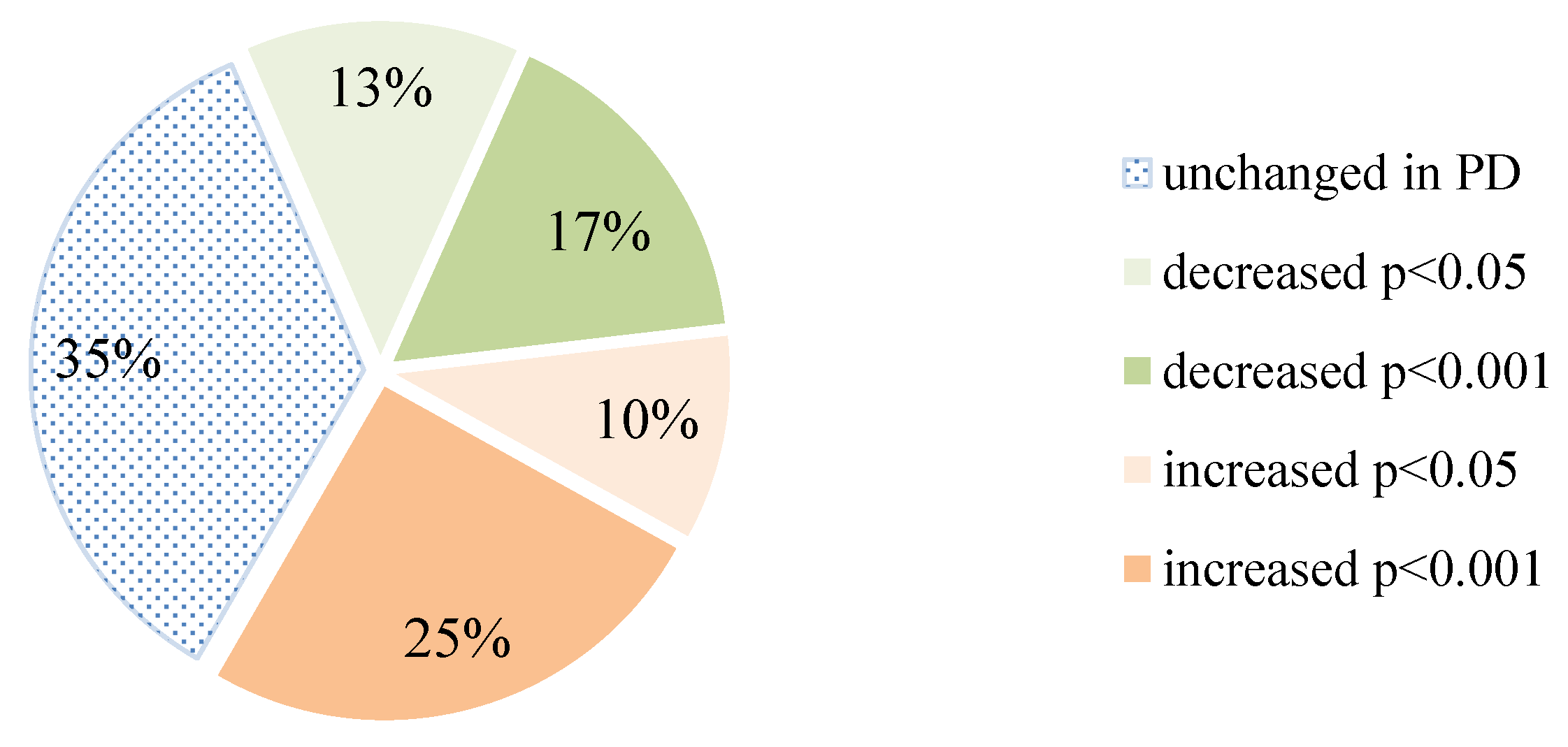
3.2. Lectin-Based Microarray
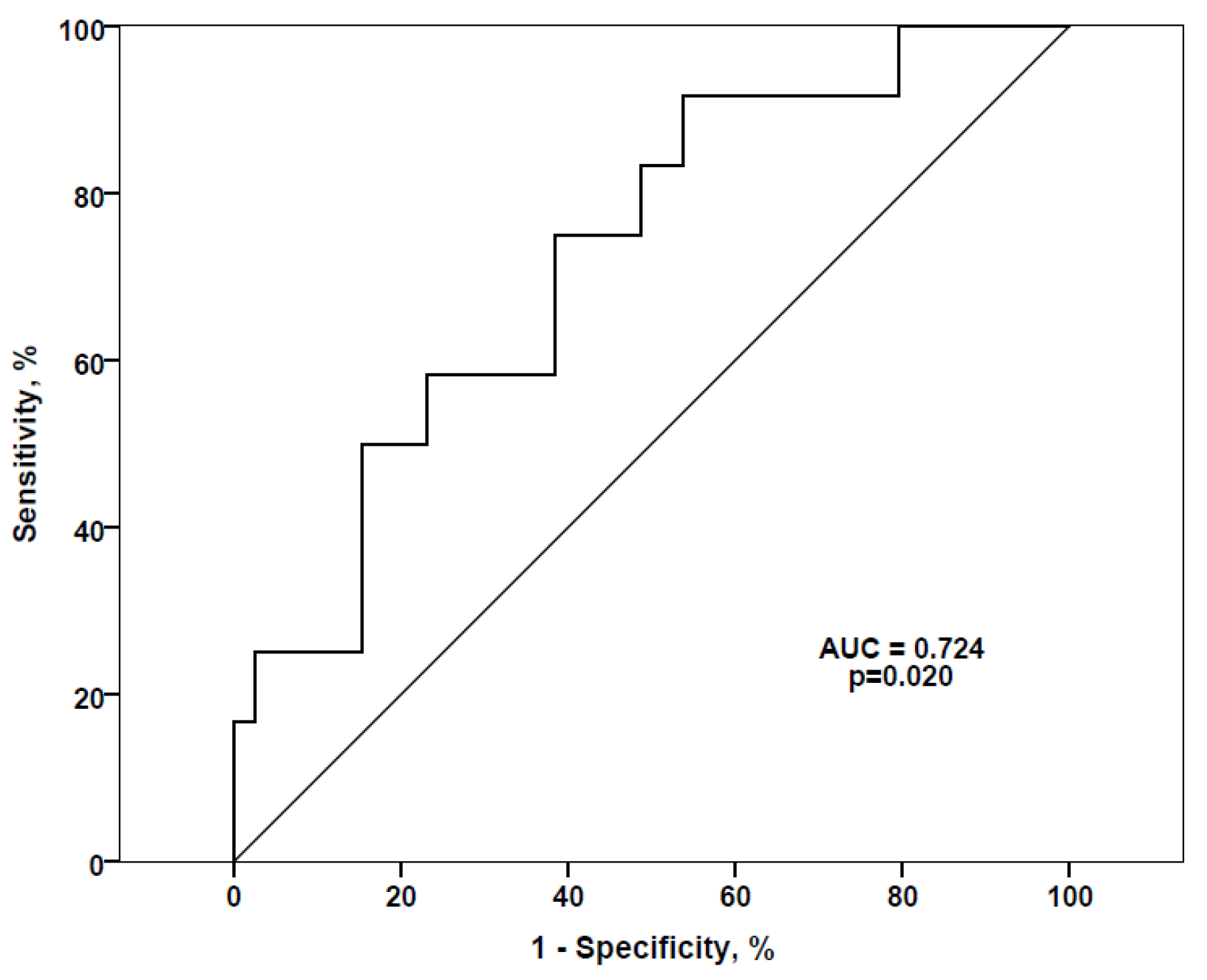
Association between Lectin-Based Microarray Results and Clinical Data
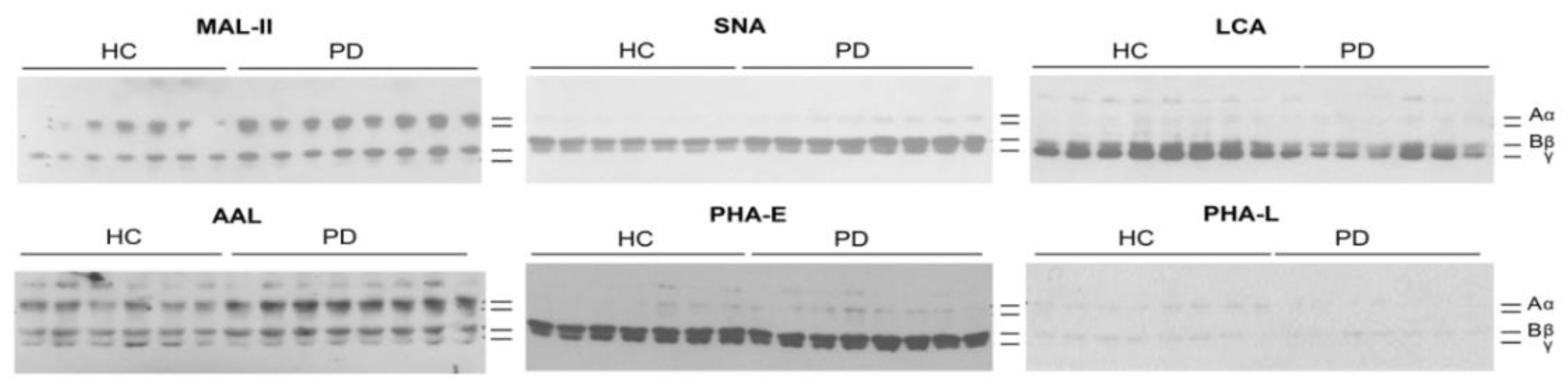
3.3. Lectin Blotting
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Reily, C.; Stewart, T.J.; Renfrow, M.B.; Novak, J. Glycosylation in health and disease. Nat. Rev. Nephrol. 2019, 15, 346–366. [Google Scholar] [CrossRef]
- Hendrickson, O.D.; Zherdev, A.V. Analytical application of lectins. Crit. Rev. Anal. Chem. 2018, 48, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Kooman, J.P.; van der Sande, F.M. Body fluids in end-stage renal disease: Statics and dynamics. Blood Purif. 2019, 47, 223–229. [Google Scholar] [CrossRef]
- Ferrantelli, E.; Farhat, K.; Ederveen, A.L.H.; Reiding, K.R.; Beelen, R.H.J.; van Ittersum, F.J.; Wuhrer, M.; Dotz, V. Effluent and serum protein N-glycosylation is associated with inflammation and peritoneal membrane transport characteristics in peritoneal dialysis patients. Sci. Rep. 2018, 8, 979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlieper, G.; Hess, K.; Floege, J.; Marx, N. The vulnerable patient with chronic kidney disease. Nephrol. Dial. Transplant. 2016, 31, 382–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunns, G.R.; Moore, E.E.; Chapman, M.P.; Moore, H.B.; Stettler, G.R.; Peltz, E.; Burlew, C.C.; Silliman, C.C.; Banerjee, A.; Sauaia, A. The hypercoagulability paradox of chronic kidney disease: The role of fibrinogen. Am. J. Surg. 2017, 214, 1215–1218. [Google Scholar] [CrossRef]
- Hoffmann, M.; Pioch, M.; Pralow, A.; Hennig, R.; Kottler, R.; Reichl, U.; Rapp, E. The fine art of destruction: A guide to in-depth glycoproteomic analyses-exploiting the diagnostic potential of fragment ions. Proteomics 2018, 18, e1800282. [Google Scholar] [CrossRef] [Green Version]
- Zauner, G.; Hoffmann, M.; Rapp, E.; Koelman, C.A.M.; Dragan, I.; Deelder, A.M.; Wuhrer, M.; Hensbergen, P.J. Glycoproteomic analysis of human fibrinogen reveals novel regions of O-glycosylation. J. Proteome Res. 2012, 11, 5804–5814. [Google Scholar] [CrossRef]
- Nagel, T.; Klaus, F.; Ibanez, I.G.; Wege, H.; Lohse, A.; Meyer, B. Fast and facile analysis of glycosylation and phosphorylation of fibrinogen from human plasma-correlation with liver cancer and liver cirrhosis. Anal. Bioanal. Chem. 2018, 410, 7965–7977. [Google Scholar] [CrossRef]
- Gligorijević, N.; Minić, S.; Križáková, M.; Katrlík, J.; Nedić, O. Structural changes of fibrinogen as a consequence of cirrhosis. Thromb. Res. 2018, 166, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Zhu, H. Protein array-based approaches for biomarker discovery in cancer. Genom. Proteom. Bioinf. 2017, 15, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Adamczyk, B.; Struwe, W.B.; Ercan, A.; Nigrovic, P.A.; Rudd, P.M. Characterization of fibrinogen glycosylation and its importance for serum/plasma N-glycome analysis. J. Proteome Res. 2013, 12, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Nagel, T.; Meyer, B. Simultaneous characterization of sequence polymorphisms, glycosylation and phosphorylation of fibrinogen in a direct analysis by LC-MS. Biochim. Biophys. Acta 2014, 1844, 2284–2289. [Google Scholar] [CrossRef] [PubMed]
- Pacchiarotta, T.; Hensbergen, P.J.; Wuhrer, M.; van Nieuwkoop, C.; Nevedomskaya, E.; Derks, R.J.; Schoenmaker, B.; Koeleman, C.A.M.; van Dissel, J.; Deelder, A.M.; et al. Fibrinogen alpha chain O-glycopeptides as possible markers of urinary tract infection. J. Proteom. 2012, 75, 1067–1073. [Google Scholar] [CrossRef]
- Hoffmann, M.; Marx, K.; Reichl, U.; Wuhrer, M.; Rapp, E. Site-specific O-glycosylation analysis of human blood plasma proteins. Mol. Cell. Proteom. 2016, 15, 624–641. [Google Scholar] [CrossRef] [Green Version]
- Mise, K.; Imamura, M.; Yamaguchi, S.; Teshigawara, S.; Tone, A.; Uchido, H.A.; Eguchi, J.; Nakatsuka, A.; Ogawa, D.; Yoshida, M.; et al. Identification of novel urinary biomarkers for predicting renal prognosis in patients with type 2 diabetes by glycan profiling in a multicenter prospective cohort study: U-CARE study 1. Diabetes Care. 2018, 41, 1765–1775. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Yu, H.; Zhang, D.; Han, Q.; Yang, X.; Liu, X.; Wang, J.; Zhang, K.; Yang, F.; Cai, G.; et al. Alteration of glycosylation in serum proteins: A new potential indicator to distinguish non-diabetic renal diseases from diabetic nephropathy. RSC Adv. 2018, 8, 38872. [Google Scholar] [CrossRef] [Green Version]
- Adua, E.; Anto, E.O.; Roberts, P.; Kantanka, O.S.; Aboagye, E.; Wang, W. The potential of N-glycosylation profiles as biomarkers for monitoring the progression of type II diabetes mellitus towards diabetic kidney disease. J. Diabetes Metab. Disord. 2018, 17, 233–246. [Google Scholar] [CrossRef]
- Barrios, C.; Zierer, J.; Gudelj, I.; Štambuk, J.; Ugrina, I.; Rodríguez, E.; Soler, M.J.; Pavić, T.; Šimurina, M.; Keser, T.; et al. Glycosylation profile of IgG in moderate kidney dysfunction. J. Am. Soc. Nephrol. 2016, 27, 933–941. [Google Scholar] [CrossRef] [Green Version]
- Hatakeyama, S.; Amano, M.; Tobisawa, Y.; Yoneyema, T.; Tsushima, M.; Hirose, K.; Yoneyema, T.; Hashimoto, Y.; Koie, T.; Saitoh, H.; et al. Serum N-glycan profiling predicts prognosis in patients undergoing hemodialysis. Sci. World J. 2013, 268407. [Google Scholar] [CrossRef]
- Schuett, K.; Savvaidis, A.; Maxeiner, S.; Lysaja, K.; Jankowski, V.; Schirmer, S.H.; Dimković, N.; Boor, P.; Kaesler, N.; Dekker, F.W.; et al. Clot structure: A potent mortality risk factor in patients on hemodialysis. J. Am. Soc. Nephrol. 2017, 28, 1622–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Hsu, H.C.; Mountz, J.D.; Allen, J.G. Unmasking fucosylation: From cell adhesion to immune system regulation and diseases. Cell Chem. Biol. 2018, 25, 499–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poland, D.C.W.; Schalkwijk, C.G.; Stehouwer, C.D.A.; Koeleman, C.A.M.; van het Hof, B.; van Dijk, W. Increased α3-fucosylation of α1-acid glycoprotein in Type I diabetic patients related to vascular function. Glycoconj. J. 2001, 18, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.S.; Heijmans, R.; Meulen, C.K.E.; Lieverse, A.G.; Gornik, O.; Sijbrands, E.J.G.; Lauc, G.; van Hoek, M. Association of the IgG N-glycome with the course of kidney function in type 2 diabetes. BMJ Open Diabetes Res. Care 2020, 8, e001026. [Google Scholar] [CrossRef]
- Fang, M.; Kang, L.; Wang, X.; Guo, X.; Wang, W.; Qin, B.; Du, X.; Tang, Q.; Lin, H. Inhibition of core fucosylation limits progression of diabetic kidney disease. Biochem. Biophys. Res. Commun. 2019, 520, 612–618. [Google Scholar] [CrossRef]
- Bermingham, M.L.; Colombo, M.; McGurnaghan, S.J.; Blackbourn, L.A.K.; Vučković, F.; Pučić Baković, M.; Trbojević-Akmačić, I.; Lauc, G.; Agakov, F.; Agakova, A.S.; et al. SDRN Type 1 Bioresource Investigators. N-glycan profile and kidney disease in type 1 diabetes. Diabetes Care 2018, 41, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Burkart, J. Metabolic consequences of peritoneal dialysis. Semin. Dial. 2004, 17, 498–504. [Google Scholar] [CrossRef]
- Farrell, D.H. Pathophysiologic roles of the fibrinogen gamma chain. Curr. Opin. Hematol. 2004, 11, 151–155. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Peritoneal Dialysis (PD), n = 52 | Healthy Control (HC), n = 32 | |||
|---|---|---|---|---|
| Male, n = 26 | Female, n = 26 | Male, n = 16 | Female, n = 16 | |
| Age (years) | 65.5 ± 15.8 | 61.0 ± 29.3 | ||
| Period on PD (months) | 30.0 ± 49.5 | / | ||
| With peritonitis | 20 (38.5%) | / | ||
| With diabetes | 20 (38.5%) | / | ||
| Receiving erythropoietin | 22 (42.3%) | / | ||
| Ultrafiltration rate (mL/day) | 1000 ± 650 | |||
| Residual urine (mL/day) | 750 ± 975 | |||
| Biochemical parameters | ||||
| Glucose (mM) | 5.6 ± 2.5 | 5.3 ± 0.9 | ||
| Urea (mM) | 16.1 ± 6.3 * | 5.1 ± 0.8 | ||
| Creatinine (μM) | 653.0 ± 204.3 * | 81.0 ± 22.0 | ||
| Uric acid (μM) | 310.0 ± 62.5 * | 325.0 ± 91.3 | ||
| Total protein (g/L) | 65.0 ± 9.3 * | 72.3 ± 2.7 | ||
| Albumin (g/L) | 37.0 ± 6.0 * | 47.5 ± 3.2 | ||
| Fibrinogen (g/L) | 4.4 ± 0.9 | 2.7 ± 0.8 | ||
| Sedimentation | 85.0 ± 44.0 * | 13.0 ± 9.5 | ||
| Iron (mM) | 11.5 ± 3.9 * | 17.7 ± 3.8 | ||
| Glucose Solutions Used in CAPD | RU < 700 mL (n = 26) | RU > 700 mL (n = 26) |
|---|---|---|
| 4 x * 1.36% | 6 | 17 |
| 4 x 1.50% | 6 | 3 |
| 3 x 1.36% + 1 x 2.27% | 2 | 3 |
| 3 x 1.50% + 1 x 2.30% | 2 | 1 |
| 2 x 1.36% + 2 x 2.27% | - | 2 |
| 3 x 1.36% + 2 x 2.27% | 4 | - |
| 2 x 1.36% + 2 x 2.27% + icodextrin | 6 | - |
| Lectin (Source) | Carbohydrate Specificity | Lectin Microarray | Lectin Blot |
|---|---|---|---|
| PNA (Arachis hypogaea) | Galβ1,3GalNAc | + (S/N < 3) | |
| MAL-I (Maackia amurensis) | NeuNAcα2,3Galβ1,4GlcNAc | + (S/N < 3) | |
| MAL-II (Maackia amurensis) | NeuNAcα2,3Galβ1,3(±NeuNAc2,6)GalNAc | + (S/N < 10) | + |
| PHA-L (Phaseolus vulgaris) | Tri/tetraantennary complex type N-glycans w/terminal Gal | + (S/N < 10) | + |
| DSL (Datura stramonium) | GlcNAcβ1,4GlcNAc oligomers; Galβ1,4GlcNAc | +(S/N < 10) | |
| GNL (Galanthus nivalis) | High mannose type N-glycans; Manα1,3Man | + (S/N < 10) | |
| GSL-I (Griffonia simplicifolia) | Galα1,3Gal; Galα1,3GalNAc | + (S/N < 50) | |
| WGA (Triticum vulgaris) | GlcNAcβ1,4GlcNAc; chitin oligomers; NeuAc | + (S/N < 50) | |
| SNA (Sambucus nigra) | NeuNAcα2,6Gal/GalNAc | + (S/N < 50) | + |
| NPL (Narcissus pseudonarcissus) | High mannose type N-glycans; Manα1,6Man | + (S/N < 50) | |
| LCA (Lens culinaris) | αDGlc, αDMan in N-glycans with Fuca1,6GlcNAc | + (S/N < 50) | + |
| PhoSL (Pholiota squarrosa) | Fucα1,6GlcNAc | + (S/N < 50) | |
| PHA-E (Phaseolus vulgaris) | Galβ1,4GlcNAcβ1,2Man with bisecting GlcNAc | + (S/N < 50) | + |
| AAL (Aleuria aurantia) | Fucα1,6GlcNAc; Fucα1,3(Galβ1,4)GlcNAc | + (S/N < 50) | + |
| ConA (Canavalia ensiformis) | Manα1,6(Manα1,3)Man | + (S/N > 50) | |
| RCA (Ricinus communis) | Galβ1,4GlcNAc | + (S/N > 50) |
| vs. | SNA | ConA | MAL-II | PHA-E | PHA-L | WGA | RCA | AAL | PhoSL | GSL-I | NPL | LCA | DSL | GNL |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SNA | 1 | 0.02202 | 0.57548 | 0.01016 | 0.61708 | 0.0096 | 0.00104 | 0.26272 | 0.7417 | 0.00078 | 0.12114 | 0.00001 | 0.00001 | 0.29834 |
| ConA | 1 | 0.06576 | 0.11134 | 0.01878 | 0.13622 | 0.02642 | 0.0098 | 0.01242 | 0.00001 | 0.90448 | 0.00001 | 0.0007 | 0.56192 | |
| MAL-II | 1 | 0.05 | 0.86502 | 0.00288 | 0.00362 | 0.88866 | 0.36812 | 0.06576 | 0.3843 | 0.00328 | 0.00001 | 0.30772 | ||
| PHA-E | 1 | 0.00001 | 0.77948 | 0.39532 | 0.00018 | 0.01732 | 0.00001 | 0.28014 | 0.00001 | 0.00188 | 0.67448 | |||
| PHA-L | 1 | 0.0001 | 0.00001 | 0.34722 | 0.12602 | 0.00012 | 0.09894 | 0.00001 | 0.00001 | 0.04236 | ||||
| WGA | 1 | 0.53526 | 0.00001 | 0.00328 | 0.00001 | 0.02852 | 0.00001 | 0.00006 | 0.1031 | |||||
| RCA | 1 | 0.00001 | 0.00001 | 0.00001 | 0.0278 | 0.00001 | 0.00152 | 0.30302 | ||||||
| AAL | 1 | 0.06576 | 0.00001 | 0.034 | 0.00001 | 0.00001 | 0.01552 | |||||||
| PHOSL | 1 | 0.00014 | 0.50286 | 0.00001 | 0.00001 | 0.29834 | ||||||||
| GSL-I | 1 | 0.00018 | 0.0088 | 0.00001 | 0.00006 | |||||||||
| NPL | 1 | 0.00001 | 0.00001 | 0.92034 | ||||||||||
| LCA | 1 | 0.00001 | 0.00001 | |||||||||||
| DSL | 1 | 0.00001 | ||||||||||||
| GNL | 1 | |||||||||||||
| SNA | ConA | MAL-II | PHA-E | PHA-L | WGA | RCA | AAL | PhoSL | GSL-I | NPL | LCA | DSL | GNL | |
| 0.05 > p > 0.001 | 0 | 4 | 1 | 2 | 0 | 4 | 4 | 0 | 0 | 1 | 1 | 0 | 2 | 2 |
| p < 0.001 | 2 | 2 | 0 | 4 | 2 | 4 | 5 | 2 | 2 | 0 | 2 | 0 | 11 | 2 |
| 0.05 > p > 0.001 | 4 | 1 | 2 | 1 | 2 | 0 | 1 | 3 | 3 | 0 | 2 | 2 | 0 | 0 |
| p < 0.001 | 1 | 1 | 1 | 0 | 4 | 1 | 0 | 4 | 2 | 11 | 1 | 11 | 0 | 1 |
| B | p | OR | CI 95% | B | p | OR | CI 95% | ||
|---|---|---|---|---|---|---|---|---|---|
| SNA | 0.621 | - | - | ConA | - | 0.228 | - | - | |
| RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 | RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 |
| MAL-II | −0.074 | 0.045 | 0.929 | 0.864–0.998 | PHA-E | - | 0.323 | - | - |
| RD | −2.006 | 0.001 | 0.134 | 0.040–0.451 | RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 |
| PHA-L | - | 0.536 | - | - | WGA | - | 0.068 | - | - |
| RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 | RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 |
| RCA | - | 0.213 | - | - | AAL | −0.006 | 0.029 | 0.994 | 0.989–0.999 |
| RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 | RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 |
| PhoSL | - | 0.172 | - | - | GSL-I | −0.044 | 0.037 | 0.957 | 0.918–0.997 |
| RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 | RD | −1.949 | 0.001 | 0.142 | 0.043–0.471 |
| NPL | −0.043 | 0.013 | 0.958 | 0.926–0.991 | LCA | −0.005 | 0.039 | 0.995 | 0.991–0.999 |
| RD | −2.084 | 0.002 | 0.124 | 0.034–0.456 | RD | −1.959 | 0.001 | 0.141 | 0.043–0.466 |
| DSL | −0.022 | 0.037 | 0.978 | 0.958–0.999 | GNL | - | 0.072 | - | - |
| RD | −2.065 | 0.001 | 0.978 | 0.036–0.447 | RD | −1.786 | 0.002 | 0.168 | 0.055–0.509 |
| MAL-II | SNA | LCA | AAL | PHA-E | PHA-L | |
|---|---|---|---|---|---|---|
| Aα | 0.27134 | 0.95216 | - | 0.22246 | 0.18352 | 0.07346 |
| Bβ | 0.01174 * | 0.00214 * | 0.06724 | 0.00652 * | 0.3843 | 0.6818 |
| γ | - | 0.00932 * | 0.00262 * | 0.01278 * | 0.03236 * | - |
| Aα/Bβ | 0.65272 | 0.05614 | - | 0.86502 | 0.14706 | 0.18352 |
| Aα/γ | - | 0.27134 | - | 0.01278 * | 0.03236 * | - |
| Bβ/γ | - | 0.07346 | 0.00804 * | 0.00318 * | 0.52218 | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baralić, M.; Gligorijević, N.; Brković, V.; Katrlík, J.; Pažitná, L.; Šunderić, M.; Miljuš, G.; Penezić, A.; Dobrijević, Z.; Laušević, M.; et al. Fibrinogen Fucosylation as a Prognostic Marker of End-Stage Renal Disease in Patients on Peritoneal Dialysis. Biomolecules 2020, 10, 1165. https://doi.org/10.3390/biom10081165
Baralić M, Gligorijević N, Brković V, Katrlík J, Pažitná L, Šunderić M, Miljuš G, Penezić A, Dobrijević Z, Laušević M, et al. Fibrinogen Fucosylation as a Prognostic Marker of End-Stage Renal Disease in Patients on Peritoneal Dialysis. Biomolecules. 2020; 10(8):1165. https://doi.org/10.3390/biom10081165
Chicago/Turabian StyleBaralić, Marko, Nikola Gligorijević, Voin Brković, Jaroslav Katrlík, Lucia Pažitná, Miloš Šunderić, Goran Miljuš, Ana Penezić, Zorana Dobrijević, Mirjana Laušević, and et al. 2020. "Fibrinogen Fucosylation as a Prognostic Marker of End-Stage Renal Disease in Patients on Peritoneal Dialysis" Biomolecules 10, no. 8: 1165. https://doi.org/10.3390/biom10081165
APA StyleBaralić, M., Gligorijević, N., Brković, V., Katrlík, J., Pažitná, L., Šunderić, M., Miljuš, G., Penezić, A., Dobrijević, Z., Laušević, M., Nedić, O., & Robajac, D. (2020). Fibrinogen Fucosylation as a Prognostic Marker of End-Stage Renal Disease in Patients on Peritoneal Dialysis. Biomolecules, 10(8), 1165. https://doi.org/10.3390/biom10081165