
Molecular Biomarkers in Cancer



Abstract
:1. Introduction
2. Cancer-Associated Alterations
2.1. Germline Genetic Variants
2.2. Somatic Genetic Mutations
2.3. Epigenetic Variants
2.4. Transcriptional Alterations
2.4.1. mRNAs
2.4.2. miRNAs
2.4.3. CircRNAs
2.4.4. Other lncRNAs
2.4.5. Summary of Transcriptional Alterations
2.5. Proteomic Changes
2.6. Cellular Phenotype
3. Sources of Molecular Cancer Biomarkers
3.1. Blood
3.1.1. WBCs
3.1.2. CTCs
3.1.3. Plasma/Serum
3.2. Urine
3.3. Stool
3.4. Exhaled Breath
3.5. Saliva/Buccal Swabs
3.6. EVs
4. Techniques Used to Detect Molecular Cancer Biomarkers
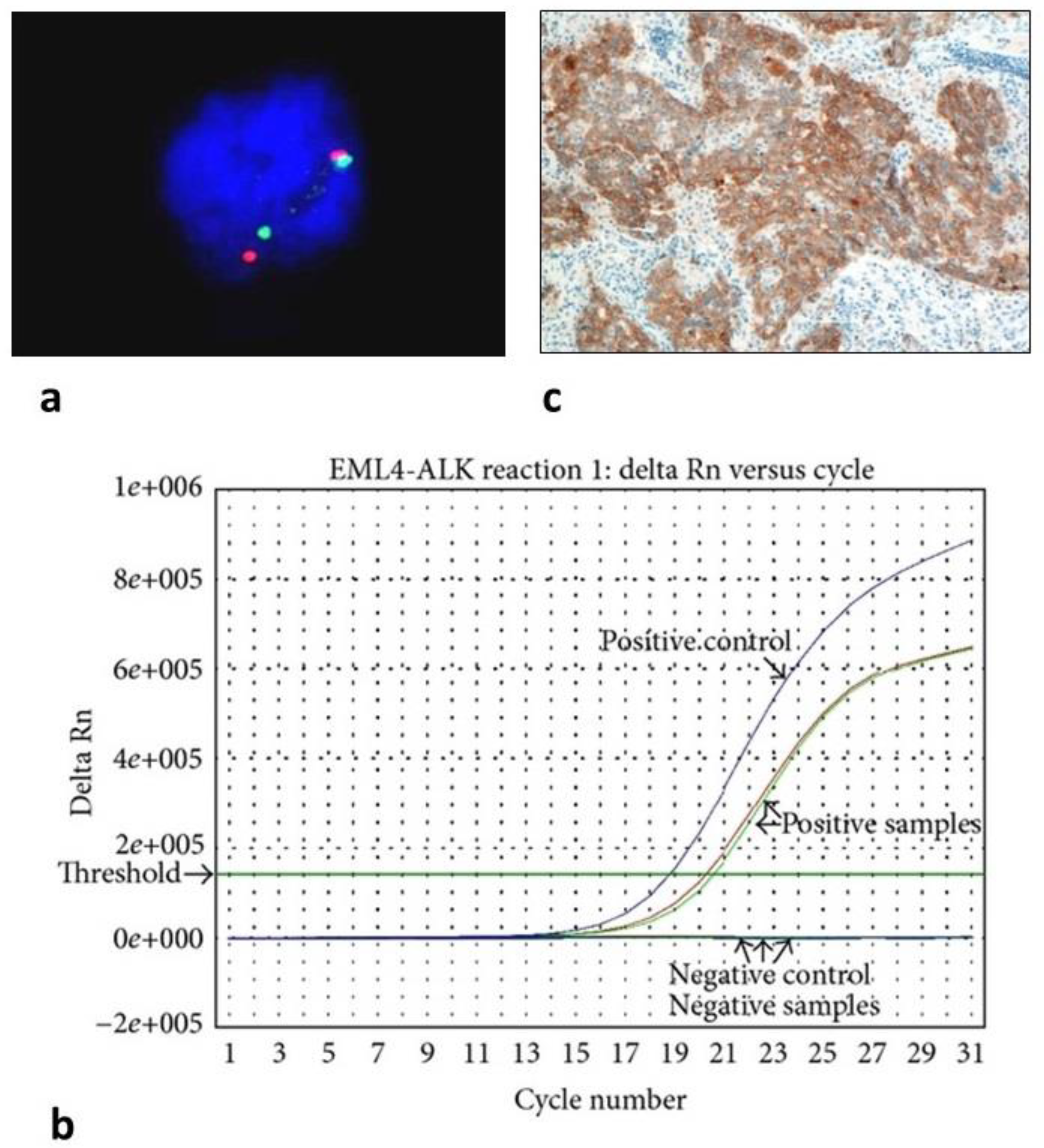
4.1. FISH
4.2. PCR/Real-Time PCR/Digital PCR
4.3. NGS
4.4. Flow Cytometry
4.5. Gene Expression Microarrays
4.6. IHC
4.7. ELISA
4.8. Lectin Microarrays
4.9. Other Proteomic Tools
4.10. Biosensors/Nanotechnology
4.11. Microfluidics
4.12. CRISPR-Based ctDNA/RNA Detection
4.13. Synthetic Biomarker Technology
5. Clinical Applications of Cancer Biomarkers: Examples
5.1. Cancer Risk Assessment Biomarkers
5.2. Screening and Early Cancer Detection Biomarkers
5.3. Accurate Cancer Diagnosis Biomarkers
5.4. Patient Prognosis Biomarker
5.5. Biomarkers Predicting Response to Cancer Therapy
5.6. Biomarkers for Cancer Surveillance and Monitoring Response
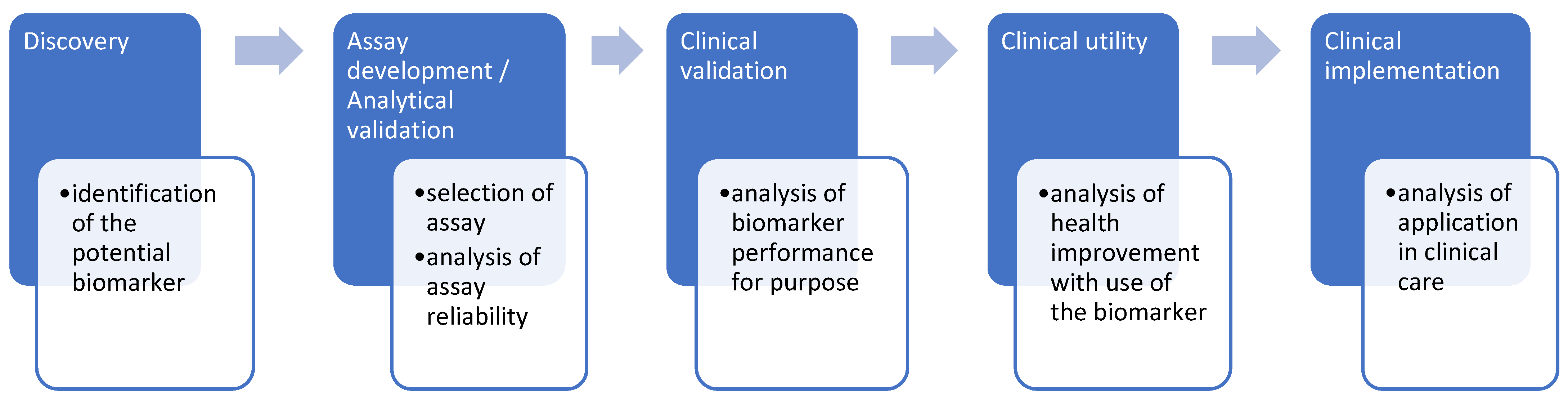
6. Steps in the Search for New Biomarkers
6.1. Discovery
6.2. Assay Development and Analytical Validation
6.3. Clinical Validation
6.4. Clinical Utility
6.5. Clinical Implementation
7. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.Cancer.Gov/Publications/Dictionaries/Cancer-Terms/Def/Tumor-Marker-Test (accessed on 22 February 2022).
- Schienda, J.; Church, A.J.; Corson, L.B.; Decker, B.; Clinton, C.M.; Manning, D.K.; Imamovic-Tuco, A.; Reidy, D.; Strand, G.R.; Applebaum, M.A.; et al. Germline Sequencing Improves Tumor-Only Sequencing Interpretation in a Precision Genomic Study of Patients With Pediatric Solid Tumor. JCO Precis. Oncol. 2021, 5, PO.21.00281. [Google Scholar] [CrossRef] [PubMed]
- Akras, Z.; Bungo, B.; Leach, B.H.; Marquard, J.; Ahluwalia, M.; Carraway, H.; Grivas, P.; Sohal, D.P.S.; Funchain, P. Primer on Hereditary Cancer Predisposition Genes Included within Somatic Next-Generation Sequencing Panels. JCO Precis. Oncol. 2019, 3, 1–11. [Google Scholar] [CrossRef]
- Slade, D. PARP and PARG Inhibitors in Cancer Treatment. Genes Dev. 2020, 34, 360–394. [Google Scholar] [CrossRef] [Green Version]
- Huang, K.-L.; Mashl, R.J.; Wu, Y.; Ritter, D.I.; Wang, J.; Oh, C.; Paczkowska, M.; Reynolds, S.; Wyczalkowski, M.A.; Oak, N.; et al. Pathogenic Germline Variants in 10,389 Adult Cancers. Cell 2018, 173, 355–370.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terraf, P.; Pareja, F.; Brown, D.N.; Ceyhan-Birsoy, O.; Misyura, M.; Rana, S.; O’Reilly, E.; Carlo, M.I.; Aghajanian, C.; Liu, Y.; et al. Comprehensive Assessment of Germline Pathogenic Variant Detection in Tumor-Only Sequencing. Ann. Oncol. 2022, 33, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Velázquez, C.; Lastra, E.; Avila Cobos, F.; Abella, L.; de la Cruz, V.; Hernando, B.A.; Hernández, L.; Martínez, N.; Infante, M.; Durán, M. A Comprehensive Custom Panel Evaluation for Routine Hereditary Cancer Testing: Improving the Yield of Germline Mutation Detection. J. Transl. Med. 2020, 18, 232. [Google Scholar] [CrossRef]
- Cortés-Ciriano, I.; Lee, J.J.-K.; Xi, R.; Jain, D.; Jung, Y.L.; Yang, L.; Gordenin, D.; Klimczak, L.J.; Zhang, C.-Z.; Pellman, D.S.; et al. Comprehensive Analysis of Chromothripsis in 2658 Human Cancers Using Whole-Genome Sequencing. Nat. Genet. 2020, 52, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Kandoth, C.; McLellan, M.D.; Vandin, F.; Ye, K.; Niu, B.; Lu, C.; Xie, M.; Zhang, Q.; McMichael, J.F.; Wyczalkowski, M.A.; et al. Mutational Landscape and Significance across 12 Major Cancer Types. Nature 2013, 502, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Pan-Cancer Analysis of Whole Genomes. Nature 2020, 578, 82–93. [CrossRef] [Green Version]
- Bailey, M.H.; Tokheim, C.; Porta-Pardo, E.; Sengupta, S.; Bertrand, D.; Weerasinghe, A.; Colaprico, A.; Wendl, M.C.; Kim, J.; Reardon, B.; et al. Comprehensive Characterization of Cancer Driver Genes and Mutations. Cell 2018, 173, 371–385.e18. [Google Scholar] [CrossRef] [Green Version]
- Youssef, O.; Sarhadi, V.K.; Armengol, G.; Piirilä, P.; Knuuttila, A.; Knuutila, S. Exhaled Breath Condensate as a Source of Biomarkers for Lung Carcinomas. A Focus on Genetic and Epigenetic Markers—A Mini-Review. Genes Chromosomes Cancer 2016, 55, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Sarhadi, V.; Lahti, L.; Saberi, F.; Youssef, O.; Kokkola, A.; Karla, T.; Tikkanen, M.; Rautelin, H.; Puolakkainen, P.; Salehi, R.; et al. Gut Microbiota and Host Gene Mutations in Colorectal Cancer Patients and Controls of Iranian and Finnish Origin. Anticancer. Res. 2020, 40, 1325–1334. [Google Scholar] [CrossRef] [PubMed]
- Armengol, G.; Sarhadi, V.K.; Ghanbari, R.; Doghaei-Moghaddam, M.; Ansari, R.; Sotoudeh, M.; Puolakkainen, P.; Kokkola, A.; Malekzadeh, R.; Knuutila, S. Driver Gene Mutations in Stools of Colorectal Carcinoma Patients Detected by Targeted Next-Generation Sequencing. J. Mol. Diagn. 2016, 18, 471–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuononen, K.; Sarhadi, V.K.; Wirtanen, A.; Rönty, M.; Salmenkivi, K.; Knuuttila, A.; Remes, S.; Telaranta-Keerie, A.I.; Bloor, S.; Ellonen, P.; et al. Targeted Resequencing Reveals ALK Fusions in Non-Small Cell Lung Carcinomas Detected by FISH, Immunohistochemistry, and Real-Time RT-PCR: A Comparison of Four Methods. Biomed. Res. Int. 2013, 2013, 757490. [Google Scholar] [CrossRef]
- Müller, D.; Győrffy, B. DNA Methylation-Based Diagnostic, Prognostic, and Predictive Biomarkers in Colorectal Cancer. Biochim. Biophys. Acta Rev. Cancer 2022, 1877, 188722. [Google Scholar] [CrossRef]
- Poon, M.T.C.; Keni, S.; Vimalan, V.; Ip, C.; Smith, C.; Erridge, S.; Weir, C.J.; Brennan, P.M. Extent of MGMT Promoter Methylation Modifies the Effect of Temozolomide on Overall Survival in Patients with Glioblastoma: A Regional Cohort Study. Neurooncol. Adv. 2021, 3, vdab171. [Google Scholar] [CrossRef]
- Constâncio, V.; Nunes, S.P.; Henrique, R.; Jerónimo, C. DNA Methylation-Based Testing in Liquid Biopsies as Detection and Prognostic Biomarkers for the Four Major Cancer Types. Cells 2020, 9, 624. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Gole, J.; Gore, A.; He, Q.; Lu, M.; Min, J.; Yuan, Z.; Yang, X.; Jiang, Y.; Zhang, T.; et al. Non-Invasive Early Detection of Cancer Four Years before Conventional Diagnosis Using a Blood Test. Nat. Commun. 2020, 11, 3475. [Google Scholar] [CrossRef]
- Mio, C.; Damante, G. Challenges in Promoter Methylation Analysis in the New Era of Translational Oncology: A Focus on Liquid Biopsy. Biochim. Biophys. Acta Mol. Basis Dis. 2022, 1868, 166390. [Google Scholar] [CrossRef]
- Larson, M.H.; Pan, W.; Kim, H.J.; Mauntz, R.E.; Stuart, S.M.; Pimentel, M.; Zhou, Y.; Knudsgaard, P.; Demas, V.; Aravanis, A.M.; et al. A Comprehensive Characterization of the Cell-Free Transcriptome Reveals Tissue- and Subtype-Specific Biomarkers for Cancer Detection. Nat. Commun. 2021, 12, 2357. [Google Scholar] [CrossRef]
- Ludwig, N.; Leidinger, P.; Becker, K.; Backes, C.; Fehlmann, T.; Pallasch, C.; Rheinheimer, S.; Meder, B.; Stähler, C.; Meese, E.; et al. Distribution of MiRNA Expression across Human Tissues. Nucleic Acids Res. 2016, 44, 3865–3877. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Yadav, T.; Rani, V. Exploring MiRNA Based Approaches in Cancer Diagnostics and Therapeutics. Crit. Rev. Oncol. /Hematol. 2016, 98, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Inoue, J.; Inazawa, J. Cancer-Associated MiRNAs and Their Therapeutic Potential. J. Hum. Genet. 2021, 66, 937–945. [Google Scholar] [CrossRef] [PubMed]
- Cacheux, J.; Bancaud, A.; Leichlé, T.; Cordelier, P. Technological Challenges and Future Issues for the Detection of Circulating MicroRNAs in Patients with Cancer. Front. Chem. 2019, 7, 815. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.; Liu, X.; Pan, B.; Hu, X.; Zhu, Y.; Su, Y.; Guo, Z.; Zhang, G.; Xu, M.; Xu, X.; et al. Serum Exosomal MiR-122 as a Potential Diagnostic and Prognostic Biomarker of Colorectal Cancer with Liver Metastasis. J. Cancer 2020, 11, 630–637. [Google Scholar] [CrossRef]
- Dohmen, J.; Semaan, A.; Kobilay, M.; Zaleski, M.; Branchi, V.; Schlierf, A.; Hettwer, K.; Uhlig, S.; Hartmann, G.; Kalff, J.C.; et al. Diagnostic Potential of Exosomal MicroRNAs in Colorectal Cancer. Diagnostics 2022, 12, 1413. [Google Scholar] [CrossRef]
- Wu, Q.; Yu, L.; Lin, X.; Zheng, Q.; Zhang, S.; Chen, D.; Pan, X.; Huang, Y. Combination of Serum MiRNAs with Serum Exosomal MiRNAs in Early Diagnosis for Non-Small-Cell Lung Cancer. Cancer Manag. Res. 2020, 12, 485–495. [Google Scholar] [CrossRef] [Green Version]
- Preethi, K.A.; Selvakumar, S.C.; Ross, K.; Jayaraman, S.; Tusubira, D.; Sekar, D. Liquid Biopsy: Exosomal MicroRNAs as Novel Diagnostic and Prognostic Biomarkers in Cancer. Mol. Cancer 2022, 21, 54. [Google Scholar] [CrossRef]
- Kaźmierczak, D.; Eide, I.J.Z.; Gencheva, R.; Lai, Y.; Lewensohn, R.; Tsakonas, G.; Grundberg, O.; de Petris, L.; McGowan, M.; Brustugun, O.T.; et al. Elevated Expression of MiR-494-3p Is Associated with Resistance to Osimertinib in EGFR T790M-Positive Non-Small Cell Lung Cancer. Transl. Lung Cancer Res. 2022, 11, 722–734. [Google Scholar] [CrossRef]
- Janpipatkul, K.; Trachu, N.; Watcharenwong, P.; Panvongsa, W.; Worakitchanon, W.; Metheetrairut, C.; Oranratnachai, S.; Reungwetwattana, T.; Chairoungdua, A. Exosomal MicroRNAs as Potential Biomarkers for Osimertinib Resistance of Non-Small Cell Lung Cancer Patients. Cancer Biomark. 2021, 31, 281–294. [Google Scholar] [CrossRef]
- Li, X.; Chen, C.; Wang, Z.; Liu, J.; Sun, W.; Shen, K.; Lv, Y.; Zhu, S.; Zhan, P.; Lv, T.; et al. Elevated Exosome-Derived MiRNAs Predict Osimertinib Resistance in Non-Small Cell Lung Cancer. Cancer Cell Int. 2021, 21, 428. [Google Scholar] [CrossRef] [PubMed]
- Leonetti, A.; Capula, M.; Minari, R.; Mazzaschi, G.; Gregori, A.; el Hassouni, B.; Papini, F.; Bordi, P.; Verzè, M.; Avan, A.; et al. Dynamic Evaluation of Circulating MiRNA Profile in EGFR-Mutated NSCLC Patients Treated with EGFR-TKIs. Cells 2021, 10, 1520. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Tang, Y.; Song, X.; Xie, L.; Zhao, S.; Song, X. Tumor-Derived Exosomal MiRNAs as Diagnostic Biomarkers in Non-Small Cell Lung Cancer. Front. Oncol. 2020, 10, 560025. [Google Scholar] [CrossRef]
- Tang, Y.; Zhang, Z.; Song, X.; Yu, M.; Niu, L.; Zhao, Y.; Wang, L.; Song, X.; Xie, L. Tumor-Derived Exosomal MiR-620 as a Diagnostic Biomarker in Non-Small-Cell Lung Cancer. J. Oncol. 2020, 2020, 6691211. [Google Scholar] [CrossRef] [PubMed]
- Todorova, V.K.; Byrum, S.D.; Gies, A.J.; Haynie, C.; Smith, H.; Reyna, N.S.; Makhoul, I. Circulating Exosomal MicroRNAs as Predictive Biomarkers of Neoadjuvant Chemotherapy Response in Breast Cancer. Curr. Oncol. 2022, 29, 613–630. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, B.; Gondaliya, P.; Kirave, P.; Rawal, R.; Jain, A.; Garg, R.; Kalia, K. Exosome-Mediated Delivery of MiR-30a Sensitize Cisplatin-Resistant Variant of Oral Squamous Carcinoma Cells via Modulating Beclin1 and Bcl2. Oncotarget 2020, 11, 1832–1845. [Google Scholar] [CrossRef] [PubMed]
- Pantano, F.; Zalfa, F.; Iuliani, M.; Simonetti, S.; Manca, P.; Napolitano, A.; Tiberi, S.; Russano, M.; Citarella, F.; Foderaro, S.; et al. Large-Scale Profiling of Extracellular Vesicles Identified MiR-625-5p as a Novel Biomarker of Immunotherapy Response in Advanced Non-Small-Cell Lung Cancer Patients. Cancers 2022, 14, 2435. [Google Scholar] [CrossRef]
- Bustos, M.A.; Gross, R.; Rahimzadeh, N.; Cole, H.; Tran, L.T.; Tran, K.D.; Takeshima, L.; Stern, S.L.; O’Day, S.; Hoon, D.S.B. A Pilot Study Comparing the Efficacy of Lactate Dehydrogenase Levels Versus Circulating Cell-Free MicroRNAs in Monitoring Responses to Checkpoint Inhibitor Immunotherapy in Metastatic Melanoma Patients. Cancers 2020, 12, 3361. [Google Scholar] [CrossRef]
- Zeng, L.; Zeng, G.; Ye, Z. Bioinformatics Analysis for Identifying Differentially Expressed MicroRNAs Derived from Plasma Exosomes Associated with Radiotherapy Resistance in Non-Small-Cell Lung Cancer. Appl. Bionics Biomech. 2022, 2022, 9268206. [Google Scholar] [CrossRef]
- Zheng, Q.; Ding, H.; Wang, L.; Yan, Y.; Wan, Y.; Yi, Y.; Tao, L.; Zhu, C. Circulating Exosomal MiR-96 as a Novel Biomarker for Radioresistant Non-Small-Cell Lung Cancer. J. Oncol. 2021, 2021, 5893981. [Google Scholar] [CrossRef]
- Vadla, G.P.; Daghat, B.; Patterson, N.; Ahmad, V.; Perez, G.; Garcia, A.; Manjunath, Y.; Kaifi, J.T.; Li, G.; Chabu, C.Y. Combining Plasma Extracellular Vesicle Let-7b-5p, MiR-184 and Circulating MiR-22-3p Levels for NSCLC Diagnosis and Drug Resistance Prediction. Sci. Rep. 2022, 12, 6693. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, H. Serum Exosomal MiR-378 Upregulation Is Associated with Poor Prognosis in Non–Small-cell Lung Cancer Patients. J. Clin. Lab. Anal. 2020, 34, e23237. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.; Liu, H.; Chen, J. Reduced Circulating Exosomal MiR-382 Predicts Unfavorable Outcome in Non-Small Cell Lung Cancer. Int. J. Clin. Exp. Pathol. 2021, 14, 469–474. [Google Scholar] [PubMed]
- Kim, D.H.; Park, H.; Choi, Y.J.; Kang, M.-H.; Kim, T.-K.; Pack, C.-G.; Choi, C.-M.; Lee, J.C.; Rho, J.K. Exosomal MiR-1260b Derived from Non-Small Cell Lung Cancer Promotes Tumor Metastasis through the Inhibition of HIPK2. Cell Death Dis. 2021, 12, 747. [Google Scholar] [CrossRef]
- Huang, D.; Qu, D. Early Diagnostic and Prognostic Value of Serum Exosomal MiR-1246 in Non-Small Cell Lung Cancer. Int. J. Clin. Exp. Pathol. 2020, 13, 1601–1607. [Google Scholar]
- Jang, J.; Kim, Y.; Kang, K.; Kim, K.; Park, Y.; Kim, C. Multiple MicroRNAs as Biomarkers for Early Breast Cancer Diagnosis. Mol. Clin. Oncol. 2020, 14, 31. [Google Scholar] [CrossRef]
- Li, D.; Wang, J.; Ma, L.-J.; Yang, H.-B.; Jing, J.-F.; Jia, M.-M.; Zhang, X.-J.; Guo, F.; Gao, J.-N. Identification of Serum Exosomal MiR-148a as a Novel Prognostic Biomarker for Breast Cancer. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7303–7309. [Google Scholar] [CrossRef]
- Xun, J.; Du, L.; Gao, R.; Shen, L.; Wang, D.; Kang, L.; Chen, C.; Zhang, Z.; Zhang, Y.; Yue, S.; et al. Cancer-Derived Exosomal MiR-138-5p Modulates Polarization of Tumor-Associated Macrophages through Inhibition of KDM6B. Theranostics 2021, 11, 6847–6859. [Google Scholar] [CrossRef]
- Wang, X.; Qian, T.; Bao, S.; Zhao, H.; Chen, H.; Xing, Z.; Li, Y.; Zhang, M.; Meng, X.; Wang, C.; et al. Circulating Exosomal MiR-363-5p Inhibits Lymph Node Metastasis by Downregulating PDGFB and Serves as a Potential Noninvasive Biomarker for Breast Cancer. Mol. Oncol. 2021, 15, 2466–2479. [Google Scholar] [CrossRef]
- Wang, B.; Mao, J.-H.; Wang, B.-Y.; Wang, L.-X.; Wen, H.-Y.; Xu, L.-J.; Fu, J.-X.; Yang, H. Exosomal MiR-1910-3p Promotes Proliferation, Metastasis, and Autophagy of Breast Cancer Cells by Targeting MTMR3 and Activating the NF-ΚB Signaling Pathway. Cancer Lett. 2020, 489, 87–99. [Google Scholar] [CrossRef]
- Sueta, A.; Yamamoto, Y.; Tomiguchi, M.; Takeshita, T.; Yamamoto-Ibusuki, M.; Iwase, H. Differential expression of exosomal miRNAs between breast cancer patients with and without recurrence. Oncotarget 2017, 8, 69934–69944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirschfeld, M.; Rücker, G.; Weiß, D.; Berner, K.; Ritter, A.; Jäger, M.; Erbes, T. Urinary Exosomal MicroRNAs as Potential Non-Invasive Biomarkers in Breast Cancer Detection. Mol. Diagn. Ther. 2020, 24, 215–232. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Mo, F.; Song, X.; He, Y.; Yuan, Y.; Yan, J.; Yang, Y.; Huang, J.; Zhang, S. Exosomal Hsa-MiR-21-5p Is a Biomarker for Breast Cancer Diagnosis. PeerJ 2021, 9, e12147. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhang, M.; Xu, F.; Wang, Y.; Leng, D. Detection Significance of MiR-3662, MiR-146a, and MiR-1290 in Serum Exosomes of Breast Cancer Patients. J. Cancer Res. Ther. 2021, 17, 749–755. [Google Scholar] [CrossRef]
- Guo, T.; Wang, Y.; Jia, J.; Mao, X.; Stankiewicz, E.; Scandura, G.; Burke, E.; Xu, L.; Marzec, J.; Davies, C.R.; et al. The Identification of Plasma Exosomal MiR-423-3p as a Potential Predictive Biomarker for Prostate Cancer Castration-Resistance Development by Plasma Exosomal MiRNA Sequencing. Front. Cell Dev. Biol. 2021, 8, 602493. [Google Scholar] [CrossRef]
- Kim, M.Y.; Shin, H.; Moon, H.W.; Park, Y.H.; Park, J.; Lee, J.Y. Urinary Exosomal MicroRNA Profiling in Intermediate-Risk Prostate Cancer. Sci. Rep. 2021, 11, 7355. [Google Scholar] [CrossRef]
- Rode, M.P.; Silva, A.H.; Cisilotto, J.; Rosolen, D.; Creczynski-Pasa, T.B. MiR-425-5p as an Exosomal Biomarker for Metastatic Prostate Cancer. Cell. Signal. 2021, 87, 110113. [Google Scholar] [CrossRef]
- Shin, S.; Park, Y.H.; Jung, S.-H.; Jang, S.-H.; Kim, M.Y.; Lee, J.Y.; Chung, Y. Urinary Exosome MicroRNA Signatures as a Noninvasive Prognostic Biomarker for Prostate Cancer. NPJ Genom. Med. 2021, 6, 45. [Google Scholar] [CrossRef]
- Li, W.; Dong, Y.; Wang, K.J.; Deng, Z.; Zhang, W.; Shen, H.F. Plasma Exosomal MiR-125a-5p and MiR-141-5p as Non-Invasive Biomarkers for Prostate Cancer. Neoplasma 2021, 67, 1314–1318. [Google Scholar] [CrossRef]
- Li, Z.; Li, L.-X.; Diao, Y.-J.; Wang, J.; Ye, Y.; Hao, X.-K. Identification of Urinary Exosomal MiRNAs for the Non-Invasive Diagnosis of Prostate Cancer. Cancer Manag. Res. 2021, 13, 25–35. [Google Scholar] [CrossRef]
- He, L.; Ping, F.; Fan, Z.; Zhang, C.; Deng, M.; Cheng, B.; Xia, J. Salivary Exosomal MiR-24-3p Serves as a Potential Detective Biomarker for Oral Squamous Cell Carcinoma Screening. Biomed. Pharmacother. 2020, 121, 109553. [Google Scholar] [CrossRef] [PubMed]
- He, T.; Guo, X.; Li, X.; Liao, C.; Wang, X.; He, K. Plasma-Derived Exosomal MicroRNA-130a Serves as a Noninvasive Biomarker for Diagnosis and Prognosis of Oral Squamous Cell Carcinoma. J. Oncol. 2021, 2021, 5547911. [Google Scholar] [CrossRef]
- Chen, C.-M.; Chu, T.-H.; Chou, C.-C.; Chien, C.-Y.; Wang, J.-S.; Huang, C.-C. Exosome-Derived MicroRNAs in Oral Squamous Cell Carcinomas Impact Disease Prognosis. Oral Oncol. 2021, 120, 105402. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yang, D.; Chen, L.; Liu, Q.; Wang, W.; Yang, Z.; Shang, A.; Quan, W.; Li, D. Plasma Exosomal MiRNA-139-3p Is a Novel Biomarker of Colorectal Cancer. J. Cancer 2020, 11, 4899–4906. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Zhuang, Y.; Zhang, J.; Chen, M.; Wu, S. Four Circulating Exosomal MiRNAs as Novel Potential Biomarkers for the Early Diagnosis of Human Colorectal Cancer. Tissue Cell 2021, 70, 101499. [Google Scholar] [CrossRef]
- Handa, T.; Kuroha, M.; Nagai, H.; Shimoyama, Y.; Naito, T.; Moroi, R.; Kanazawa, Y.; Shiga, H.; Kakuta, Y.; Kinouchi, Y.; et al. Liquid Biopsy for Colorectal Adenoma: Is the Exosomal MiRNA Derived from Organoid a Potential Diagnostic Biomarker? Clin. Transl. Gastroenterol. 2021, 12, e00356. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liu, Y.; Sun, P.; Leng, K.; Xu, Y.; Mei, L.; Han, P.; Zhang, B.; Yao, K.; Li, C.; et al. Colorectal Cancer-Derived Exosomal MiR-106b-3p Promotes Metastasis by down-Regulating DLC-1 Expression. Clin. Sci. 2020, 134, 419–434. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Zhang, P.P.; Huang, J.J.; Wang, Z.Y.; Zhang, Z.H.; Yuan, J.Z.; Ma, E.M.; Liu, X.; Bai, J. Reduced Serum Exosomal MiR-874 Expression Predicts Poor Prognosis in Colorectal Cancer. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 664–672. [Google Scholar]
- Cho, W.-C.; Kim, M.; Park, J.W.; Jeong, S.-Y.; Ku, J.-L. Exosomal MiR-193a and Let-7g Accelerate Cancer Progression on Primary Colorectal Cancer and Paired Peritoneal Metastatic Cancer. Transl. Oncol. 2021, 14, 101000. [Google Scholar] [CrossRef]
- van Zweeden, A.A.; Opperman, R.C.M.; Honeywell, R.J.; Peters, G.J.; Verheul, H.M.W.; van der Vliet, H.J.; Poel, D. The Prognostic Impact of Circulating MiRNAs in Patients with Advanced Esophagogastric Cancer during Palliative Chemotherapy. Cancer Treat. Res. Commun. 2021, 27, 100371. [Google Scholar] [CrossRef]
- Gao, S.-S.; Wang, Y.-J.; Zhang, G.-X.; Zhang, W.-T. Potential Diagnostic Value of MiRNAs in Peripheral Blood for Osteosarcoma: A Meta-Analysis. J. Bone Oncol. 2020, 23, 100307. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Santillan, M.; Larrabeiti-Etxebarria, A.; Arzuaga-Mendez, J.; Lopez-Lopez, E.; Garcia-Orad, A. Circulating MiRNAs as Biomarkers in Diffuse Large B-Cell Lymphoma: A Systematic Review. Oncotarget 2018, 9, 22850–22861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayed, D.; Donia, T.; El-Shanshory, M.; Ali, E.; Mohamed, T. Evaluation of MicroRNA92, MicroRNA638 in Acute Lymphoblastic Leukemia of Egyptian Children. Asian Pac. J. Cancer Prev. 2021, 22, 1567–1572. [Google Scholar] [CrossRef]
- Manganelli, M.; Grossi, I.; Ferracin, M.; Guerriero, P.; Negrini, M.; Ghidini, M.; Senti, C.; Ratti, M.; Pizzo, C.; Passalacqua, R.; et al. Longitudinal Circulating Levels of MiR-23b-3p, MiR-126-3p and LncRNA GAS5 in HCC Patients Treated with Sorafenib. Biomedicines 2021, 9, 813. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhang, Q.; Zhang, J.; Li, C.; Miao, Y.-R.; Lei, Q.; Li, Q.; Guo, A.-Y. EVmiRNA: A Database of MiRNA Profiling in Extracellular Vesicles. Nucleic Acids Res. 2019, 47, D89–D93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, B.; Tian, Z.; Fan, W.; Ni, B. Circular RNA: A Novel Biomarker and Therapeutic Target for Human Cancers. Int. J. Med. Sci. 2019, 16, 292–301. [Google Scholar] [CrossRef] [Green Version]
- Qian, Y.; Shi, L.; Luo, Z. Long Non-Coding RNAs in Cancer: Implications for Diagnosis, Prognosis, and Therapy. Front. Med. 2020, 7, 902. [Google Scholar] [CrossRef]
- Zhang, J.; Yan, S.; Li, R.; Wang, G.; Kang, S.; Wang, Y.; Hou, W.; Wang, C.; Tian, W. CRMarker: A Manually Curated Comprehensive Resource of Cancer RNA Markers. Int. J. Biol. Macromol. 2021, 174, 263–269. [Google Scholar] [CrossRef]
- Wang, S.; Zhang, K.; Tan, S.; Xin, J.; Yuan, Q.; Xu, H.; Xu, X.; Liang, Q.; Christiani, D.C.; Wang, M.; et al. Circular RNAs in Body Fluids as Cancer Biomarkers: The New Frontier of Liquid Biopsies. Mol. Cancer 2021, 20, 13. [Google Scholar] [CrossRef]
- Stowell, S.R.; Ju, T.; Cummings, R.D. Protein Glycosylation in Cancer. Annu. Rev. Pathol. 2015, 10, 473–510. [Google Scholar] [CrossRef] [Green Version]
- Park, R.; da Silva, L.L.; Saeed, A. Immunotherapy Predictive Molecular Markers in Advanced Gastroesophageal Cancer: MSI and Beyond. Cancers 2021, 13, 1715. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Wang, N.; Ji, N.; Chen, Z.-S. Proteomics Technologies for Cancer Liquid Biopsies. Mol. Cancer 2022, 21, 53. [Google Scholar] [CrossRef]
- Bertok, T.; Bertokova, A.; Jane, E.; Hires, M.; Aguedo, J.; Potocarova, M.; Lukac, L.; Vikartovska, A.; Kasak, P.; Borsig, L.; et al. Identification of Whole-Serum Glycobiomarkers for Colorectal Carcinoma Using Reverse-Phase Lectin Microarray. Front Oncol. 2021, 11, 735338. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Wu, H.-C.; Kehm, R.; Santella, R.M.; Brenner, D.J.; Terry, M.B. DNA Repair Phenotype and Cancer Risk: A Systematic Review and Meta-Analysis of 55 Case–Control Studies. Sci. Rep. 2022, 12, 3405. [Google Scholar] [CrossRef]
- Grupińska, J.; Budzyń, M.; Brzeziński, J.; Gryszczyńska, B.; Kasprzak, M.; Kycler, W.; Leporowska, E.; Iskra, M. Association between Clinicopathological Features of Breast Cancer with Adipocytokine Levels and Oxidative Stress Markers before and after Chemotherapy. Biomed. Rep. 2021, 14, 30. [Google Scholar] [CrossRef] [PubMed]
- Chao, M.-R.; Evans, M.D.; Hu, C.-W.; Ji, Y.; Møller, P.; Rossner, P.; Cooke, M.S. Biomarkers of Nucleic Acid Oxidation—A Summary State-of-the-Art. Redox Biol. 2021, 42, 101872. [Google Scholar] [CrossRef]
- Pour Khavari, A.; Liu, Y.; He, E.; Skog, S.; Haghdoost, S. Serum 8-Oxo-DG as a Predictor of Sensitivity and Outcome of Radiotherapy and Chemotherapy of Upper Gastrointestinal Tumours. Oxidative Med. Cell. Longev. 2018, 2018, 4153574. [Google Scholar] [CrossRef]
- Mirjolet, C.; Merlin, J.L.; Truc, G.; Noël, G.; Thariat, J.; Domont, J.; Sargos, P.; Renard-Oldrini, S.; Ray-Coquard, I.; Liem, X.; et al. RILA Blood Biomarker as a Predictor of Radiation-Induced Sarcoma in a Matched Cohort Study. EBioMedicine 2019, 41, 420–426. [Google Scholar] [CrossRef] [Green Version]
- National Cancer InstituteTumor Markers in Common Use Was Originally Published by National Cancer Institute. Available online: https://www.cancer.gov/about-cancer/diagnosis-staging/diagnosis/tumor-markers-list (accessed on 22 February 2022).
- Zhang, H.; Lin, X.; Huang, Y.; Wang, M.; Cen, C.; Tang, S.; Dique, M.R.; Cai, L.; Luis, M.A.; Smollar, J.; et al. Detection Methods and Clinical Applications of Circulating Tumor Cells in Breast Cancer. Front. Oncol. 2021, 11, 652253. [Google Scholar] [CrossRef]
- Ren, X.; Foster, B.M.; Ghassemi, P.; Strobl, J.S.; Kerr, B.A.; Agah, M. Entrapment of Prostate Cancer Circulating Tumor Cells with a Sequential Size-Based Microfluidic Chip. Anal. Chem. 2018, 90, 7526–7534. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, R.; Zhang, L.; Guo, S. Nanomaterial-Based Immunocapture Platforms for the Recognition, Isolation, and Detection of Circulating Tumor Cells. Front. Bioeng. Biotechnol. 2022, 10, 850241. [Google Scholar] [CrossRef] [PubMed]
- List of Cleared or Approved Companion Diagnostic Devices (In Vitro and Imaging Tools). Available online: https://Www.Fda.Gov/Medical-Devices/in-Vitro-Diagnostics/List-Cleared-or-Approved-Companion-Diagnostic-Devices-in-Vitro-and-Imaging-Tools (accessed on 22 February 2022).
- Sammallahti, H.; Kokkola, A.; Rezasoltani, S.; Ghanbari, R.; Asadzadeh Aghdaei, H.; Knuutila, S.; Puolakkainen, P.; Sarhadi, V.K. Microbiota Alterations and Their Association with Oncogenomic Changes in Pancreatic Cancer Patients. Int. J. Mol. Sci. 2021, 22, 12978. [Google Scholar] [CrossRef]
- Youssef, O.; Lahti, L.; Kokkola, A.; Karla, T.; Tikkanen, M.; Ehsan, H.; Carpelan-Holmström, M.; Koskensalo, S.; Böhling, T.; Rautelin, H.; et al. Stool Microbiota Composition Differs in Patients with Stomach, Colon, and Rectal Neoplasms. Dig. Dis. Sci. 2018, 63, 2950–2958. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Patel, S.; Patel, P.; Tanavde, V. Saliva Based Liquid Biopsies in Head and Neck Cancer: How Far Are We from the Clinic? Front. Oncol. 2022, 12, 828434. [Google Scholar] [CrossRef]
- Gaw, G.; Gribben, M. Can We Detect Biomarkers of Oral Squamous Cell Carcinoma from Saliva or Mouth Swabs? Evid. Based Dent. 2022, 23, 32–33. [Google Scholar] [CrossRef] [PubMed]
- Elmahgoub, F. Could Salivary Biomarkers Be Useful in the Early Detection of Oral Cancer and Oral Potentially Malignant Disorders, and Is There a Relationship between These Biomarkers and Risk Factors? Evid.-Based Dent. 2022, 23, 30–31. [Google Scholar] [CrossRef] [PubMed]
- Mattox, A.K.; Fakhry, C.; Agrawal, N. Biomarker-Based Evaluation of Treatment Response and Surveillance of HPV-Associated Squamous Cell Carcinoma. Curr. Otorhinolaryngol. Rep. 2022, 10, 85–95. [Google Scholar] [CrossRef]
- Xu, R.; Rai, A.; Chen, M.; Suwakulsiri, W.; Greening, D.W.; Simpson, R.J. Extracellular Vesicles in Cancer—Implications for Future Improvements in Cancer Care. Nat. Rev. Clin. Oncol. 2018, 15, 617–638. [Google Scholar] [CrossRef]
- Allenson, K.; Castillo, J.; San Lucas, F.A.; Scelo, G.; Kim, D.U.; Bernard, V.; Davis, G.; Kumar, T.; Katz, M.; Overman, M.J.; et al. High prevalence of mutant KRAS in circulating exosome-derived DNA from early-stage pancreatic cancer patients. Ann Oncol. 2017, 28, 741–747. [Google Scholar] [CrossRef]
- Konoshenko, M.Y.; Lekchnov, E.A.; Vlassov, A.V.; Laktionov, P.P. Isolation of Extracellular Vesicles: General Methodologies and Latest Trends. BioMed Res. Int. 2018, 2018, 8545347. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-J.; Xie, G.-Y.; Miao, Y.-R.; Xia, M.; Wang, Y.; Lei, Q.; Zhang, Q.; Guo, A.-Y. EVAtlas: A Comprehensive Database for NcRNA Expression in Human Extracellular Vesicles. Nucleic Acids Res. 2022, 50, D111–D117. [Google Scholar] [CrossRef] [PubMed]
- Bayani, J.M.; Squire, J.A. Applications of SKY in Cancer Cytogenetics. Cancer Investig. 2002, 20, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Rydzewski, N.R.; Peterson, E.; Lang, J.M.; Yu, M.; Laura Chang, S.; Sjöström, M.; Bakhtiar, H.; Song, G.; Helzer, K.T.; Bootsma, M.L.; et al. Predicting Cancer Drug TARGETS-TreAtment Response Generalized Elastic-NeT Signatures. NPJ Genom. Med. 2021, 6, 76. [Google Scholar] [CrossRef]
- Nguyen, B.; Cusumano, P.G.; Deck, K.; Kerlin, D.; Garcia, A.A.; Barone, J.L.; Rivera, E.; Yao, K.; de Snoo, F.A.; van den Akker, J.; et al. Comparison of Molecular Subtyping with BluePrint, MammaPrint, and TargetPrint to Local Clinical Subtyping in Breast Cancer Patients. Ann. Surg. Oncol. 2012, 19, 3257–3263. [Google Scholar] [CrossRef]
- Arya, S.; Estrela, P. Recent Advances in Enhancement Strategies for Electrochemical ELISA-Based Immunoassays for Cancer Biomarker Detection. Sensors 2018, 18, 2010. [Google Scholar] [CrossRef] [Green Version]
- Dang, K.; Zhang, W.; Jiang, S.; Lin, X.; Qian, A. Application of Lectin Microarrays for Biomarker Discovery. ChemistryOpen 2020, 9, 285–300. [Google Scholar] [CrossRef]
- Kowalczyk, T.; Ciborowski, M.; Kisluk, J.; Kretowski, A.; Barbas, C. Mass Spectrometry Based Proteomics and Metabolomics in Personalized Oncology. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165690. [Google Scholar] [CrossRef]
- Coarfa, C.; Grimm, S.L.; Rajapakshe, K.; Perera, D.; Lu, H.-Y.; Wang, X.; Christensen, K.R.; Mo, Q.; Edwards, D.P.; Huang, S. Reverse-Phase Protein Array: Technology, Application, Data Processing, and Integration. J. Biomol. Tech. JBT 2021, 32, 15–29. [Google Scholar] [CrossRef]
- Hasan, M.R.; Ahommed, M.S.; Daizy, M.; Bacchu, M.S.; Ali, M.R.; Al-Mamun, M.R.; Saad Aly, M.A.; Khan, M.Z.H.; Hossain, S.I. Recent Development in Electrochemical Biosensors for Cancer Biomarkers Detection. Biosens. Bioelectron. X 2021, 8, 100075. [Google Scholar] [CrossRef]
- Jou, A.F.; Lu, C.-H.; Ou, Y.-C.; Wang, S.-S.; Hsu, S.-L.; Willner, I.; Ho, J.A. Diagnosing the MiR-141 Prostate Cancer Biomarker Using Nucleic Acid-Functionalized CdSe/ZnS QDs and Telomerase. Chem. Sci. 2015, 6, 659–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sina, A.A.I.; Carrascosa, L.G.; Liang, Z.; Grewal, Y.S.; Wardiana, A.; Shiddiky, M.J.A.; Gardiner, R.A.; Samaratunga, H.; Gandhi, M.K.; Scott, R.J.; et al. Epigenetically Reprogrammed Methylation Landscape Drives the DNA Self-Assembly and Serves as a Universal Cancer Biomarker. Nat. Commun. 2018, 9, 4915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, Y.; Gao, Y.; Tang, W.; Qiang, L.; Han, Y.; Gao, J.; Zhang, Y.; Liu, H.; Han, L. Attomolar-Level Ultrasensitive and Multiplex MicroRNA Detection Enabled by a Nanomaterial Locally Assembled Microfluidic Biochip for Cancer Diagnosis. Anal. Chem. 2021, 93, 5129–5136. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, Y.D.; Malsagova, K.A.; Popov, V.P.; Pleshakova, T.O.; Kozlov, A.F.; Galiullin, R.A.; Shumov, I.D.; Kapustina, S.I.; Tikhonenko, F.V.; Ziborov, V.S.; et al. Nanoribbon-Based Electronic Detection of a Glioma-Associated Circular MiRNA. Biosensors 2021, 11, 237. [Google Scholar] [CrossRef]
- Ivanov, Y.D.; Goldaeva, K.V.; Malsagova, K.A.; Pleshakova, T.O.; Galiullin, R.A.; Popov, V.P.; Kushlinskii, N.E.; Alferov, A.A.; Enikeev, D.V.; Potoldykova, N.V.; et al. Nanoribbon Biosensor in the Detection of MiRNAs Associated with Colorectal Cancer. Micromachines 2021, 12, 1581. [Google Scholar] [CrossRef]
- Li, C.; He, W.; Wang, N.; Xi, Z.; Deng, R.; Liu, X.; Kang, R.; Xie, L.; Liu, X. Application of Microfluidics in Detection of Circulating Tumor Cells. Front. Bioeng. Biotechnol. 2022, 10, 907232. [Google Scholar] [CrossRef]
- Malhotra, R.; Patel, V.; Chikkaveeraiah, B.V.; Munge, B.S.; Cheong, S.C.; Zain, R.B.; Abraham, M.T.; Dey, D.K.; Gutkind, J.S.; Rusling, J.F. Ultrasensitive Detection of Cancer Biomarkers in the Clinic by Use of a Nanostructured Microfluidic Array. Anal. Chem. 2012, 84, 6249–6255. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Bai, Y.; Cheng, Z.; Liu, F.; Wang, P.; Yang, D.; Li, G.; Jin, Q.; Mao, H.; Zhao, J. Absolute Quantification of DNA Methylation Using Microfluidic Chip-Based Digital PCR. Biosens. Bioelectron. 2017, 96, 339–344. [Google Scholar] [CrossRef]
- Bruch, R.; Baaske, J.; Chatelle, C.; Meirich, M.; Madlener, S.; Weber, W.; Dincer, C.; Urban, G.A. CRISPR/Cas13a-Powered Electrochemical Microfluidic Biosensor for Nucleic Acid Amplification-Free MiRNA Diagnostics. Adv. Mater. 2019, 31, 1905311. [Google Scholar] [CrossRef] [Green Version]
- Chi, Z.; Wu, Y.; Chen, L.; Yang, H.; Khan, M.R.; Busquets, R.; Huang, N.; Lin, X.; Deng, R.; Yang, W.; et al. CRISPR-Cas14a-Integrated Strand Displacement Amplification for Rapid and Isothermal Detection of Cholangiocarcinoma Associated Circulating MicroRNAs. Anal. Chim. Acta 2022, 1205, 339763. [Google Scholar] [CrossRef]
- Kwong, G.A.; Ghosh, S.; Gamboa, L.; Patriotis, C.; Srivastava, S.; Bhatia, S.N. Synthetic Biomarkers: A Twenty-First Century Path to Early Cancer Detection. Nat. Rev. Cancer 2021, 21, 655–668. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network National Comprehensive Cancer Network Compendium. Available online: https://www.nccn.org/compendia-templates/compendia/biomarkers-compendium (accessed on 22 February 2022).
- Food and Drug Administration Table of Pharmacogenomic Biomarkers in Drug Labeling. Available online: https://www.fda.gov/drugs/scienceresearch/researchareas/pharmacogenetics/ucm083378.htm (accessed on 22 February 2022).
- Dingerdissen, H.M.; Bastian, F.; Vijay-Shanker, K.; Robinson-Rechavi, M.; Bell, A.; Gogate, N.; Gupta, S.; Holmes, E.; Kahsay, R.; Keeney, J.; et al. OncoMX: A Knowledgebase for Exploring Cancer Biomarkers in the Context of Related Cancer and Healthy Data. JCO Clin. Cancer Inform. 2020, 4, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Nagel, Z.D.; Engelward, B.P.; Brenner, D.J.; Begley, T.J.; Sobol, R.W.; Bielas, J.H.; Stambrook, P.J.; Wei, Q.; Hu, J.J.; Terry, M.B.; et al. Towards Precision Prevention: Technologies for Identifying Healthy Individuals with High Risk of Disease. Mutat. Res. Fundam. Mol. Mech. Mutagenesis 2017, 800–802, 14–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haverfield, E.V.; Esplin, E.D.; Aguilar, S.J.; Hatchell, K.E.; Ormond, K.E.; Hanson-Kahn, A.; Atwal, P.S.; Macklin-Mantia, S.; Hines, S.; Sak, C.W.M.; et al. Physician-Directed Genetic Screening to Evaluate Personal Risk for Medically Actionable Disorders: A Large Multi-Center Cohort Study. BMC Med. 2021, 19, 199. [Google Scholar] [CrossRef]
- Turnbull, C.; Sud, A.; Houlston, R.S. Cancer Genetics, Precision Prevention and a Call to Action. Nat. Genet. 2018, 50, 1212–1218. [Google Scholar] [CrossRef]
- Louie, A.D.; Huntington, K.; Carlsen, L.; Zhou, L.; El-Deiry, W.S. Integrating Molecular Biomarker Inputs Into Development and Use of Clinical Cancer Therapeutics. Front. Pharmacol. 2021, 12, 2850. [Google Scholar] [CrossRef]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W.; Kemper, A.R.; et al. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1901–1913. [Google Scholar] [CrossRef]
- Kiebish, M.A.; Tekumalla, P.; Ravipaty, S.; Dobi, A.; Srivastava, S.; Wu, W.; Patil, S.; Friss, T.; Klotz, A.; Srinivasan, A.; et al. Clinical Utility of a Serum Biomarker Panel in Distinguishing Prostate Cancer from Benign Prostate Hyperplasia. Sci. Rep. 2021, 11, 15052. [Google Scholar] [CrossRef]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V.; Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Smith, D.; Richards, D.; et al. Sensitive and Specific Multi-Cancer Detection and Localization Using Methylation Signatures in Cell-Free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Lennon, A.M.; Buchanan, A.H.; Kinde, I.; Warren, A.; Honushefsky, A.; Cohain, A.T.; Ledbetter, D.H.; Sanfilippo, F.; Sheridan, K.; Rosica, D.; et al. Feasibility of Blood Testing Combined with PET-CT to Screen for Cancer and Guide Intervention. Science 2020, 369, eabb9601. [Google Scholar] [CrossRef]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and Localization of Surgically Resectable Cancers with a Multi-Analyte Blood Test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raoof, S.; Kennedy, C.J.; Wallach, D.A.; Bitton, A.; Green, R.C. Molecular Cancer Screening: In Search of Evidence. Nat. Med. 2021, 27, 1139–1142. [Google Scholar] [CrossRef] [PubMed]
- Hequet, D.; Harrissart, G.; Krief, D.; Maumy, L.; Lerebours, F.; Menet, E.; Callens, C.; Rouzier, R. Prosigna Test in Breast Cancer: Real-Life Experience. Breast Cancer Res. Treat. 2021, 188, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Piccart, M.; van’t Veer, L.J.; Poncet, C.; Lopes Cardozo, J.M.N.; Delaloge, S.; Pierga, J.-Y.; Vuylsteke, P.; Brain, E.; Vrijaldenhoven, S.; Neijenhuis, P.A.; et al. 70-Gene Signature as an Aid for Treatment Decisions in Early Breast Cancer: Updated Results of the Phase 3 Randomised MINDACT Trial with an Exploratory Analysis by Age. Lancet Oncol. 2021, 22, 476–488. [Google Scholar] [CrossRef]
- Herold, T.; Rothenberg-Thurley, M.; Grunwald, V.V.; Janke, H.; Goerlich, D.; Sauerland, M.C.; Konstandin, N.P.; Dufour, A.; Schneider, S.; Neusser, M.; et al. Validation and Refinement of the Revised 2017 European LeukemiaNet Genetic Risk Stratification of Acute Myeloid Leukemia. Leukemia 2020, 34, 3161–3172. [Google Scholar] [CrossRef] [Green Version]
- Inaba, H.; Mullighan, C.G. Pediatric Acute Lymphoblastic Leukemia. Haematologica 2020, 105, 2524–2539. [Google Scholar] [CrossRef]
- Batis, N.; Brooks, J.M.; Payne, K.; Sharma, N.; Nankivell, P.; Mehanna, H. Lack of Predictive Tools for Conventional and Targeted Cancer Therapy: Barriers to Biomarker Development and Clinical Translation. Adv. Drug Deliv. Rev. 2021, 176, 113854. [Google Scholar] [CrossRef]
- Gerhards, N.M.; Rottenberg, S. New Tools for Old Drugs: Functional Genetic Screens to Optimize Current Chemotherapy. Drug Resist. Updates 2018, 36, 30. [Google Scholar] [CrossRef]
- Miteva-Marcheva, N.N.; Ivanov, H.Y.; Dimitrov, D.K.; Stoyanova, V.K. Application of Pharmacogenetics in Oncology. Biomark. Res. 2020, 8, 32. [Google Scholar] [CrossRef]
- Whirl-Carrillo, M.; Huddart, R.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Whaley, R.; Klein, T.E. An Evidence-Based Framework for Evaluating Pharmacogenomics Knowledge for Personalized Medicine. Clin. Pharmacol. Ther. 2021, 110, 563–572. [Google Scholar] [CrossRef]
- Syed, Y.Y. Oncotype DX Breast Recurrence Score®: A Review of Its Use in Early-Stage Breast Cancer. Mol. Diagn. Ther. 2020, 24, 621–632. [Google Scholar] [CrossRef] [PubMed]
- Schaafsma, E.; Zhang, B.; Schaafsma, M.; Tong, C.-Y.; Zhang, L.; Cheng, C. Impact of Oncotype DX Testing on ER+ Breast Cancer Treatment and Survival in the First Decade of Use. Breast Cancer Res. 2021, 23, 74. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann. Surg. Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef] [PubMed]
- Averbeck, D.; Candéias, S.; Chandna, S.; Foray, N.; Friedl, A.A.; Haghdoost, S.; Jeggo, P.A.; Lumniczky, K.; Paris, F.; Quintens, R.; et al. Establishing Mechanisms Affecting the Individual Response to Ionizing Radiation. Int. J. Radiat. Biol. 2020, 96, 297–323. [Google Scholar] [CrossRef] [Green Version]
- Boelens, M.C.; Wu, T.J.; Nabet, B.Y.; Xu, B.; Qiu, Y.; Yoon, T.; Azzam, D.J.; Twyman-Saint Victor, C.; Wiemann, B.Z.; Ishwaran, H.; et al. Exosome Transfer from Stromal to Breast Cancer Cells Regulates Therapy Resistance Pathways. Cell 2014, 159, 499–513. [Google Scholar] [CrossRef] [Green Version]
- Meehan, J.; Gray, M.; Martínez-Pérez, C.; Kay, C.; Pang, L.Y.; Fraser, J.A.; Poole, A.V.; Kunkler, I.H.; Langdon, S.P.; Argyle, D.; et al. Precision Medicine and the Role of Biomarkers of Radiotherapy Response in Breast Cancer. Front. Oncol. 2020, 10, 628. [Google Scholar] [CrossRef]
- Goodman, C.R.; Seagle, B.-L.L.; Friedl, T.W.P.; Rack, B.; Lato, K.; Fink, V.; Cristofanilli, M.; Donnelly, E.D.; Janni, W.; Shahabi, S.; et al. Association of Circulating Tumor Cell Status with Benefit of Radiotherapy and Survival in Early-Stage Breast Cancer. JAMA Oncol. 2018, 4, e180163. [Google Scholar] [CrossRef] [Green Version]
- Veldwijk, M.R.; Seibold, P.; Botma, A.; Helmbold, I.; Sperk, E.; Giordano, F.A.; Gürth, N.; Kirchner, A.; Behrens, S.; Wenz, F.; et al. Association of CD4+ Radiation-Induced Lymphocyte Apoptosis with Fibrosis and Telangiectasia after Radiotherapy in 272 Breast Cancer Patients with >10-Year Follow-Up. Clin. Cancer Res. 2019, 25, 562–572. [Google Scholar] [CrossRef] [Green Version]
- Benitez, C.M.; Knox, S.J. Harnessing Genome-Wide Association Studies to Minimize Adverse Radiation-Induced Side Effects. Radiat. Oncol. J. 2020, 38, 226. [Google Scholar] [CrossRef]
- Chalubinska-Fendler, J.; Graczyk, L.; Piotrowski, G.; Wyka, K.; Nowicka, Z.; Tomasik, B.; Fijuth, J.; Kozono, D.; Fendler, W. Lipopolysaccharide-Binding Protein Is an Early Biomarker of Cardiac Function After Radiation Therapy for Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1074–1083. [Google Scholar] [CrossRef]
- Scheerens, H.; Malong, A.; Bassett, K.; Boyd, Z.; Gupta, V.; Harris, J.; Mesick, C.; Simnett, S.; Stevens, H.; Gilbert, H.; et al. Current Status of Companion and Complementary Diagnostics: Strategic Considerations for Development and Launch. Clin. Transl. Sci. 2017, 10, 84–92. [Google Scholar] [CrossRef]
- Bradley, R.; Braybrooke, J.; Gray, R.; Hills, R.; Liu, Z.; Peto, R.; Davies, L.; Dodwell, D.; McGale, P.; Pan, H.; et al. Trastuzumab for Early-Stage, HER2-Positive Breast Cancer: A Meta-Analysis of 13,864 Women in Seven Randomised Trials. Lancet Oncol. 2021, 22, 1139–1150. [Google Scholar] [CrossRef]
- Coleman, R.L.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.; Scambia, G.; et al. Rucaparib Maintenance Treatment for Recurrent Ovarian Carcinoma after Response to Platinum Therapy (ARIEL3): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet 2017, 390, 1949. [Google Scholar] [CrossRef] [Green Version]
- Lei, Y.; Li, X.; Huang, Q.; Zheng, X.; Liu, M. Progress and Challenges of Predictive Biomarkers for Immune Checkpoint Blockade. Front. Oncol. 2021, 11, 609. [Google Scholar] [CrossRef]
- Wang, Y.; Tong, Z.; Zhang, W.; Zhang, W.; Buzdin, A.; Mu, X.; Yan, Q.; Zhao, X.; Chang, H.H.; Duhon, M.; et al. FDA-Approved and Emerging Next Generation Predictive Biomarkers for Immune Checkpoint Inhibitors in Cancer Patients. Front. Oncol. 2021, 11, 2115. [Google Scholar] [CrossRef] [PubMed]
- Kilgour, E.; Rothwell, D.G.; Brady, G.; Dive, C. Liquid Biopsy-Based Biomarkers of Treatment Response and Resistance. Cancer Cell 2020, 37, 485–495. [Google Scholar] [CrossRef]
- de Kock, R.; van den Borne, B.; Youssef-El Soud, M.; Belderbos, H.; Stege, G.; de Saegher, M.; van Dongen-Schrover, C.; Genet, S.; Brunsveld, L.; Scharnhorst, V.; et al. Circulating Biomarkers for Monitoring Therapy Response and Detection of Disease Progression in Lung Cancer Patients. Cancer Treat. Res. Commun. 2021, 28, 100410. [Google Scholar] [CrossRef] [PubMed]
- Heidrich, I.; Ačkar, L.; Mossahebi Mohammadi, P.; Pantel, K. Liquid Biopsies: Potential and Challenges. Int. J. Cancer 2021, 148, 528–545. [Google Scholar] [CrossRef] [PubMed]
- Goossens, N.; Nakagawa, S.; Sun, X.; Hoshida, Y. Cancer Biomarker Discovery and Validation. Transl. Cancer Res. 2015, 4, 256–269. [Google Scholar] [CrossRef]
- Gion, M.; Trevisiol, C.; Fabricio, A.S.C. State of the Art and Trends of Circulating Cancer Biomarkers. Int. J. Biol. Markers 2020, 35, 12–15. [Google Scholar] [CrossRef]
- Hayes, D.F. Biomarker Validation and Testing. Mol. Oncol. 2015, 9, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Ou, F.S.; Michiels, S.; Shyr, Y.; Adjei, A.A.; Oberg, A.L. Biomarker Discovery and Validation: Statistical Considerations. J. Thorac. Oncol. 2021, 16, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Simon, R. Clinical Trials for Predictive Medicine: New Challenges and Paradigms. Clin. Trials 2010, 7, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, K.; Yu, Q.; Shen, R.; Sun, S.-Y.; Moreno, C.S.; Li, X.; Qin, Z.S. Pan-Cancer Analysis of Pathway-Based Gene Expression Pattern at the Individual Level Reveals Biomarkers of Clinical Prognosis. Cell Rep. Methods 2021, 1, 100050. [Google Scholar] [CrossRef]
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and Other Tools) Resource; Food and Drug Administration: Silver Spring, MD, USA, 2016.
- O’Connor, J.P.B.; Aboagye, E.O.; Adams, J.E.; Aerts, H.J.W.L.; Barrington, S.F.; Beer, A.J.; Boellaard, R.; Bohndiek, S.E.; Brady, M.; Brown, G.; et al. Imaging Biomarker Roadmap for Cancer Studies. Nat. Rev. Clin. Oncol. 2017, 14, 169–186. [Google Scholar] [CrossRef]
- Saah, A.J.; Hoover, D.R. “Sensitivity” and “Specificity” Reconsidered: The Meaning of These Terms in Analytical and Diagnostic Settings. Ann. Intern. Med. 1997, 126, 91–94. [Google Scholar] [CrossRef]
- Hayes, D.F. Defining Clinical Utility of Tumor Biomarker Tests: A Clinician’s Viewpoint. J. Clin. Oncol. 2021, 39, 238–248. [Google Scholar] [CrossRef]
- Henry, N.L.; Hayes, D.F. Cancer Biomarkers. Mol. Oncol. 2012, 6, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Ray, P.; Manach, Y.; Riou, B.; Houle, T.T. Statistical Evaluation of a Biomarker. Anesthesiology 2010, 112, 1023–1040. [Google Scholar] [CrossRef] [Green Version]
- Brower, V. Biomarkers: Portents of Malignancy. Nature 2011, 471, S19–S20. [Google Scholar] [CrossRef]
- Parker, J.L.; Kuzulugil, S.S.; Pereverzev, K.; Mac, S.; Lopes, G.; Shah, Z.; Weerasinghe, A.; Rubinger, D.; Falconi, A.; Bener, A.; et al. Does Biomarker Use in Oncology Improve Clinical Trial Failure Risk? A Large-Scale Analysis. Cancer Med. 2021, 10, 1955–1963. [Google Scholar] [CrossRef] [PubMed]
- Hayes, D.F. Precision Medicine and Testing for Tumor Biomarkers-Are All Tests Born Equal? JAMA Oncol. 2018, 4, 773–774. [Google Scholar] [CrossRef] [PubMed]
- Poste, G. Bring on the Biomarkers. Nature 2011, 469, 156–157. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| miRNA | Sample | Cancer | Application | Reference |
|---|---|---|---|---|
| Predictive markers of drug response | ||||
| miR-494-3p | Plasma EVs | NSCLC | Resistance to osimertinib | Kaźmierczak et al., 2022 [30] |
| miR-323-3p, miR-1468-3p, miR-5189-5p and miR-6513-5p | Plasma EVs | NSCLC | Resistance to osimertinib | Janpipatkul et al., 2021 [31] |
| miR-184, miR-3913-5p | Serum EVs | NSCLC | Resistance to osimertinib | Li et al., 2021 [32] |
| miR-21 | Plasma ctRNA | EGFR mutated NSCLC | Response to EGFR_TKIs | Leonetti et al., 2021 [33] |
| miR-125b-5p | Serum EVs | NSCLC | Predictive of chemotherapy response | Zhang et al., 2020 [34] |
| miR-620 | Serum EVs | NSCLC | Predictive of chemotherapy response/Diagnosis | Tang et al., 2020 [35] |
| miR-30b, miR-328, and miR-423 | Plasma EVs | Breast Cancer | Predictive of chemotherapy response | Todorova et al., 2022 [36] |
| miR-30a | Serum EVs | Oral Cancer | Diagnostic, prognostic, cisplatin-resistance | Kulkarni et al., 2020 [37] |
| Predictive markers of response to immunotherapy | ||||
| miR-625-5p | Plasma EVs | NSCLC | Overall survival after immune checkpoint inhibitor treatment | Pantano et al.2022 [38] |
| miR-4649-3p, miR-615-3p, and miR-1234-3p | Plasma EVs | Melanoma | Response/prognosis after immune checkpoint inhibitor treatment | Bustos et al., 2020 [39] |
| Predictive markers of response to radiotherapy | ||||
| miR-92a-3p | Plasma EVs | NSCLC | Resistance to radiotherapy (upregulation) | Zeng et al., 2022 [40] |
| miR-96 | Plasma EVs | NSCLC | Radioresistant | Zheng et al., 2021 [41] |
| Diagnostic/prognostic markers | ||||
| * (Let-7b-5p and miR-22-3p and miR-184) | Plasma EVs | NSCLC | Diagnostic | Vadla et al., 2022 [42] |
| miR-125b-5p and miR-5684 | Serum EVs | NSCLC | Diagnostic | Zhang et al., 2020 [34] |
| miR-378 | Serum EVs | NSCLC | Prognostic/monitoring | Zhang et al., 2020 [43] |
| miR-382 | Serum EVs | NSCLC | Prognostic | Luo et al., 2021 [44] |
| miR-1260b | Plasma EVs | NSCLC | Prognostic | Kim et al., 2021 [45] |
| miR-486-5p and miR-146a-5p | Serum EVs | NSCLC | Diagnostic | Wu et al., 2020 [28] |
| miR-1246 | Serum EVs | NSCLC | Diagnostic and prognostic | Huang et al., 2020 [46] |
| miR-1246 and miR-96 | Plasma EVs | NSCLC | Diagnostic | Zheng et al., 2021 [41] |
| * (miR-206, miR-24, miR-1246, and miR-373) | Plasma EVs | Breast cancer | Diagnostic, combination 98% accuracy | Jang et al., 2021 [47] |
| miR-148a | Serum EVs | Breast cancer | Prognosis | Li et al., 2020 [48] |
| miR-138-5p | Serum EVs | Breast cancer | Prognosis | Xun et al. (2021) [49] |
| miR-363-5p | Plasma EVs | Breast cancer | Prognostic | Wang X et al., 2021 [50] |
| miR-1910-3p | Serum EVs | Breast cancer | Diagnostic (with CA153) | Wang B et al. (2020) [51] |
| miR-17-5p | Serum EVs | Breast cancer | Prognostic | Sueta et al., 2017 [52] |
| miR-423, miR-424, let7-i, and miR-660 | Urine EVs | Breast cancer | Diagnostic | Hirschfeld et al., 2020 [53] |
| miR-21-5p | Plasma EVs | Breast cancer | Diagnostic | Liu et al., 2021 [54] |
| miR-3662, miR-146a, and miR-1290 | Serum EVs | Breast cancer | Diagnostic | Li et al., 2021 [55] |
| miR-423-3p | Plasma EVs | Prostate cancer | Predictive of castration-resistance | Guo et al., 2021 [56] |
| miR-532-5p | Urine EVs | Prostate cancer | Prognostic | Kim et al., 2021 [57] |
| miR-425-5p | Plasma EVs | Prostate cancer | Diagnostic of metastatic prostate cancer | Rode et al., 2021 [58] |
| miR-16-5p, miR-451a, miR-142-3p, miR-21-5p, and miR-636 | Urine EVs | Prostate cancer | Prognostic | Shin et al., 2021 [59] |
| miR-125a-5p and miR-141-5p | Plasma EVs | Prostate cancer | Diagnostic | Li et al., 2020 [60] |
| miR-375 and miR-451a | Urine EVs | Prostate cancer | Diagnostic | Li et al., 2021 [61] |
| iR-24-3p | Saliva EVs | Oral cancer | Diagnostic | He et al., 2020 [62] |
| miR-130a | Plasma EVs | Oral cancer | Diagnostic and prognostic | He et al., 2021 [63] |
| miR-126, miR-155, and miR-21 | Serum EVs | Oral cancer | Diagnostic and prognostic | Chen et al., 2021 [64] |
| Let7, miR-16, and miR-23 | Serum EVs | CRC | Diagnostic | Dohmen et al., 2022 [27] |
| miR-139-3p | Plasma EVs | CRC | Diagnosis | Li et al., 2020 [65] |
| miR-126, miR-1290, miR-23a, and miR-940 | Serum EVs | CRC | Diagnostic | Shi et al., 2021 [66] |
| miR-4323, miR-4284, miR-1290, and miR-1246 | Serum EVs | CRC | Diagnostic | Handa et al., 2021 [67] |
| miR-106b-3p | Serum EVs | CRC | Diagnostic and prognostic | Liu et al., 2020 [68] |
| miR-874 | Serum EVs | CRC | Diagnostic and prognostic | Zhang et al. (2020) [69] |
| let-7g and miR-193a | Plasma EVs | CRC | Diagnostic and prognostic | Cho et al. (2021) [70] |
| miR-122 | Serum EVs | CRC | Diagnostic of metastatic CRC (liver) | Sun et al., 2020 [26] |
| miR-375 | Plasma | Esophageal adenocarcinoma | Prognostic, Overall survival | van Zweeden et al.2021 [71] |
| miR-17-5p, miR-25-3p, miR-27a, miR-27b, miR-191, miR-199a-5p, miR-211, miR-300, miR-542-3p, miR-586, miR-663a | Plasma/serum | Osteosarcoma | Diagnostic (Higher expression of individual miRNAs) | Meta-analysis by Gao et al., 2020 [72] |
| miR-34a, miR-101, miR-124, miR-125b, miR-139-5p, miR-144, miR-148a, miR-152, miR-194, miR-195, miR-222, miR-223, miR-326, miR-375, miR-491-5p | Plasma/serum | Osteosarcoma | Diagnostic (Lower expression of individual miRNAs) | Meta-analysis by Gao et al., 2020 [72] |
| * (miR-21, miR-199a-3p, miR-143) | Plasma/serum | Osteosarcoma | Diagnostic (Higher expression, miRNA group) | Meta-analysis by Gao et al., 2020 [72] |
| * (miR-199b-5p/miR-124); (miR-195-5p, miR-199a-3p, miR-320a, miR-374a-5p); (miR-586, miR-223) | Plasma/serum | Osteosarcoma | Diagnostic (Lower expression, miRNA group) | Meta-analysis by Gao et al., 2020 [72] |
| miR-21 | Plasma | Diffuse large B-cell lymphoma | Diagnostic (upregulation) | Meta-analysis Lopez-Santillan et al., 2018 [73] |
| miR-92a and miR-638 | Plasma | Acute lymphoblastic leukemia | Diagnostic | Fayed et al., 2021 [74] |
| miR-23b-3p | Plasma | Hepatocellular carcinoma | Diagnostic (downregulation) | Manganelli et al., 2021 [75] |
| Top differentially expressed miRNAs in plasma EVs of cancer patients | Compiled from the EVmiRNA database (http://bioinfo.life.hust.edu.cn/EVmiRNA, accessed on 20 June 2022) (Liu et al., 2019) [76] | |||
| miR-17-5p, miR-3960, miR-4488 | Plasma Exo | Breast adenocarcinoma | Diagnostic | |
| miR-3168, miR-3178, miR-425-3p | Plasma EVs | Breast adenocarcinoma | Diagnostic | |
| miR-10a-3p, miR-10a-5p, miR-1290, miR-141-3p, miR-183-5p, miR-191-5p, miR-192-5p, miR-194-5p, miR-182-5p, miR-19b-3p, miR-200a-5p, miR-200b-3p, miR-215-5p, miR-19a-3p, miR-429 | Plasma Exo | CRC | Diagnostic | |
| miR-1224-5p, miR-451a | Plasma EVs | CRC | Diagnostic | |
| let-7f-5p, let-7g-5p, miR-106b-3p, miR-1246, miR-1260b, miR-1290, miR-146a-5p, miR-155-5p, miR-16-2-3p, miR-17-5p, miR-181a-2-3p, miR-20a-5p, miR-30e-3p, miR-339-5p, miR-4488. | Plasma Exo | Chronic lymphocytic leukemia | Diagnostic | |
| miR-126-5p, miR-182-5p, miR-183-5p | Plasma EVs | Chronic lymphocytic leukemia | Diagnostic | |
| miR-103a-3p, miR-106b-3p, miR-10b-5p, miR-1307-5p, miR-130b-3p, miR-142-5p, miR-181a-3p, miR-186-5p, miR-191-5p, miR-25-3p, miR-423-3p, miR-4767, miR-877-5p, miR-92a-3p, miR-92b-3p | Plasma Exo | Lymphoma | Diagnostic | |
| miR-151a-5p, miR-3195, miR-3960, miR-4792, miR-7641, miR-7704. | Plasma Exo | Oral cancer | Diagnostic | |
| miR-1224-5p, miR-9-5p | Plasma Exo | Prostate cancer | Diagnostic | |
| miR-1224-5p, miR-9-5p | Plasma EVs | Prostate cancer | Diagnostic |
| Biomarker | Cancer | Application | Tumor Tissue/Bone Marrow | Blood | Urine | Stool | Cerebrospinal Fluid | Saliva/Buccal Swab |
|---|---|---|---|---|---|---|---|---|
| ALK gene rearrangements and overexpression | NSCLC, anaplastic large cell lymphoma, and histiocytosis | To help determine treatment and prognosis | X | |||||
| Alpha-fetoprotein (AFP) | Liver cancer and germ cell tumors | To help diagnose liver cancer and follow response to treatment; to assess stage, prognosis, and response to treatment of germ cell tumors | X | |||||
| B-cell immunoglobulin gene rearrangement | B-cell lymphoma | To help in diagnosis, to evaluate effectiveness of treatment, and to check for recurrence | X | X | ||||
| BCL2 gene rearrangement | Lymphomas and leukemias | For diagnosis and planning therapy | X | X | ||||
| BCR–ABL fusion gene | Chronic myeloid leukemia, acute lymphoblastic leukemia, and acute myelogenous leukemia | To confirm diagnosis, predict response to targeted therapy, help determine treatment, and monitor disease status | X | X | ||||
| Beta-2-microglobulin (B2M) | Multiple myeloma, chronic lymphocytic leukemia, and some lymphomas | To determine prognosis and follow response to treatment | X | X | X | |||
| Beta-human chorionic gonadotropin (Beta-hCG) | Choriocarcinoma and germ cell tumors | To assess stage, prognosis, and response to treatment | X | X | ||||
| Bladder Tumor Antigen (BTA) | Bladder cancer and cancer of the kidney or ureter | As surveillance with cytology and cystoscopy of patients already known to have bladder cancer | X | |||||
| BRAF gene V600 mutations | Cutaneous melanoma, Erdheim–Chester disease, Langerhans cell histiocytosis, CRC, and NSCLC | To help determine treatment | X | |||||
| BRCA1 and BRCA2 gene mutations | Ovarian and breast cancers | To help determine treatment | X | X | ||||
| CA15-3/CA27.29 | Breast cancer | To assess whether treatment is working or if cancer has recurred | X | |||||
| CA19-9 | Pancreatic, gallbladder, bile duct, and gastric cancers | To assess whether treatment is working | X | |||||
| CA-125 | Ovarian cancer | To help in diagnosis, assessment of response to treatment, and evaluation of recurrence | X | |||||
| CA27.29 | Breast cancer | To detect metastasis or recurrence | X | |||||
| Calcitonin | Medullary thyroid cancer | To help in diagnosis, check whether treatment is working, and assess recurrence | X | |||||
| Carcinoembryonic antigen (CEA) | CRC and some other cancers | To monitor the effectiveness of treatment and to detect recurrence or spread | X | |||||
| CD19 | B-cell lymphomas and leukemias | To help in diagnosis and to help determine treatment | X | X | ||||
| CD20 | Non-Hodgkin lymphoma | To help determine treatment | X | |||||
| CD22 | B-cell lymphomas and leukemias | To help in diagnosis and to help determine treatment | X | X | ||||
| CD25 | Non-Hodgkin (T-cell) lymphoma | To help determine treatment | X | |||||
| CD30 | Classic Hodgkin lymphoma, and B-cell and T-cell lymphomas | To help determine treatment | X | |||||
| CD33 | Acute myeloid leukemia | To help determine treatment | X | |||||
| Chromogranin A (CgA) | Neuroendocrine tumors | To help in diagnosis, assessment of treatment response, and evaluation of recurrence | X | |||||
| Chromosome 17p deletion | Chronic lymphocytic leukemia | To help determine treatment | X | |||||
| Chromosomes 3, 7, 17, and 9p21 | Bladder cancer | To help in monitoring for tumor recurrence | X | |||||
| Circulating tumor cells of epithelial origin (CELLSEARCH) | Metastatic breast, prostate, and CRC | To inform clinical decision-making, and to assess prognosis | X | |||||
| C-kit/CD117 | Gastrointestinal stromal tumor, mucosal melanoma, acute myeloid leukemia, and mast cell disease | To help in diagnosis and to help determine treatment | X | X | ||||
| Cyclin D1 (CCND1) gene rearrangement or expression | Lymphoma and myeloma | To help in diagnosis | X | |||||
| Cytokeratin fragment 21-1 | Lung cancer | To help in monitoring for recurrence | X | |||||
| Des-gamma-carboxy prothrombin (DCP) | Hepatocellular carcinoma | To monitor the effectiveness of treatment and to detect recurrence | X | |||||
| DPD gene mutation | Breast, CRC, gastric, and pancreatic cancers | To predict the risk of a toxic reaction to 5-fluorouracil therapy | X | |||||
| EGFR gene mutation | NSCLC | To help determine treatment and prognosis | X | |||||
| Estrogen receptor (ER)/progesterone receptor (PR) | Breast cancer | To help determine treatment | X | |||||
| FGFR2 and FGFR3 gene mutations | Bladder cancer | To help determine treatment | X | |||||
| Fibrin/fibrinogen | Bladder cancer | To monitor progression and response to treatment | X | |||||
| FLT3 gene mutations | Acute myeloid leukemia | To help determine treatment | X | |||||
| FoundationOne CDx (F1CDx) genomic test | Any solid tumor | As a companion diagnostic test to determine treatment | X | X | ||||
| Gastrin | Gastrin-producing tumor (gastrinoma) | To help in diagnosis, monitor the effectiveness of treatment, and detect recurrence | X | |||||
| Guardant360 CDx genomic test | Any solid tumor | As a companion diagnostic test to determine treatment and for general tumor mutation profiling | X | |||||
| HE4 | Ovarian cancer | To plan cancer treatment, assess disease progression, and monitor for recurrence | X | |||||
| HER2/neu gene amplification or protein overexpression | Breast, ovarian, bladder, pancreatic, and stomach cancers | To help determine treatment | X | |||||
| 5-HIAA | Carcinoid tumors | To help in diagnosis and to monitor disease | X | |||||
| IDH1 and IDH2 gene mutations | Acute myeloid leukemia | To help determine treatment | X | X | ||||
| Immunoglobulins | Multiple myeloma and Waldenström macroglobulinemia | To help diagnose disease, assess response to treatment, and look for recurrence | X | X | ||||
| IRF4 gene rearrangement | Lymphoma | To help in diagnosis | X | |||||
| JAK2 gene mutation | Certain types of leukemia | To help in diagnosis | X | X | ||||
| KRAS gene mutation | CRC and NSCLC | To help determine treatment | X | |||||
| Lactate dehydrogenase | Germ cell tumors, lymphoma, leukemia, melanoma, and neuroblastoma | To assess stage, prognosis, and response to treatment | X | |||||
| Mammaprint test (70-gene signature) | Breast cancer | To evaluate risk of recurrence | X | |||||
| Microsatellite instability (MSI) and/or deficient mismatch repair (dMMR) | CRC and other solid tumors | To guide treatment and to identify those at high risk of certain cancer-predisposing syndromes | X | |||||
| MYC gene expression | Lymphomas and leukemias | To help in diagnosis and to help determine treatment | X | |||||
| MYD88 gene mutation | Lymphoma and Waldenström macroglobulinemia | To help in diagnosis and to help determine treatment | X | |||||
| Myeloperoxidase (MPO) | Leukemia | To help in diagnosis | X | |||||
| Neuron-specific enolase (NSE) | Small cell lung cancer and neuroblastoma | To help in diagnosis and to assess response to treatment | X | |||||
| NTRK gene fusion | Any solid tumor | To help determine treatment | X | |||||
| Nuclear matrix protein 22 | Bladder cancer | To monitor response to treatment | X | |||||
| Oncotype DX Breast Recurrence Score test (21-gene signature) | Breast cancer | To evaluate risk of distant recurrence and to help plan treatment | X | |||||
| Oncotype DX Genomic Prostate Score test (17-gene signature) | Prostate cancer | To predict the aggressiveness of prostate cancer and to help manage treatment | X | |||||
| OVA1 test (5-protein signature) | Ovarian cancer | To pre-operatively assess pelvic mass for suspected ovarian cancer | X | |||||
| PCA3 mRNA | Prostate cancer | To determine need for repeating biopsy after a negative biopsy | X | |||||
| PML/RARα fusion gene | Acute promyelocytic leukemia | To diagnose, to predict response to all-trans-retinoic acid or arsenic trioxide therapy, to assess effectiveness of therapy, monitor minimal residual disease, and predict early relapse | X | X | ||||
| Programmed death ligand 1 (PD-L1) | NSCLC, liver cancer, stomach cancer, gastroesophageal junction cancer, classical Hodgkin lymphoma, and other aggressive lymphoma subtypes | To help determine treatment | X | |||||
| Prolaris test (46-gene signature) | Prostate cancer | To predict the aggressiveness of prostate cancer and to help manage treatment | X | |||||
| Prostate-specific antigen (PSA) | Prostate cancer | To help in diagnosis, to assess response to treatment, and to look for recurrence | X | |||||
| Prostatic Acid Phosphatase (PAP) | Metastatic prostate cancer | To help in diagnosing poorly differentiated carcinomas | X | |||||
| ROS1 gene rearrangement | NSCLC | To help determine treatment | X | |||||
| Soluble mesothelin-related peptides (SMRP) | Mesothelioma | To monitor progression or recurrence | X | |||||
| Somatostatin receptor | Neuroendocrine tumors affecting the pancreas or gastrointestinal tract | To help determine treatment | X | |||||
| T-cell receptor gene rearrangement | T-cell lymphoma | To help in diagnosis; sometimes to detect and evaluate residual disease | X | X | ||||
| Terminal transferase (TdT) | Leukemia and lymphoma | To help in diagnosis | X | X | ||||
| Thiopurine S-methyltransferase (TPMT) enzyme activity or TPMT genetic test | Acute lymphoblastic leukemia | To predict the risk of severe bone marrow toxicity (myelosuppression) with thiopurine treatment | X | X | ||||
| Thyroglobulin | Thyroid cancer | To evaluate response to treatment and to look for recurrence | x | |||||
| UGT1A1*28 variant homozygosity | CRC | To predict toxicity from irinotecan therapy | X | X | ||||
| Urine catecholamines: VMA and HVA | Neuroblastoma | To help in diagnosis | X | |||||
| Urokinase plasminogen activator (uPA) and plasminogen activator inhibitor (PAI-1) | Breast cancer | To determine the aggressiveness of cancer and guide treatment | X | |||||
| DNA methylation markers based on References [16,17] | ||||||||
| Methylation of MGMT promoter | Glioblastoma | Drug response to chemotherapy | X | |||||
| Methylation of MLH1 | Lynch syndrome | Treatment decision | X | |||||
| Methylation of NDRG4 and BMP3 | Colorectal Cancer | Diagnostic | X | |||||
| Methylation of SEPT9 promoter | Colorectal Cancer | Diagnostic | X |
| Technology | Applications | Advantages | Disadvantages |
|---|---|---|---|
| FISH | Detection of chromosomal abnormalities | Cell-based genetic results, specificity, simplicity, and reliability | Unable to detect sequence mutations |
| PCR/real-time PCR/digital PCR | Detection of targeted sequence mutations, gene fusions, or DNA methylation | High sensitivity and specificity, simplicity, good reproducibility, suitable in a clinical setting, and low cost | Restricted to targeted mutations and limited throughput |
| NGS | Detection of somatic and germline alterations in a large number of genes | High-throughput tool; can be targeted or genome-wide, and can detect different types of genetic alterations at the same time | Results depend on the platform. Difficult to interpret the significance of low-frequency variants. Genome-wide approaches require bioinformatic analysis. Site-specific testing for clinical applications |
| Flow cytometry | Cell count and identification, DNA quantification | High sensitivity and rapid analysis | Restricted to specific parameters |
| Gene expression microarrays | Differences in gene expression between tumor subtypes or between tumor and normal tissue or in tumor tissue before and after treatment, etc. | High-throughput tool | Bioinformatic analysis is required. Not all targets are identified |
| IHC | Detection of protein expression | Localization of protein expression in the tumor tissue | Restricted to proteins with available antibodies. Subjective interpretation |
| ELISA | Detection of protein expression, primarily in body fluids | Easy procedure and quantitative | Restricted to proteins with available antibodies. Limited detection sensitivity in body fluids |
| Lectin microarrays | Glycomic profiling | Can be useful in tumor tissues and body fluids, high-throughput tool, high sensitivity, and rapid analysis | Inconsistencies due to variation between batches and between purification procedures |
| MS | Protein profiling of tumor tissues or body fluids | Can be used for targeted assays or biomarker discovery, and highly multiplex | Procedure complexity, low sensitivity, and throughput |
| RPPA | Targeted detection of protein levels | High reproducibility, high throughput, and lower cost than MS | Need for special devices, restricted to proteins with validated antibodies |
| Biosensors/nanotechnology | Detection of low concentration biomarkers primarily in body fluids | High sensitivity and specificity, and ease of use | Low stability, poor reproducibility, problems in miniaturizing devices, and low performance in human whole blood samples |
| Microfluidics | Detection of low concentration biomarkers primarily in body fluids | High sensitivity, high throughput, cost-effective tool, and can be combined with biosensors | Needs improvement in accuracy and efficiency |
| CRISPR-based ctDNA/RNA detection | Detection of low concentration biomarkers primarily in body fluids | High sensitivity and specificity; can be combined with biosensors | Complicated multi-step procedure; lack of high-throughput design |
| Synthetic biomarker technology | Sensing of dysregulated activity of tumor cells or tumor microenvironment | Molecular amplification of tumor biomarker | Significant noise from off-target activity; need for better knowledge on early stage cancer pathogenesis |
| Term | Definition |
|---|---|
| Analytical Sensitivity | The smallest concentration of a substance in a biological specimen that can be reliably measured by an analytical procedure |
| Analytical Specificity | The ability of an assay to measure the specific substance (intended target), rather than others, in a biological specimen |
| Analytical Accuracy | The closeness of agreement between the value which is accepted either as a conventional true value or an accepted reference value and the value found. Usually, there is a comparison with another measurement technique |
| Analytical Repeatability | A measure of the extent to which a test conducted multiple times on the same subject, in the same laboratory, using the same equipment, by the same operator, over a short period of time, gives the same result |
| Analytical Reproducibility | A measure of the extent to which a test conducted multiple times in different laboratories, using different equipment, by different operators, or over different periods of time, gives comparable results |
| Term | Definition |
|---|---|
| Diagnostic Sensitivity | The measure of how often a binary biomarker test correctly indicates the presence of a particular characteristic in individuals that truly have the characteristic. Biomarker sensitivity is the number of true positive results divided by the number of true-positive plus false-negative results. |
| Diagnostic Specificity | The measure of how often a binary biomarker test correctly indicates the absence of a particular characteristic in individuals who truly do not have the characteristic. Biomarker specificity is the number of true-negative results divided by the number of true-negative plus false-positive results. |
| Positive predictive value | The measure of how often a binary biomarker test correctly indicates the presence of a particular characteristic in individuals that have a positive test result. Biomarker positive predictive value is the number of true positive results divided by the number of true-positive plus false-positive results. |
| Negative predictive value | The measure of how often a binary biomarker test correctly indicates the absence of a particular characteristic in individuals that have a negative test result. Biomarker negative predictive value is the number of true negative results divided by the number of true-negative plus false-negative results. |
| Receiver operating characteristics (ROC) curve | Plot showing the relationship between sensitivity (true positive) and 1-specificity (true negative). It is a graphical way of describing likelihood ratios at various values of the biomarker test. |
| Area under the ROC curve (AUCROC) | The ability of a binary biomarker to distinguish two or more groups of individuals. It is a measure of discrimination. Values range from 0 to 1, and 1 corresponds to perfect discriminative power. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarhadi, V.K.; Armengol, G. Molecular Biomarkers in Cancer. Biomolecules 2022, 12, 1021. https://doi.org/10.3390/biom12081021
Sarhadi VK, Armengol G. Molecular Biomarkers in Cancer. Biomolecules. 2022; 12(8):1021. https://doi.org/10.3390/biom12081021
Chicago/Turabian StyleSarhadi, Virinder Kaur, and Gemma Armengol. 2022. "Molecular Biomarkers in Cancer" Biomolecules 12, no. 8: 1021. https://doi.org/10.3390/biom12081021
APA StyleSarhadi, V. K., & Armengol, G. (2022). Molecular Biomarkers in Cancer. Biomolecules, 12(8), 1021. https://doi.org/10.3390/biom12081021